

Skin nonmelanocytic tumor
Adnexal tumors
Sweat gland derived (apocrine & eccrine glands)
Poroma
Authors: Aayushma Regmi, M.B.B.S., Jodi Speiser, M.D.
Resident / Fellow Advisory Board: Farres Obeidin, M.D.


Last author update: 23 December 2021
Last staff update: 24 January 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Poroma

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Regmi A, Speiser J. Poroma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skintumornonmelanocyticeccrineporoma.html. Accessed December 20th, 2024.
Definition / general
- Benign glandular adnexal tumor that usually originates from cells of the outer layer of the acrosyringium and terminal eccrine duct
- Has both eccrine and apocrine origin (AMA Arch Derm 1956;74:511)
- Malignant counterpart is referred to as porocarcinoma
Essential features
- Single, slow growing, asymptomatic, well circumscribed, smooth, skin colored to red, slightly scaly papule or nodule
- Most commonly on palms and sole or sides of the foot
- Well circumscribed broad anastomosing bands of poroma cells with sharp demarcation from adjacent keratinocytes
- Excellent prognosis with simple excision
Terminology
- Eccrine poroma / hidroacanthoma simplex / dermal duct tumor, apocrine poroma
ICD coding
- ICD-10: D23.9 - other benign neoplasm of skin, unspecified
Epidemiology
- M = F (Arch Craniofac Surg 2017;18:44)
- Most commonly affects adults (Ann Dermatol 2011;23:250)
- Presentation in childhood and congenital onset are unusual (J Eur Acad Dermatol Venereol 2008;22:366)
- Eccrine porocarcinoma:
- Also known as malignant eccrine poroma
- Develops after several years from a pre-existing poroma
- Most commonly affects elderly, with F > M
- Tumors are often ulcerated and many bleed on trauma
Sites
- Most commonly on palms and sole or sides of the foot (AMA Arch Derm 1956;74:511)
- Occasionally on the head, neck, scalp, chest, abdomen, proximal extremities and the external auditory canal (J Am Acad Dermatol 2001;44:48, Otolaryngol Head Neck Surg 2003;128:439)
Pathophysiology
- Falls under the broad category of poroid neoplasms or acrospiromas
- Poroid neoplasms include the eccrine poroma, apocrine poroma, hidroacanthoma simplex and dermal duct tumor (Clin Exp Dermatol 2014;39:119)
- Eccrine poroma: derived from cells of the outer layer of the acrosyringium and the upper dermal eccrine duct, both epidermal and dermal (AMA Arch Derm 1956;74:511)
- Apocrine poroma: reflects the common embryological ancestry of the 3 units (the folliculosebaceous apocrine unit) (Pathologe 2014;35:456)
Etiology
- Exact etiology is unknown (World J Surg Oncol 2011;9:94)
- No family predilection has been identified for the development of poromas
- Rare cases are associated with radiation therapy or chronic scarring (J Eur Acad Dermatol Venereol 2007;21:1128, Am J Dermatopathol 2013;35:615)
Clinical features
- Asymptomatic, slow growing, solitary, sessile, skin colored to red, slightly scaly nodule, papule or plaque (Int J Dermatol 2014;53:1053)
- Less commonly pigmented or pedunculated (J Dermatol 1990;17:555)
- Occasionally reported with Bowen disease, pregnancy and hypohidrotic ectodermal dysplasia (Ann Dermatol 2018;30:222, Arch Dermatol 1977;113:472)
- Rarely reported as arising within nevus sebaceous (Case Rep Dermatol 2016;8:80)
- Rarely, multiple poromas known as poromatosis can occur following chemotherapy or radiotherapy (Ann Dermatol 2020;32:422)
- Dermoscopic findings: white interlacing areas around vessels, yellow structureless areas, milky red globules, poorly visualized vessels and branched vessels with rounded endings (J Eur Acad Dermatol Venereol 2018;32:1263, Clin Case Rep 2021;9:1601)
Diagnosis
- Clinical appearance confirmed by characteristic histologic findings
Prognostic factors
- Excellent; most cases do not show aggressive behavior
- Rarely progresses to porocarcinoma (World J Surg Oncol 2011;9:94)
- Poromatosis is of cosmetic concern for the patient (Skin Appendage Disord 2015;1:95)
Case reports
- 40 year old woman with an asymptomatic red to brown colored hemorrhagic crusted nodule on the left forearm (Ann Dermatol 2011;23:250)
- 58 year old man had painless, progressive mass below the left temporal eyebrow for 8 years (Indian J Ophthalmol 2020;68:2522)
- 64 year old man with papules near his left nipple and left ankle (Dermatol Online J 2008;14:3)
- 67 year old man initially presented with a nonpainful, exophytic and pigmented lesion on scalp (Am J Case Rep 2019;20:179)
- 70 year old nondiabetic man presented with mass over the medial aspect of his right upper eyelid (Indian J Ophthalmol 2019;67:131)
- 74 year old man with a 4 year history of nodules on the chest and back (An Bras Dermatol 2017;92:550)
Treatment
- No treatment is necessary
- Simple excision with shave or electrosurgical destruction is curative
- Reference: StatPearls: Poroma [Accessed 30 September 2021]
Clinical images
Contributed by Aayushma Regmi, M.B.B.S. and Jodi Speiser, M.D.

