

Skin nontumor
Alopecia
Alopecia areata
Editorial Board Member: Kiran Motaparthi, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 15 November 2021
Last staff update: 15 November 2021
Copyright: 2020-2024, PathologyOutlines.com, Inc.
PubMed Search: Alopecia areata[title] free full text[SB] review[PT]

Table of Contents
Definition / general | Essential features | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Immunofluorescence description | Positive stains | Electron microscopy description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Saleh J, Speiser J. Alopecia areata. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnontumoralopeciaareata.html. Accessed December 4th, 2024.
Definition / general
- Hair loss secondary to an autoimmune disorder that targets the hair follicle bulb (Nat Rev Dis Primers 2017;3:17011)
Essential features
- Originates from loss of the immune privilege of the hair follicle, which allows for a lymphocyte mediated autoimmune attack of the hair follicle bulb (Expert Rev Clin Immunol 2015;11:1335)
- A characteristic clinical finding is exclamation point hairs: 2 - 3 mm hairs that appear to float on the scalp because of shaft narrowing and hypopigmentation near the scalp surface that appear at the advancing margin of the patches (Postepy Dermatol Alergol 2014;31:113)
- Increased miniaturized hairs and characteristic "swarm of bees" peribulbar mononuclear cell inflammation affecting terminal anagen and catagen hairs seen in acute phase (Histopathology 2010;56:24, Arch Dermatol 2003;139:1555)
- Numerous miniaturized (vellus) hairs and mild peribulbar mononuclear cell inflammation involving nanogen hairs seen in chronic phase (Arch Dermatol 2003;139:1555)
Epidemiology
- Affects males and females of all ages and ethnicities (Nat Rev Dis Primers 2017;3:17011, Histopathology 2010;56:24)
- Lifetime risk is 1 - 2% (Nat Rev Dis Primers 2017;3:17011)
- 50% of patients experience onset in childhood, 60% before the age of 20 and 85.5% before the age of 40 (BMJ 2010;341:c3671)
- A family history of alopecia areata or other autoimmune disease is present in 15.5 - 18.3% and 12.7% of patients, respectively (Indian J Dermatol 2008;53:70)
- Associated with higher rates of thyroid disease, vitiligo and atopic eczema (Nat Rev Dis Primers 2017;3:17011)
- Increased prevalence in patients with chromosomal disorders such as Down syndrome (Int J Trichology 2013;5:227)
- May be drug induced when arising in patients on biologic medicines (Nat Rev Dis Primers 2017;3:17011)
Sites
- Scalp and hair bearing skin
- Any site with hair can be affected
Pathophysiology
- Originates from loss of the immune privilege of the hair follicle, which allows for a lymphocyte mediated autoimmune attack of the hair follicle bulb (Expert Rev Clin Immunol 2015;11:1335)
- Lymphocytes are comprised of CD8+ NK group 2D positive (NKG2D+) T cells that release proinflammatory cytokines and chemokines that reject the hair (Clin Dev Immunol 2013;2013:348546)
- Exact mechanism is not yet understood although a genome wide association study provided evidence that both acquired and innate immunity contribute to the pathogenesis of alopecia areata (Nature 2010;466:113)
- Onset or recurrence of hair loss is sometimes triggered by viral infection, trauma, hormonal changes or emotional / physical stressors (Nat Rev Dis Primers 2017;3:17011)
Clinical features
- Classic alopecia areata
- Bald patch or thinning hair is initially noted (Postepy Dermatol Alergol 2014;31:113)
- Also presents with trichodynia, which is a burning, prickly discomfort in the affected areas (Int J Dermatol 2016;55:382)
- Presents with patchy, well circumscribed or rarely diffuse hair loss without evidence of inflammation that may affect any hair bearing area, including the scalp, eyebrows, eyelashes and beard (Postepy Dermatol Alergol 2014;31:113)
- Lesions may appear suddenly and expand rapidly (Postepy Dermatol Alergol 2014;31:113)
- A characteristic clinical finding is exclamation point hairs - 2 - 3 mm hairs that appear to float on the scalp because of shaft narrowing and hypopigmentation near the scalp surface that appear at the advancing margin of the patches (Postepy Dermatol Alergol 2014;31:113)
- Regrowing hairs are often initially depigmented (Postepy Dermatol Alergol 2014;31:113)
- Subtypes of alopecia areata (Chin Med Sci J 2017;32:44)
- Alopecia totalis (5% of cases)
- All or the majority of scalp hair is lost
