

Soft tissue
Fibroblastic / myofibroblastic
Solitary fibrous tumor
Editorial Board Member: Jose G. Mantilla, M.D.
Deputy Editor-in-Chief: Borislav A. Alexiev, M.D.


Last author update: 10 May 2021
Last staff update: 26 February 2024
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Soft tissue solitary fibrous tumor
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Molecular / cytogenetics images | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Dermawan JK, Fritchie K. Solitary fibrous tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/softtissuesft.html. Accessed April 25th, 2024.
Definition / general
- Fibroblastic tumor characterized by haphazardly arranged spindled to ovoid cells, prominent staghorn vasculature and NAB2-STAT6 gene rearrangement
Essential features
- Haphazard arrangement of spindled to ovoid cells arranged around branching and dilated vasculature within variably collagenous stroma
- Occurs at any anatomical site with a wide range of histological patterns
- CD34 usually strong and diffuse but nonspecific
- STAT6 immunohistochemistry highly sensitive and specific surrogate for NAB2-STAT6 gene fusion (Mod Pathol 2014;27:390)
- Risk stratification preferred over anatomic staging (Mod Pathol 2017;30:1433)
Terminology
- Hemangiopericytoma (no longer preferred) (Cancer 1975;36:2232)
- Giant cell angiofibroma (no longer preferred)
ICD coding
- ICD-10: D48.1 - neoplasm of uncertain behavior of connective and other soft tissue
Epidemiology
- M = F
- Adults, peak incidence 40 - 70 years old (Cancer 1975;36:2232)
Sites
- Any anatomic site: superficial and deep soft tissues, visceral organs and bone (Cancer 2002;94:1057)
- Deep > superficial (Eur J Surg Oncol 2016;42:1064)
- Extrapleural > pleural locations (see pleural solitary fibrous tumor) (Mod Pathol 2012;25:1298)
- Extremities, abdominal cavity, pelvis, retroperitoneum > head and neck (sinonasal, orbit), trunk
Pathophysiology
- Paracentric inversion involving chromosome 12q, resulting in NAB2-STAT6 gene fusion (Nat Genet 2013;45:131, Nat Genet 2013;45:180)
- NAB2-STAT6 fusions converts NAB2 from transcriptional repressor to activator
- Altered NAB2 function leads to constitutive (deregulated) expression of early growth response 1 (EGR1) target genes, including IGF2, FGFR1 (Genes Chromosomes Cancer 2013;52:873, J Pathol 2010;221:300)
- Other mechanisms include overexpression of:
- ALDH1, EGFR, JAK2 (PLoS One 2013;8:e64497)
- TERT promoter mutations (Histopathology 2018;73:843)
Etiology
- Unknown
Diagrams / tables
Images hosted on other servers:

Modified 4 variable risk stratification model
Clinical features
- Symptoms associated with anatomic location
- Somatic soft tissue tumors present as slow growing, painless mass
- Abdominopelvic tumors produce symptoms due to organ impingement (Eur Urol 2008;54:1188)
- Pleural tumors often discovered incidentally but could grow exophytically into lungs
- Paraneoplastic syndrome (Doege-Potter syndrome) extremely rare; due to IGF2 production by tumor (J Endocr Soc 2019;3:537)
Diagnosis
- Imaging features are nonspecific and diagnosis is dependent on histologic findings
Radiology description
- CT: well defined, sometimes lobulated mass that is isodense to skeletal muscle with heterogeneous contrast enhancement (Clin Imaging 2018;48:48)
- MRI: T1 intermediate and T2 hypointense (cellular / fibrous areas) to hyperintense (myxoid areas) signals (Radiol Clin North Am 2016;54:565)
Radiology images
Contributed by Borislav A. Alexiev, M.D.
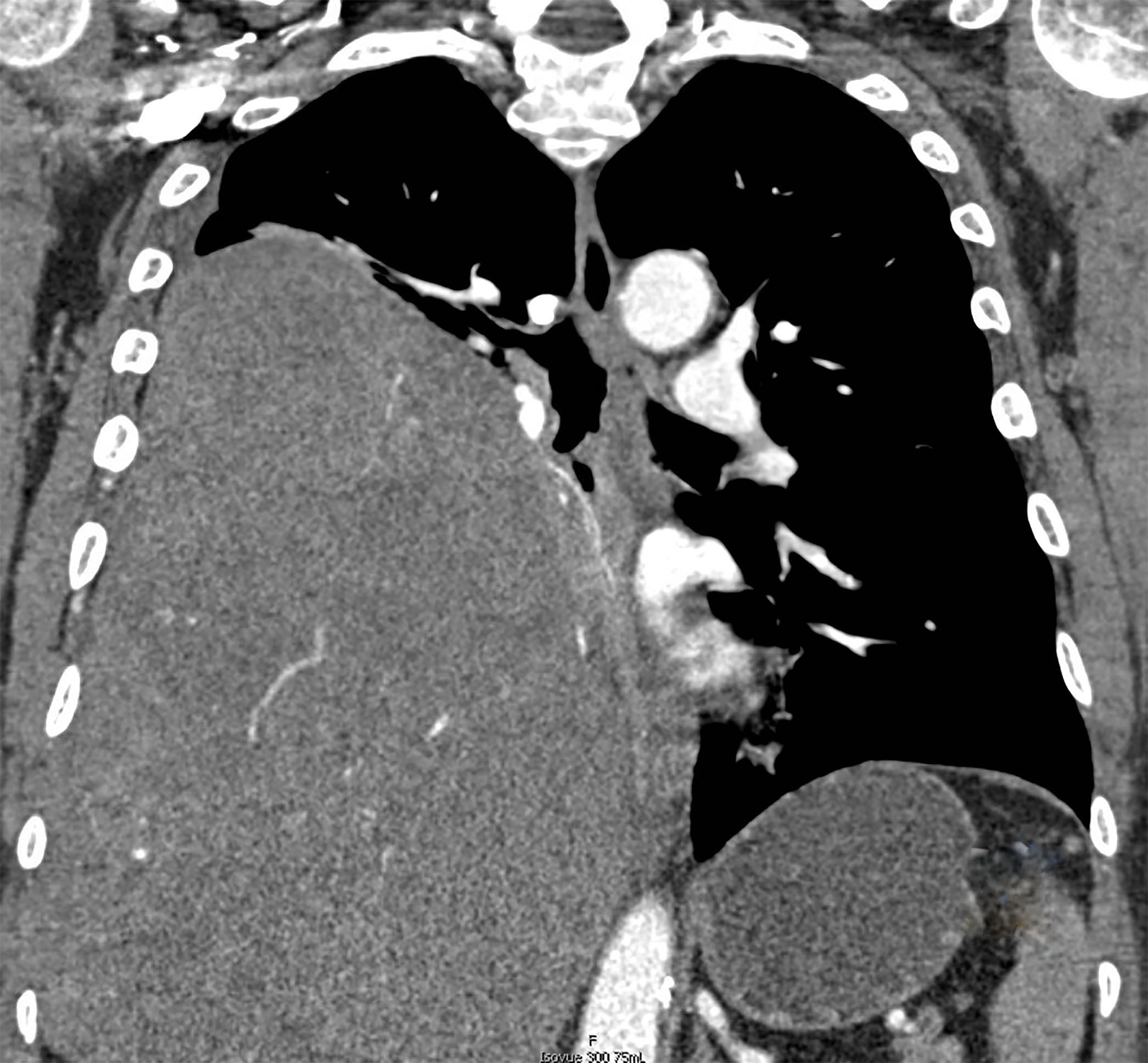
Pleural mass
Images hosted on other servers:

Bulky thyroid tumor (CT)

Huge perineal mass (CT)

Ischiorectal fossa mass (MRI)

Bladder serosa mass (CT)
Prognostic factors
- 10 - 30% (local or distant) recurrence rate (Cancer 1975;36:2232, Ann Oncol 2017;28:1979, Mod Pathol 2012;25:1298, Eur J Surg Oncol 2016;42:1064)
- 5 and 10 year disease specific survival rates 89 and 73%, respectively (Mod Pathol 2012;25:1298)
- Adverse prognostic factors: mitotic count > 4 per 10 high power fields, tumor size > 10 cm, necrosis, hypercellularity, cellular atypia, dedifferentiation, location in chest, abdomen or pelvis, TERT promoter mutations (Eur J Surg Oncol 2016;42:1064, Am J Surg Pathol 1998;22:1501, Ann Oncol 2017;28:1979, Ann Surg Oncol 2017;24:3865, Mod Pathol 2012;25:1298, Mod Pathol 2016;29:1511, Virchows Arch 2019;475:467)
- Numerous risk stratification models exist, the most widely used one classifies tumors into groups of low, intermediate and high risk for metastasis using mitotic count, age, tumor size and necrosis (Mod Pathol 2017;30:1433, J Thorac Oncol 2018;13:1349)
- French Federation of Cancer Centers Sarcoma Group (FNCLCC) grading system is not applicable
Case reports
- 18 year old man with right orbital tumor (J Cancer Res Ther 2019;15:719)
- 34 year old woman with kidney mass showing sarcomatous overgrowth (APMIS 2008;116:1020)
- 41 year old man with massive bladder mass (J Med Case Rep 2015;9:46)
- 44 year old woman with recurrent spinal cord mass (Clin Neuropathol 2020;39:86)
- 48 year old man with a scrotal mass (BMC Urol 2019;19:138)
- 57 year old man with a palatal mass (Head Neck Pathol 2008;2:236)
- 62 year old man with prostatic mass (Diagn Pathol 2017;12:50)
- 64 year old man with 23.0 cm perineal mass (Case Rep Urol 2017;2017:4876494)
- 68 year old woman with left retroperitoneal soft tissue mass anterior to the psoas (Case of the Month #505)
- 77 year old woman with a 1.5 cm tracheal mass (Gen Thorac Cardiovasc Surg 2020;68:1523)
Treatment
- Surgical resection remains gold standard of treatment (Brain Res 1998;809:297, Ann Surg Oncol 2013;20:4090)
- Long term surveillance following surgery recommended (ERJ Open Res 2020;6:00055)
- Combined surgery and radiation therapy may improve local control (Am J Clin Oncol 2018;41:81)
- Role of chemotherapy controversial and limited (J Thorac Oncol 2015;10:309)
Clinical images
Images hosted on other servers:

Palatal mass causing proptosis

Huge perineal mass
Gross description
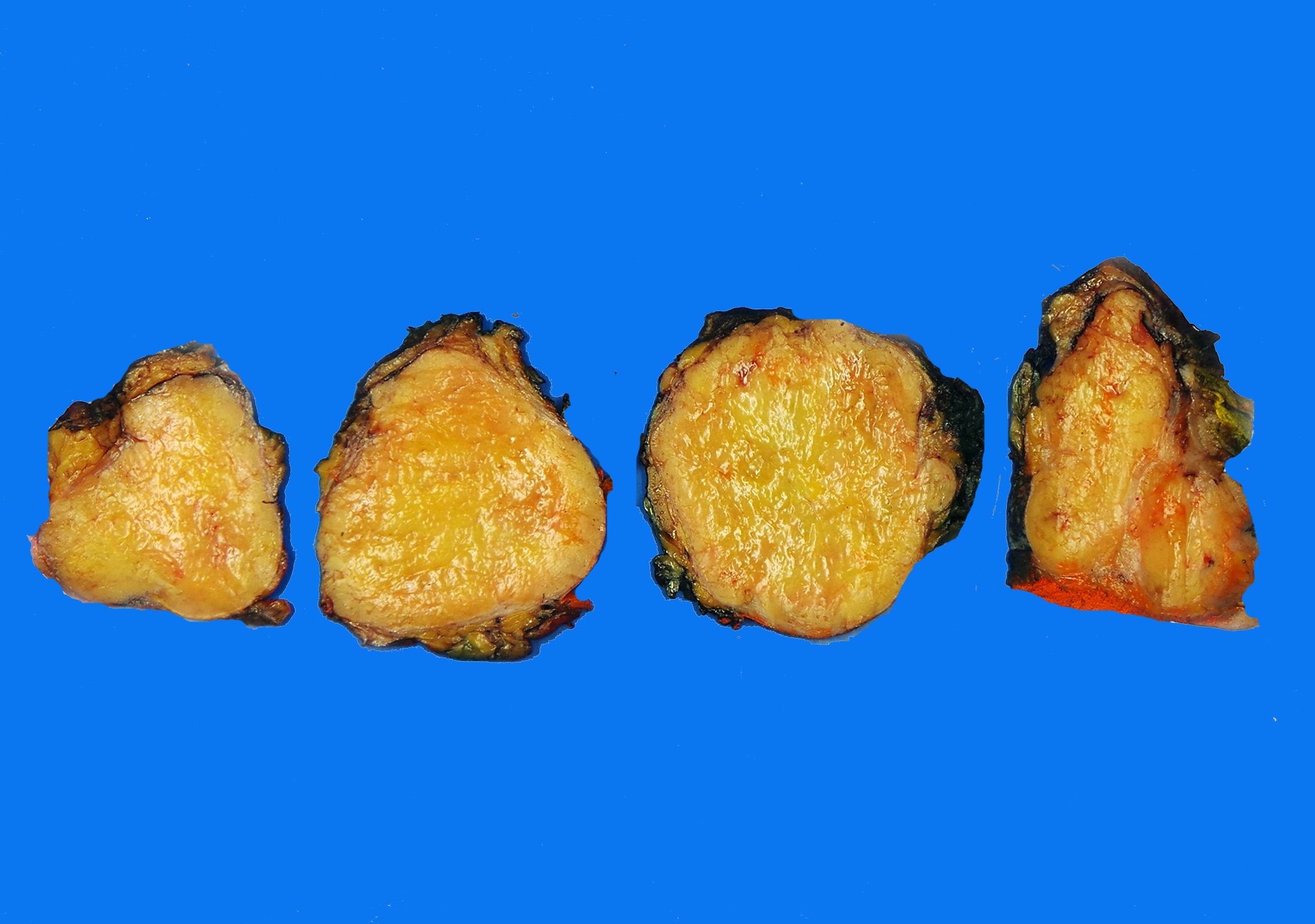
- Usually unencapsulated but well circumscribed mass, sometimes lobulated
- Exophytic lesions on serosal surfaces
- 5 - 15 cm in greatest diameter
- Gray-white, yellow to red-brown color
- Fibrous and firm cut surface
- Cystic, hemorrhagic or myxoid degeneration may be present
- Tumor necrosis and hemorrhage in malignant tumors
- Reference: Am J Surg Pathol 1995;19:1257
Gross images
Contributed by Borislav A. Alexiev, M.D. (Case #505)
Fat forming SFT
Images hosted on other servers:

