
Pancreas
Exocrine carcinomas
Undifferentiated carcinoma
Author: Claudio Luchini, M.D., Ph.D.
Editorial Board Member: Wei Chen, M.D., Ph.D.
Deputy Editor-in-Chief: Raul S. Gonzalez, M.D.

Last author update: 13 February 2023
Last staff update: 13 February 2023
Copyright: 2012-2025, PathologyOutlines.com, Inc.
PubMed Search: Undifferentiated carcinoma pancreas


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Luchini C. Undifferentiated carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/pancreasundifferentiated.html. Accessed March 31st, 2025.
Definition / general
- Carcinoma of the pancreas that does not show a definitive direction of differentiation
- Under this definition, there are 4 variants: anaplastic, sarcomatoid, rhabdoid and carcinosarcoma (Mod Pathol 2015;28:248)
Essential features
- Undifferentiated carcinoma with atypical neoplastic cells and without gland formation
- Absence of osteoclast-like giant cells
- Very poor prognosis
Terminology
- Undifferentiated carcinoma of the pancreas
- Old terminology, not in use: spindle cell carcinoma, pleomorphic carcinoma
ICD coding
Epidemiology
- M:F = 2:1 (World J Gastroenterol 2016;22:8631)
- Commonly presents in the sixth to seventh decades (World J Gastroenterol 2016;22:8631, J Am Coll Surg 2012;215:627)
- 1 - 5% of all pancreatic cancers (World J Gastroenterol 2016;22:8631, J Am Coll Surg 2012;215:627)
Sites
- Head of the pancreas (50% of cases), body / tail (45%), entire pancreas (5%) (World J Gastroenterol 2016;22:8631)
Pathophysiology
- The process of epithelial to mesenchymal transition may play an important role (Pancreas 2019;48:36, Virchows Arch 2021;478:319)
- Chronic inflammation with histiocytes is not a crucial mechanism as in undifferentiated carcinoma with osteoclast-like giant cells (Hum Pathol 2018;81:157)
Clinical features
- Presenting symptoms include jaundice (tumors in the pancreatic head), abdominal or back pain, weight loss, nausea and anemia (Diagn Cytopathol 2016;44:538, World J Gastroenterol 2016;22:8631, World J Clin Cases 2019;7:236)
Diagnosis
- CT scan and MRI are the preferred imaging modality (J Med Imaging Radiat Oncol 2019;63:580)
- Diagnosis is by biopsy or surgical resection
Radiology description