- Alopecia universalis (less than 1% of cases)
- All or the majority of hair on the scalp and body is lost
- Ophiasis
- Pattern of alopecia areata affecting the occipital and lateral scalp in which a bald area encircles the scalp
- Diffuse alopecia areata (alopecia areata incognita)
- Sudden, diffuse loss of hair characterized by the gray color of the persisting hair (turning white overnight) and has a positive hair pull test
- Alopecia areata of the nails (affects 10 - 50% of patients with alopecia areata)
- Regular pitting and ridging of the nails
- Alopecia totalis (5% of cases)
Diagnosis
- Scalp biopsy followed by histologic examination
- Trichoscopy (J Dermatol 2018;45:692)
- Findings include yellow dots, short vellus hairs, black dots, broken hairs, exclamation mark hairs, tapered hair, upright regrowing hairs, pigtail (circle) hairs, and Pohl-Pinkus constrictions
Prognostic factors
- Treatment may help halt further hair loss or initiate hair regrowth (Can Fam Physician 2015;61:757)
- Prognostic factors associated with poor outcomes in individuals with alopecia areata (Can Fam Physician 2015;61:751)
- Extensive loss
- Ophiasis variant
- Nail changes
- Early age of onset
- Family history
- Concomitant autoimmune diseases (e.g. atopy, Hashimoto thyroiditis)
Case reports
- 24 year old man with celiac disease and obesity (Rev Fac Cien Med Univ Nac Cordoba 2020;77:49)
- 50 year old woman taking clobenzorex for obesity (Int J Trichology 2019;11:236)
- 70 year old man receiving ixekizumab for psoriatic arthritis (JAAD Case Rep 2019;6:51)
Treatment
- First line treatment: topical or intralesional corticosteroid, minoxidil, anthralin, topical immunotherapy (i.e. diphenylcyclopropenone, squaric acid dibutylester and dinitrochlorobenzene) or topical retinoids (Clin Cosmet Investig Dermatol 2011;4:107)
- Second line treatment: sulfasalazine, photochemotherapy, excimer laser or fractional photothermolysis laser (Clin Cosmet Investig Dermatol 2011;4:107)
- Third line treatment: systemic corticosteroids, methotrexate, cyclosporine, azathioprine or biologics (Clin Cosmet Investig Dermatol 2011;4:107)
- Recent studies have found that JAK inhibitors, including oral tofacitinib and ruxolitinib, are effective in treating alopecia areata; however, interruption of treatment can result in recurrence (Indian J Dermatol Venereol Leprol 2021;87:621, Dermatol Clin 2021;39:407, Clin Cosmet Investig Dermatol 2021;14:691)
Clinical images
Images hosted on other servers:

Patchy hair loss

Trichoscopy

Regrowth after treatment
Microscopic (histologic) description
- Hair cycle consists of three phases: anagen (the growth phase), catagen (the regressing phase) and telogen (the resting phase) (J Investig Dermatol Symp Proc 2003;8:56)
- Anagen:
- Terminal anagen hair extends from its bulb in the subcutaneous tissue to its point of emergence from the epidermis through the follicular infundibulum (J Investig Dermatol Symp Proc 2003;8:56)
- Has fully developed inner and outer root sheaths with no signs of apoptosis in the outer root sheath
- Catagen:
- Hair shaft tracts upward and the lower follicle disappears, leaving an angiofibrotic strand or streamer (stela) (J Investig Dermatol Symp Proc 2003;8:56)
- Has thickening of the basal membrane and apoptotic bodies in outer root sheath
- Telogen:
- Club shaped root is situated at the level of the bulge at the insertion of the arrector pili muscle (J Investig Dermatol Symp Proc 2003;8:56)
- Has wrinkling of the inner root sheath (flamethrower appearance)
- Acute and subacute disease
- Normal total number of hairs (Histopathology 2010;56:24)
- Increased miniaturized hairs (Arch Dermatol 2003;139:1555)
- Increased number of terminal catagen and telogen hairs (Dermatol Ther 2011;24:369)
- Characteristic "swarm of bees" peribulbar mononuclear cell inflammation affecting terminal anagen and catagen hairs (Histopathology 2010;56:24, Arch Dermatol 2003;139:1555)
- Trichomalacia and narrowing of hair shafts (Histopathology 2010;56:24)
- Chronic disease
- Majority of hairs are in catagen / telogen phase (Histopathology 2010;56:24)
- Numerous miniaturized (vellus) hairs (Dermatol Ther 2011;24:369)
- Mild peribulbar mononuclear cell inflammation involving nanogen hairs (Arch Dermatol 2003;139:1555)
- When telogen hairs predominate, inflammation may be absent (Arch Dermatol 2003;139:1555)
Microscopic (histologic) images
Contributed by Jodi Speiser, M.D.