Pink, scaly nodule

Erythematous nodule

Pedunculated and pigmented nodule
Gross description
- Solitary, well circumscribed, smooth, pink to red papule, nodule or plaque (Int J Dermatol 2014;53:1053)
Microscopic (histologic) description
- Eccrine poroma:
- Well circumscribed
- Replaces the epidermis and extends into the dermis in broad anastomosing bands
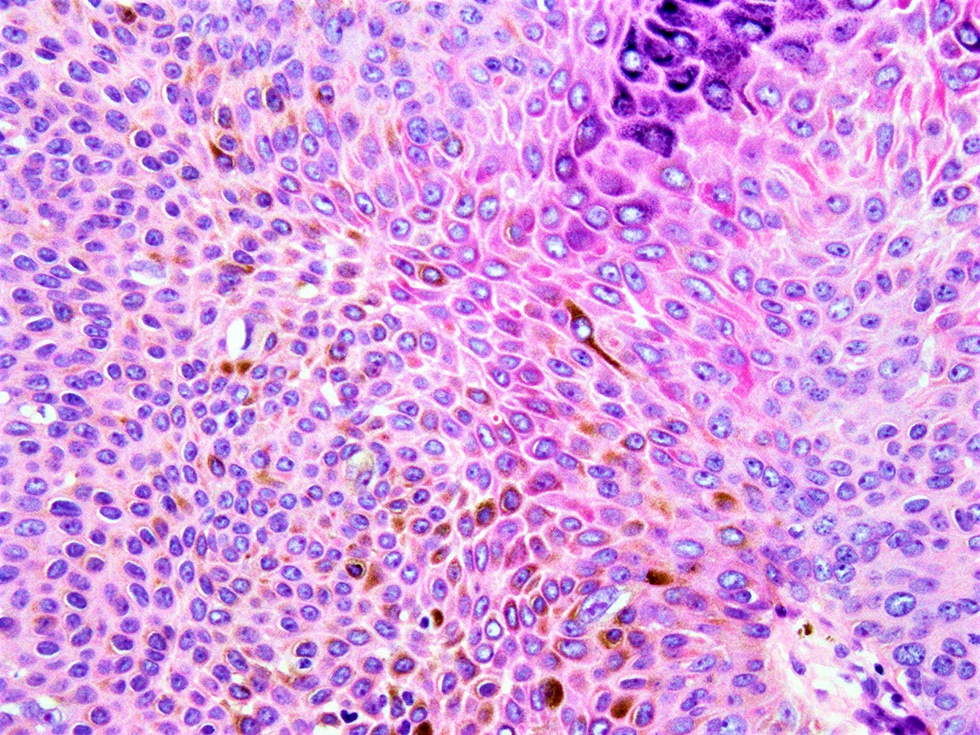
- Poroma cells are monomorphic, small, cuboidal with basophilic round nuclei, inconspicuous nucleoli and compact eosinophilic cytoplasm
- Sharp demarcation present between the normal keratinocytes and poroma cells
- Devoid of peripheral palisading
- Ductal lumina with single row of luminal cells covered by eosinophilic lining or cystic spaces devoid of any formal lining
- Cells are united by conspicuous intercellular bridges and supported by a delicate fibrovascular stroma (J Dermatol 1980;7:263)
- Poroma cells usually contain glycogen (Int J Dermatol 2014;53:1053)
- Occasionally, pigmented variants with associated dendritic melanocytes and tumor cell melanin deposition (J Dermatol 2010;37:542, J Eur Acad Dermatol Venereol 2008;22:303)
- Dystrophic calcification and transepidermal elimination of tumor nests are exceptional findings (J Dermatol Case Rep 2009;3:38, J Dermatol 1997;24:539)
- Apocrine poroma:
- Shows sebaceous differentiation with the occasional presence of follicular differentiation and foci of apocrine-like features (J Cutan Pathol 2001;28:101)
- Anastomosing trabeculae, displaying multiple points of origin from the epidermis and located largely in the papillary and upper reticular dermis
- Cells are small and uniform with scanty cytoplasm and round to oval nuclei united by inconspicuous intercellular bridges
- Foci of ductal differentiation with a well developed eosinophilic cuticle
- Follicular differentiation in the form of epithelial lobules (Am J Dermatopathol 1999;21:31)
- Sebaceous cells, singly and in clusters with bubbly cytoplasm and crenated nuclei is an infrequent feature (Am J Dermatopathol 1996;18:1)
- Eccrine porocarcinoma:
- May remain completely intraepidermal (in situ porocarcinoma) but is more often associated with an invasive dermal component
- Poroma cells, with typical ductal lumina, associated with cytological features of malignancy, including nuclear and cytoplasmic pleomorphism, nuclear hyperchromatism and mitotic activity (Am J Surg Pathol 2001;25:710)
- Prone to have local recurrence (17%) and is occasionally associated with nodal metastases (19%); however, systemic spread is rare (11%) (Am J Surg Pathol 2001;25:710)
Microscopic (histologic) images
Contributed by Aayushma Regmi, M.B.B.S. and Jodi Speiser, M.D.