- Usually mass lesions with delayed enhancement, intratumor calcifications (J Med Imaging Radiat Oncol 2019;63:580)
Prognostic factors
- Prognosis is very poor, with an average survival time of just 5 months, making it difficult to describe significant prognostic factors (J Am Coll Surg 2012;215:627)
- Absence of osteoclast-like giant cells is important for the diagnosis of real, undifferentiated carcinoma (i.e., to avoid misdiagnosis) but is essential for the prognosis as well, since the prognosis of real, undifferentiated carcinoma is very poor, compared with that of carcinoma with osteoclast-like giant cells
Case reports
- 59 year old man with undifferentiated carcinoma of the pancreas, sarcomatoid type (World J Clin Cases 2019;7:236)
- 63 year old man with undifferentiated carcinoma of the pancreas, rhabdoid type, with multiple metastases (autopsy report) (Pathol Int 2015;65:264)
- 64 year old woman with undifferentiated carcinoma of the pancreas, anaplastic type, associated with cystic degeneration of the lesion (World J Gastroenterol 2016;22:8631)
- 65 year old man with undifferentiated carcinoma of the pancreas, anaplastic type, involving the ampullary region (Am J Case Rep 2019;20:597)
- 73 year old woman with undifferentiated carcinoma of the pancreas, carcinosarcoma type (Pancreas 2017;46:1225)
Treatment
- Surgical resection if possible; gemcitabine based chemotherapy / radiotherapy (J Surg Res 2017;219:238)
- A recent study highlighted a possible role of immunotherapy in selected cases, PDL1 positive (Expert Opin Ther Targets 2021;25:1007)
Gross description
- Very often similar to conventional pancreatic ductal adenocarcinoma
- May show cystic degeneration and necrosis (World J Gastroenterol 2016;22:8631)
Gross images
Contributed by Claudio Luchini, M.D., Ph.D. and AFIP
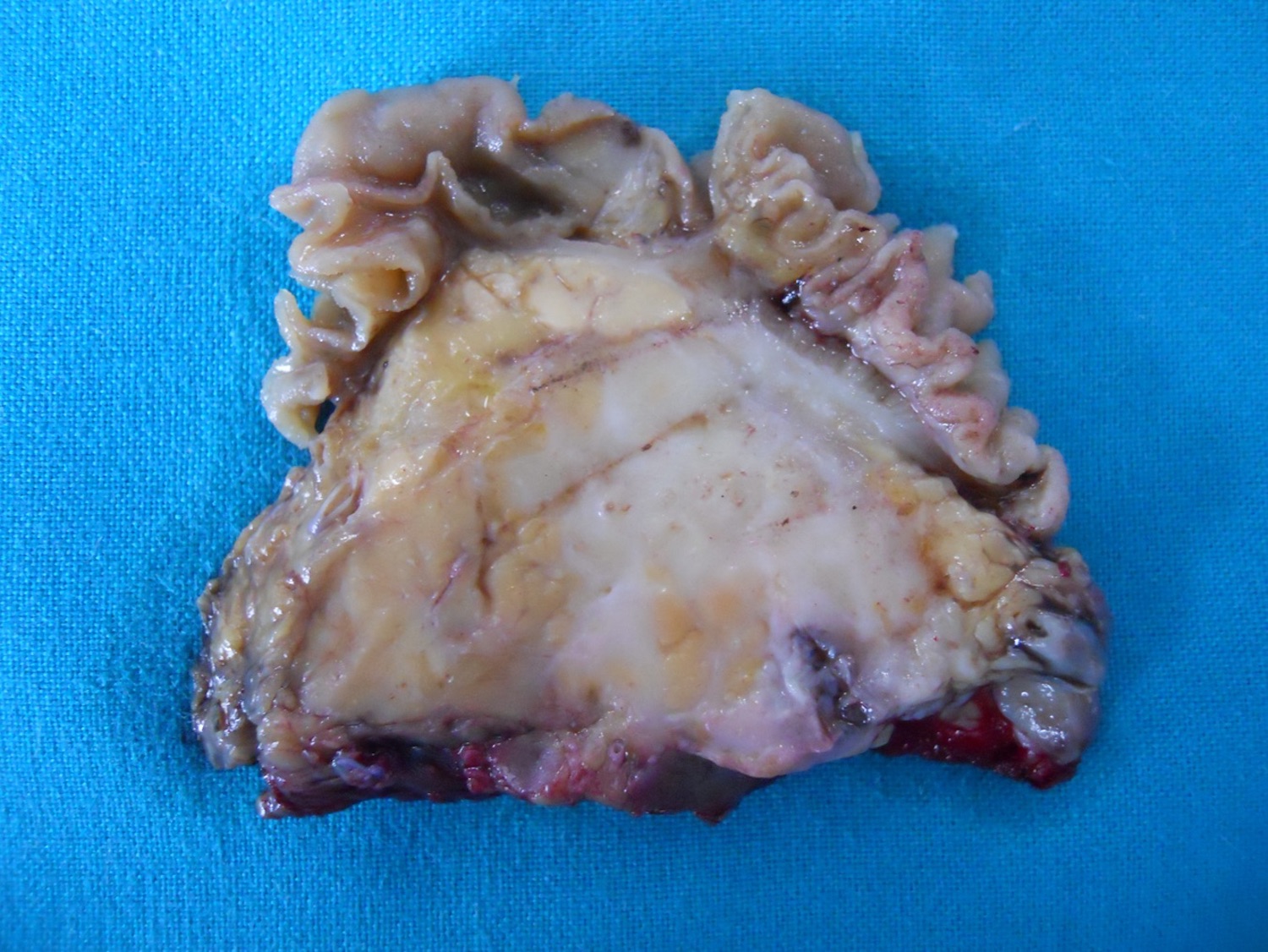
Ductal
adenocarcinoma
with undifferentiated
component
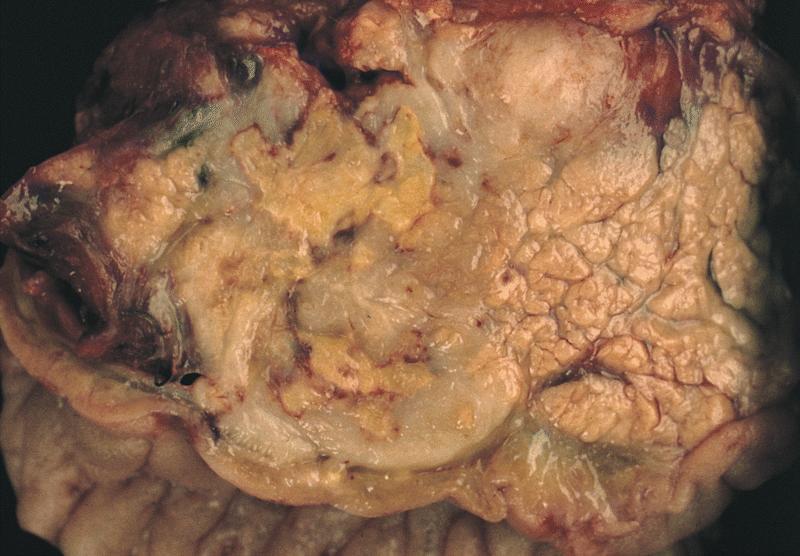
Ill demarcated tumor in head of pancreas

Extensive hemorrhagic necrosis
Frozen section description
- Hypercellular neoplasm with atypical cells
Microscopic (histologic) description
- Unlike conventional ductal adenocarcinoma, this tumor is composed of poorly cohesive cells