Solid white cut surface

Circumscribed lobulated mass

Central necrosis

Fleshy nodules
Frozen section description
- Circumscribed spindled cell tumor
- Presence of staghorn vasculature helpful but not entirely specific
Microscopic (histologic) description
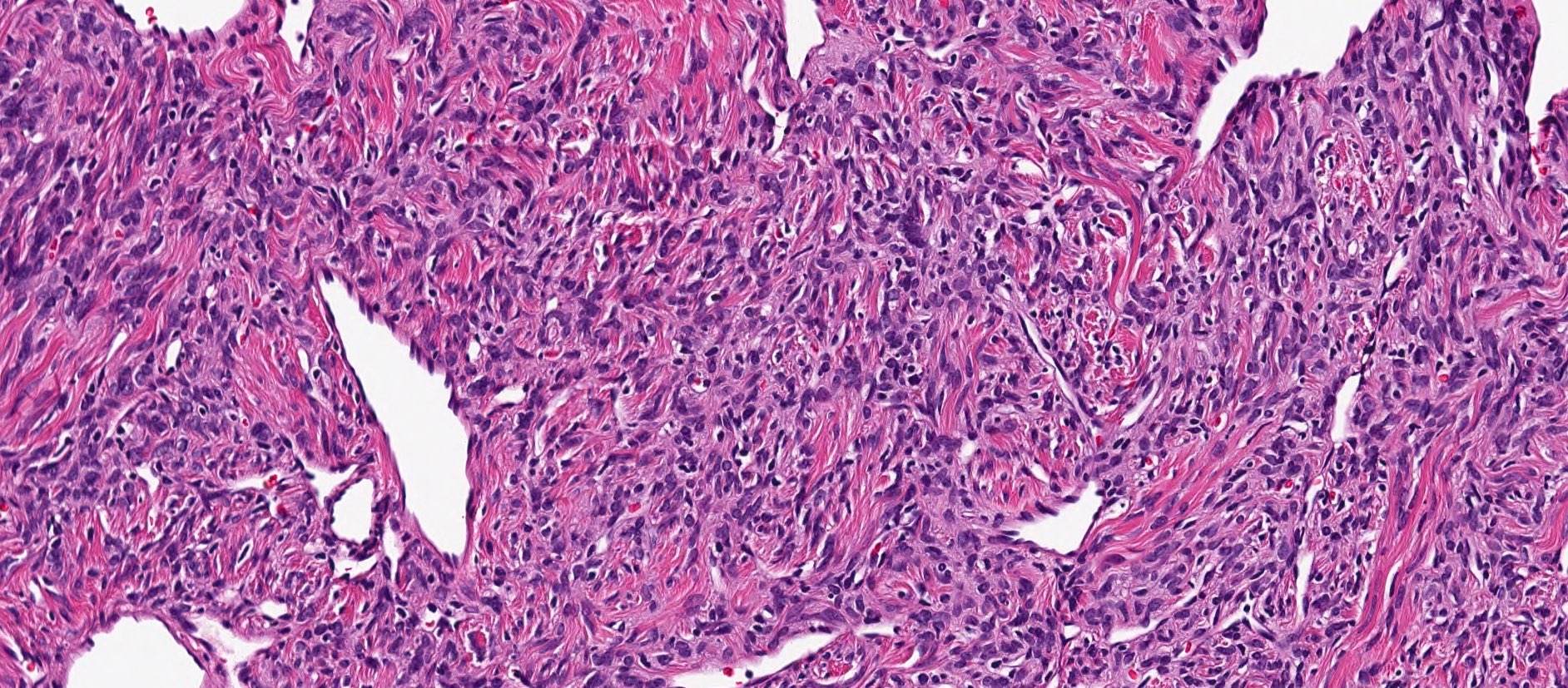
- Ovoid to fusiform spindle cells with indistinct cell borders arranged haphazardly or in short, ill defined fascicles
- Dilated, branching, hyalinized staghorn-like (hemangiopericytoma-like) vasculature
- Hyalinized to collagenous stroma, sometimes with streaming of cells between collagen
- Myxoid changes can be prominent (Mod Pathol 1999;12:463)
- Lipomatous variant contains variable amount of fat (Am J Surg Pathol 1999;23:1201)
- Giant cell rich variant, formerly known as giant cell angiofibroma, shows admixed multinucleated giant cells lining pseudovascular spaces (Am J Surg Pathol 1995;19:1286)
