

Skin nonmelanocytic tumor
Cysts
Proliferating pilar tumor
Editorial Board Member: Jonathan D. Ho, M.B.B.S., D.Sc.


Last author update: 24 August 2022
Last staff update: 24 August 2022
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Proliferating pilar tumor
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Beatty CJ, Kazlouskaya V. Proliferating pilar tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumornonmelanocyticpilartumor.html. Accessed April 19th, 2024.
Definition / general
- Proliferating pilar tumor (PPT) is an uncommon neoplasm within the dermis or subcutis that arises from the isthmus region of the outer root sheath of the hair follicle
- Generally develops from a pilar cyst (sometimes following trauma) but may also arise de novo
Essential features
- Most commonly arises on the scalp of elderly women
- Histologically resembles a trichilemmal cyst but with central lobules of squamous proliferation and variable atypia and mitotic figures
- Complete excision and clinical follow up is recommended due to the small risk for recurrence and metastasis
Terminology
- Proliferating pilar cyst
- Proliferating trichilemmal cyst
Epidemiology
- Elderly women are most commonly affected (80% of cases arise in females) (Am J Clin Pathol 2004;122:566)
Sites
- Scalp (85%), less commonly on the trunk (Am J Clin Pathol 2004;122:566)
Pathophysiology
- Proliferating pilar tumors are believed to arise from pilar cysts; however, it remains unknown what triggers the proliferative activity (Dermatol Surg 2007;33:1102)
- Trauma and inflammation have been suggested as the triggers in some cases (J Dermatol Surg Oncol 1987;13:1339)
Etiology
- Genetic basis of hereditary pilar cysts has been reported as mutations in PLCD1; it is not known whether proliferating pilar tumors share this genetic alteration (Sci Rep 2020;10:6035)
Clinical features
- Slowly growing nodule on the scalp
- Lesions are generally well circumscribed, although they may be multinodular
- Tend to shell out from surrounding tissue upon surgical excision, similar to pilar cysts
- Average size is several centimeters; however, tumors up to 25 cm have been reported (Cancer 1971;28:701)
Diagnosis
- Based on histopathologic findings following skin biopsy or excision of the nodule
Prognostic factors
- Nonscalp location, recent rapid growth, size > 5 cm and histologic features of extensive necrosis, high mitotic activity, poor circumscription with areas of invasion and cytologic atypia are all concerning for more aggressive or malignant behavior (J Cutan Pathol 2003;30:492)
- Local recurrence rate is 6.6%; risk of lymph node involvement is 2.6% (Am J Clin Pathol 2004;122:566)
Case reports
- 33 year old woman with multiple proliferating pilar tumors and a porokeratotic adnexal ostial nevus (JAAD Case Rep 2020;6:344)
- 46 and 54 year old women with proliferating pilar tumors treated with Mohs micrographic surgery (J Drugs Dermatol 2021;20:1346)
- 76 year old woman with a proliferating trichilemmal cyst with delayed treatment due to COVID outbreak (Front Surg 2021;8:680160)
Treatment
- Complete surgical excision, either via wide local excision or Mohs micrographic surgery (Dermatol Surg 2007;33:1102)
- If the lesion was enucleated in its entirety, well circumscribed and without other concerning histologic features, additional surgical therapy is not required
- Ongoing surveillance to monitor for recurrence or metastasis is recommended
Clinical images
Contributed by Viktoryia Kazlouskaya, M.D., Ph.D.