- Undifferentiated carcinoma of the pancreas is a hypercellular tumor with scant stroma and scant desmoplastic reaction; this differs from conventional pancreatic ductal adenocarcinoma which has a large amount of desmoplastic stroma with few neoplastic cells / glands
- This is a major point in the differential diagnosis between these 2 entities
- Perineural invasion and vascular invasion are very common
- Different subtypes are characterized at the histological level by different morphologic hallmarks:
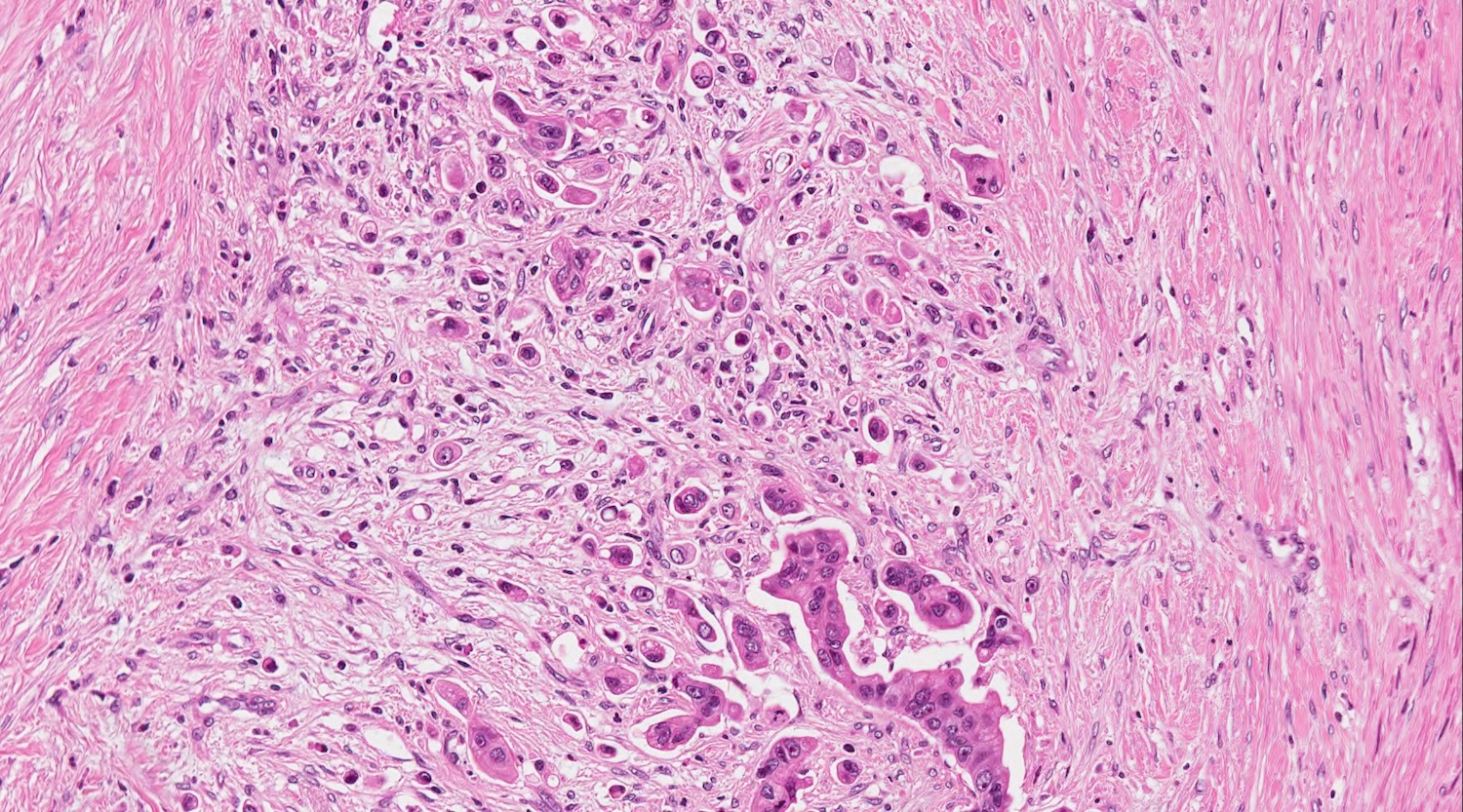
- Anaplastic subtype is a tumor composed of > 80% highly atypical cells that have pleomorphic nuclei and lack gland formation
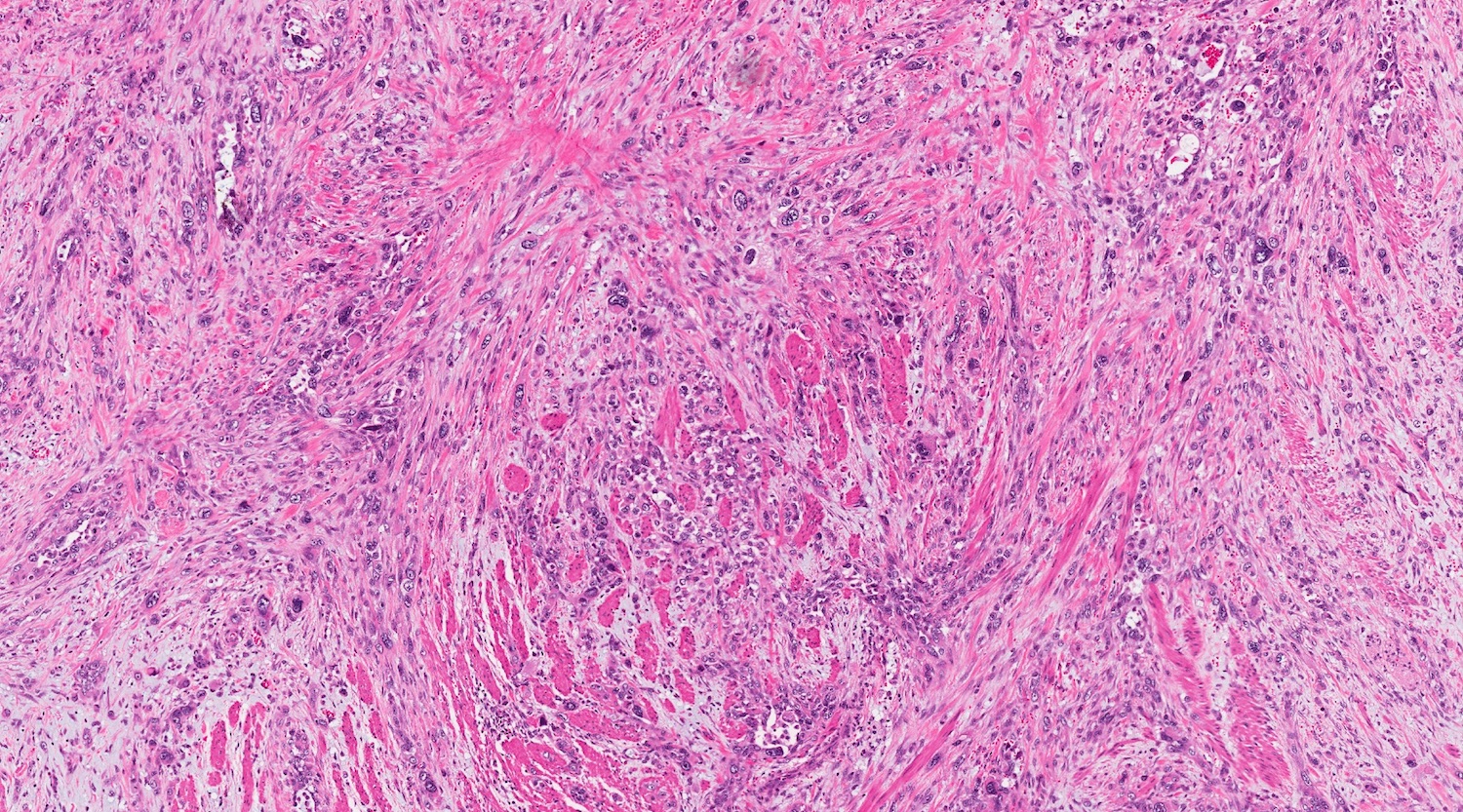
- Sarcomatoid subtype is composed of > 80% atypical spindle cells, resembling a sarcoma (Int J Mol Sci 2022;23:1283, Hum Pathol 2022;128:124)
- Rhabdoid subtype is a very rare sarcomatoid variant which is composed of large atypical cells with eosinophilic cytoplasm and eccentrically located nuclei
- Carcinosarcoma is a subtype in which there is a mixture of roundish epithelioid cells and spindle sarcomatous cells; each component should arbitrarily constitute 30% of the neoplasm to qualify as carcinosarcoma
