

Skin nontumor
Neutrophilic and eosinophilic dermatoses
Pyoderma gangrenosum
Authors: Bicong (Crane) Wu, M.D., Michi Shinohara, M.D.
Editorial Board Member: Kiran Motaparthi, M.D.


Last author update: 15 November 2021
Last staff update: 23 January 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Pyoderma gangrenosum pathology [TIAB]
Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Wu B, Shinohara M. Pyoderma gangrenosum. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnontumorpyodermagangrenosum.html. Accessed April 26th, 2024.
Definition / general
- Noninfectious neutrophilic dermatosis with painful nodules / pustules that progress to necrotic ulcers with a characteristic violaceous edge
- Pyoderma gangrenosum is a diagnosis of exclusion based on clinical and histological findings
Essential features
- Painful ulcers
- Up to 50% associated with systemic disease, particularly inflammatory bowel disease
- Diagnosis of exclusion
- Early lesions show neutrophilic folliculitis / perfolliculitis with dermal abscess
- Later lesions are ulcerated with mixed dermal inflammation and neutrophilic abscess that undermines the ulcer edge
ICD coding
- ICD-10: L88 - pyoderma gangrenosum
Epidemiology
- Uncommon; ~3 - 10 cases per million people per year
- M = F
- Any age; most common between 20 - 50 years old
- Reference: J Eur Acad Dermatol Venereol 2009;23:1008
Sites
- Any site; most common lower legs, peristomal
Pathophysiology
- Likely multifactorial but poorly understood
- Neutrophil dysfunction: abnormal neutrophil trafficking possibly related to abnormal intracellular metabolic oscillations (J Invest Dermatol 1998;111:259)
- Genetic predisposition: mutations like in the PSTP1P1 / CD2BP1 gene identified for pyoderma gangrenosum associated syndromes, such as pyogenic arthritis, pyoderma gangrenosum and acne (PAPA) syndrome (Hum Mol Genet 2002;11:961)
- Immune system dysregulation / systemic inflammation: increased proinflammatory and neutrophil chemotactic factors (Lab Invest 2000;80:595, Arch Dermatol 2011;147:1203, Am J Clin Dermatol 2017;18:355)
Etiology
- Unknown etiology; 25 - 50% idiopathic
- Up to 50% associated with systemic disease:
- Inflammatory bowel disease (e.g. ulcerative colitis)
- Arthritis
- Hematological malignancy or monoclonal gammopathies
- Other associated conditions: rheumatoid arthritis, seronegative arthritis, pregnancy, viral hepatitis, HIV, granulomatosis with polyangiitis
- Reference: Clin Med (Lond) 2019;19:224
Clinical features
- 4 major subtypes:
- Ulcerative / classic (most common): erythematous lesion that rapidly progresses to ulcer with undermined edge, violaceous border and purulent base
- Painful, with or without fever
- Possible pathergy (precipitated by minor trauma)
- Bullous: often associated with a hematological malignancy (Arch Dermatol 1972;106:901)
- Pustular: often associated with inflammatory bowel disease (Clin Exp Dermatol 2003;28:600)
- Vegetative / superficial granulomatous: mildly painful, verrucous quality, often without systemic condition (J Am Acad Dermatol 1988;18:511)
- Ulcerative / classic (most common): erythematous lesion that rapidly progresses to ulcer with undermined edge, violaceous border and purulent base
Diagnosis
- Nonspecific clinical and histologic findings; a diagnosis of exclusion
- Proposed diagnostic criteria by Delphi Consensus of International Experts (JAMA Dermatol 2018;154:461):
- Need major criteria + ≥ 4 minor criteria
- Major criteria: neutrophilic infiltrate on biopsy of ulcer edge
- Minor criteria:
- Exclude infection
- Pathergy
- History of inflammatory bowel disease or inflammatory arthritis
- History of papule, pustule, vesicle within 4 days of ulceration
- Peripheral erythema, undermining border and tenderness
- Multiple ulceration, at least 1 on anterior lower leg
- Healed ulcer site with wrinkled paper scar
- Decreased ulcer size upon initiating immunosuppressant
Prognostic factors
- > 50% achieve complete wound healing in 1 year (Australas J Dermatol 2011;52:218)
- Unfavorable prognostic factors: male, old age onset, bullous pyoderma gangrenosum associated with hematologic malignancy
- Favorable prognostic factors: no underlying disease
Case reports
- 11 month old girl with papular, erythematous eruption on her legs, buttock, torso and oral mucosa (Pediatr Dermatol 2018;35:e257)
- 36 year old woman with extensive pyoderma gangrenosum after caesarean section (Int J Surg Case Rep 2021;81:105697)
- 67 year old woman and 87 year old woman with rheumatoid arthritis on rituximab that developed vulvovaginal pyoderma gangrenosum (JAAD Case Rep 2021;10:75)
- 68 year old man with history of ulcerative rectocolitis and erythematous and painful lesion on his leg (Dermatol Ther 2019;32:e12928)
Treatment
- General measures: control underlying disease, manage pain, wound care, avoid trauma
- For limited disease: topical therapy with corticosteroid and calcineurin inhibitors
- For extensive or advanced disease: first line therapy with systemic glucocorticoids or cyclosporine; second line / adjunctive therapy with tumor necrosis factor alpha (TNF alpha) inhibitors and anti-interleukin therapy
- Reference: Am J Clin Dermatol 2017;18:355
Clinical images
Contributed by Michi Shinohara, M.D.

