
Stomach
Carcinoma
Early gastric carcinoma
Author: Nathalie Guedj, M.D., Ph.D.
Editorial Board Member: Aaron R. Huber, D.O.
Deputy Editor-in-Chief: Catherine E. Hagen, M.D.

Last author update: 6 August 2021
Last staff update: 6 September 2023
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Early gastric carcinoma


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Molecular / cytogenetics images | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Guedj N. Early gastric carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/stomachearlygastriccarcinoma.html. Accessed April 1st, 2025.
Definition / general
- Early gastric cancer (EGC) is defined as a cancer confined to the mucosa or submucosa, regardless of lymph node metastasis
Essential features
- Defined as a cancer confined to the mucosa or submucosa, regardless of lymph node metastasis
- Tubular adenocarcinoma is the most common histologic type
- EGC is preceded by a cascade of precancerous lesions
- Diagnosis is made by endoscopy confirmed by biopsy
- Lymph node metastasis is the most important prognostic factor
Terminology
- Mucosal or submucosal gastric carcinoma
ICD coding
- ICD-10: C16 - malignant neoplasm of stomach
Epidemiology
- In a large Chinese series of 4,380 consecutive gastric carcinomas (J Dig Dis 2018;19:586):
- Frequency: 17%
- Average age of patients: 62.2 years
- M:F = 2.29:1
- EGC is more commonly observed in China, Japan and Korea, due in large part to screening
Sites
- In the stomach (J Dig Dis 2018;19:586):
- Cardia: 18.8%
- Corpus / fundus: 13.4%
- Antrum / angularis / pylorus: 67.8%
Pathophysiology