Microscopic (histologic) images
Contributed by Claudio Luchini, M.D., Ph.D. and AFIP
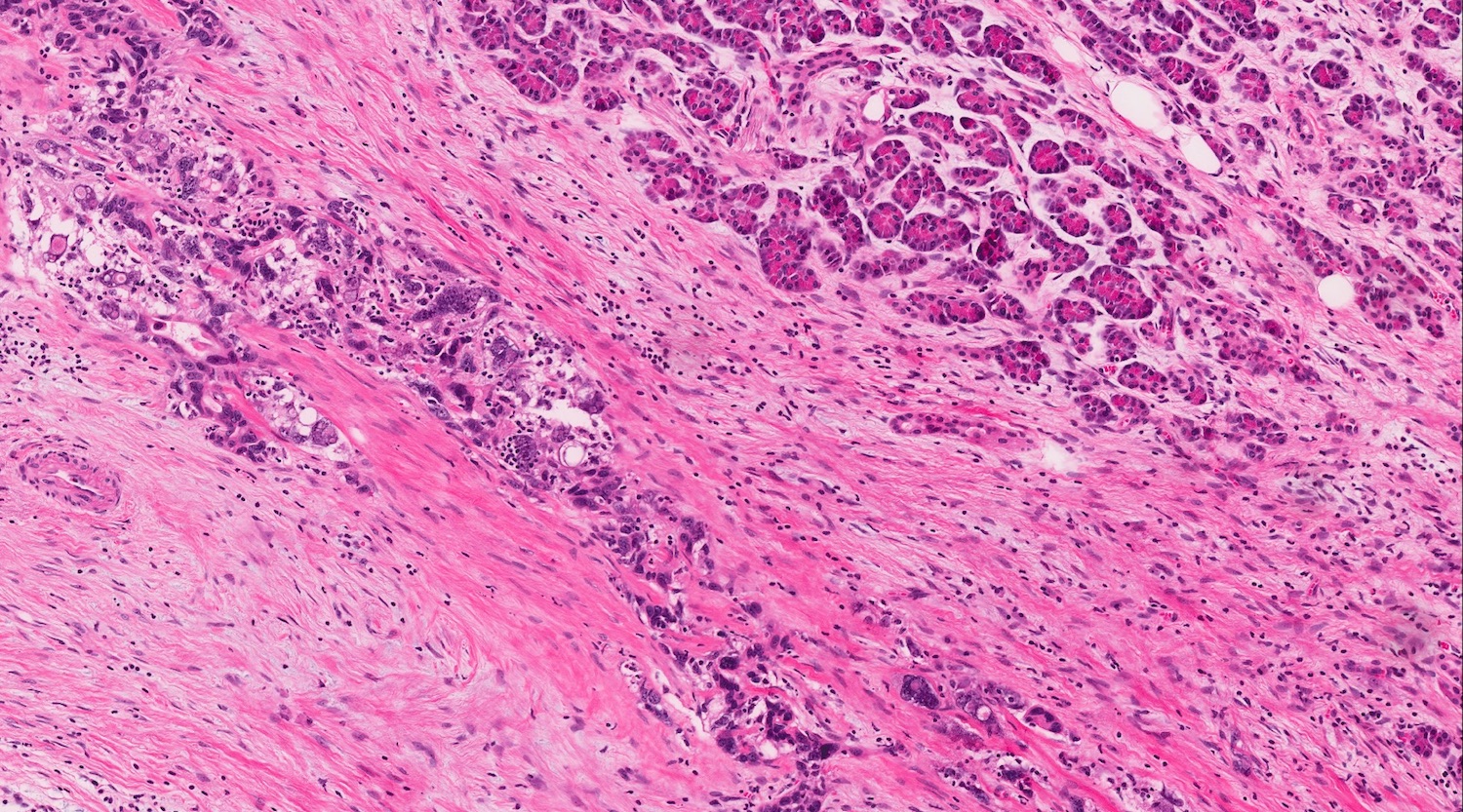
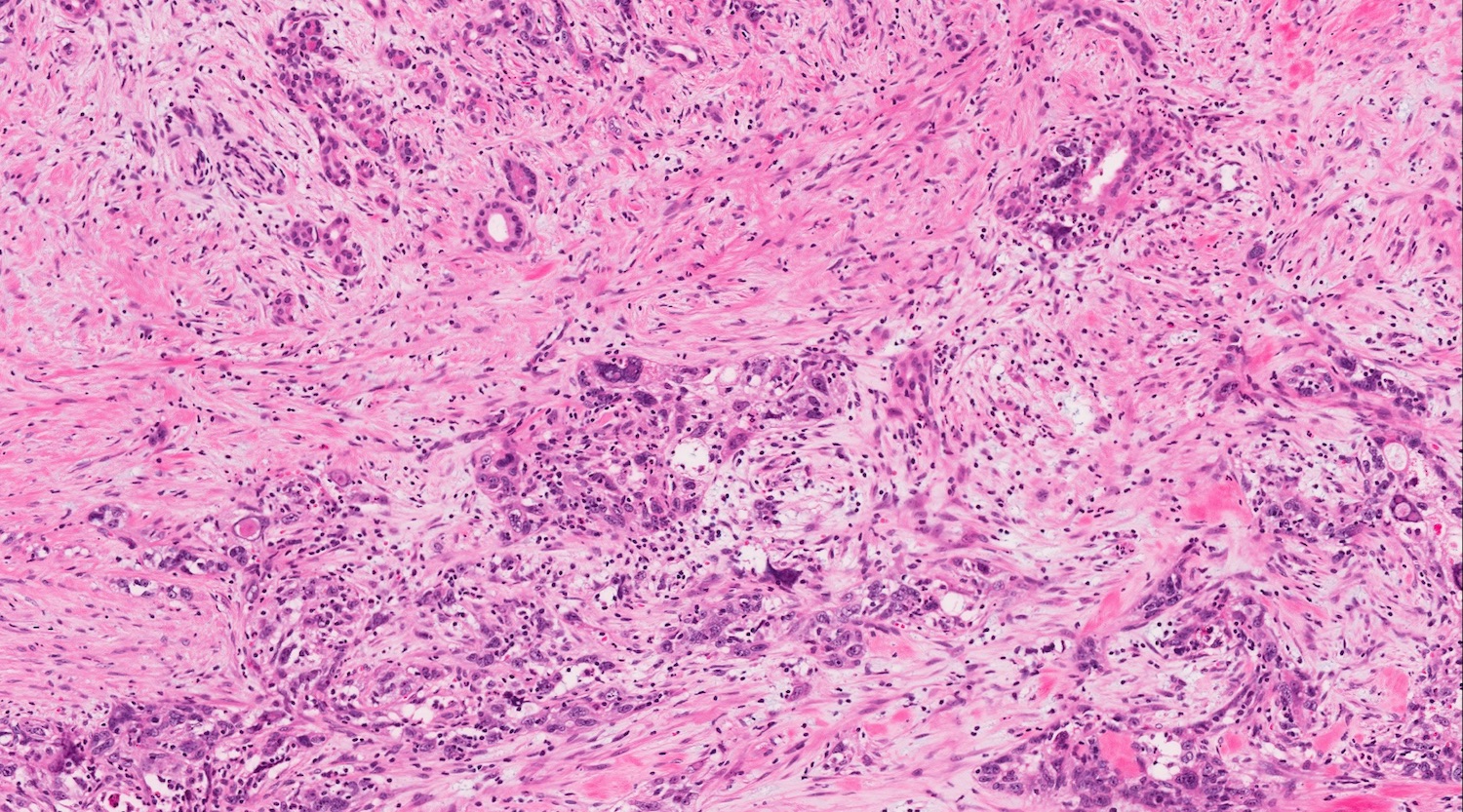
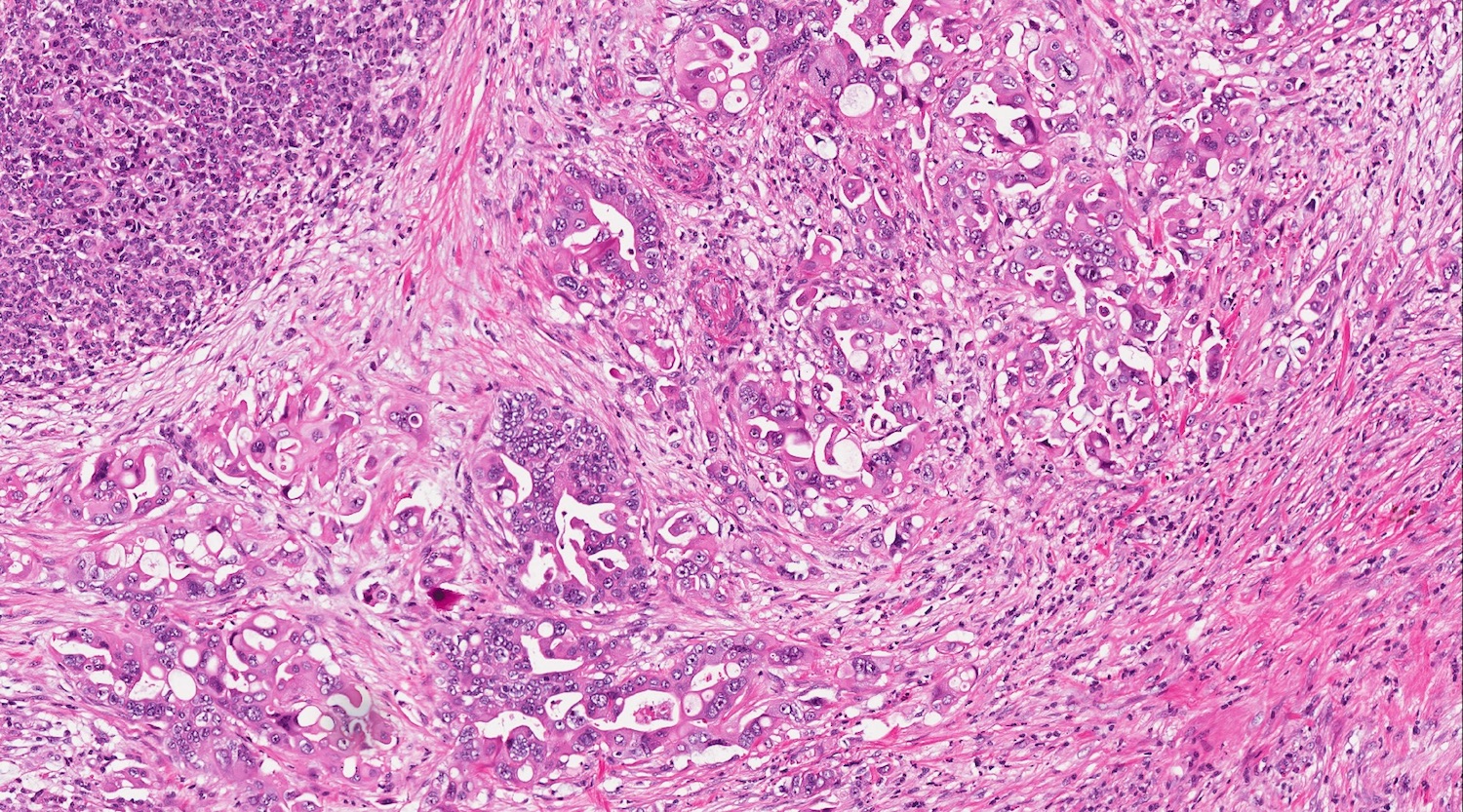
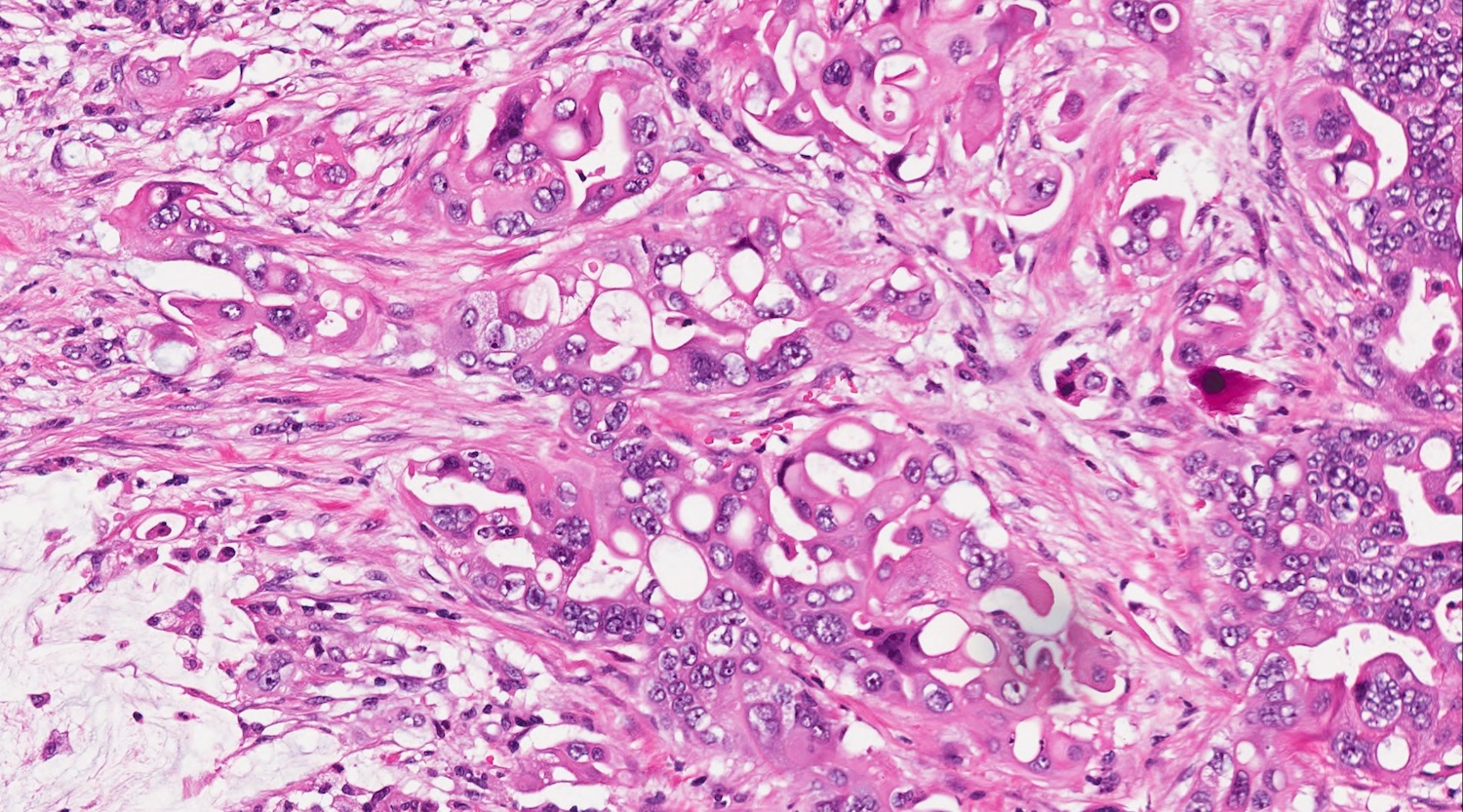
Anaplastic undifferentiated carcinoma
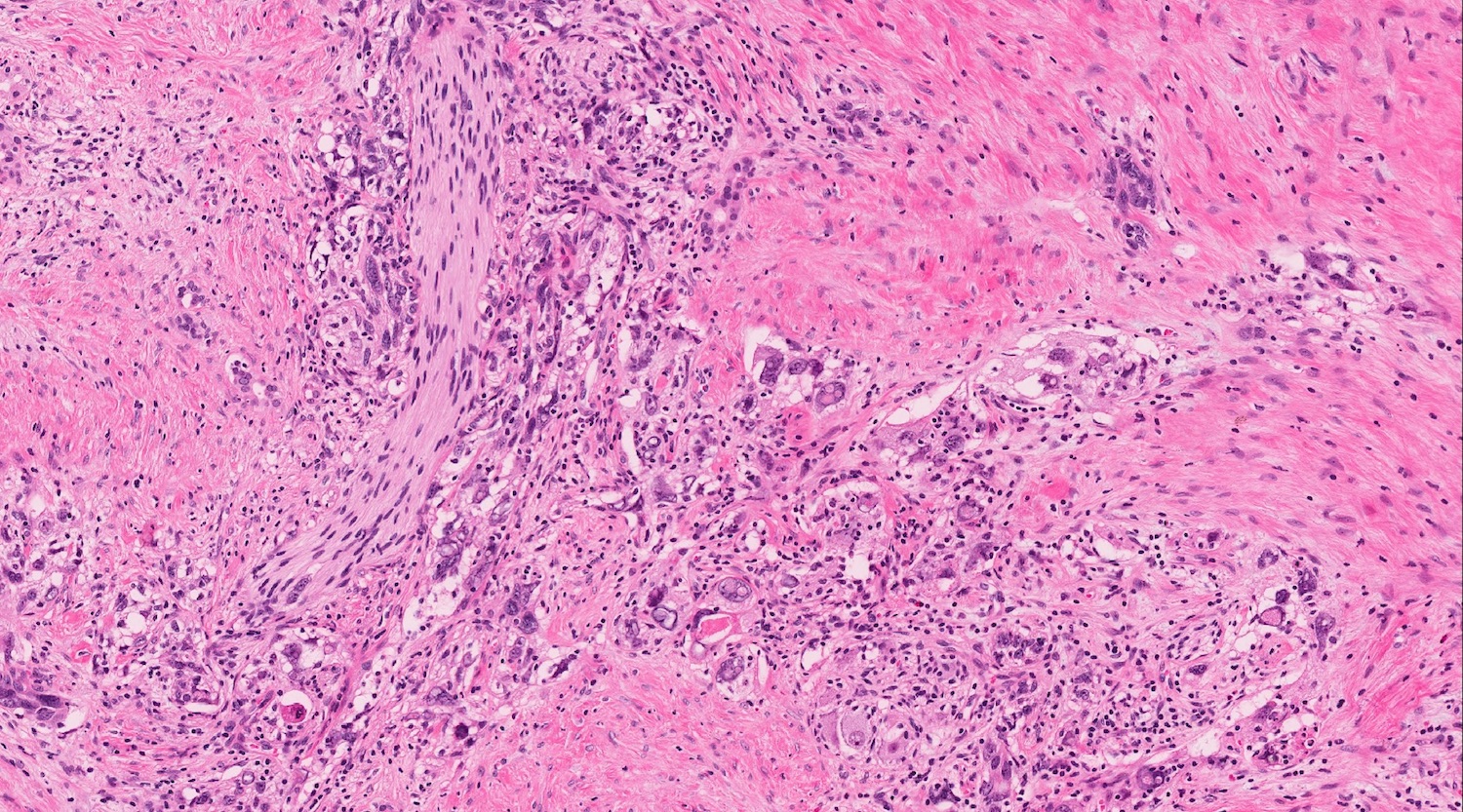
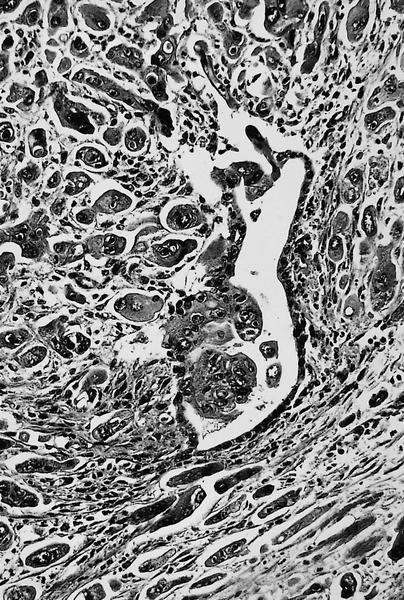
Massive perineural invasion
Massive vascular invasion
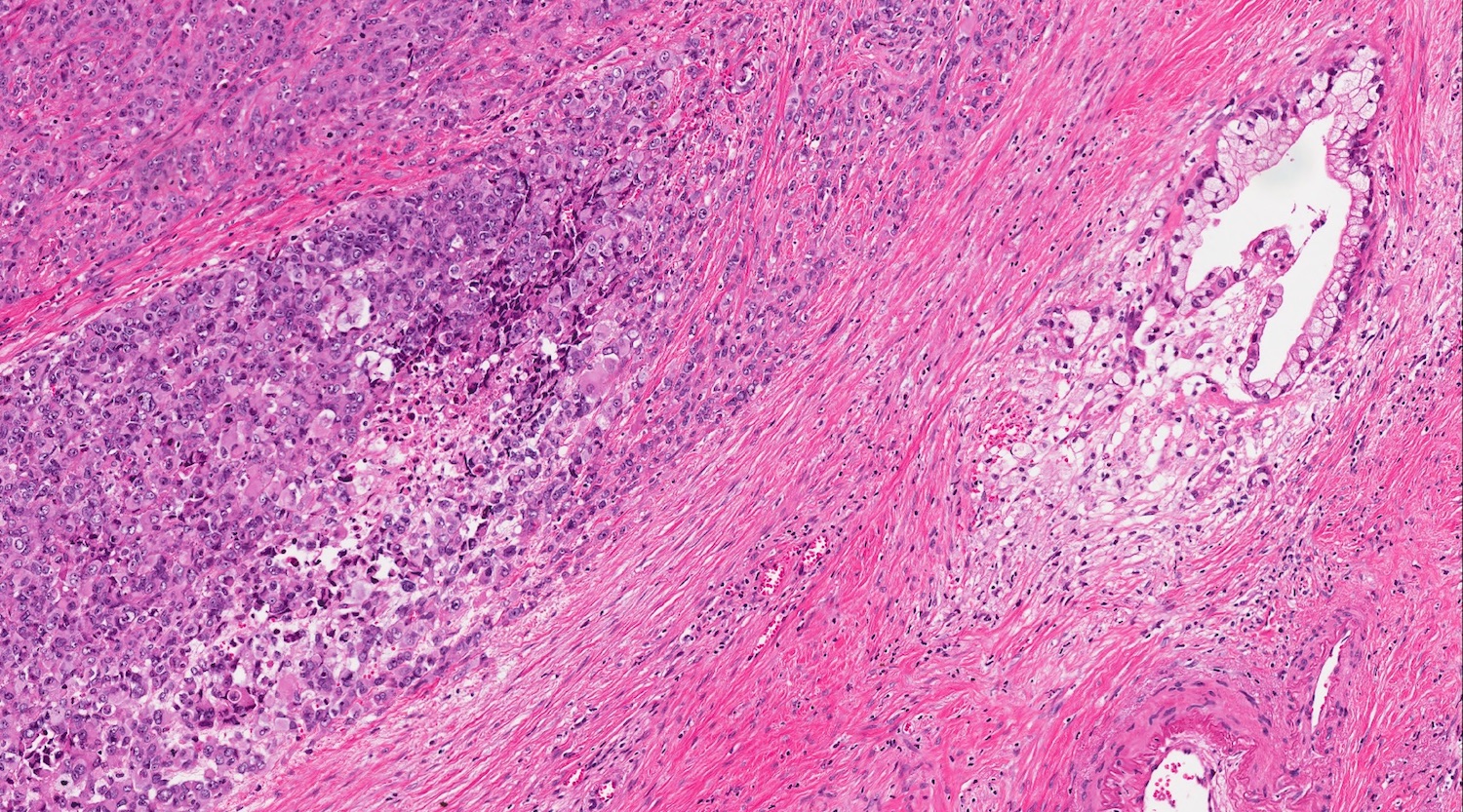
Association with ductal adenocarcinoma
Invasion of duodenum
Rhabdoid aspects
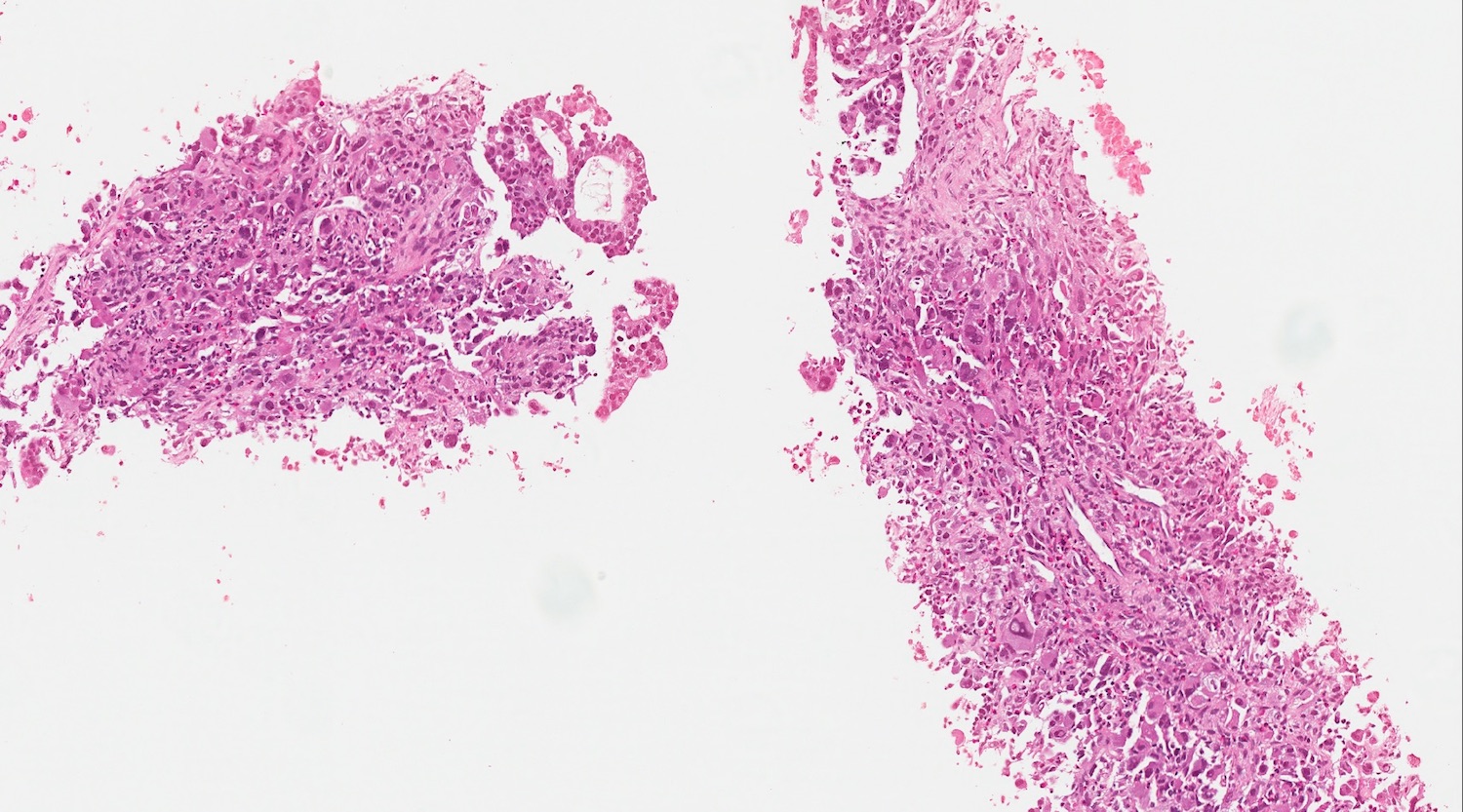
Biopsy
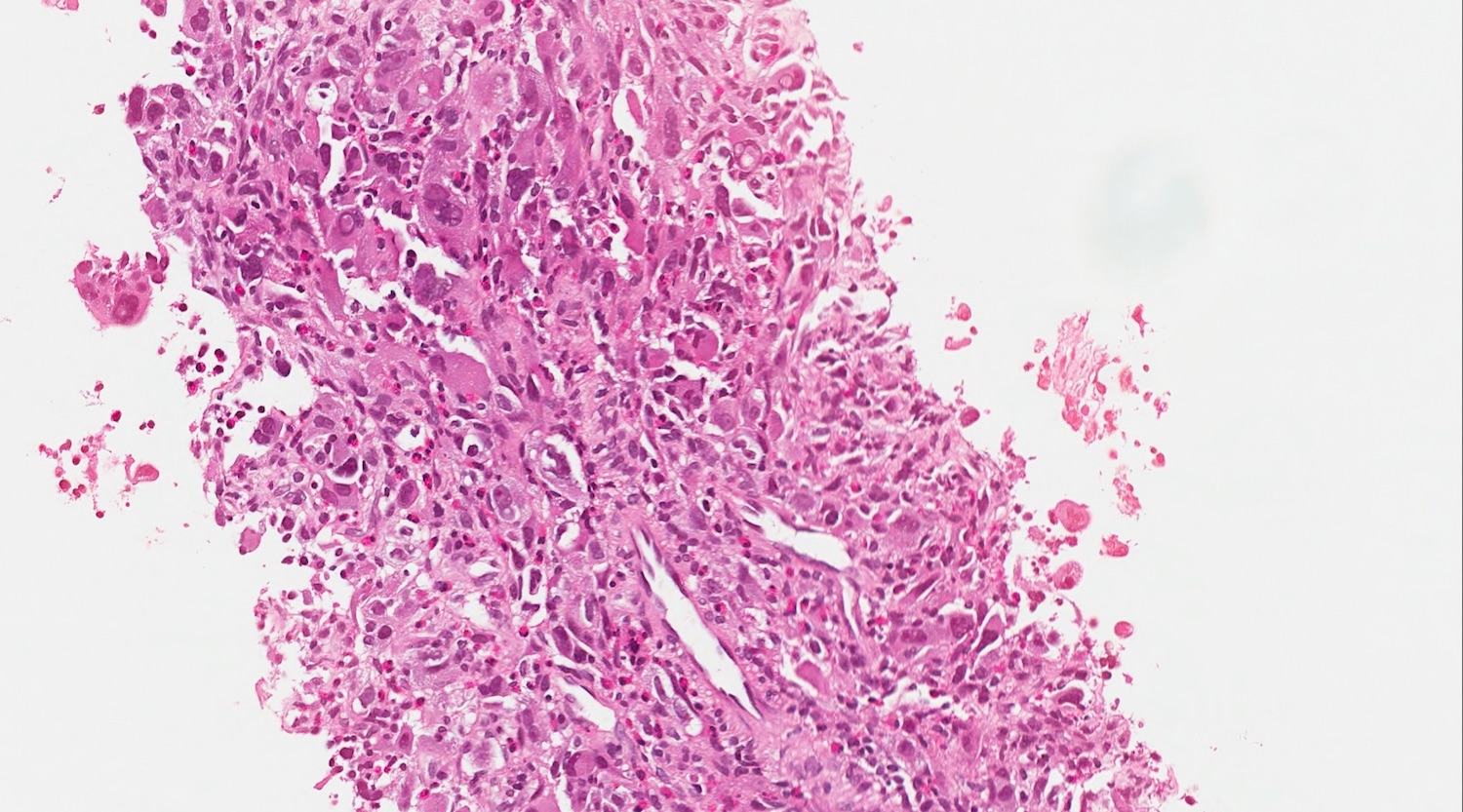
Details on biopsy
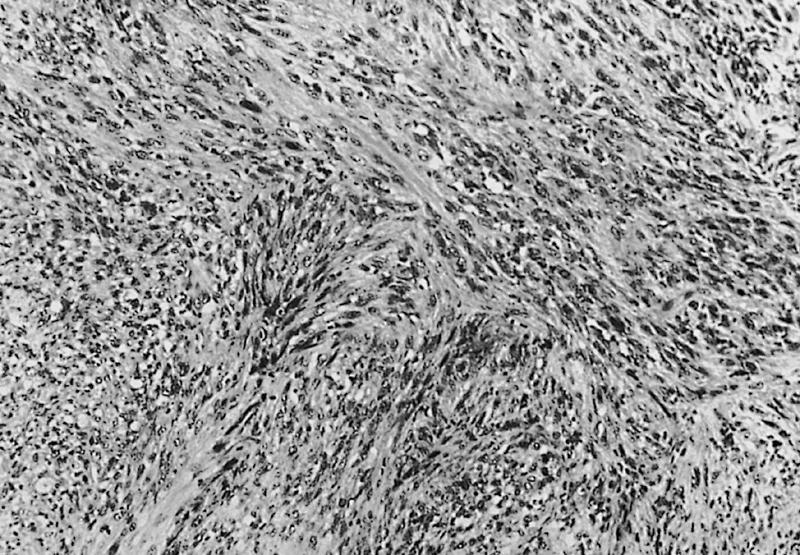

Spindle cell sarcomatoid features
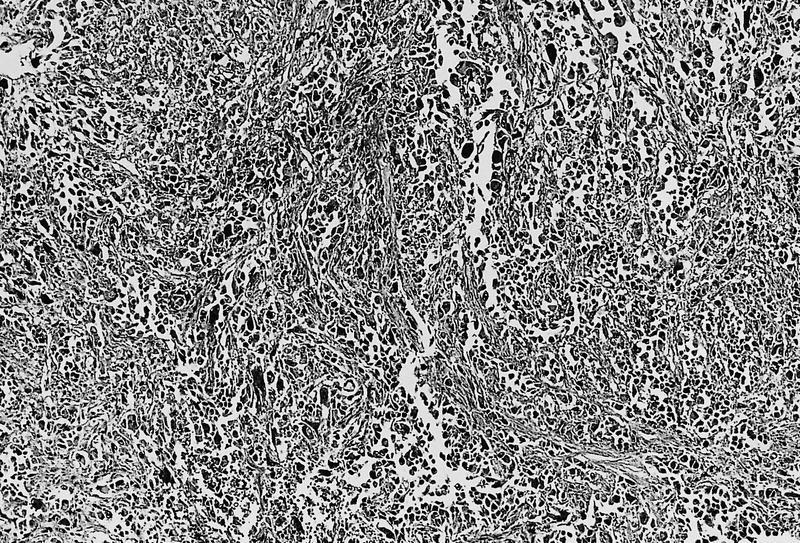
Pleomorphic large cells
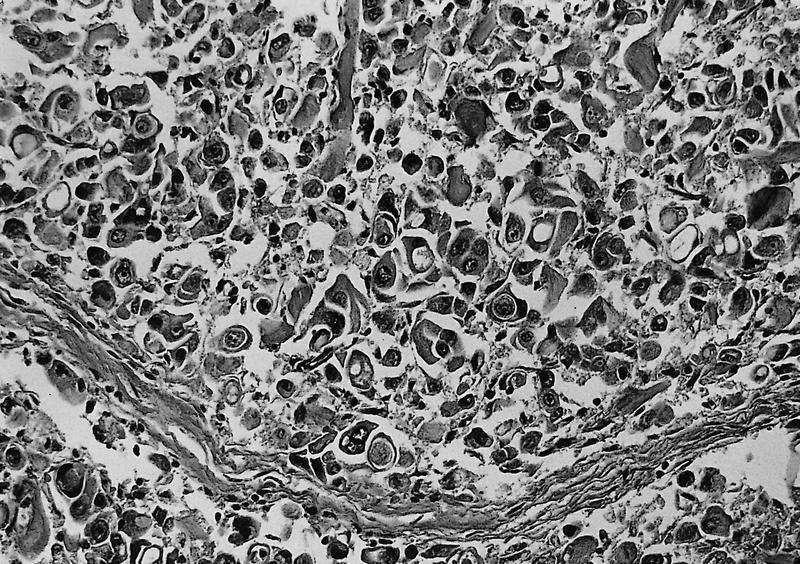
Engulfment of red blood cells
Glandular differentiation
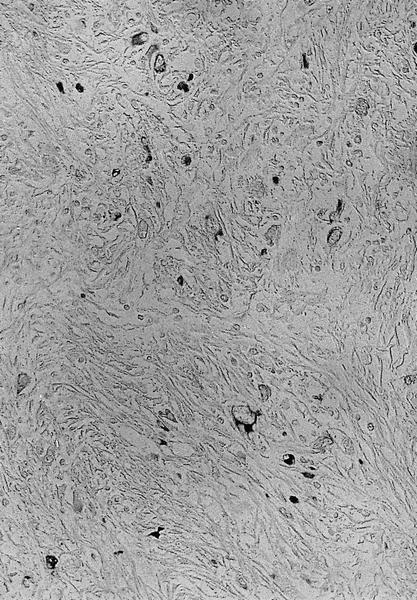
Tumor is keratin+
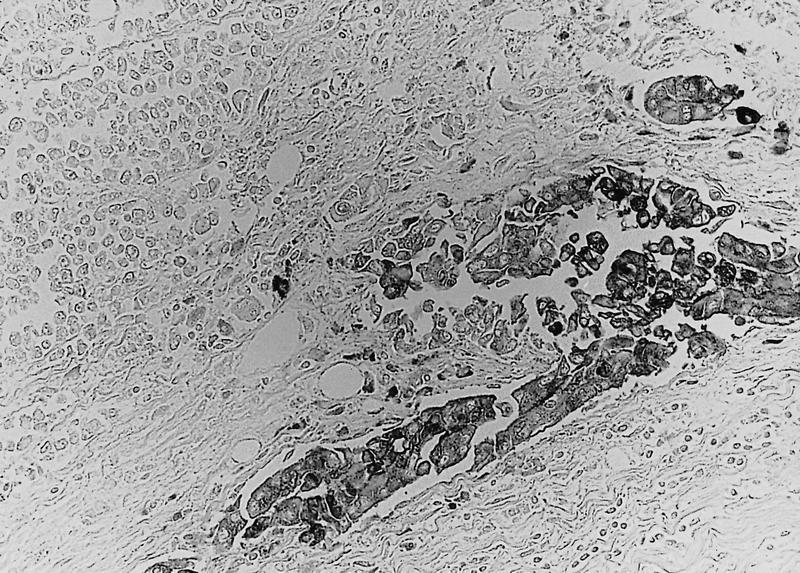
Tumor is CEA+ in glandular portions
Cytology description
- Hypercellular neoplasm: presence of highly atypical cells
Negative stains
- Neoplastic cells are negative for E-cadherin
- ~50% of undifferentiated rhabdoid carcinomas typically present a nuclear loss of SMARCB1 / INI1 at immunohistochemistry (J Gastrointest Oncol 2021;12:874, Mod Pathol 2015;28:248)
Molecular / cytogenetics description
- Overlaps with the genetic profile of conventional ductal adenocarcinoma
- In the rhabdoid variant, KRAS alterations and SMARCB1 expression status define 2 subtypes, with possible translational implications (Mod Pathol 2015;28:248)
- There is an enrichment in KRAS amplification in both rhabdoid and sarcomatoid variants, if compared with conventional ductal adenocarcinoma (Mod Pathol 2015;28:248, Hum Pathol 2022;128:124)
- SMAD4 alterations appear as a rare molecular event in the sarcomatoid variant, if compared with conventional ductal adenocarcinoma (Hum Pathol 2022;128:124)
Sample pathology report
- Pancreas, pancreatectomy:
- Pancreatic undifferentiated carcinoma
- Pancreas, biopsy / cytology:
- Pancreatic undifferentiated carcinoma (see comment)
- Comment: Cellular neoplasm with highly atypical cells is consistent with undifferentiated carcinoma of the pancreas.