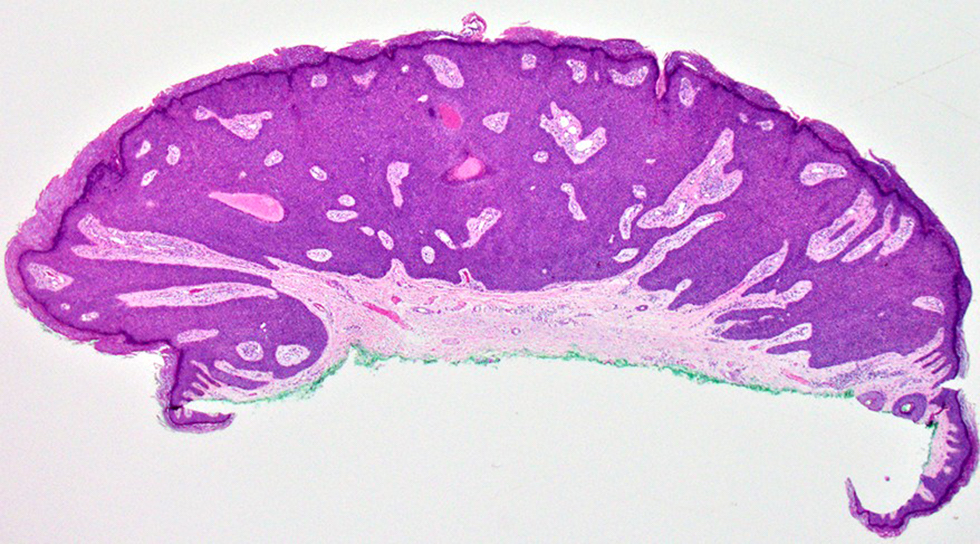
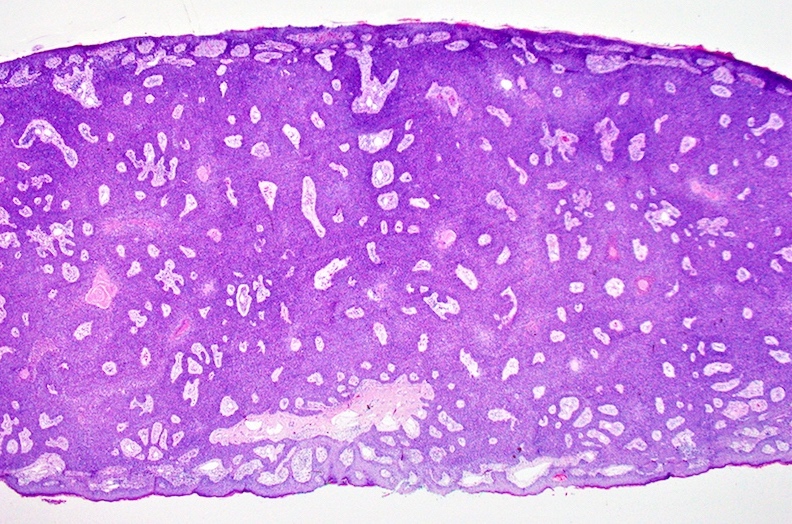
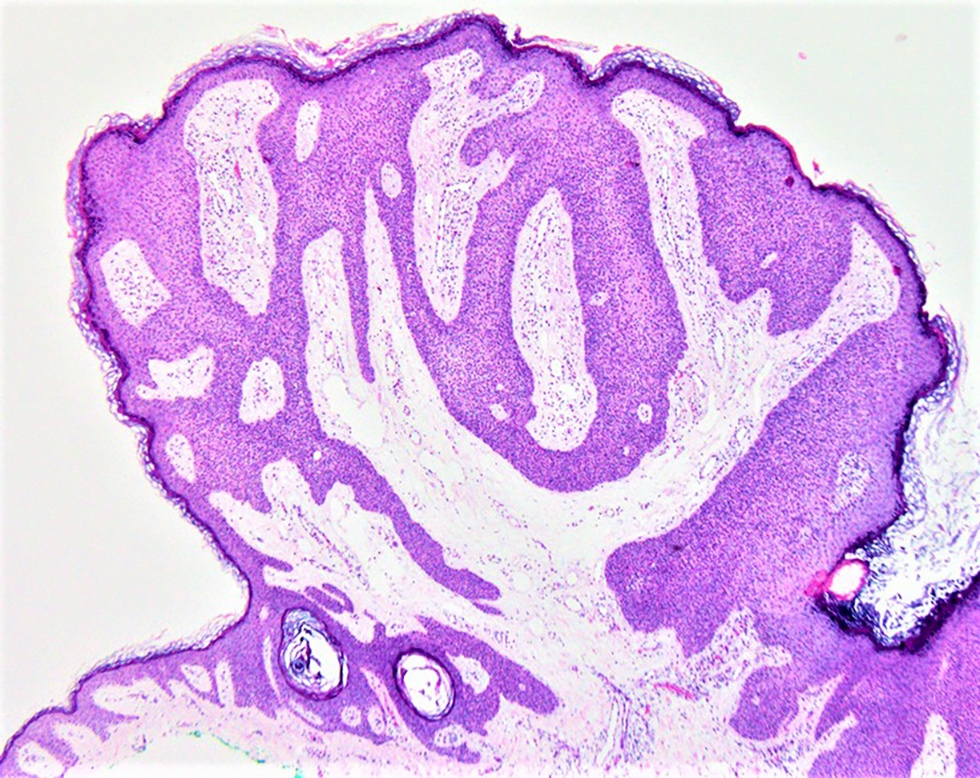
Tumor with epidermal connection
Tumor with epidermal connection
Pedunculated nodule
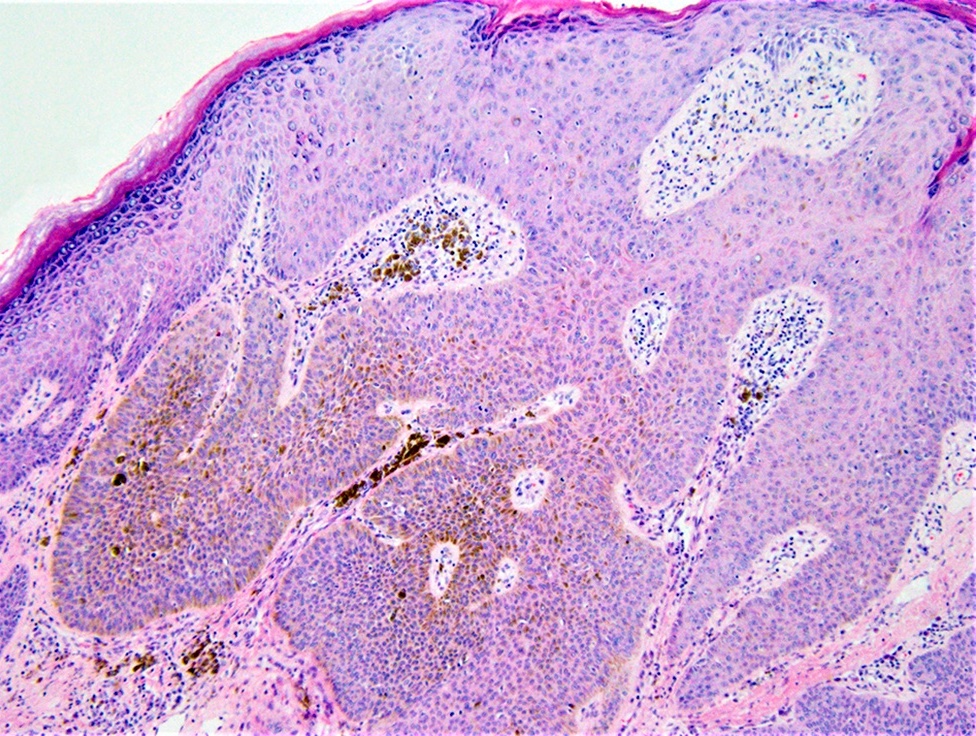
Pigmented poroma
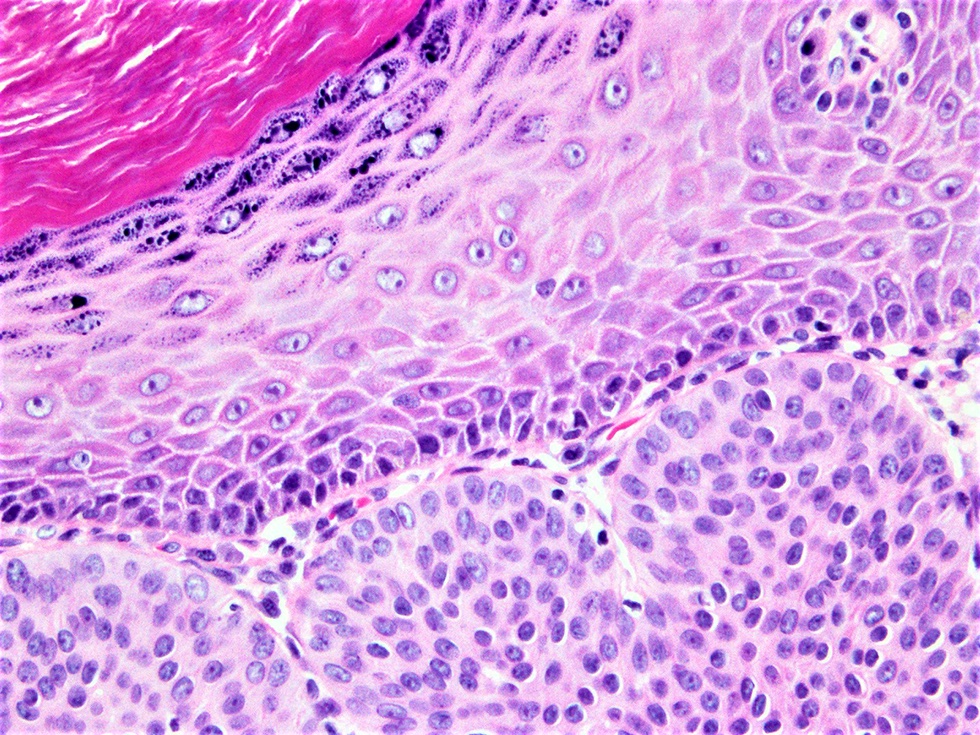
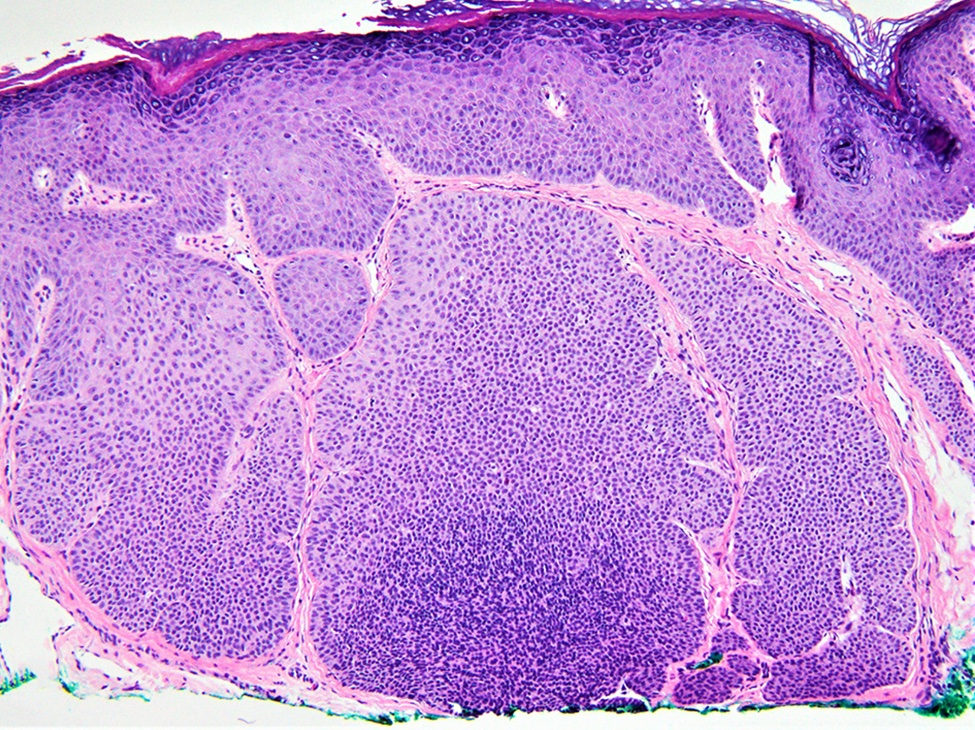
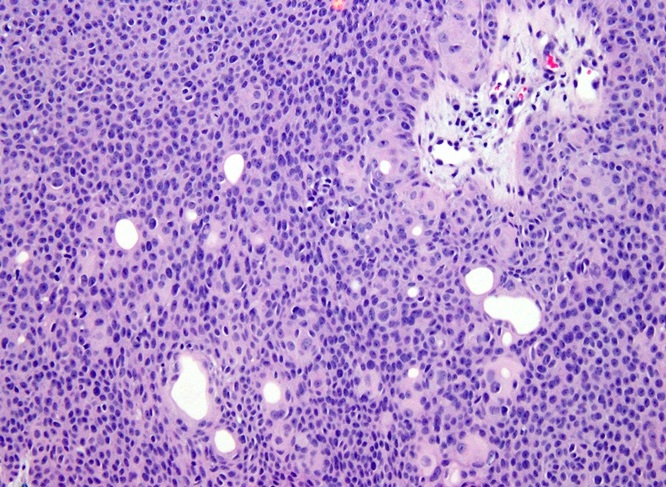
Poroma cells and adjacent keratinocytes
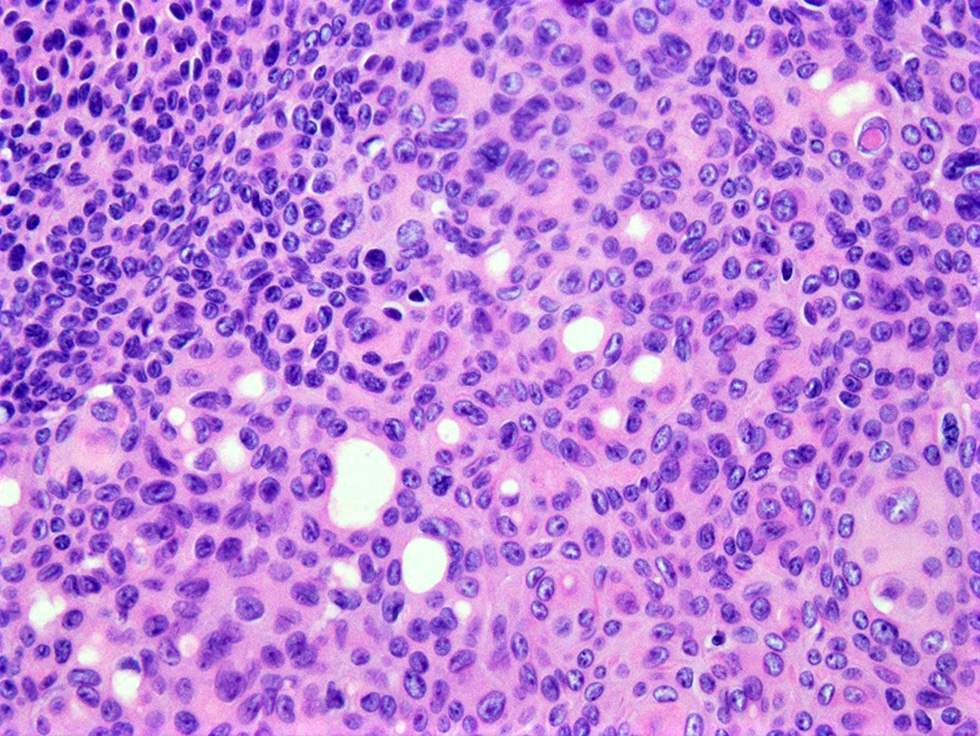
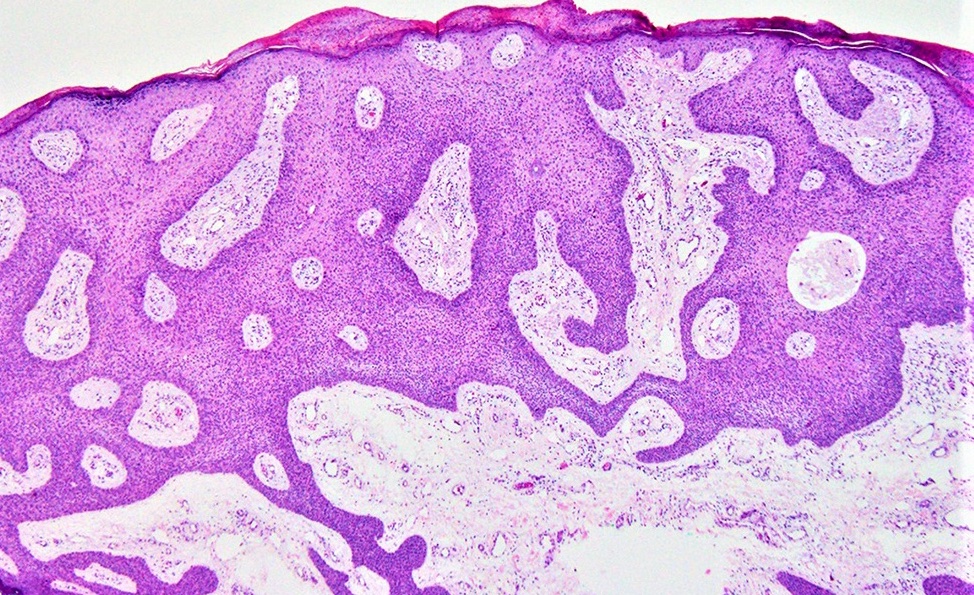
Poroma cells with duct
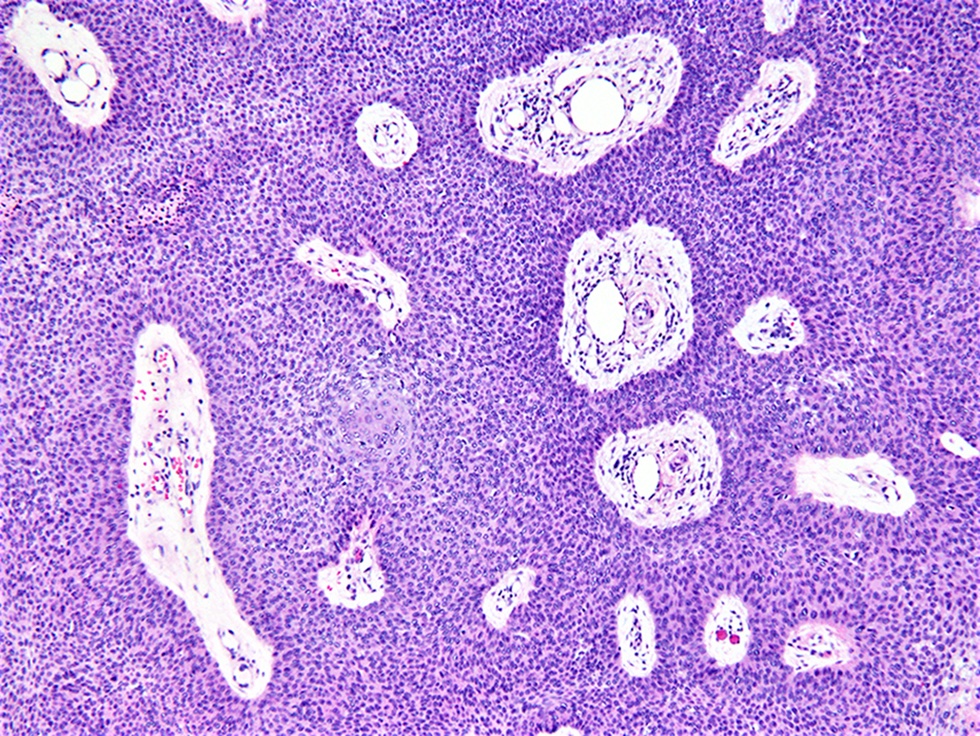
Hyalinized stroma and blood vessels
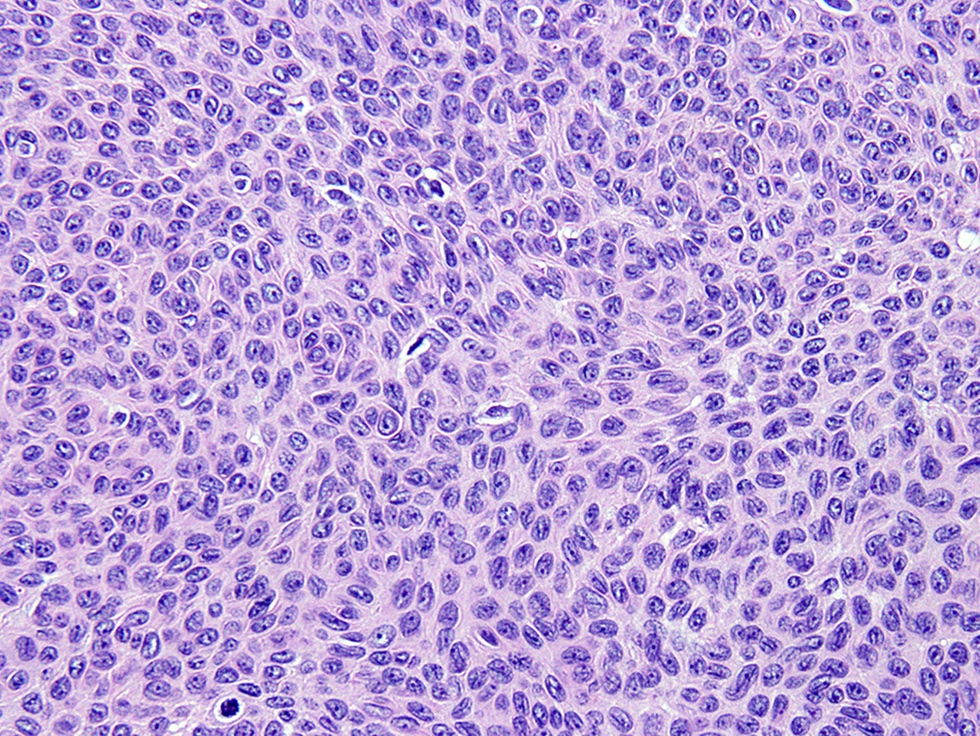
Poroma cells
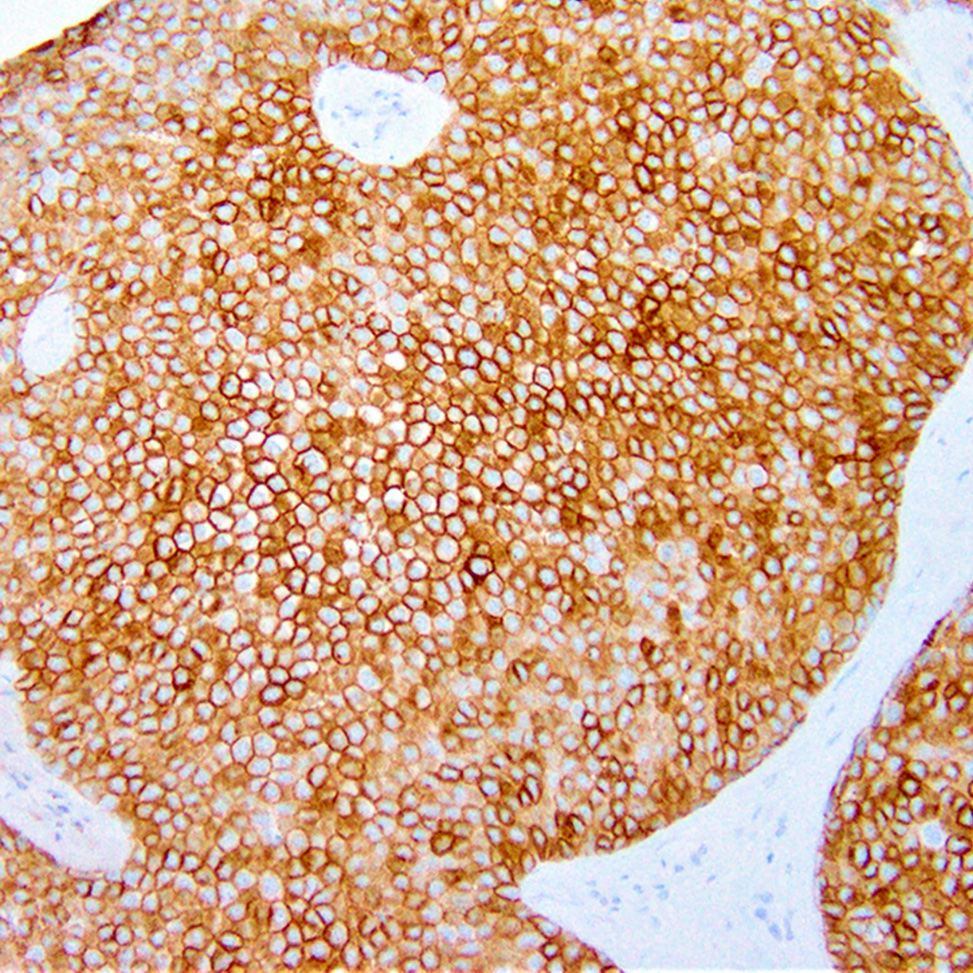