Large cystic lesion
Gross description
- Encapsulated, pearly white nodule; may be multinodular
Microscopic (histologic) description
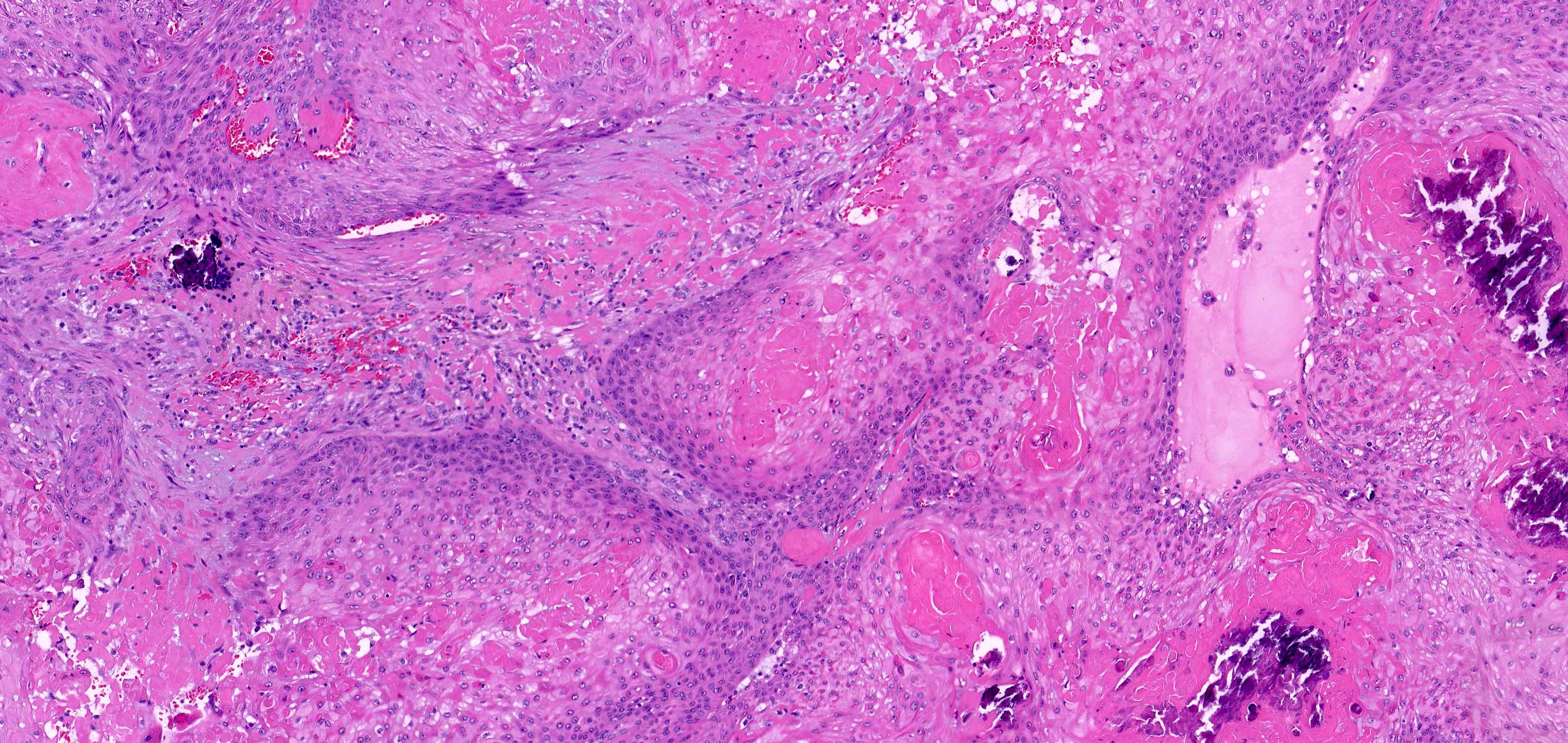
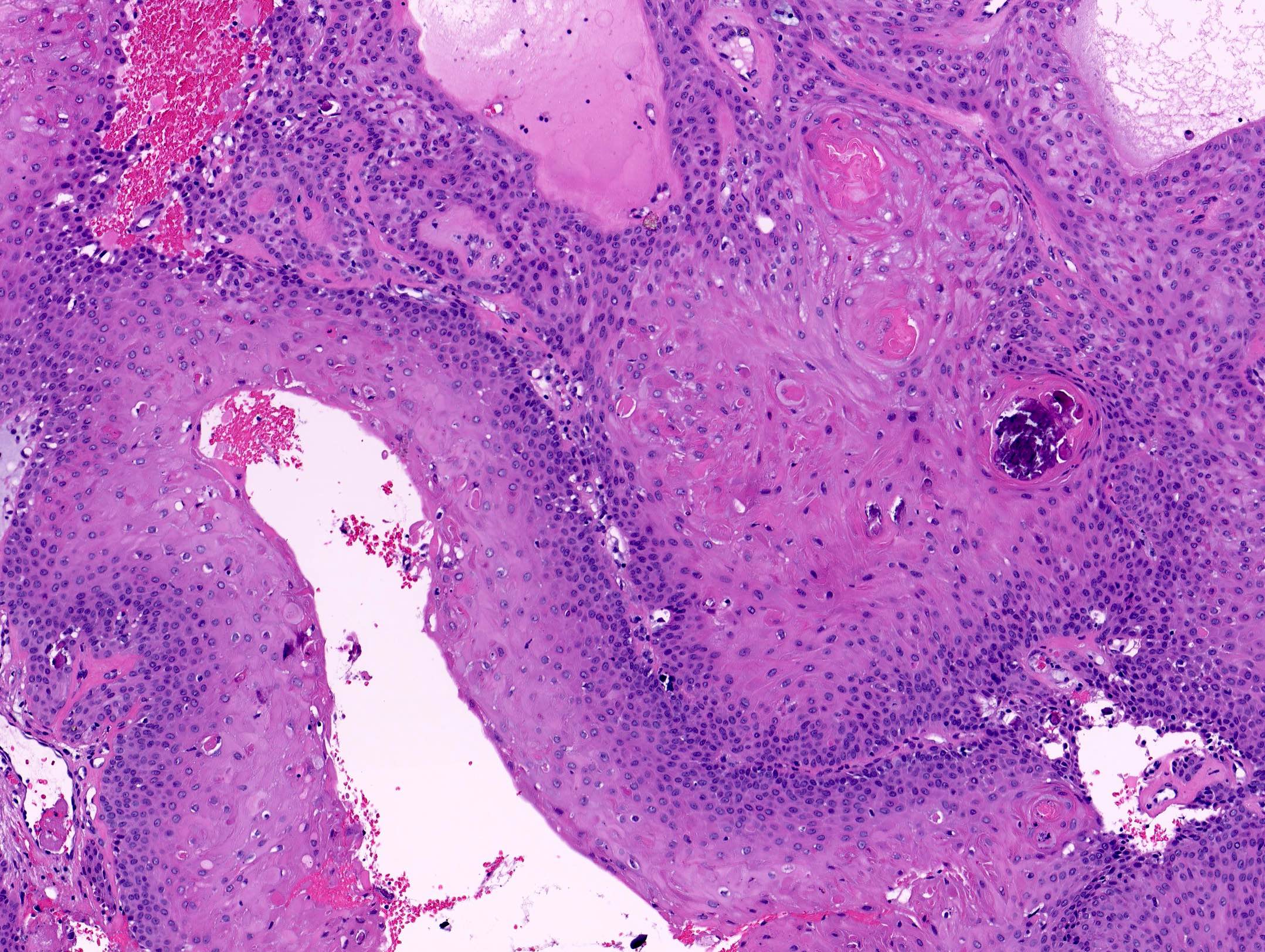
- Features of a pilar cyst with abrupt trichilemmal keratinization with additional extensive epithelial proliferation within the center of the cystic space
- Mitotic activity and cytologic atypia may be variable
- Invasion into the surrounding soft tissue should not be present