- Surgical resection: percentage of the undifferentiated component; infiltration, if any, of duodenum, common bile duct, neck margin, intestinal margin and retroperitoneal margin if Whipple resection, spleen and pancreatic margin if distal pancreatectomy; vascular / perineural invasion if any; nodal metastasis (if any); pTNM staging.
Differential diagnosis
- Undifferentiated carcinoma of the pancreas with osteoclast-like giant cells:
- Presence of osteoclast-like giant cells
- Sarcoma:
- Keratin is negative
- Melanoma:
Additional references
Board review style question #1
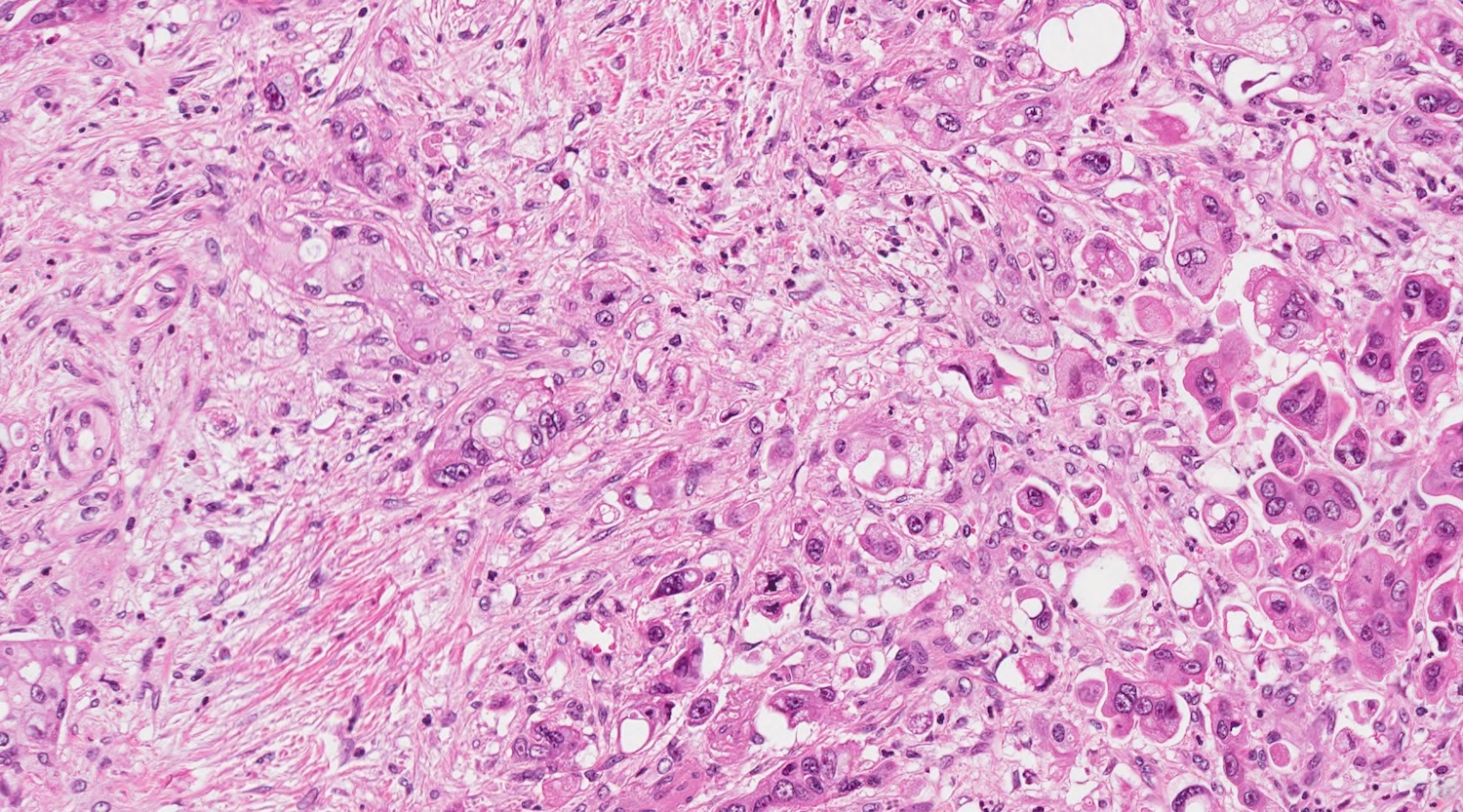
This is a high magnification field of a tumor within the pancreas. Can the diagnosis of undifferentiated carcinoma be made based on morphology only?
- No, electron microscopy must be used to rule out a melanoma
- No, immunohistochemistry is mandatory
- No, molecular analysis is mandatory
- No, special histochemical stains are mandatory
- Yes, morphology only is sufficient
Board review style answer #1
B. No, immunohistochemistry is mandatory. Morphology is the most important step for the diagnosis; however, immunohistochemistry for keratin and vimentin should be performed in most cases to rule out sarcoma, melanoma and metastasis. This is particularly true for undifferentiated carcinoma with sarcomatoid features, to avoid misdiagnosis with sarcomas and for anaplastic type, to rule out melanoma or metastases.
Comment Here
Reference: Undifferentiated carcinoma
Comment Here
Reference: Undifferentiated carcinoma
Board review style question #2
How do the fibrosis and desmoplastic reactions seen in conventional ductal adenocarcinoma of the pancreas compare to that of undifferentiated carcinoma?
- Conventional ductal adenocarcinoma typically has more fibrosis and desmoplasia
- Only anaplastic type undifferentiated carcinoma shows more fibrosis / desmoplasia than conventional ductal adenocarcinoma
- There is always more fibrosis in undifferentiated carcinoma
- There is the same quantity of fibrosis in both diagnoses
- They are highly variable in both diagnoses
Board review style answer #2
A. Conventional ductal adenocarcinoma usually has much more fibrosis / desmoplasia than undifferentiated carcinoma. This is a major point in the differential diagnosis between the 2 diagnoses.
Comment Here
Reference: Undifferentiated carcinoma
Comment Here
Reference: Undifferentiated carcinoma