- In response to gastric epithelial injury, mainly by environmental factors such as Helicobacter pylori and Epstein-Barr virus (EBV) induced chronic inflammation, gastric stem cells in the affected region become dysfunctional, leading to dysregulated differentiation and gastric carcinoma (Gastrointest Tumors 2017;3:115)
- EGC is preceded by a cascade of precancerous lesions: chronic gastritis (atrophic or not) → intestinal metaplasia (complete or not) → low grade dysplasia → high grade dysplasia (in situ carcinoma) → invasive carcinoma (J Dig Dis 2012;13:2)
Etiology
- Multifactorial disease
- Sporadic in 90% of cases
- Familial / hereditary setting in 10%: CDH1 mutation in hereditary diffuse gastric carcinoma, APC mutation and proximal polyposis
- Environmental factors include smoking, diet (high intake of salt, preserved or smoked foods, meat), Helicobacter pylori or EBV infection
- Reference: Gastroenterol Clin North Am 2013;42:219
Clinical features
- Frequently asymptomatic
- If symptomatic, clinical features are nonspecific (epigastralgia, dyspeptic syndrome)
Diagnosis
- Endoscopy, with or without the dye spraying method, is the method of choice
- Diagnosis is confirmed with biopsies
Laboratory
- Anemia
Radiology description
- Endoscopic ultrasound (EUS) has become a reliable method for predicting the invasion depth of EGC
Radiology images
Images hosted on other servers:

EUS, mucosal gastric cancer
Prognostic factors
- 5 year cancer specific survival for gastric cancer confined to the mucosa and submucosa is 99.3% and 96.7%, respectively (Dig Endosc 2020;32:180)