- Tumors with high mitotic count, hypercellularity, atypia (round cell and anaplastic morphology, nuclear pleomorphism) and necrosis have been termed malignant (Am J Surg Pathol 2009;33:1314, Am J Surg Pathol 1998;22:1501)
- Dedifferentiated (anaplastic) solitary fibrous tumor shows transition to high grade sarcomatous areas with or without heterologous components (Am J Surg Pathol 2009;33:1314, Am J Surg Pathol 2012;36:1202, Ann Diagn Pathol 2013;17:457)
Microscopic (histologic) images
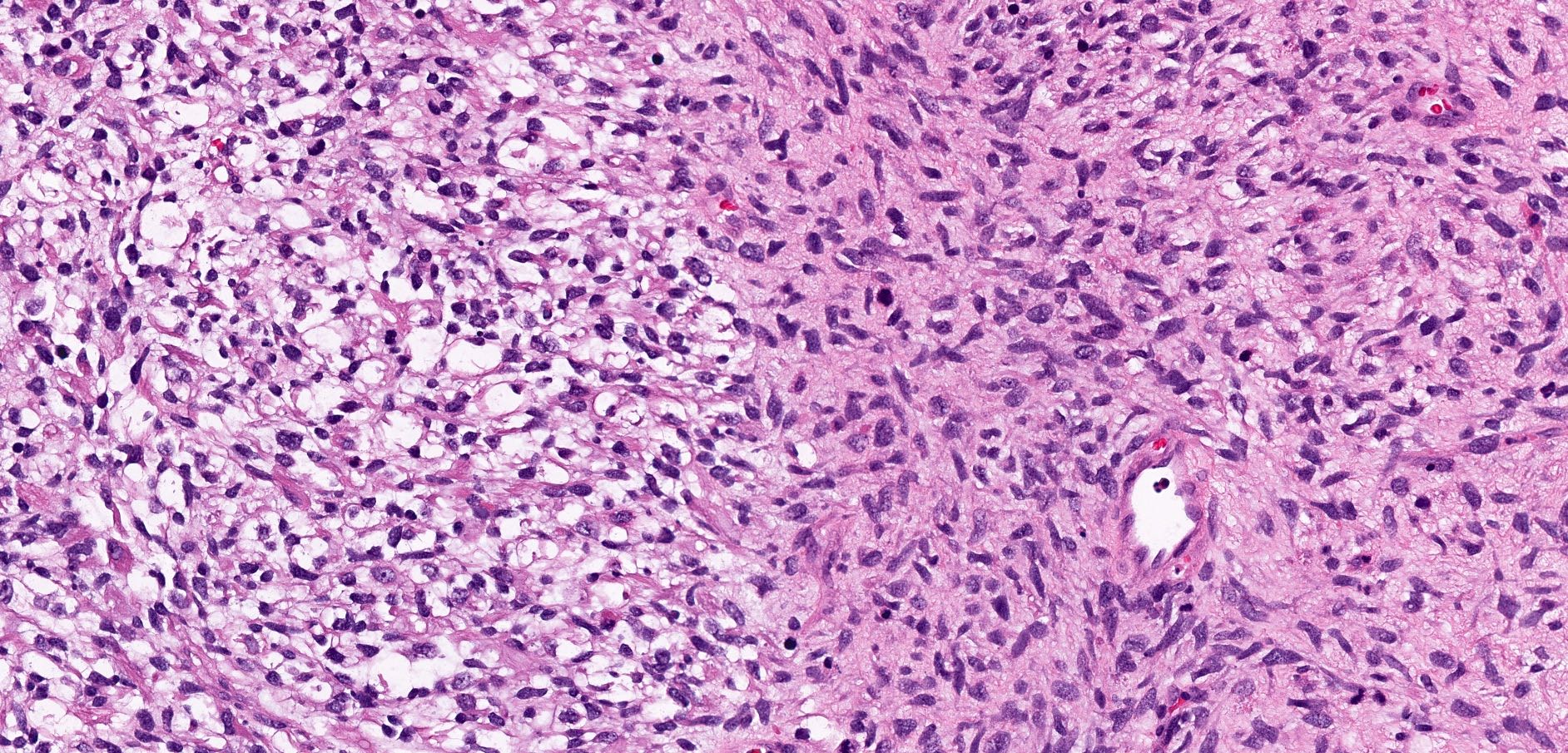
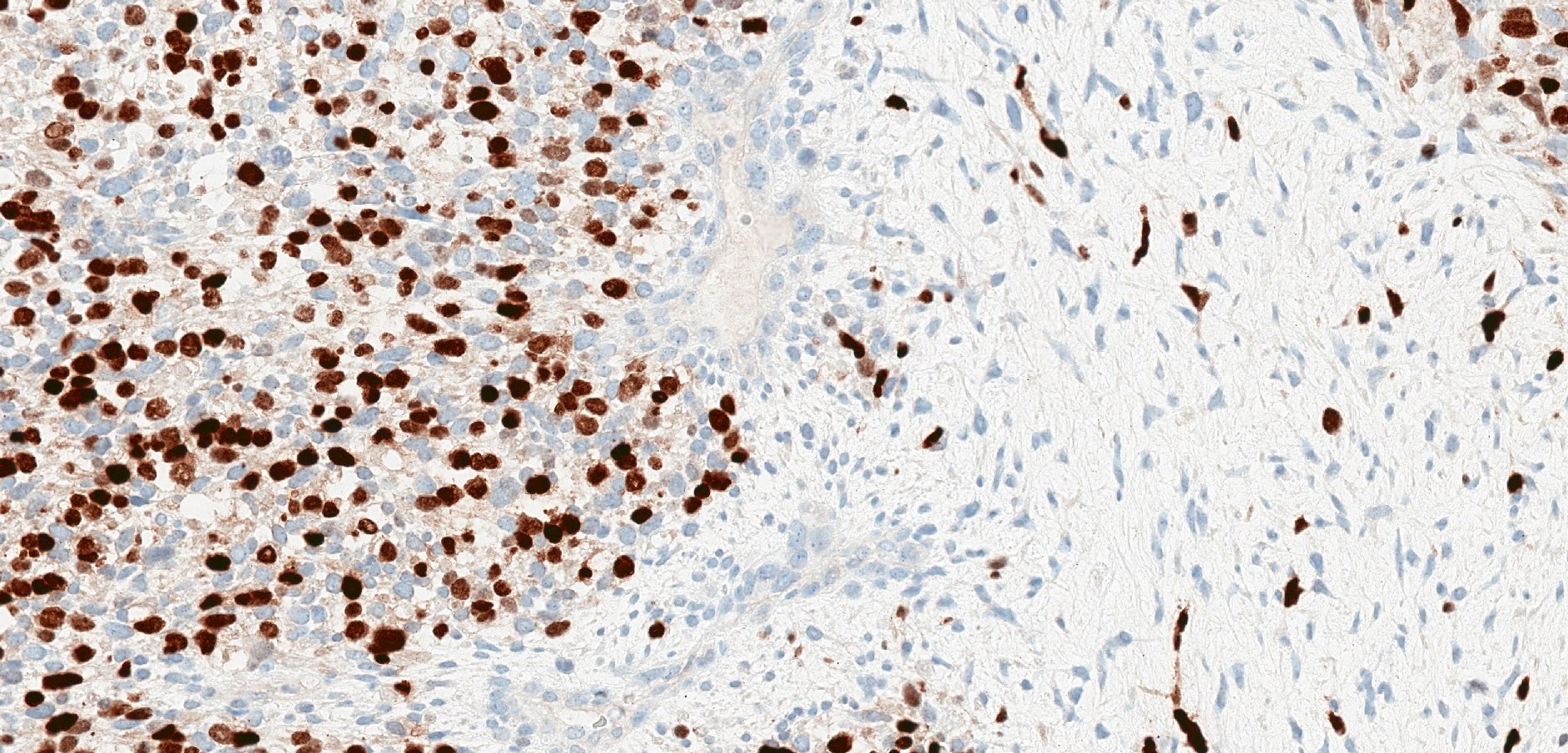
Contributed by Josephine Dermawan, M.D., Ph.D., Karen Fritchie, M.D.
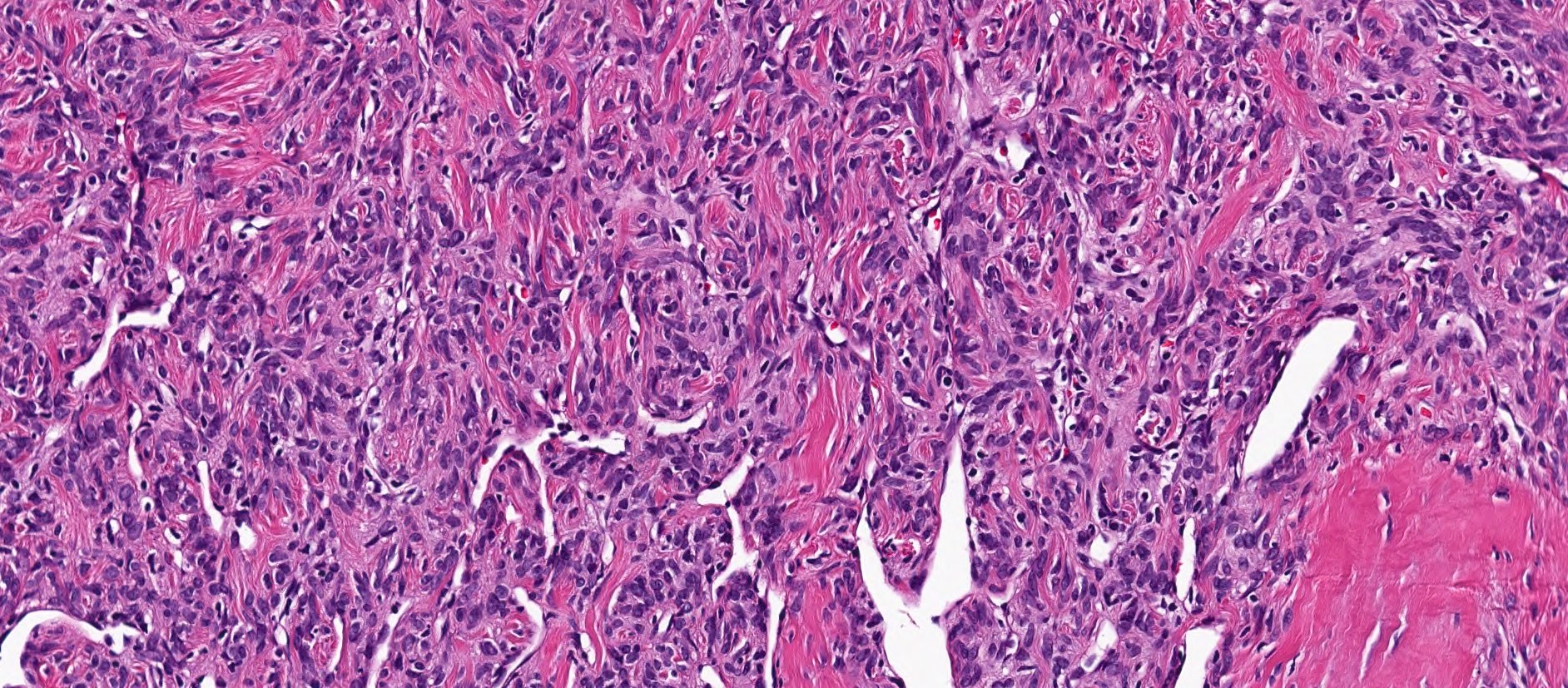
Ovoid to fusiform cells
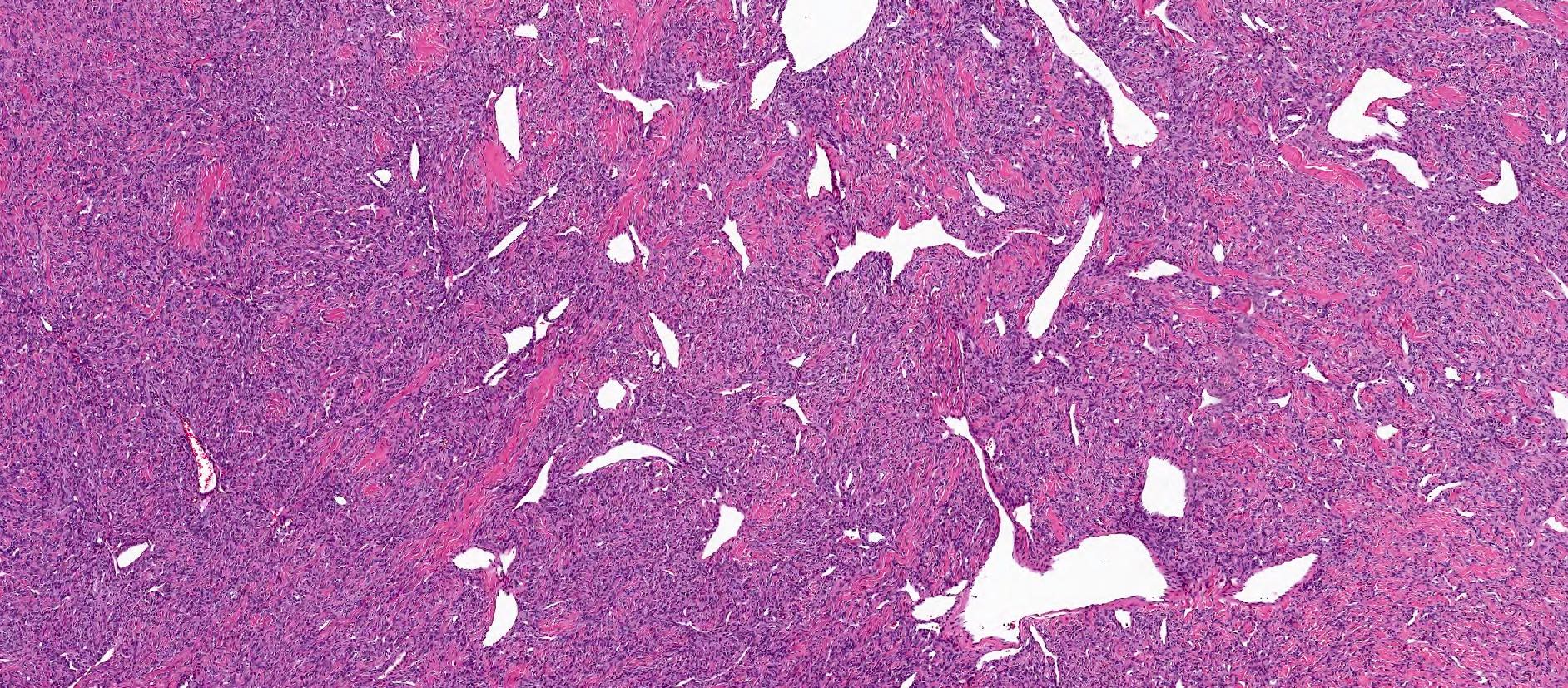
Staghorn vasculature
Collagenous stroma
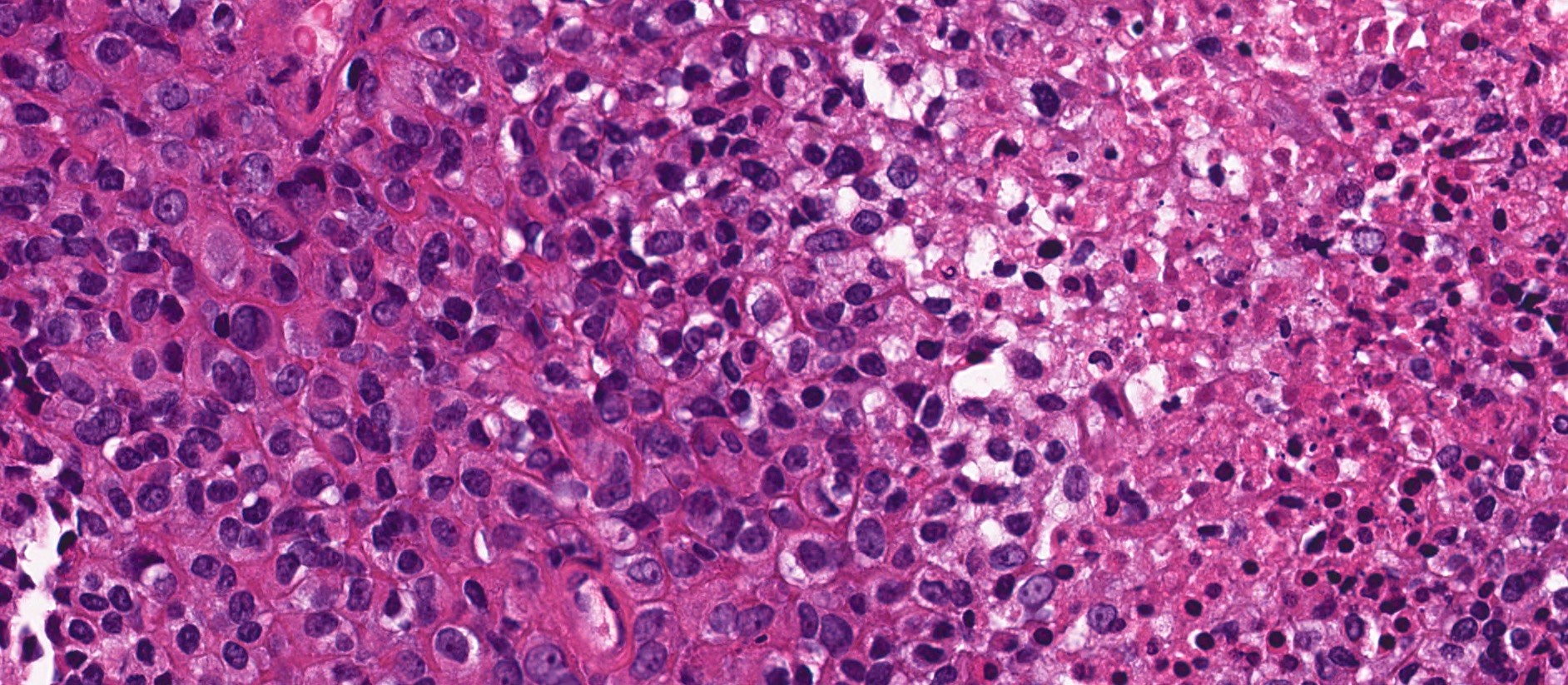
High risk solitary fibrous tumor