EMA
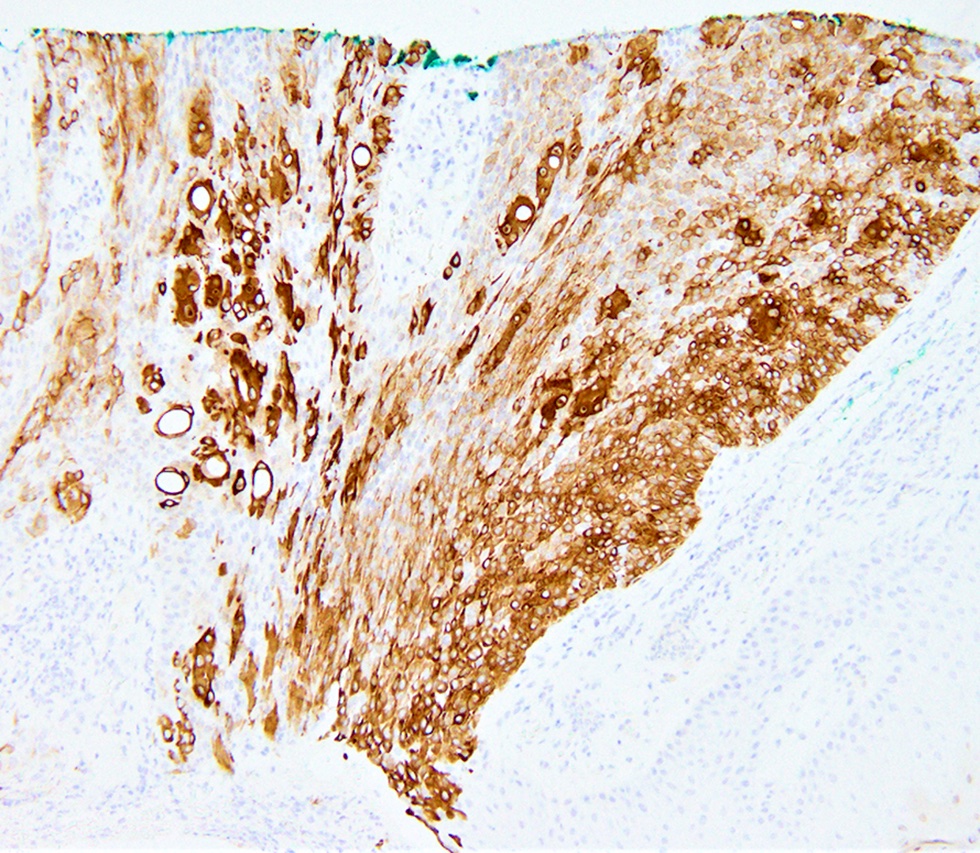
CK7
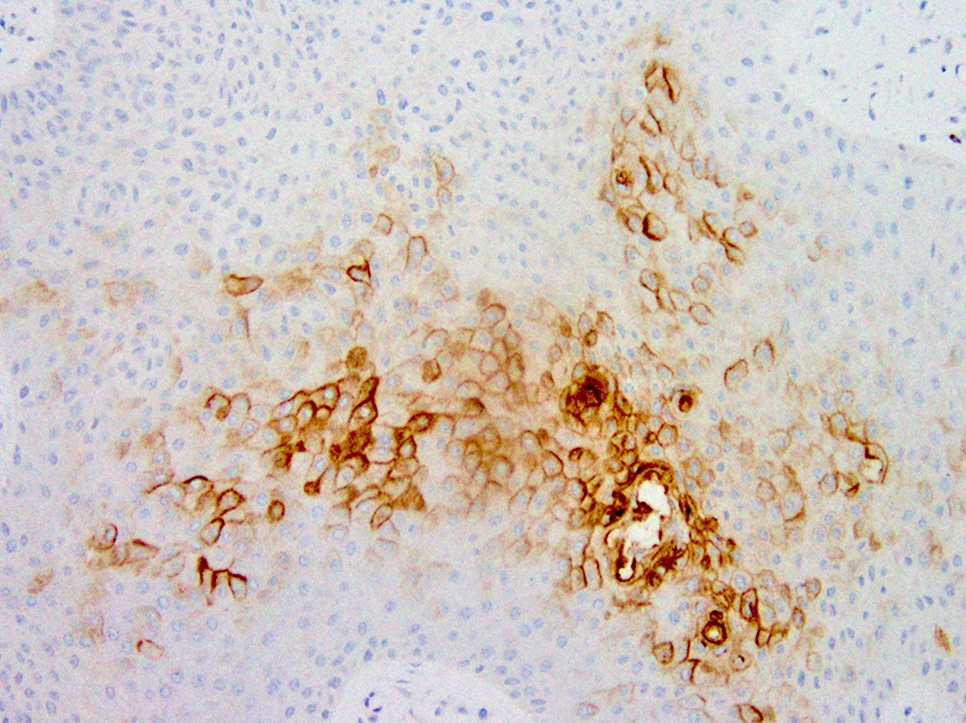
CEA
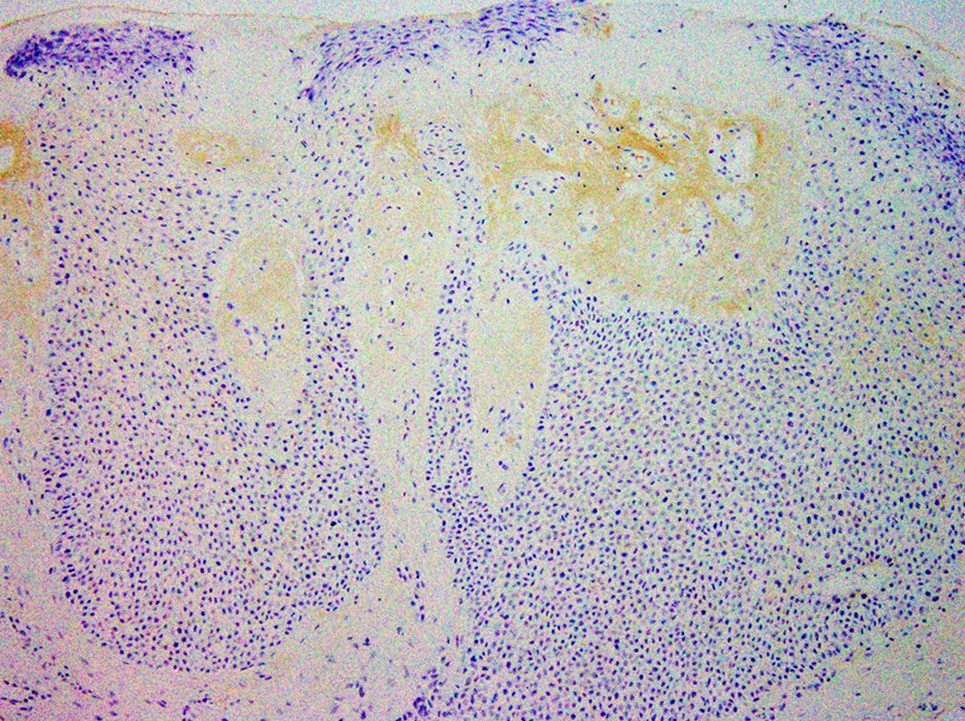
BerEp4
Virtual slides
Images hosted on other servers:

Poroma cells with epidermal connection
Positive stains
- CK5/6, CK7, EMA, CEA, CAM5.2, CD117, diastase PAS (J Cutan Pathol 1999;26:232)
- S100 protein in the diagnoses of recurrent and metastatic dedifferentiated eccrine porocarcinoma (Ann Dermatol 2013;25:348)
Negative stains
- BerEP4, S100 (benign poroma) (Recent Results Cancer Res 1995;139:303)
Electron microscopy description
- Cells have numerous connecting desmosomes, cytoplasmic tonofilaments, glycogen granules and intracytoplasmic lumina (J Dermatol 1980;7:263)