- Lymph node metastasis is the most important prognostic factor in gastric carcinoma
Case reports
- 40 year old asymptomatic woman (Korean J Gastroenterol 2013;62:122)
- 49 year old woman was hospitalized due to epigastric pain (Niger J Clin Pract 2017;20:1342)
- 64 year old Japanese woman presented with a recurrent cystic lesion on the left bulbar conjunctiva (Gastric Cancer 2002;5:102)
Treatment
- Gastrectomy with lymphadenectomy is the gold standard treatment (Dig Endosc 2020;32:180)
- However, when the prognosis of patients with endoscopic resection is similar to that of patients with gastrectomy in some categories of EGC, endoscopic resection is acceptable
- Endoscopic resection should be en bloc because precise pathological diagnosis is essential for risk assessment of lymph node metastasis and there is potential risk of local recurrence after piecemeal resection
- Endoscopic resection is sufficient if the risk of lymph node metastasis is low:
- Tumor size < 30 mm
- Absence of lymphatic invasion
- Submucosal invasion < 500 μm (sm1)
- Negative vertical margin
- Absence of vascular invasion
Clinical images
Images hosted on other servers:

Endoscopy, type 0 lesions
Gross description
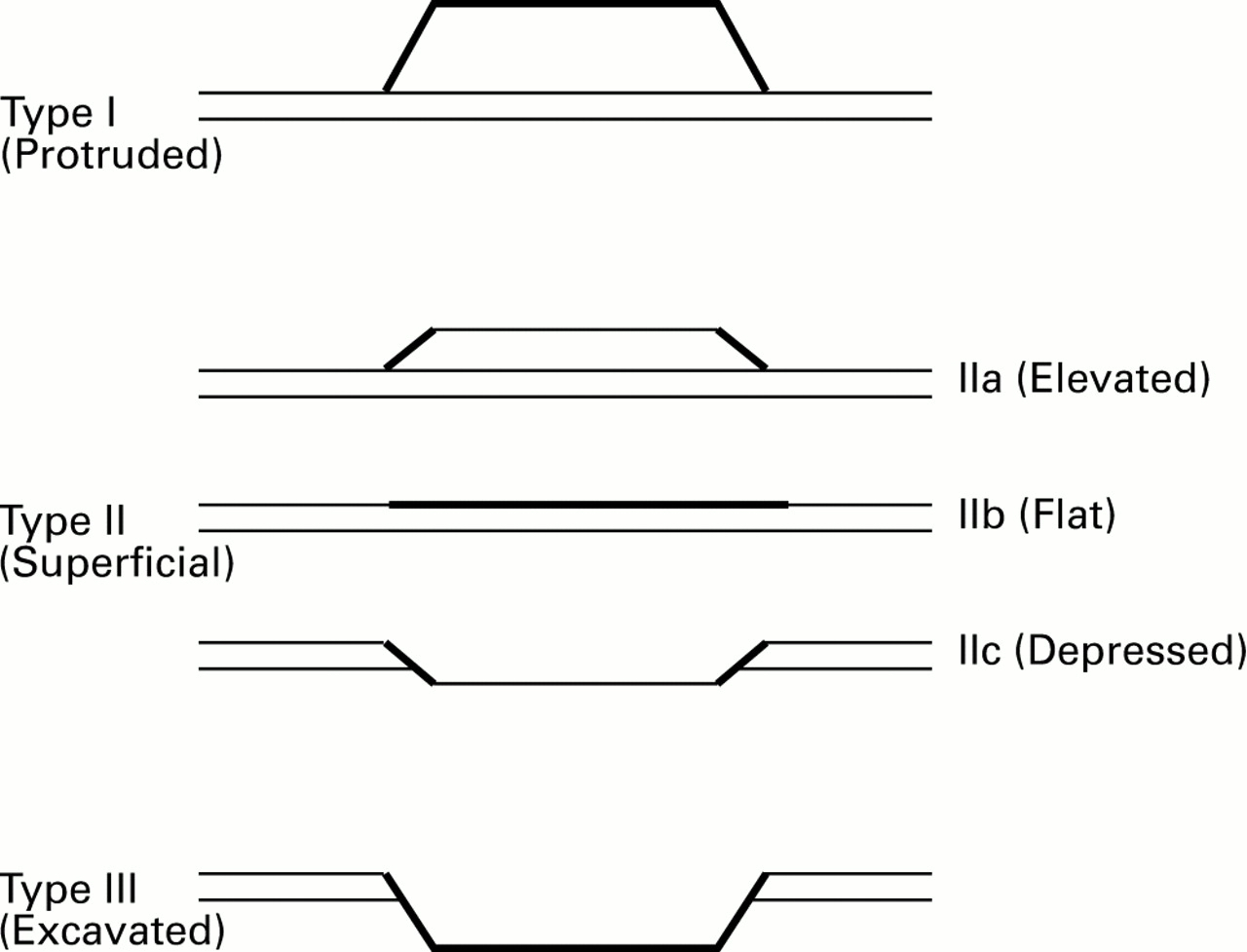
- Macroscopically subclassified into 3 main types: 0-I, 0-II and 0-III (see Diagram above)
- Type 0-I: protruding
- Type 0-IIa: superficially elevated
- Type 0-IIb: flat
- Type 0-IIc: superficially depressed
- Type 0-III: excavated
- Reference: Rev Gastroenterol Mex (Engl Ed) 2020;85:69
Gross images
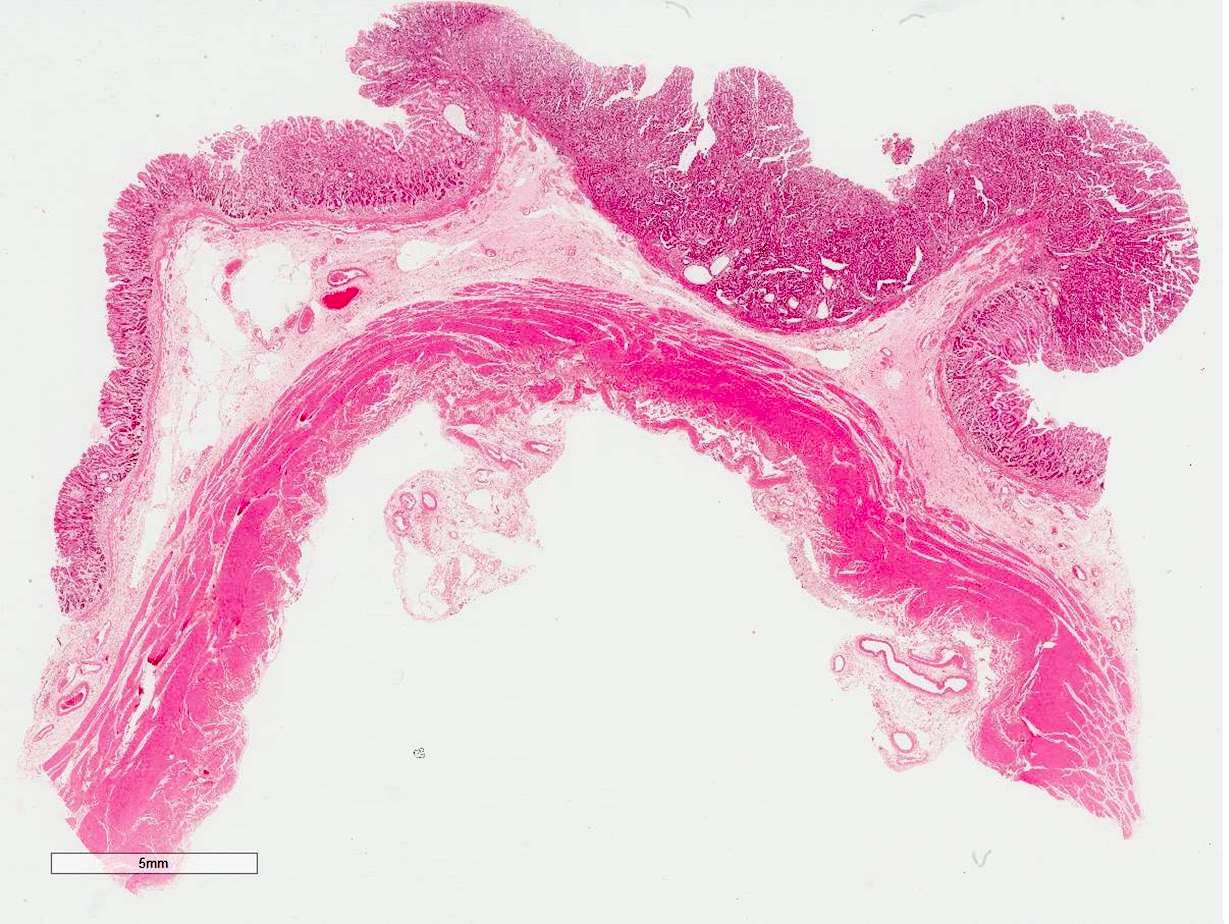
Contributed by Guedj Nathalie, M.D., Ph.D.