Metastatic solitary fibrous tumor
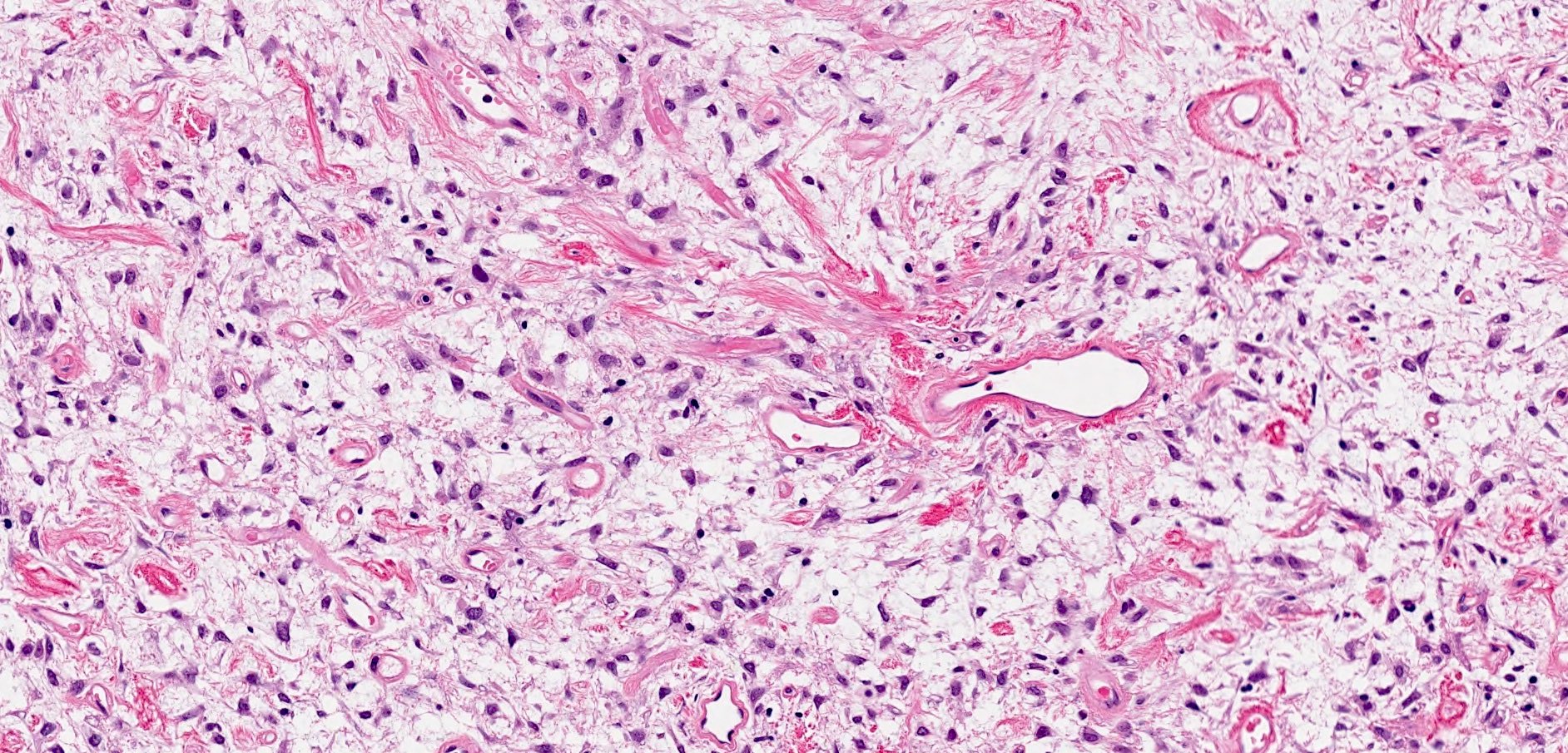
Myxoid solitary fibrous tumor
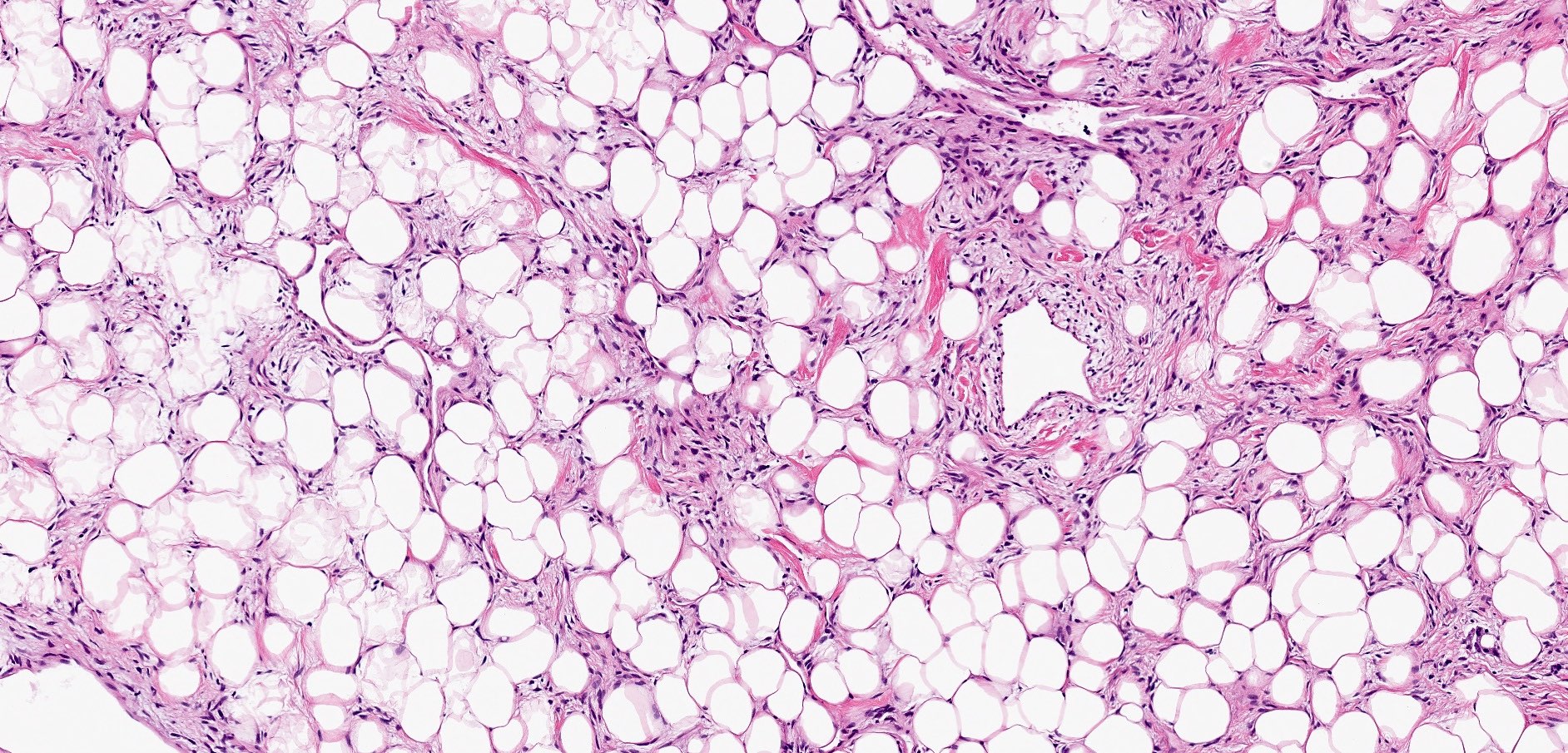
Lipomatous solitary fibrous tumor
Dedifferentiated solitary fibrous tumor

