

Table of Contents
Definition / general | Epidemiology | Clinical features | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Differential diagnosis | Additional referencesCite this page: Do HK. Chromoblastomycosis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnontumorfungiChromoblastomycosis.html. Accessed May 1st, 2024.
Definition / general
- Chronic deep cutaneous fungal infection usually affecting the limbs at the inoculation site
- Causative agents include several fungi found in soil, wood and decaying plant material:
- Phialophora verrucosa
- Fonsecaea pedrosi
(most common pathogen, accounts for > 90% of the cases in South America) - Fonsecaea compacta
- Cladosporium carrionii
- Rhinocladiella aquaspersa (Ramichloridium cerophilum)
- Phialophora verrucosa
Epidemiology
- First case of chromoblastomycosis was reported by Pedroso in Brazil in 1911
- Incidence of chromoblastomycosis is greatest in tropical and subtropical regions, including Madagascar, Brazil, Gabon, Colombia, Venezuela, Cuba, the Dominican Republic and Mexico
- Up to 70% of cases occur in males
- Barefooted farmers account for almost 75% of patients with chromoblastomycosis
Clinical features
- Common clinical presentation is verrucous lesion over extremities of adult men engaged in outdoor work (Indian J Pathol Microbiol 2010;53:666)
- The disease is slowly progressive - the average time between the initial lesion and the clinical diagnosis is 15 years
- Lesion starts as a small firm red / gray bump on the traumatized skin on the foot or hand
- Grows slowly (2 mm/year) to form raised hyperkeratotic (crusted, warty-looking) plaque
- The affected limp can be enlarged (elephantiasis)
- Can develop satellites lesions (new lesions near primary lesion)
- Rarely, squamous cell carcinoma develops within longstanding chromoblastomycosis (An Bras Dermatol 2010;85:267)
- Diagnosis: culture at 25 - 30 degrees Celsius grows olive-green to black fungal colonies after 1 - 2 weeks
Treatment
- Treatment is difficult and long
- A Mexican study showed 30% cure rate, 60% improvement, and 10% failed therapy
- Smaller lesions are best treated with surgical excision or cryotherapy (multiple treatments may span up to 10 years)
- Extensive lesions can be treated with itraconazole (up to several years), or terbinafine (up to several months)
- Often dramatic improvement at first, but difficult to cure
- Some studies suggest a multidrug approach is more effective: itraconazole + flucytosine; flucytosine + amphotericin B
- Recalcitrant lesions can be treated with a combination of itraconazole and cryotherapy or local hyperthermia or CO2 laser vaporization
Clinical images
Images hosted on other servers:

Hyperkeratotic plaque

Cultures are
typically olive
black with a
suede-like surface
Microscopic (histologic) description
- Clinical suspicious is important to alert pathologists to check for sclerotic bodies, which may be rare
- The classical histopathological hallmarks are pseudoepitheliomatous hyperplasia with intraepidermal abscess and pigmented fungal sclerotic bodies (Medlar bodies or copper bodies)
- Fungi appear in clusters that reproduce by equatorial septation rather than budding
- Fungal stains show fungi within macrophages and rarely in factor XIIIa positive dedrocytes or Langerhan cells
Microscopic (histologic) images
Images hosted on other servers:


Sclerotic bodies: H&E and KOH prep

H&E stain of
sclerotic bodies in
an intraepidermal
abscess

Skin biopsy specimen
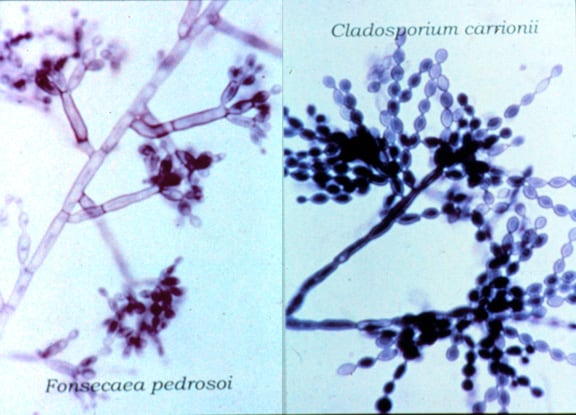
Cladosporium carrionii (left) and Fonsecaea pedrosoi (right), the 2 most common pathogenic fungi causing chromoblastomycosis
Differential diagnosis
- Leishmaniasis
- Sporotrichosis
- Squamous cell carcinoma
Additional references