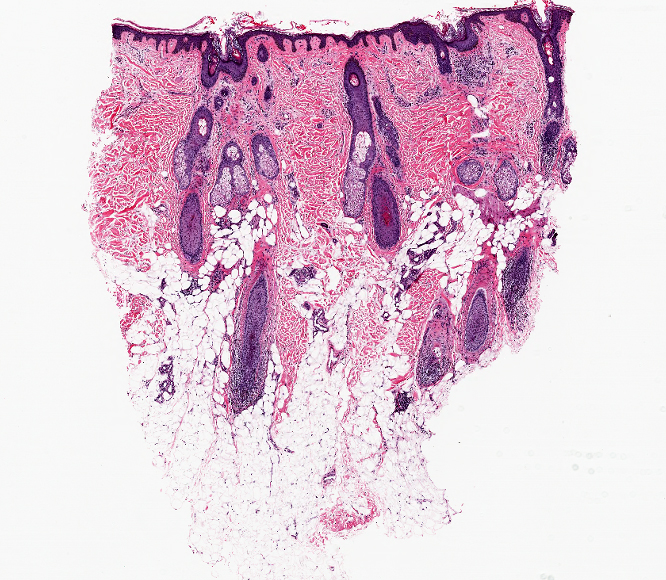
Vertical section of scalp biopsy
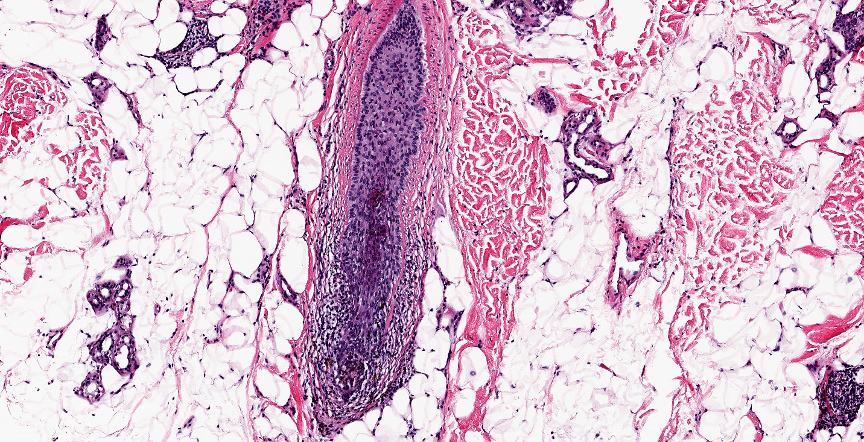
Perifollicular lymphocytes
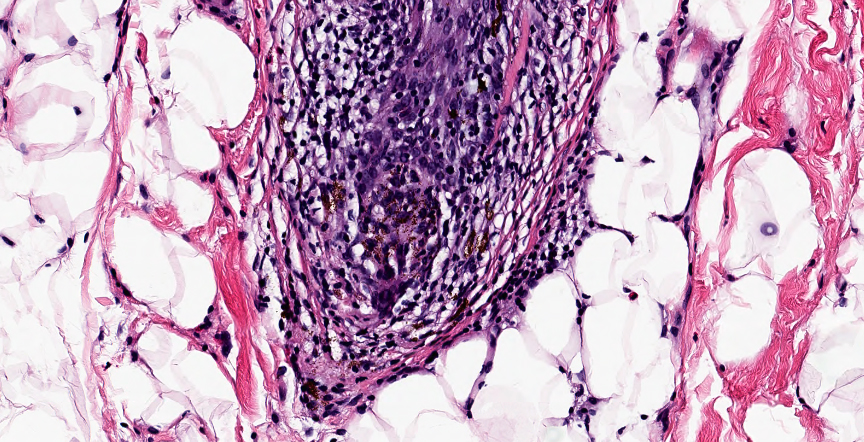
Peribulbar / intrabulbar
lymphocytic infiltration
Immunofluorescence description
- Abnormal deposits of C3 and occasionally of IgG and IgM in approximately 92% of cases (J Invest Dermatol 1979;73:317)
Positive stains
- Elastic fibers / Verhoeff van Gieson shows narrow fibrous tracts and no significant changes in elastic network (J Cutan Pathol 2013;40:211)
- Periodic acid Schiff (PAS) shows normal basement membrane thickness
- CD3 highlights T cells
Electron microscopy description
- 4 patterns (J Dermatol 2013;40:1045)
- Long tapering structure with no accumulation of scales
- Club shaped hair root with fine scales
- Proximal accumulation of scales
- Sharp tapering of the proximal end of hair
Sample pathology report
- Skin, left posterior scalp, punch biopsy:
- Nonscarring alopecia (see comment)
- Comment: Histological sections show a reduction in number of hair follicles with evidence of miniaturization. There is bulbar and periadnexal lymphocytic inflammation. Immunohistochemical stain for CD3 demonstrates lymphocytes are predominantly T cells. There is a catagen / telogen shift. PAS stain shows normal basement membrane thickness and EVG stain shows preservation of elastic fibers. These findings are consistent with alopecia areata.
Differential diagnosis
- Syphilitic alopecia:
- Characterized by superficial and deep (peribulbar) inflammation with plasma cells (in contrast to alopecia areata and psoriatic alopecia, which have peribulbar lymphocytic infiltrates with occasional eosinophils)
- Confirmatory serology is recommended
- Endothelial cell predominance
- May be indistinguishable based on histopathology alone
- Telogen effluvium:
- Normal number of total hair follicles but with catagen / telogen shift
- No miniaturization of hair follicles
- Minimal inflammation is present
- Synchronization is typical of alopecia areata but not telogen effluvium
- While alopecia areata can have catagen / telogen counts of 50% or more, this is not observed in telogen effluvium