Diffuse and strong CD34
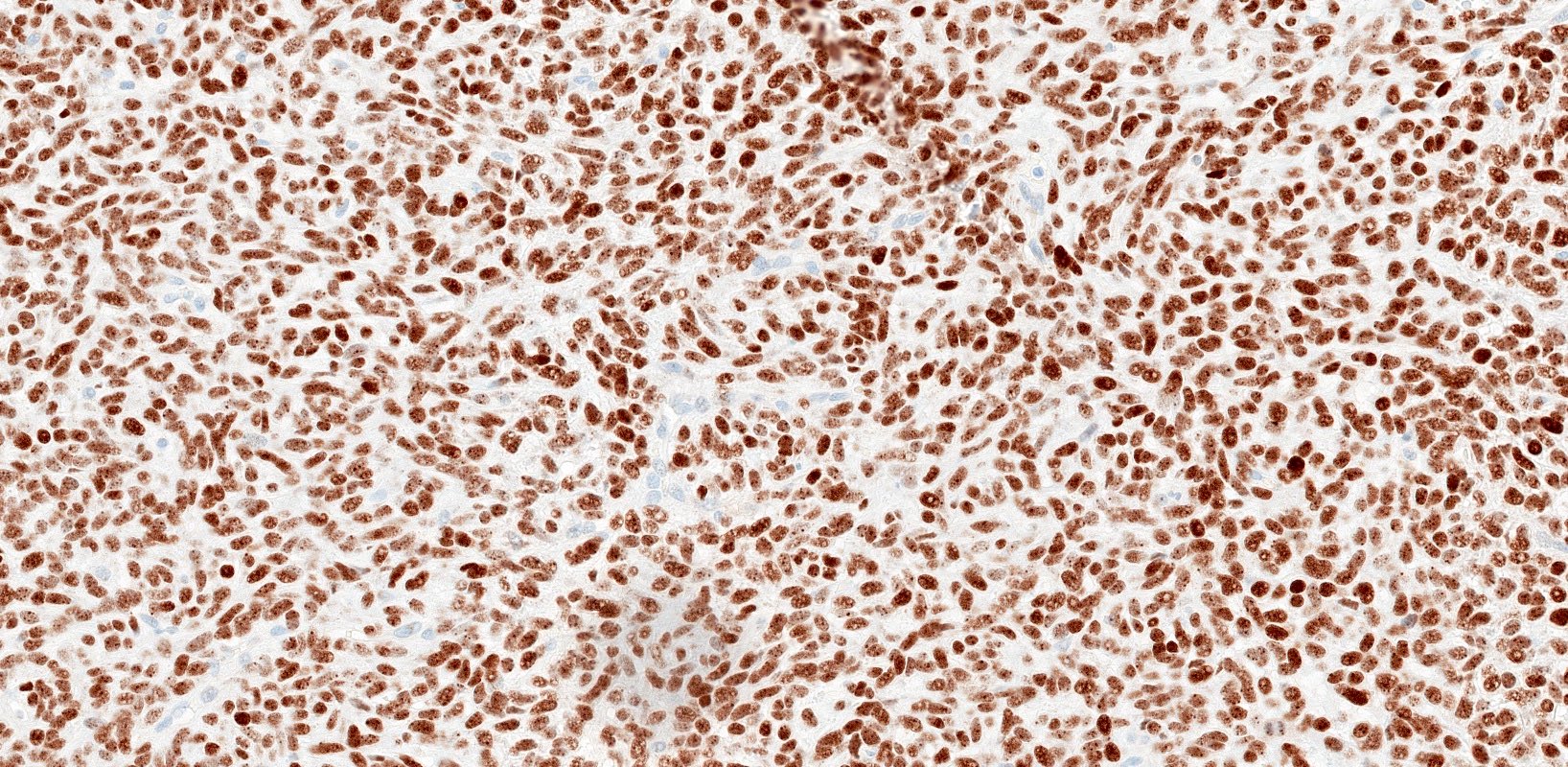
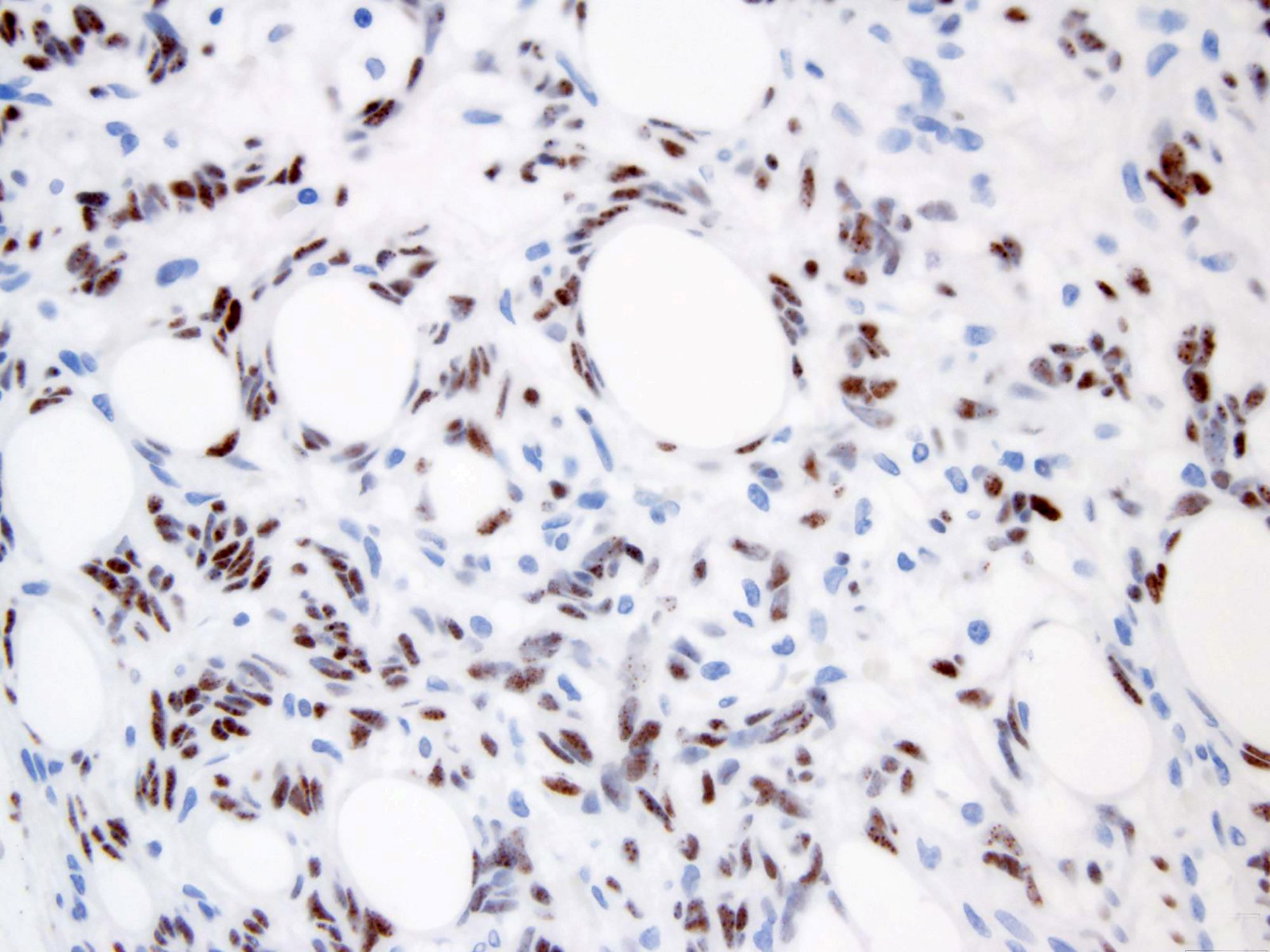
STAT6
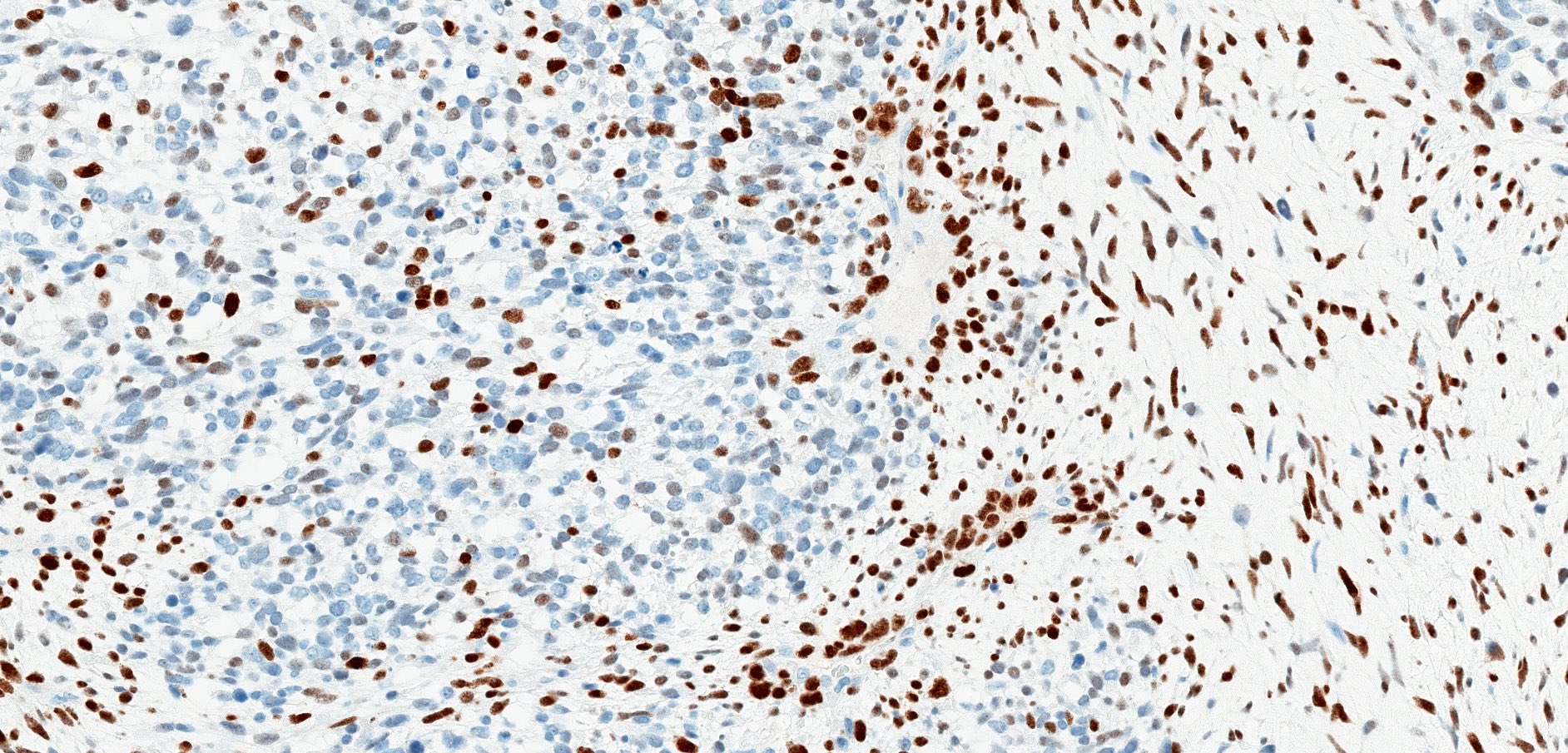
STAT6 loss
Myogenin
Contributed by Borislav A. Alexiev, M.D. (Case #505)
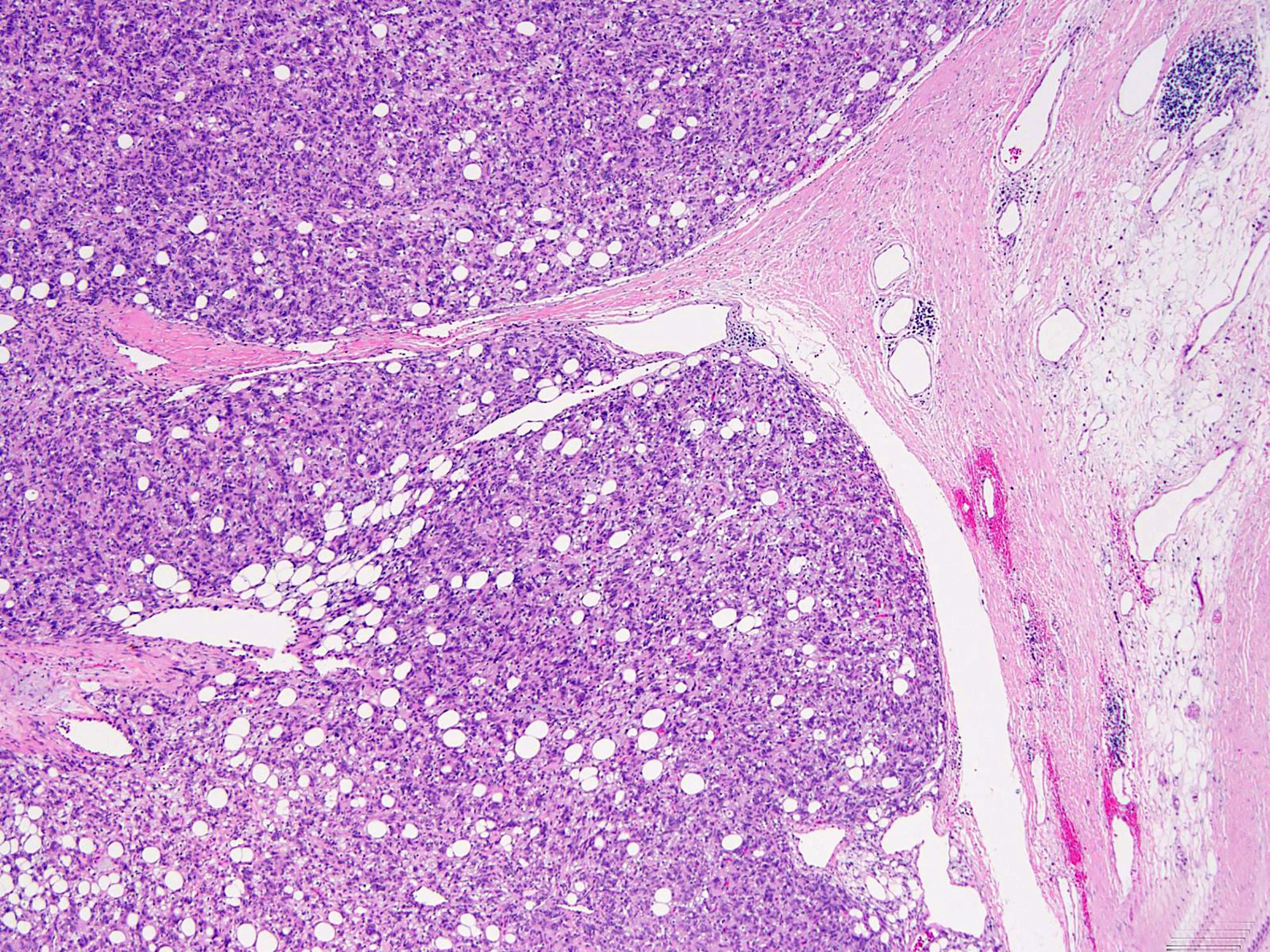