Leg ulcer
Microscopic (histologic) description
- Variable, dependent on the lesion age and site
- Early lesion:
- Neutrophilic folliculitis and perifolliculitis
- Intradermal neutrophilic abscess formation
- Later lesions:
- Epidermal ulceration
- Superficial dermal necrosis
- Mixed inflammation with undermining at ulcer edge (characteristic) and abscess
- Occasional giant cells (associated with inflammatory bowel disease)
- Advancing edge often has subepidermal edema
- Leukocytoclastic vasculitis and lymphocytic vasculitis may be present (J Cutan Pathol 2003;30:97)
- Acanthosis in perilesional zone
- Variants:
- Ulcerative / classic variant: central neutrophilic abscess and peripheral angiocentric lymphocytic infiltrates
- Bullous variant: subepidermal bullae and dermal neutrophilic infiltrates
- Pustular variant: subcorneal pustules, subepidermal edema, dense dermal neutrophilic infiltrates
- Vegetative / superficial granulomatous variant: reactive epidermal proliferation, dermal abscess, sinus tracts and palisading granulomas
Microscopic (histologic) images
Contributed by Michi Shinohara, M.D.
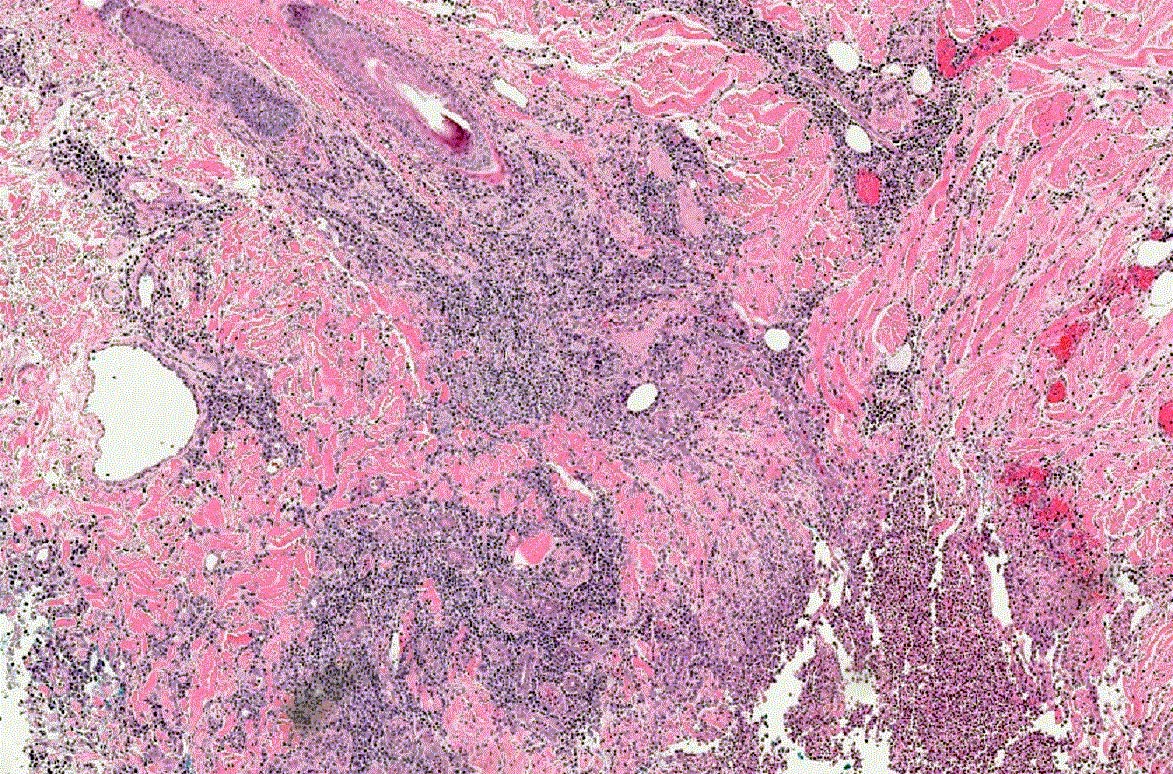
Early lesion
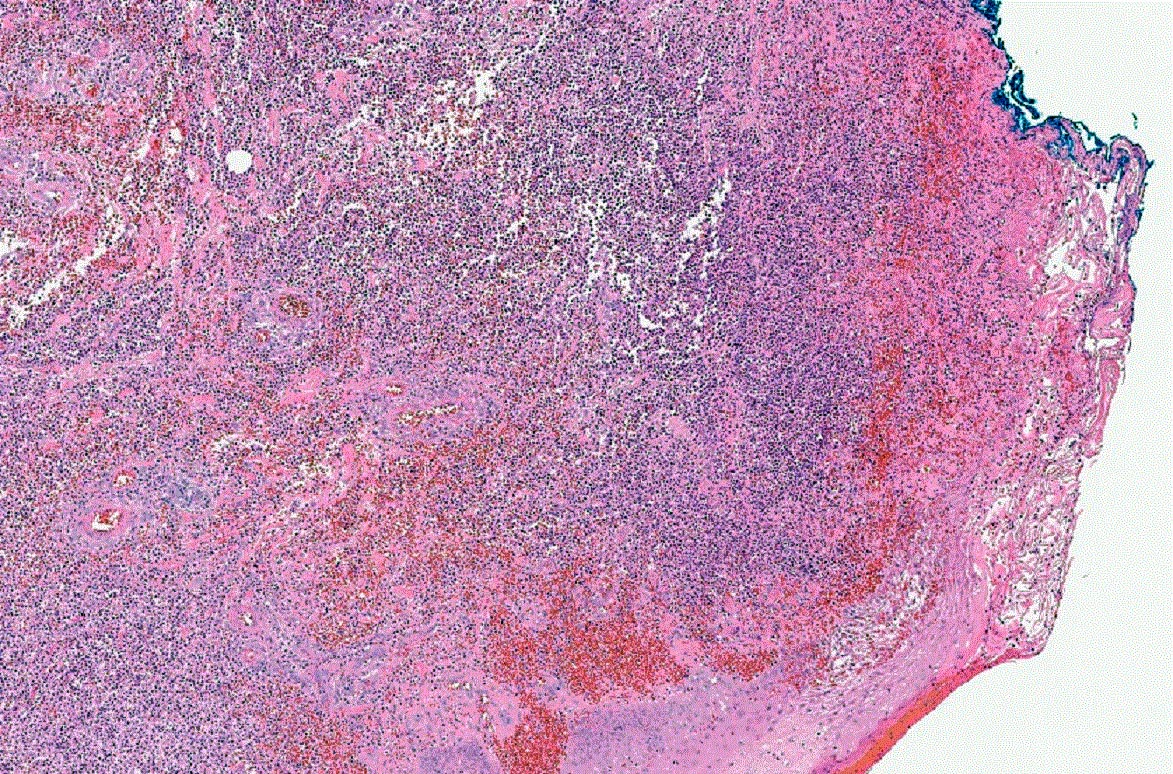
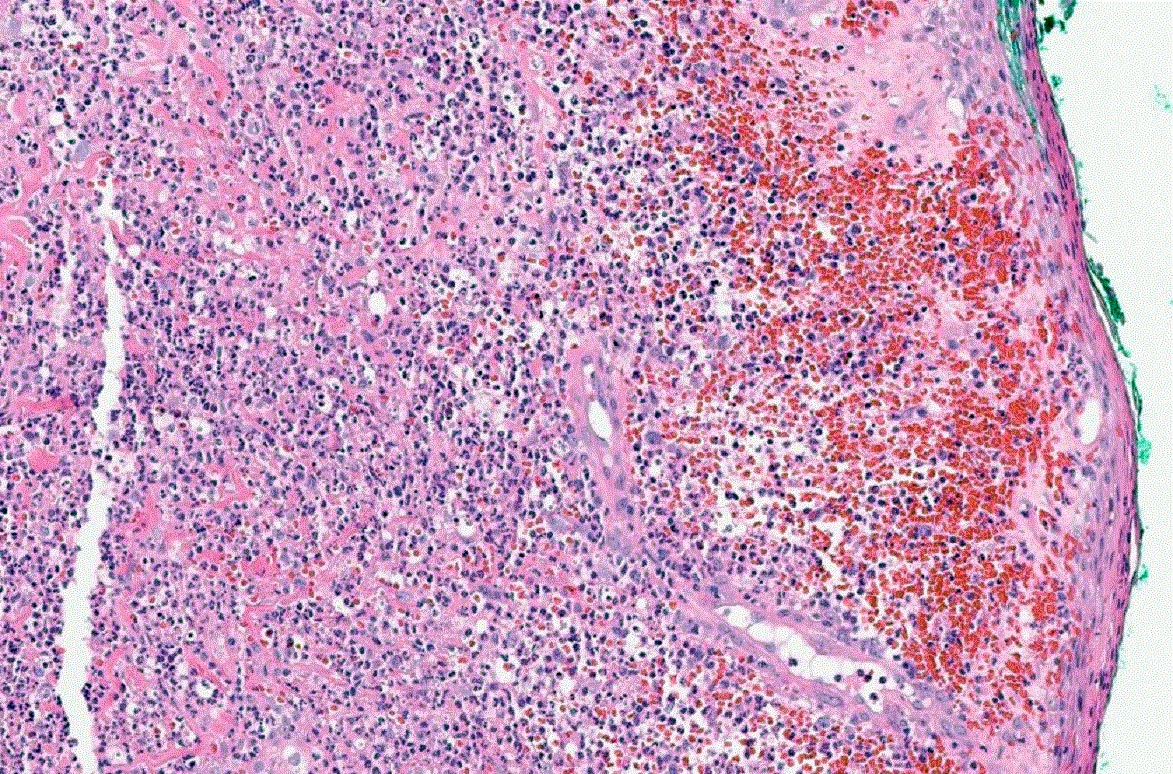
Late lesion
Videos
Pyoderma gangrenosum versus nonspecific chronic ulcer changes
Sample pathology report
- Skin, leg, punch biopsy:
- Ulcer with mixed dermal inflammation (see comment)
- Comment: The findings are nonspecific but could be compatible with pyoderma gangrenosum. Pyoderma gangrenosum is a diagnosis of exclusion and other causes of ulceration, including infection, must be ruled out.
Differential diagnosis
- Sweet syndrome:
- Not typically associated with ulcer, prominent karyorrhexis and deeper / more extensive inflammation
- Infection or necrotizing fasciitis:
- Involves deeper subcutaneous tissue; presence of microorganisms
- Arthropod bite reaction:
- Numerous eosinophils
- Venous stasis ulceration:
- Can show identical findings, usually without prominent neutrophils
- Can show identical findings
Additional references
Board review style question #1

Which of the following systemic diseases is most often associated with pyoderma gangrenosum?
- Diabetes mellitus
- Peripheral vascular disease
- Systemic lupus erythematosus
- Ulcerative colitis
Board review style answer #1
Board review style question #2
Which of the following is a feature of early pyoderma gangrenosum biopsies?
- Eosinophilic pustulosis
- Epidermal ulceration
- Neutrophilic folliculitis
- Subepidermal bullae
Board review style answer #2