Type 0-IIc
Microscopic (histologic) description
- Tubular adenocarcinoma is the most common histologic type (Gastrointest Tumors 2017;3:115)
- Nuclear abnormalities
- Hyperchromasia, nuclear enlargement, high nuclear to cytoplasmic ratio, marked pleomorphism, increased mitotic figures with atypical forms, prominent nucleoli
- Glandular structures with subtle architectural changes, mimicking the letters W, H , Y or X at low power view
- Nuclear abnormalities
- Papillary adenocarcinoma
- Finger-like projections on the mucosal surface
- Lined with neoplastic columnar cells
- Micropapillary and tubular components
- Worse prognosis compared with tubular adenocarcinoma: more lymphovascular invasion and nodal metastasis
- Poorly cohesive carcinoma, including signet ring cell carcinoma
- Neoplastic cells that are isolated or arranged in small aggregates without well formed glands
- Signet ring cells are characterized by a central, optically clear, globoid droplet of cytoplasmic mucin with an eccentrically placed nucleus
- There is low risk of nodal metastasis for intramucosal signet ring cell carcinoma
- Mucinous adenocarcinoma
- Malignant epithelium and extracellular mucin pools
- Rare subtypes: gastric carcinoma with lymphoid stroma, hepatoid adenocarcinoma, micropapillary adenocarcinoma, gastric adenocarcinoma of fundic gland type
Microscopic (histologic) images
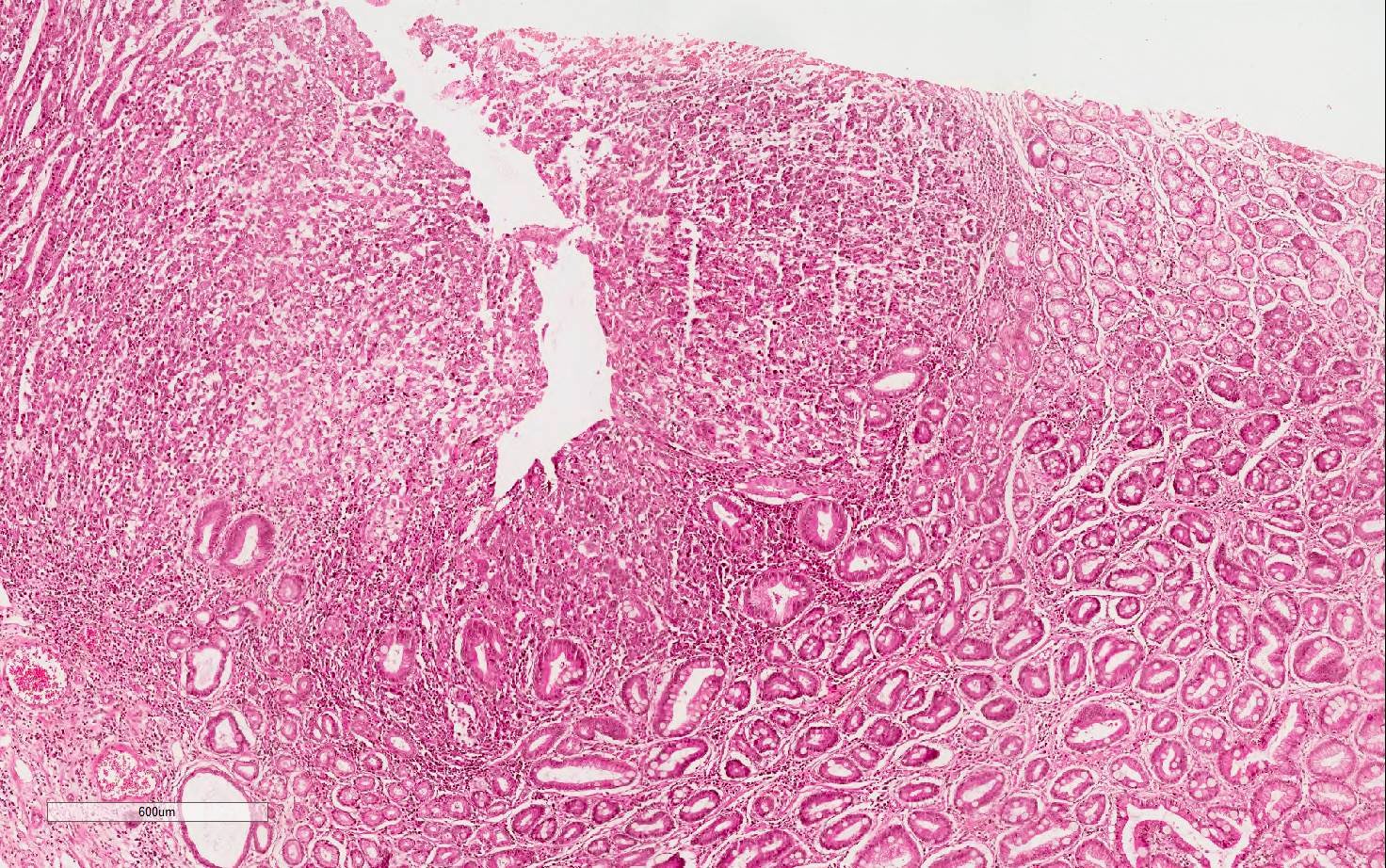
Contributed by Guedj Nathalie, M.D., Ph.D.