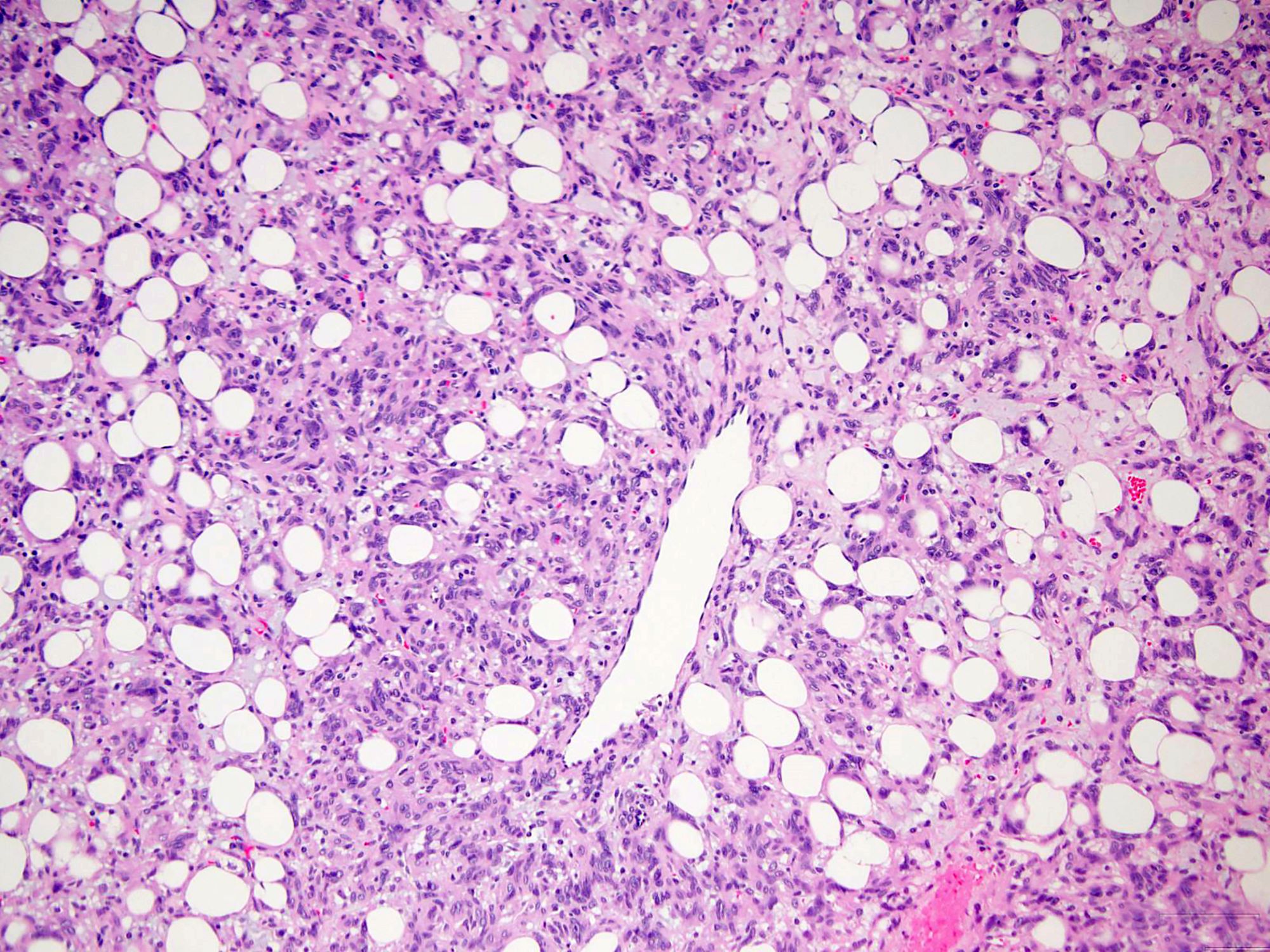
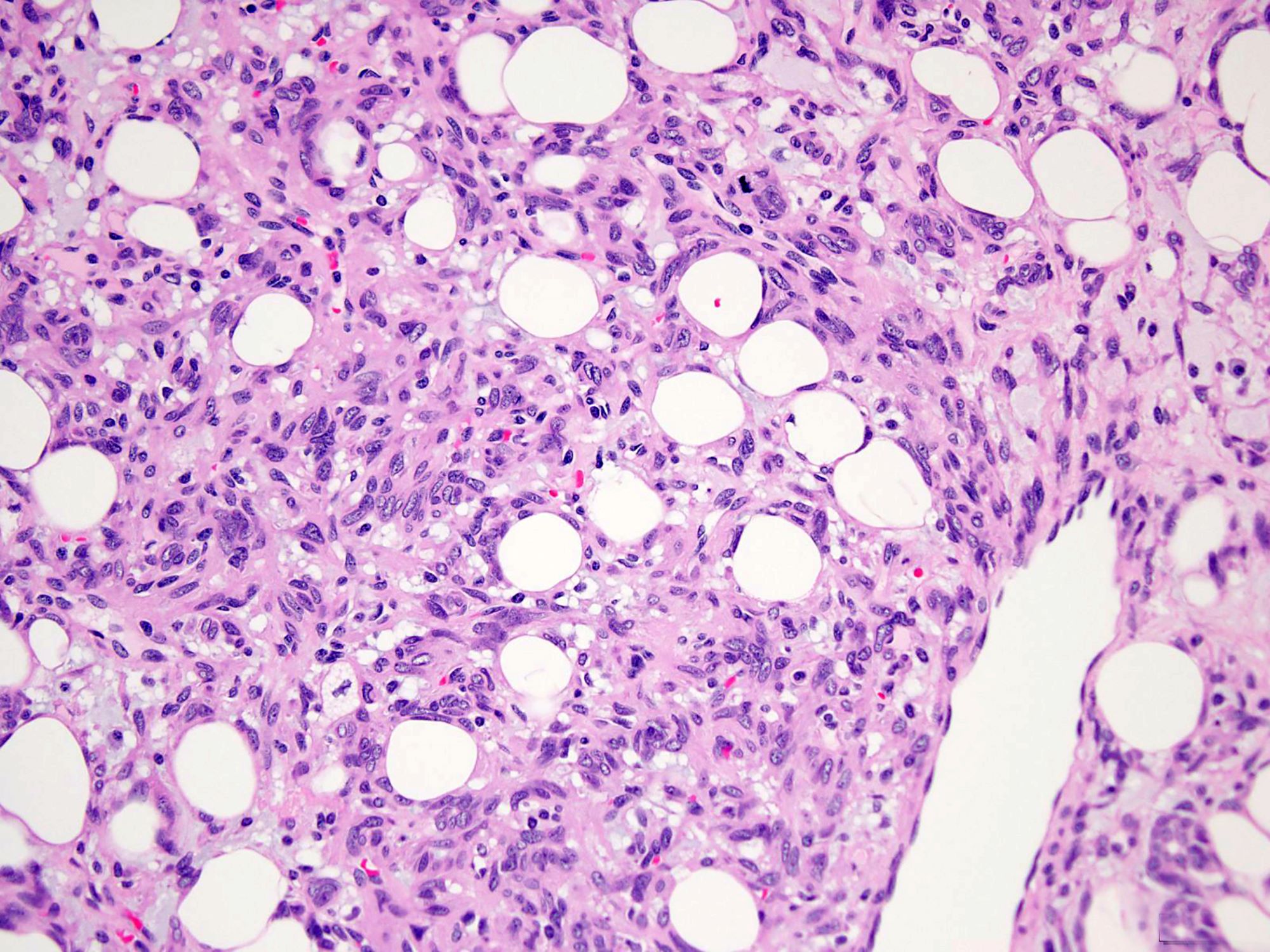
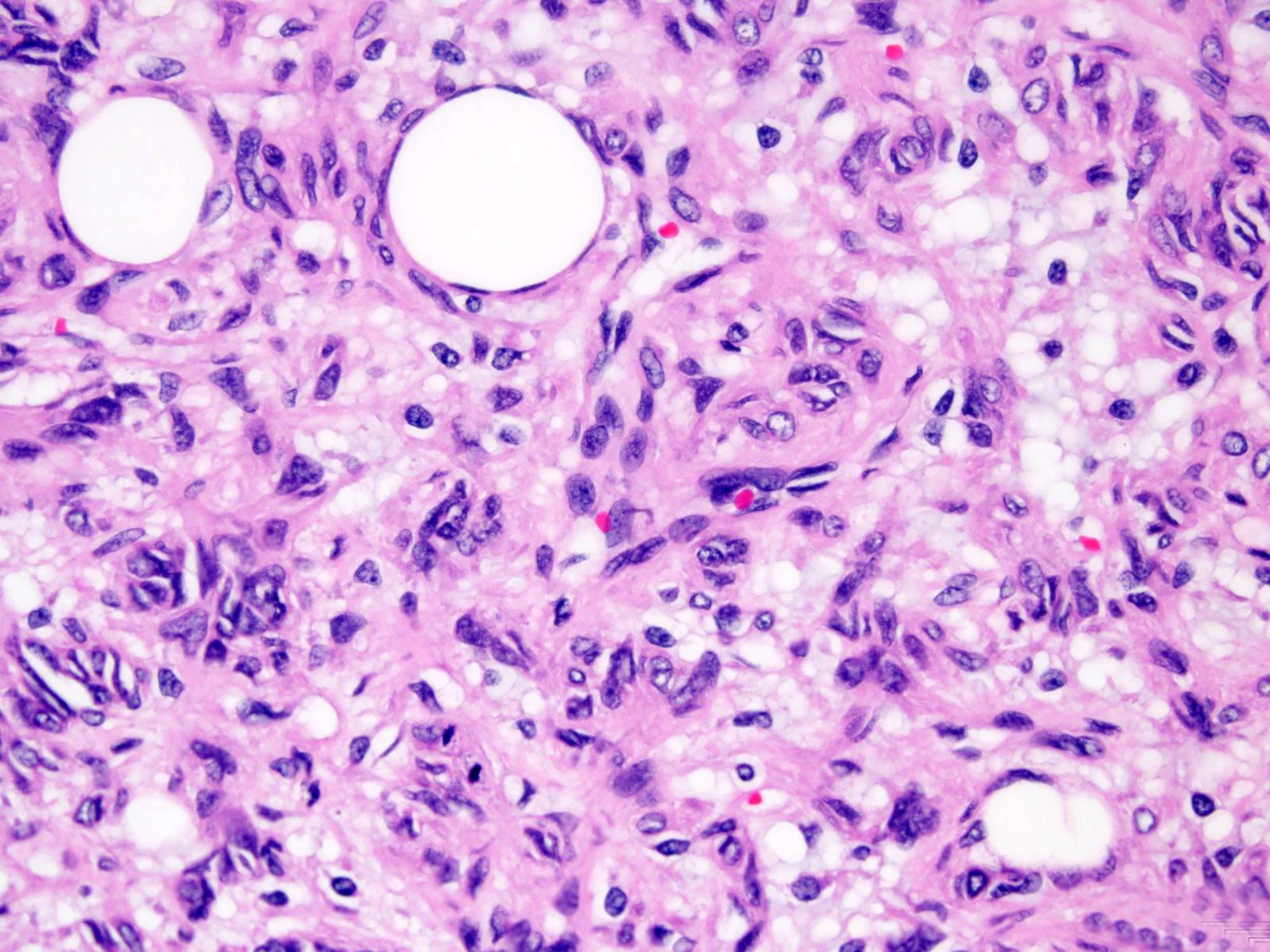
Fat forming SFT
Virtual slides
Images hosted on other servers:

Solitary fibrous tumor
Cytology description
- Low to moderate cellularity
- Oval, elongate, rounded or stellate cells with wispy cytoplasm and pink collagenous stroma (Cancer Cytopathol 2018;126:36)
- High cellularity and nuclear pleomorphism in malignant cases
Cytology images
Images hosted on other servers:

Diff-Quik, fine needle aspiration

Pap, touch prep
Positive stains
- CD34: diffuse to focal but nonspecific, present in 85 - 95% of cases, may be lost in malignant or dedifferentiated cases (Am J Surg Pathol 2012;36:1202, Am J Surg Pathol 2009;33:1314)
- STAT6 (nuclear): highly sensitive and specific marker (close to 100%) but could be lost in dedifferentiated cases (Mod Pathol 2014;27:390, Acta Neuropathol 2013;125:651, Mod Pathol 2015;28:1074, Int J Surg Pathol 2017;25:58)
- May have focal EMA (30%) and actin (20%) (Hum Pathol 1998;29:636)
- BCL2 (30%) and CD99 (70%): nonspecific and not diagnostically useful
Negative stains
Electron microscopy description
- Fibroblast-like cells with well developed rough endoplasmic reticulum and surrounded by collagen fibers (Med Mol Morphol 2009;42:239)
Molecular / cytogenetics description
- NAB2-STAT6 gene fusion best detected by multiplexed massively parallel sequencing assays (Nat Genet 2013;45:131, Nat Genet 2013;45:180)
- Detection of gene fusion difficult by conventional cytogenetic methods due to close proximity of NAB2 and STAT6 on chromosome 12q
- Diverse fusion variants makes PCR based detection methods difficult
- NAB2 exon 4 STAT6 exon 2 / 4: most common genotype, associated with thoracic location and older age (Hum Pathol 2015;46:347, Mod Pathol 2015;28:1324, Cancer Med 2016;5:159)
- NAB2 exon 6 STAT6 exon 16 / 18: associated with extrapleural location and aggressive phenotype (Hum Pathol 2015;46:347, Mod Pathol 2015;28:1324)
Molecular / cytogenetics images
Images hosted on other servers:

Capillary sequencing and RT PCR
Videos
Solitary fibrous tumor
Sample pathology report
- Soft tissue, pelvis, excision:
- Solitary fibrous tumor (5.6 cm), completely excised (see comment)
- Comment: Histologic sections demonstrate a moderately cellular spindled cell tumor in a collagenous stroma with prominent dilated staghorn type vasculature. Mitotic rate is approximately 1 - 2 per 10 high power fields. Overt cytologic atypia and tumor necrosis are not identified. Immunohistochemical studies show that the tumor cells are diffusely and strongly positive for CD34 and STAT6 and are negative for SOX10, S100 and AE1 / AE3, supporting the above diagnosis. According to the 2017 risk stratification criteria by Demicco et al, this should be classified as a low risk solitary fibrous tumor.
Differential diagnosis
- Synovial sarcoma:
- Mesenchymal chondrosarcoma:
- Frequently exhibits hemangiopericytoma-like vasculature
- Islands of well differentiated cartilage
- Negative for STAT6
- HEY1-NCOA2 gene fusions
- Deep fibrous histiocytoma:
- Polymorphous spindled cells arranged in short fascicles and storiform pattern
- Peripheral collagen trapping
- Negative for STAT6
- Mammary type myofibroblastoma:
- Myopericytoma:
- Bland ovoid to spindled cells growing concentrically around small vessels
- Hemangiopericytoma-like blood vessels may be present
- Strong and diffuse expression for smooth muscle actin
- Negative for STAT6
- Dermatofibrosarcoma protuberans:
- Gastrointestinal stromal tumor:
- Wide histologic spectrum
- Arise from anywhere in the gastrointestinal tract
- Usually CD34 positive
- Negative for STAT6
- Majority positive for DOG1 and CD117 (c-KIT)
- Well differentiated or dedifferentiated liposarcoma:
- Lipomatous solitary fibrous tumor can be mistaken for well differentiated or dedifferentiated liposarcoma
- Rare cases of dedifferentiated liposarcoma may show weak expression of STAT6 (Mod Pathol 2014;27:390)
- MDM2 gene amplification by FISH
Additional references
Board review style question #1
A 54 year old woman presents with a 9.6 cm, well circumscribed, firm mass in the deep soft tissue of the thigh. Histologic sections show ovoid to spindled cells arranged haphazardly around prominent thin walled, hyalinized, dilated staghorn type vasculature (see image above). Which of the following is the most sensitive and specific immunohistochemical marker for the diagnosis of this tumor?
- Actin
- BCL2
- CD34
- Cytokeratin CAM 5.2
- STAT6
Board review style answer #1
Board review style question #2
Which of the following is a favorable prognostic factor for solitary fibrous tumor?
- Age < 55 years old
- Mitotic rate ≥ 4 per 10 high power fields
- TERT promoter mutations
- Tumor necrosis
- Tumor size ≥ 10 cm
Board review style answer #2
Board review style question #3
Which of the following is true about the majority of fat forming solitary fibrous tumor cases?
- All tumors show reactivity for CD34
- Fat forming solitary fibrous tumors usually occur in younger adults, predominantly in females
- Multivacuolated lipoblasts are more common in the malignant subset
- The imaging findings of fat forming solitary fibrous tumor are specific
- The mediastinum is the most commonly affected site
Board review style answer #3
C. Multivacuolated lipoblasts are more common in the malignant subset
Comment Here
Reference: Soft tissue - Solitary fibrous tumor
Comment Here
Reference: Soft tissue - Solitary fibrous tumor
