
Pancreas
Exocrine carcinomas
Molecular genetics of pancreatic ductal carcinoma
Author: Claudio Luchini, M.D., Ph.D.
Editorial Board Member: Catherine E. Hagen, M.D.
Deputy Editor-in-Chief: Raul S. Gonzalez, M.D.

Last author update: 22 December 2020
Last staff update: 6 December 2024
Copyright: 2020-2025, PathologyOutlines.com, Inc.
PubMed Search: Molecular genetics of pancreatic ductal carcinoma


Table of Contents
Definition / general | Essential features | Somatic mutations | Germline mutations / genetic syndromes | Transcriptomic subtypes | Other relevant genetic alterations | Clinical features | Prognostic factors | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Luchini C. Molecular genetics of pancreatic ductal carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/pancreasmolecularaspects.html. Accessed April 2nd, 2025.
Definition / general
- Pancreatic ductal adenocarcinoma (PDAC) is the most common type of pancreatic cancer, representing > 90% of all pancreatic malignancies
- From a genetic point of view, PDAC is a complex disease with several genes altered through different mechanisms, which include point mutations, chromosomal aberrations and epigenetic changes
Essential features
- Somatic mutations affect, above all, four genes: KRAS, which is an oncogene and TP53, CDKN2A and SMAD4, which are tumor suppressor genes (Lancet 2016;388:73)
- A subset of pancreatic cancer arises in the background of genetic syndromes with germline mutations affecting different genes, such as CDKN2A, TP53, STK11, BRCA1 / 2, ATM and MMR (J Clin Oncol 2017;35:3382)
- Transcriptomic profile divides pancreatic cancer into different groups; among them, the most important distinction involves the identification of the so called squamous subtype, which has the worst prognosis (Nature 2016;531:47)
- Only a few molecular alterations have a predictive value in pancreatic cancer
- BRCA mutated tumors show a good response to platinum based therapy and to poly ADP ribose polymerase (PARP) inhibitors; tumors with microsatellite instability can be treated with immunotherapy (N Engl J Med 2019;381:317, J Clin Oncol 2020;38:1)
Somatic mutations
- Four genes are the most commonly mutated in PDAC: KRAS, which is an oncogene and TP53, CDKN2A and SMAD4, which are tumor suppressor genes (Lancet 2016;388:73)
- KRAS
- Most frequently mutated gene in PDAC (90 - 92% of cases)
- Oncogene
- Located on chromosome 12
- Downstream pathways: MAPK and PI3K
- TP53
- Mutated in 50 - 60% of PDAC
- Tumor suppressor gene
- Located on chromosome 17
- Encodes for P53, a crucial protein that controls cell growth, metabolism, senescence, DNA repair and apoptosis
- CDKN2A
- Mutated in > 60% of PDAC
- Tumor suppressor gene
- Located on chromosome 9
- Encodes for P16, a protein encoded that acts as a mediator of the retinoblastoma signaling pathway
- SMAD4
- Mutated in 30 - 55% of PDAC
- Tumor suppressor gene
- Located on chromosome 18