Gastric adenocarcinoma
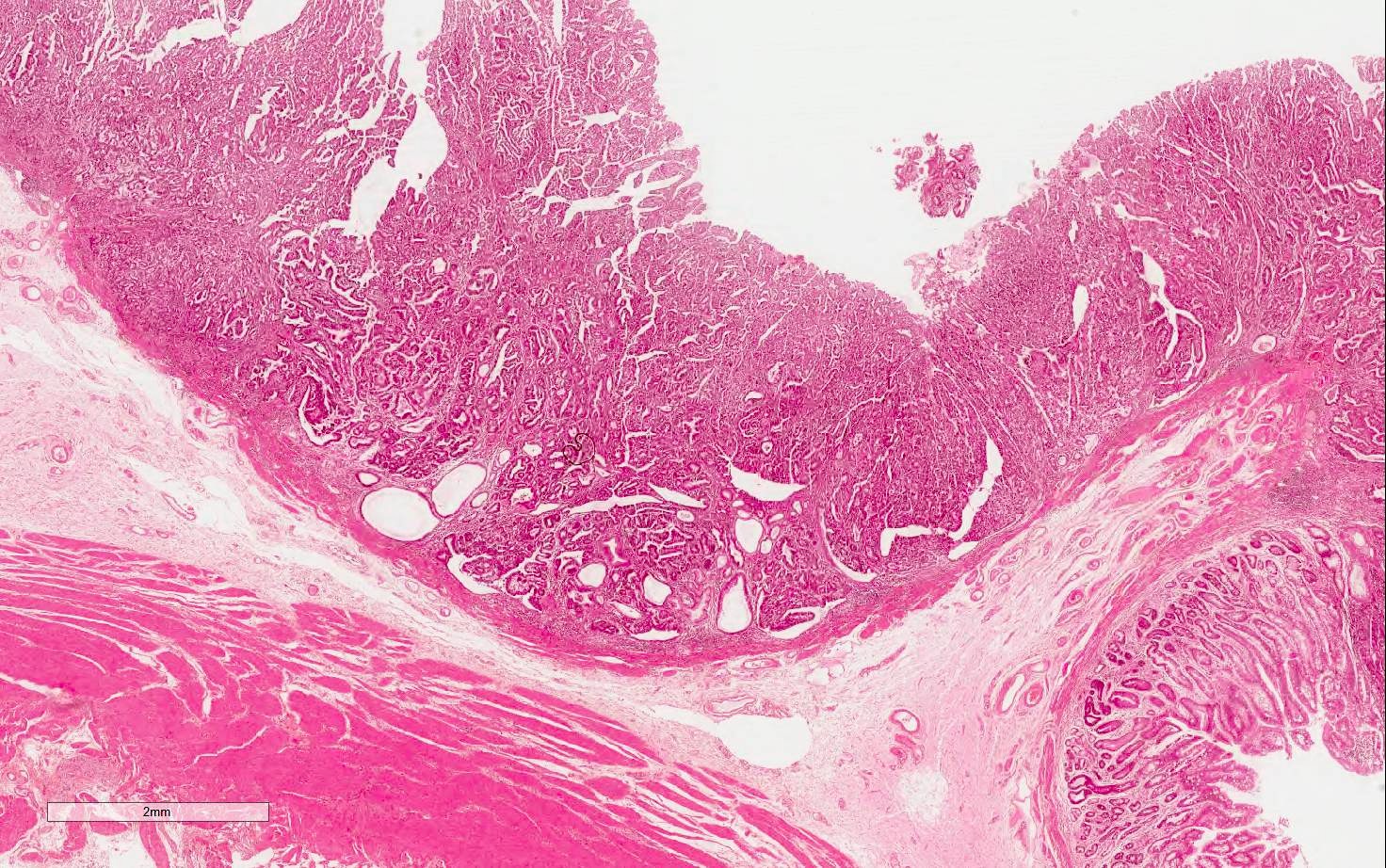
Tubular adenocarcinoma

Cytologic and nuclear atypia
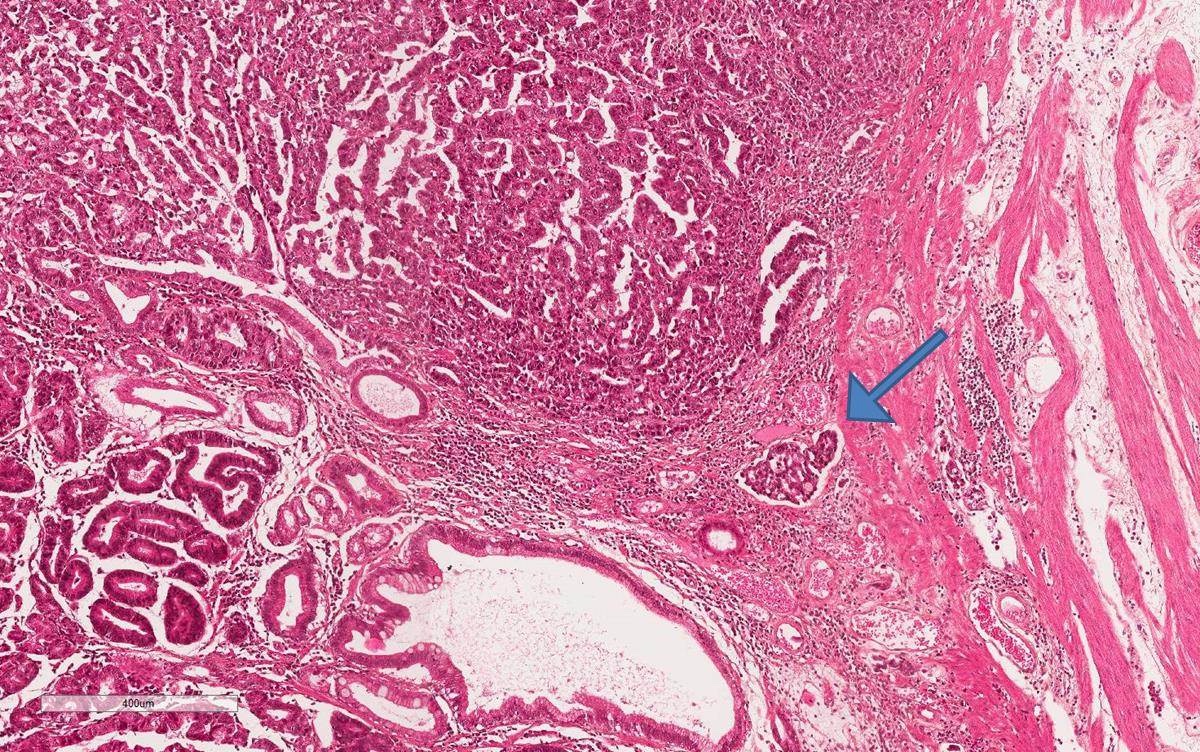
Angioinvasion
Positive stains
Negative stains
Molecular / cytogenetics description
Molecular / cytogenetics images
Videos
Early gastric carcinoma
Sample pathology report
- Stomach, distal gastrectomy:
- Submucosal tubular gastric adenocarcinoma; an elevated lesion, type 0-IIa of 4 cm (see comment)
- Comment: Histological study of whole lesion shows predominantly intramucosal adenocarcinoma, with focal extension beyond the muscularis mucosa. The infiltration depth does not exceed 500 μm. Carcinoma architecture is tubular. Lymphovascular invasion is present.
Differential diagnosis
Additional references
Board review style question #1
What is the most common histologic type of early gastric carcinoma?
- Hepatoid carcinoma
- Mucinous adenocarcinoma
- Papillary adenocarcinoma
- Signet ring cell carcinoma
- Tubular adenocarcinoma
Board review style answer #1
Board review style question #2
What is the most important prognostic factor of early gastric carcinoma?
- Angioinvasion
- Incomplete mucosal resection
- Lymph node metastasis
- Perineural invasion
- Tumor size
Board review style answer #2