- Psoriatic alopecia:
- Normal or decreased number of total hair follicles but with catagen / telogen shift
- Extensive follicular miniturization
- Atrophy of sebaceous glands
- Epidermal changes of seborrheic dermatitis or psoriasis
- May show mild, focal peribulbar lymphocytic infiltrates with occasional eosinophils
- Premature desquamation of the inner root sheath
- Trichotillomania::
- May have the follwing histologic features:
- Incomplete, disrupted follicular anatomy and increased catagen / teolgen hairs without inflammation or miniaturization
- Trichomalacia
- Melanin in collapsed fibrous root sheaths
- Fractured hair shafts
- Perifollicular and interfollicular hemorrhage
- Has pigment casts but these are nonspecific and can be observed in alopecia areata, traction alopecia and syphilis
- Clinical history is especially important
- May have the follwing histologic features:
- Acute traction alopecia:
- May have the follwing histologic features:
- Normal follicular count with catagen / telogen shift
- Trichomalacia and pigment casts present
- Clinical history is espcially important - tight hair pulling or braiding
- Absence of inflammation
- Often sharp reduction in terminal hairs but with preservation of sebaceous lobules
- May have the follwing histologic features:
- Androgenetic alopecia:
- Reduced follicular count at dermal / subcutaneous junction
- Prominent sebaceous glands, minimal inflammation
- Anisotrichosis and miniaturization with minimal inflammation
- Mild increase in catagen / telogen hairs
- Solar elastosis present in more advanced cases
Board review style question #1
Which of the following is true about the disorder shown in the image above?
- Increased number of terminal catagen and telogen hair
- Not associated with autoimmune disorders
- No hair follicular miniaturization
- Predominantly affects young Caucasian women
Board review style answer #1
Board review style question #2
In which of the following alopecias are exclamation point hairs seen?
- Alopecia areata
- Androgen alopecia
- Cicatricial alopecia
- Syphilitic alopecia
Board review style answer #2