- Protein encoded by SMAD4 is an effector of the transforming growth factor (TGF) β signaling pathway
- KRAS
- In addition to these four main genetic drivers, other important genes can be altered by somatic mutations in PDAC with a lower but significant prevalence (Lancet 2016;388:73, Gastroenterology 2019;156:2242):
- ARID1A (AT rich interaction domain 1A, 5 - 10% of cases), a tumor suppressor located on chromosome 3 involved in chromatin remodeling
- BRCA1 (breast cancer gene-1, up to 2% of cases) and BRCA2 (breast cancer gene-2, up to 7% of cases) are tumor suppressor genes located on chromosome 17 and 13, respectively, involved in the process of homologous recombination repair pathway
- BRAF (B-Raf proto-oncogene, up to 2% of cases), an oncogene located on chromosome 7, involved in MAPK pathway and with mutations that are almost always mutually exclusive with those affecting KRAS
- GNAS (guanine nucleotide binding protein, alpha stimulating activity polypeptide) is an oncogene located on chromosome 20; is typically mutated in the case of a cancer derived from an intraductal papillary mucinous neoplasm (IPMN)
Germline mutations / genetic syndromes
- A subset of pancreatic cancer arises in the background of genetic syndromes with germline mutations most commonly affecting the following genes
(J Clin Oncol 2017;35:3382, Ann Gastroenterol Surg 2020;4:229):
- CDKN2A: germline mutations of this gene characterize the familial atypical multiple mole melanoma (FAMMM) syndrome, an autosomal dominant syndrome in which the cumulative risk for PDAC development is up to 15%
- TP53: germline mutations of this gene characterize the Li-Fraumeni syndrome, an autosomal dominant syndrome in which the cumulative risk for PDAC development is up to 5%
- BRCA1 / 2 and PALB2: germline mutations of these genes characterize the hereditary breast and ovarian cancer syndrome, an autosomal dominant syndrome in which the cumulative risk for PDAC development is up to 7%
- ATM: germline mutations of this gene characterize the ataxia telangiectasia, familial breast cancer syndrome, an autosomal recessive syndrome in which the cumulative risk for PDAC development is up to 5%
- MMR genes: germline mutations of these genes characterize Lynch syndrome, an autosomal dominant syndrome in which the cumulative risk for PDAC development is up to 9%
- STK11: germline mutations of this gene characterize the Peutz-Jeghers syndrome, an autosomal dominant syndrome in which the cumulative risk for PDAC development is up to 30%
- PRSS1 and SPINK1: germline mutations of these gene characterize the hereditary pancreatitis syndrome through an autosomal dominant (PRSS1) or recessive (SPINK1) inheritance, in which the cumulative risk for PDAC development is up to 50%
- CFTR: germline mutations of this gene characterize the cystic fibrosis syndrome, an autosomal recessive syndrome in which the cumulative risk for PDAC development is up to 5%
Transcriptomic subtypes