- Grading criteria as suggested by Ye et al. stratifies proliferating pilar tumors into 3 groups based on histologic characteristics (Am J Clin Pathol 2004;122:566):
- Group 1:
- Circumscribed silhouettes with pushing margins, modest nuclear atypia and an absence of pathologic mitoses, necrosis and invasion of nerves or vessels
- Behaves in a benign manner
- Group 2:
- Similar to group 1 but manifest irregular, locally invasive silhouettes with involvement of the deep dermis and subcutis
- Small risk of local recurrence
- Group 3:
- Invasive growth patterns, marked nuclear atypia, pathologic mitotic forms and geographic necrosis, with or without the involvement of nerves or vascular structures
- Potential for regional recurrence and metastasis
- Group 1:
Microscopic (histologic) images
Contributed by Viktoryia Kazlouskaya, M.D., Ph.D. and Colleen J. Beatty, M.D.
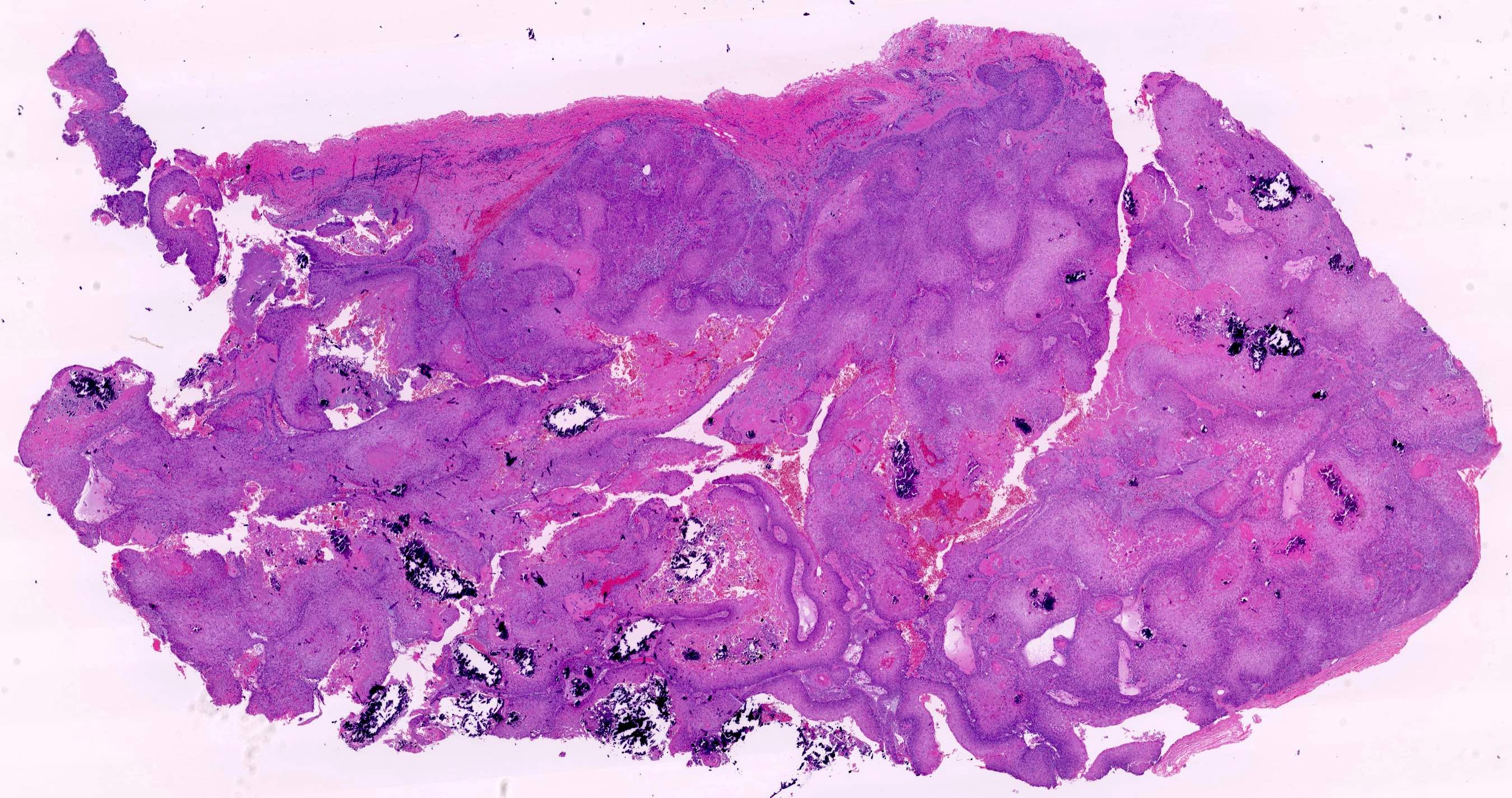
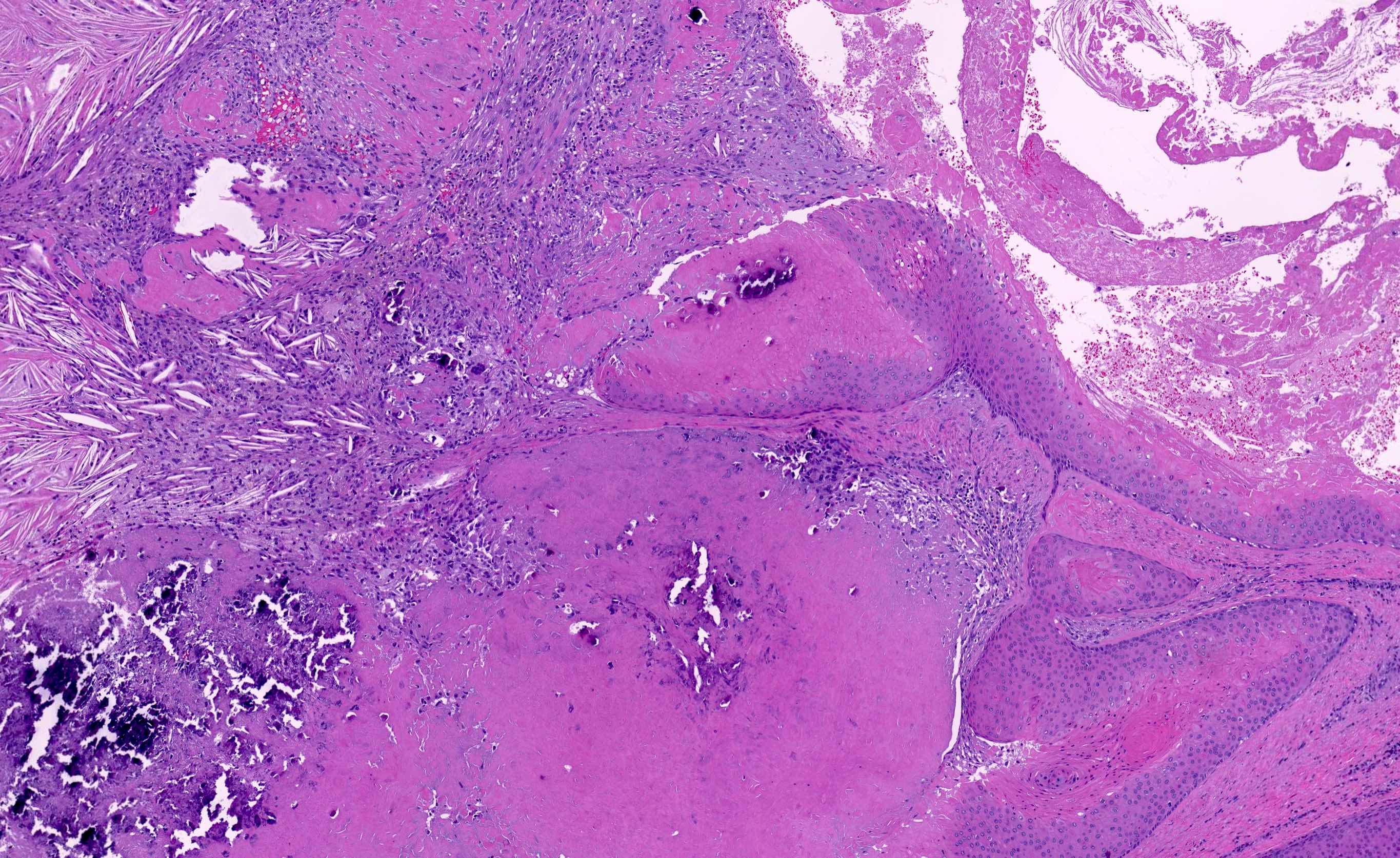
Lesion with trichilemmal differentiation
Proliferating lesion, trichilemmal differentiation
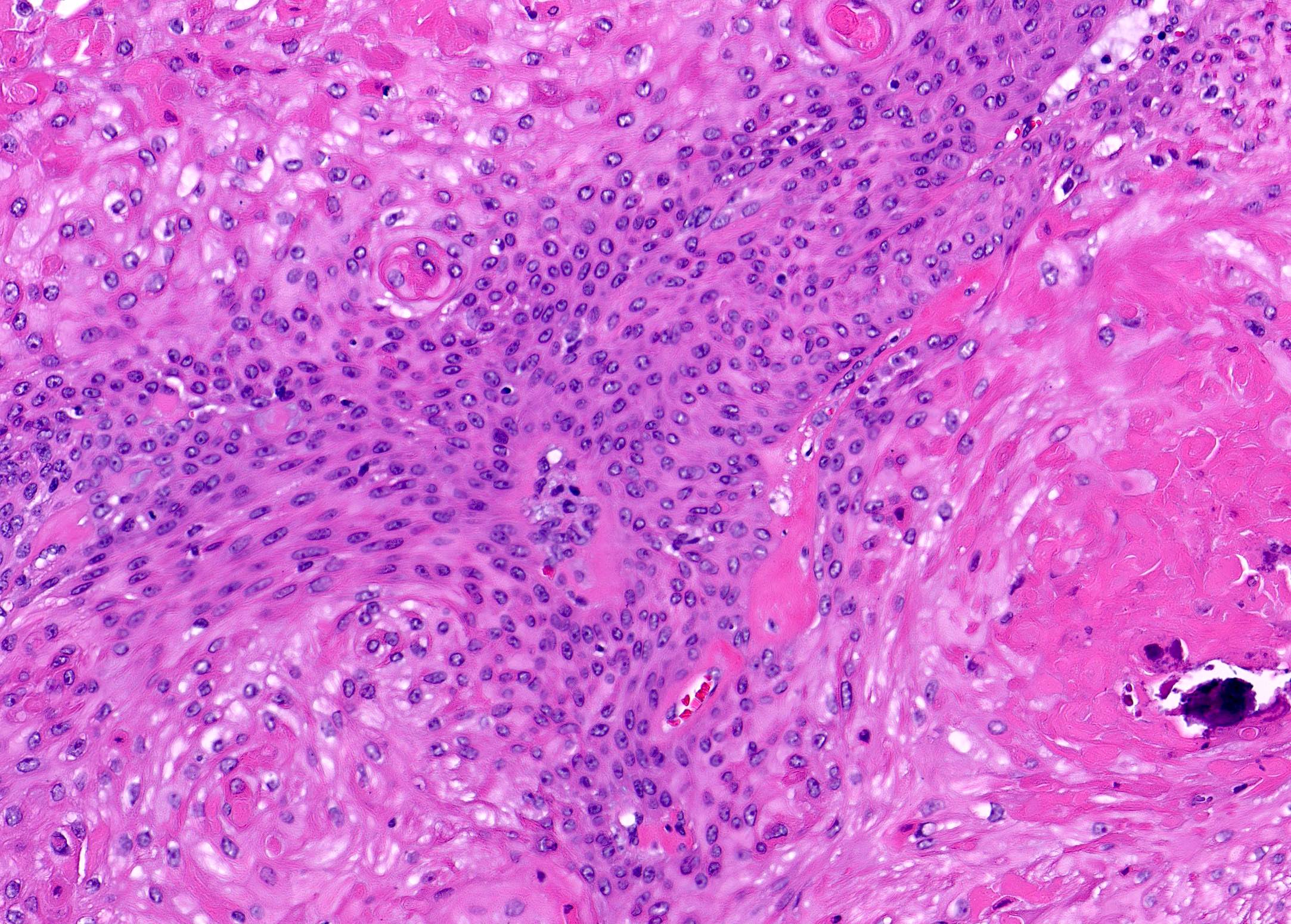
Trichilemmal differentiation without atypia

Proliferative cystic lesion
Proliferative trichilemmal lesion