Molecular / cytogenetics description
- p53 expression is a feature of both poroma and porocarcinoma (Am J Dermatopathol 2001;23:402)
- p16 overexpression is only seen in porocarcinoma (J Cutan Pathol 2019;46:659)
Sample pathology report
- Skin, left palm, excision:
- Eccrine poroma, extending to the deep margin
Differential diagnosis
- Hidroacanthoma simplex:
- Entirely intraepidermal
- Discrete circumscribed populations of poroma cells within an irregularly acanthotic epidermis
- Dermal duct tumor:
- Entirely intradermal, the epidermis is unaffected
- Large lobules of uniform poroma cells in the mid and lower dermis
- Basal cell carcinoma:
- Squamous cell carcinoma (SCC):
- Lacks evidence of ductal differentiation
- Squamous differentiation abundant, eosinophilic cytoplasm with keratin pearls, intercellular bridges and keratinization
- Greater cytologic atypia, dyskeratotic cells
- Irritated / clonal seborrheic keratosis (SK):
- Shows follicular differentiation with keratinizing pseudohorn cysts, no ductal differentiation
- Cells are typically larger than in poroma
- Hidradenoma:
- Nests and nodules of epithelial cells lacking epidermal connection
- Shows both solid and cystic components
- More commonly shows clear cell features
- Eccrine syringofibroadenoma:
- Benign eccrine proliferation
- Thin anastomosing reticulated cords and strands of basaloid monomorphous cuboidal cells extending from the basal layer of epidermis into dermis