- Different studies have tried to address transcriptomic profiles and, along this line, the most reliable classification indicates the following four categories (Nat Med 2011;17:500, Nature 2016;531:47):
- Squamous subtype: characterized by a strong upregulation of TP63 and downregulation of GATA6; such tumors show the worst prognosis
- Pancreatic progenitor subtype: expresses transcriptional networks involving PDX1, FOXA2 and FOXA3, crucial for pancreatic cell fate determination
- Aberrantly differentiated endocrine exocrine (ADEX) subtype: expresses transcriptional networks crucial for more advanced stage of normal pancreatic differentiation
- Immunogenic subtype: correlates with a marked immune infiltrate, mainly B and T cells, with upregulation of immune checkpoints CTLA4 and PD1, suggesting a possible role for immunotherapy drugs in this tumor subtype
Other relevant genetic alterations
- Microsatellite instability (MSI): a genetic condition due to mutations of the mismatch repair (MMR) genes, leading to a hypermutated phenotype with mutations clustered in specific regions known as microsatellites (Ann Oncol 2019;30:1232)
- POLE mutation: a rare occurrence in pancreatic cancer associated with an ultra hypermutated phenotype due to mutations affecting polymerase ε; associated with prolonged survival (Pancreas 2020;49:999)
- Kinase fusion genes: genetic alterations present in KRAS wild type pancreatic cancer; the genes most commonly involved are FGFR2, RAF, ALK, RET, MET and NTRK1 (Gastroenterology 2019;156:2242)
Clinical features
- Some genetic alterations have been recently associated with specific clinical features (Gastroenterology 2019;156:2242):
- Mutations in KRAS, SMAD4 are more frequent in older patients (≥ 50 years)
- Alterations in BRCA1 / 2 are more frequent in younger patients (< 50 years)
- Mutations in KRAS, SMAD4 and CDKN2A are more frequent in female patients
- Mutations in GNAS and ATM are more frequent in male patients
Prognostic factors
- SMAD4 mutations are associated with more aggressive behavior and with a widespread metastasis pattern (J Clin Oncol 2009;27:1806)
- MSI tumors do not always have a more favorable prognosis, as in colorectal or gastric cancer (Gut 2020 Apr 29 [Epub ahead of print])
Treatment
- Tumors with germline BRCA mutations can be treated with platinum based therapy and with PARP inhibitors (N Engl J Med 2019;381:317)
- MSI tumors may be susceptible to immune checkpoint blockade (J Clin Oncol 2020;38:1)
- Cancer with ALK fusion may be treated with ALK inhibitors (J Natl Compr Canc Netw 2017;15:555)
Microscopic (histologic) description
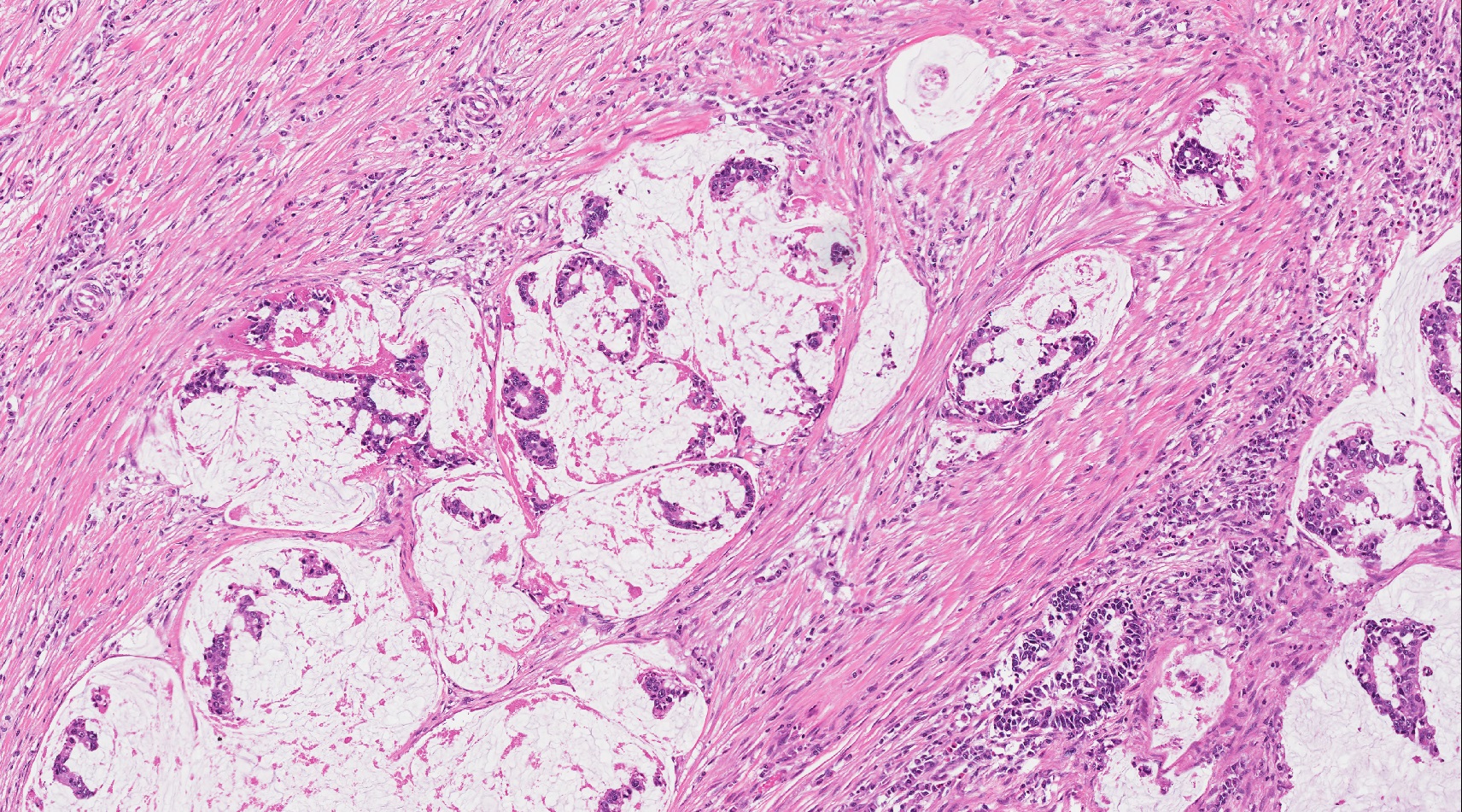
- MSI tumors more often show a medullary or colloid morphology (Gut 2020 Apr 29 [Epub ahead of print])
- Germline mutated ATM tumors more often show a mucinous / colloid histology (Mod Pathol 2019;32:1806)
- Tumors with squamous features show a very poor prognosis (Nat Med 2011;17:500, Nature 2016;531:47)
Microscopic (histologic) images
Contributed by Claudio Luchini, M.D., Ph.D.