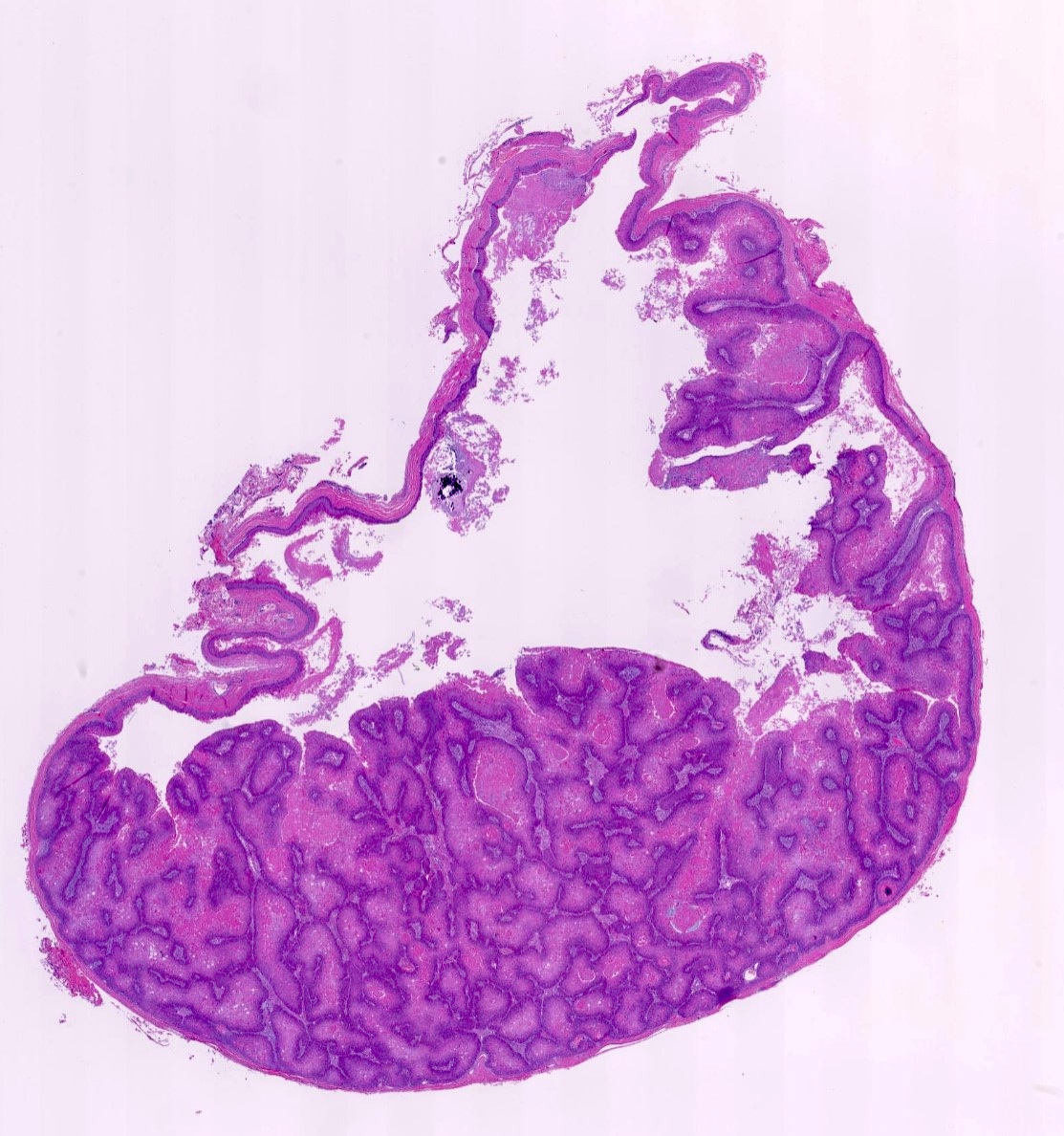
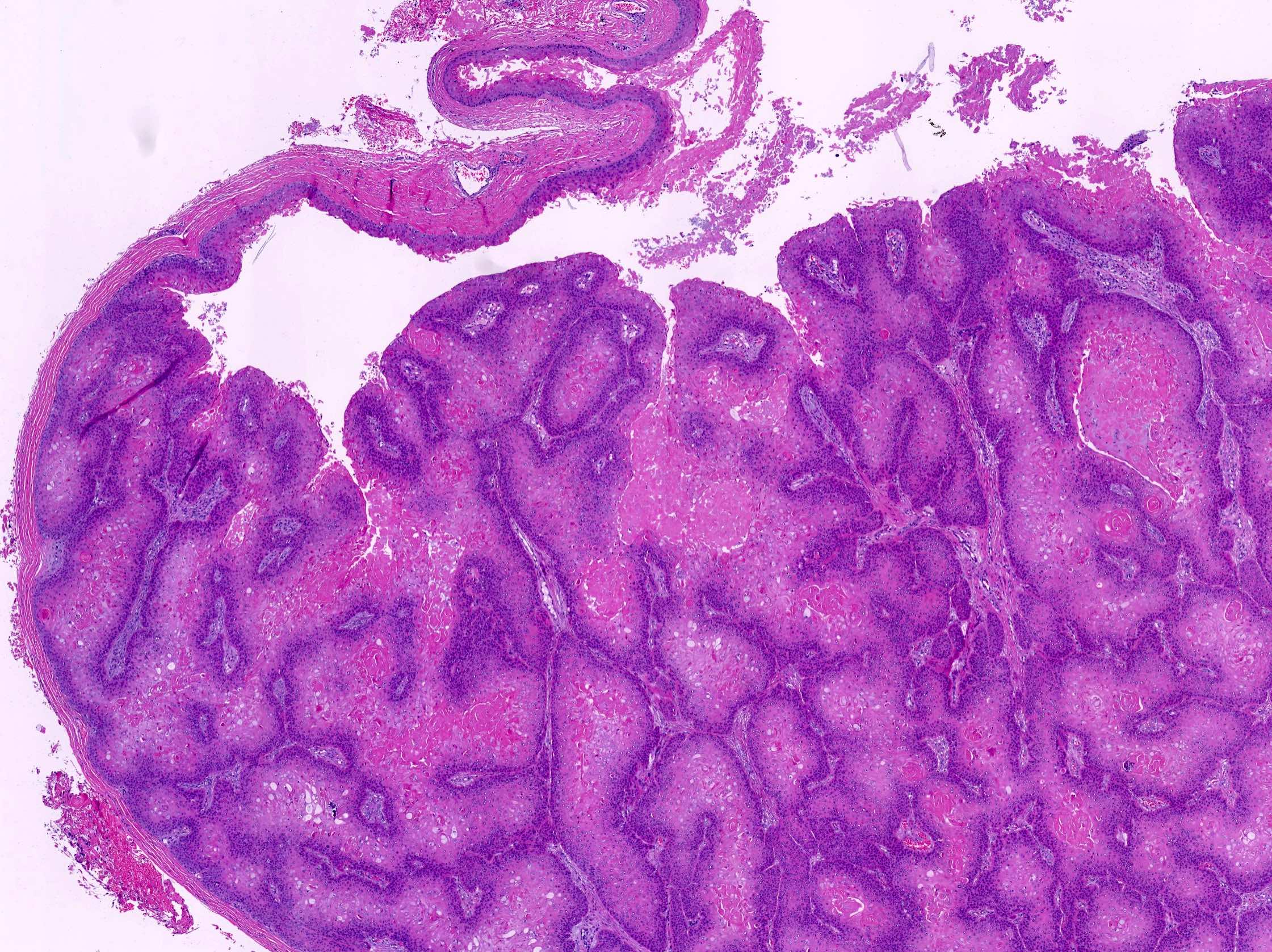
Cyst with proliferative areas
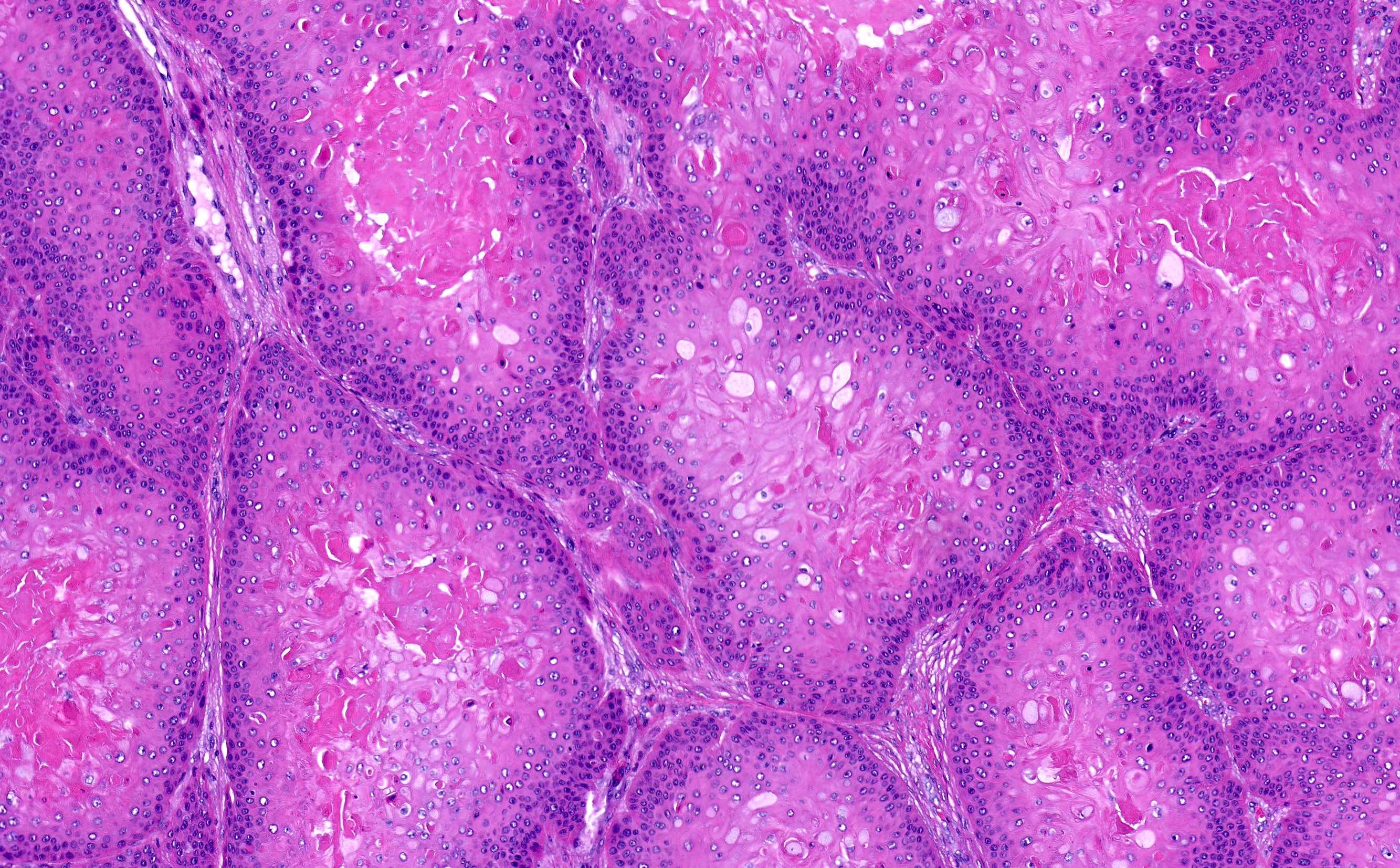
Proliferative area with trichilemmal differentiation
Videos
Proliferating pilar tumor overview by Dr. Gardner
Sample pathology report
- Skin, scalp, biopsy:
- Proliferating pilar tumor (see comment)
- Comment: Examination reveals a well circumscribed nodule composed of lobules of proliferative squamous epithelium showing trichilemmal keratinization with an adjacent typical pilar cyst. No significant cytologic atypia