- Loose fibrovascular stroma
Board review style question #1
Which of the following vascular patterns is observed in the dermatoscopic evaluation of eccrine poroma?
- Glomerular
- Hairpin
- Mosaic
- Hairpin and glomerular
- Hairpin and mosaic
Board review style answer #1
D. Hairpin and glomerular. The vascular patterns commonly seen in eccrine poroma are the polymorphic, glomerular, linear irregular, leaf and flower-like and looped or hairpin variants. The leaf and flower-like pattern appears to be relatively unique to the poroma. Mosaic pattern is not observed in eccrine poroma (Clin Case Rep 2021;9:1601).
Comment Here
Reference: Poroma
Comment Here
Reference: Poroma
Board review style question #2
Which of the following is true about eccrine poroma?
- Most commonly occurs on central part of the body: frontal scalp, anterior chest and around umbilicus
- No distinct demarcation between the poroma cells and adjacent keratinocytes
- Presence of monomorphic, basaloid cells with peripheral palisading
- Presence of sheets and trabeculae of monomorphic, round basophilic cells containing scattered duct-like structures
Board review style answer #2
D. Presence of sheets and trabeculae of monomorphic, round basophilic cells containing scattered duct-like structures
Comment Here
Reference: Poroma
Comment Here
Reference: Poroma