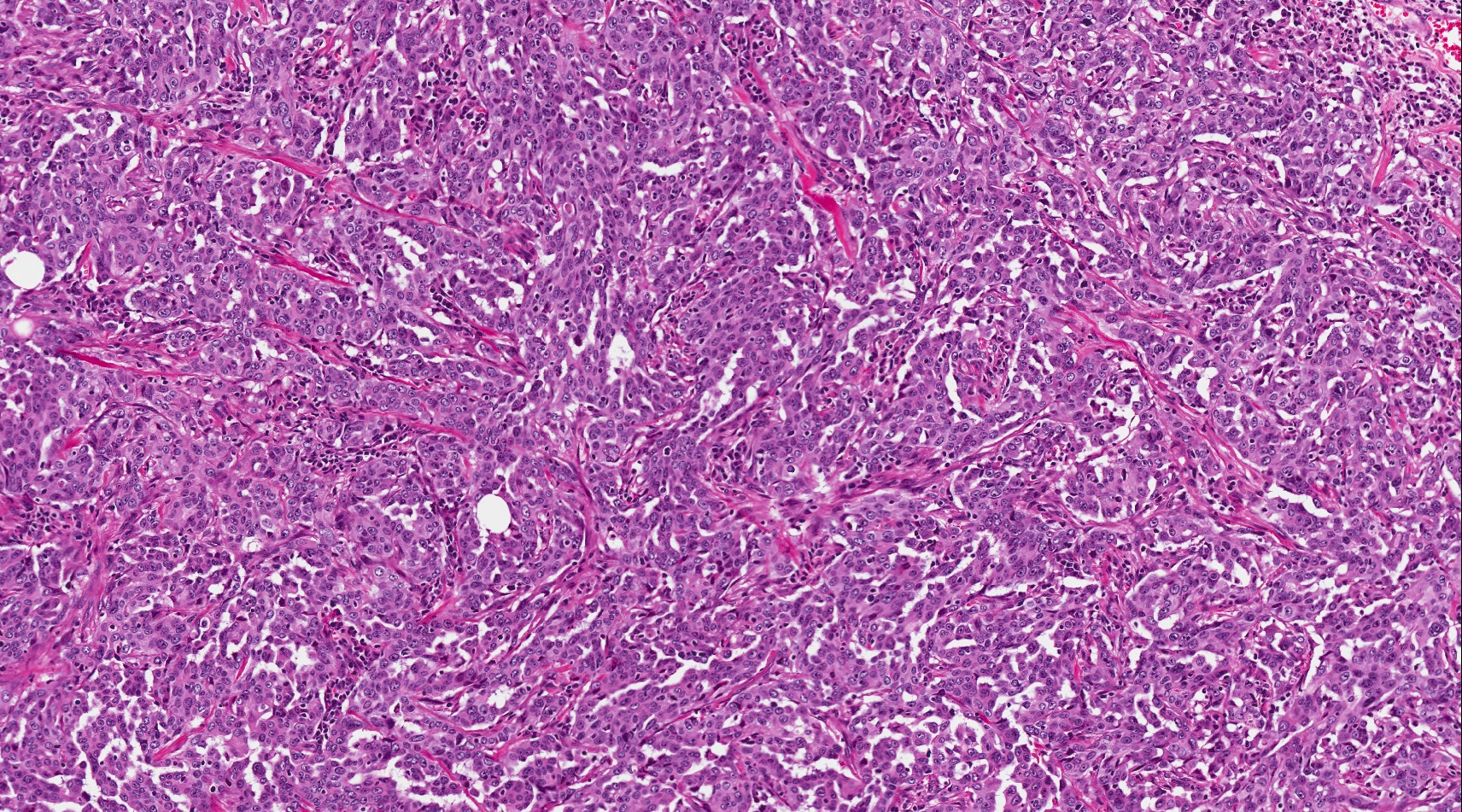
Medullary histology
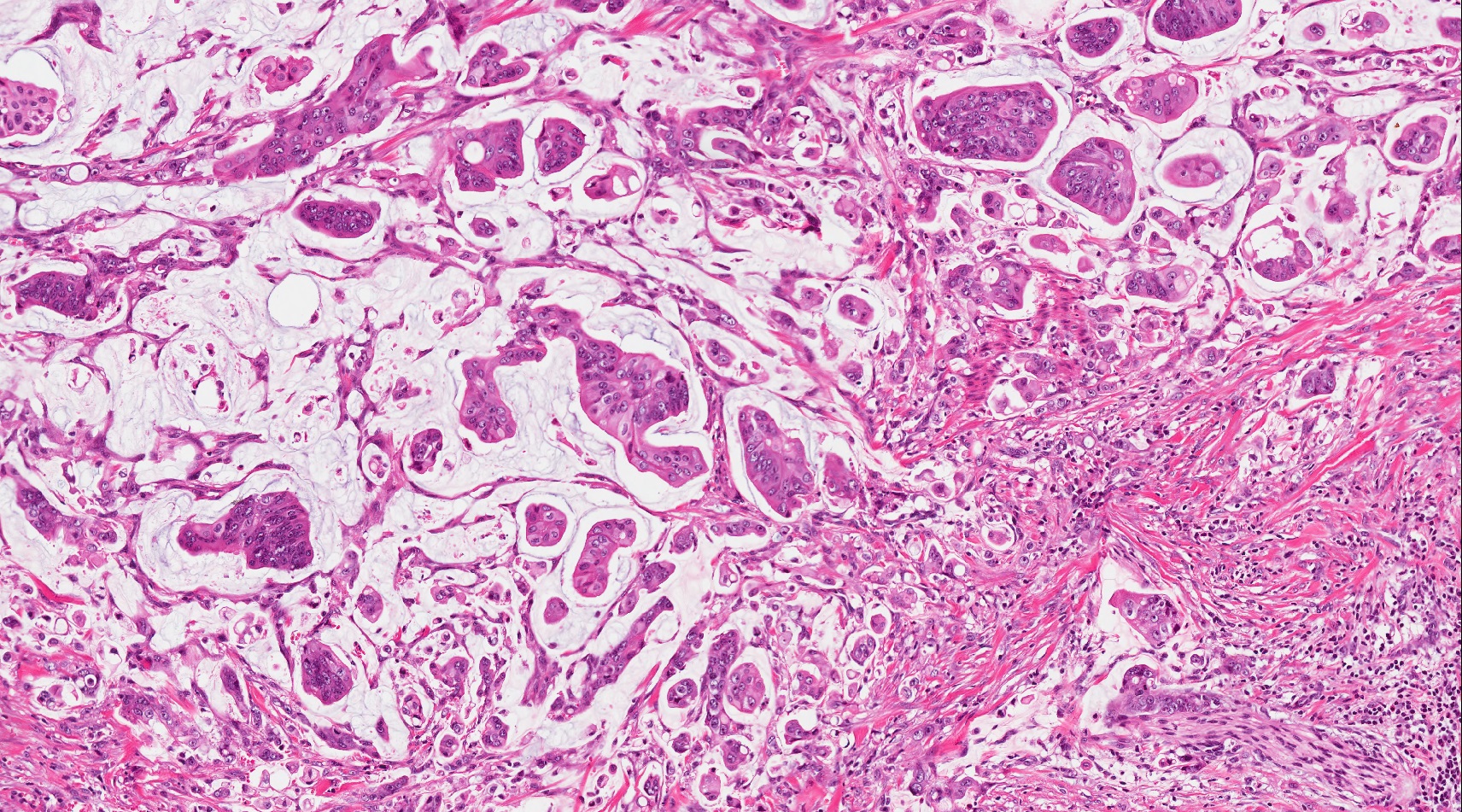
Mucinous colloid histology
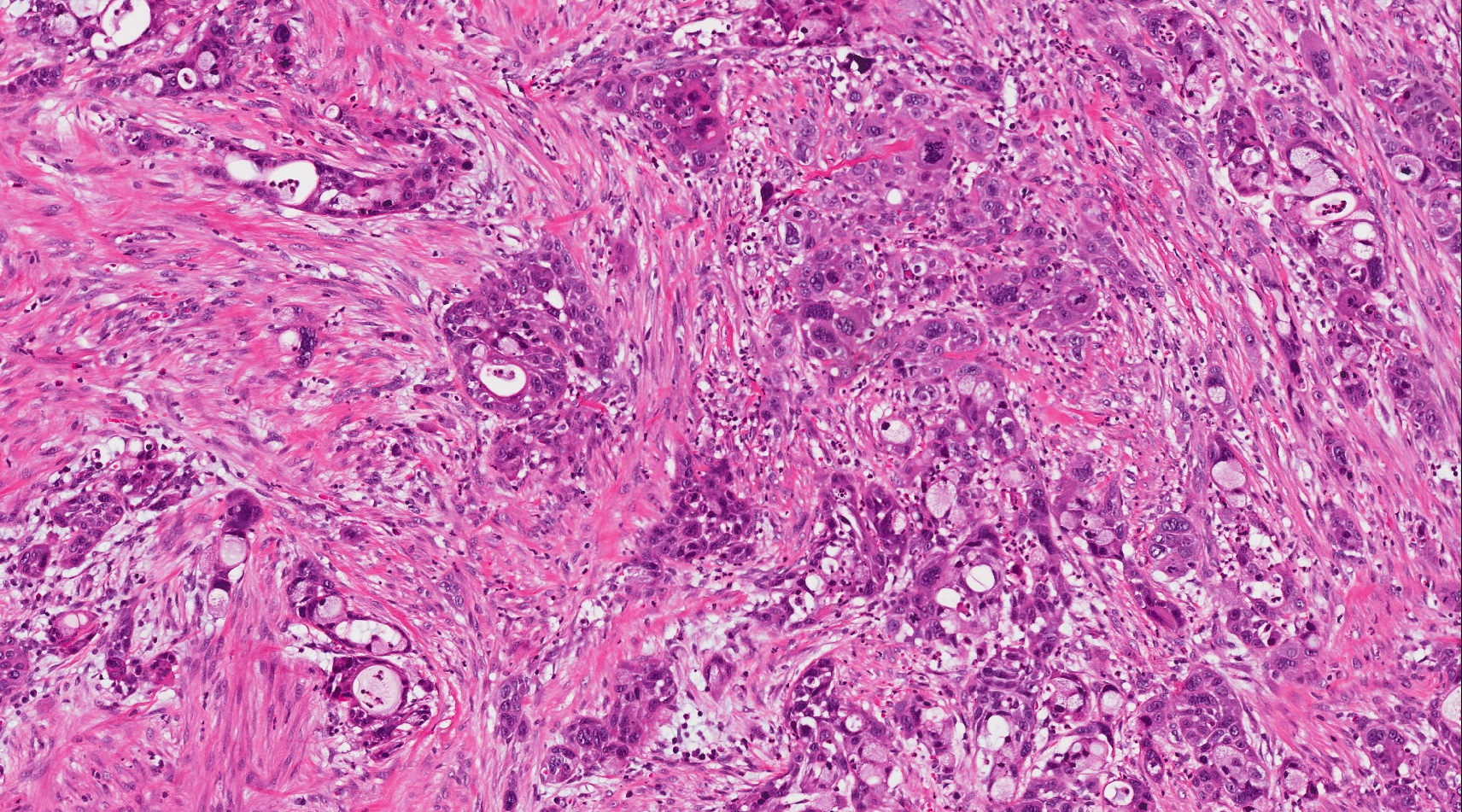
Adenosquamous histology
Board review style question #1
What is an important histologic characteristic associated with the genetic alteration of microsatellite instability in pancreatic cancer?
- Adenosquamous histology
- Hepatoid features
- Mucinous colloid histology
- Squamous histology
- Undifferentiated anaplastic histology
Board review style answer #1
C. Mucinous colloid histology is a classic histology encountered in MSI pancreatic cancer.
Comment Here
Reference: Molecular genetics of pancreatic ductal carcinoma
Comment Here
Reference: Molecular genetics of pancreatic ductal carcinoma
Board review style question #2
Which is the most important and frequently mutated gene in pancreatic ductal adenocarcinoma?
- ARID1A
- CDKN2A
- KRAS
- SMAD4
- TP53
Board review style answer #2
C. KRAS is the most important and frequent mutated gene in pancreatic ductal adenocarcinoma.
Comment Here
Reference: Molecular genetics of pancreatic ductal carcinoma
Comment Here
Reference: Molecular genetics of pancreatic ductal carcinoma