or atypical mitoses are observed. The lesion appears to be excised in total; however, clinical correlation and follow up are recommended.
Differential diagnosis
- Pilar (trichilemmal) cyst:
- Well circumscribed cyst lined by stratified squamous epithelium exhibiting trichilemmal keratinization
- Squamous cell carcinoma:
- Malignancy of epidermal keratinocytes exhibiting invasion and variable degrees of atypia
- Key differentiators are absence of areas of trichilemmal keratinization and a lack of staining with markers of outer root sheath differentiation
- Malignant proliferating pilar tumor:
- Features of a proliferating pilar tumor but with invasion into the surrounding tissue along with atypical mitoses, marked nuclear atypia and geographic necrosis
Board review style question #1
Proliferating pilar tumors are thought to arise from pilar cysts, potentially incited by trauma to a pre-existing pilar cyst. What is a histologic hallmark of a proliferating pilar tumor?
- Cyst with eosinophilic cuticle and associated sebaceous glands
- Cystic lining with granular layer and keratinization
- Lobules of squamous epithelium arising within a cyst with trichilemmal keratinization
- Proliferation of hair matrical cells and ghost cells
Board review style answer #1
C. Lobules of squamous epithelium arising within a cyst with trichilemmal keratinization
Comment Here
Reference: Proliferating pilar tumor
Comment Here
Reference: Proliferating pilar tumor
Board review style question #2
The following lesion is found on the scalp of an elderly woman. What is the diagnosis?
- Pilomatricoma
- Proliferating pilar cyst
- Squamous cell carcinoma
- Steatocystoma
Board review style answer #2
