

Pancreas
Acinar cell lesions
Acinar cell carcinoma
Author: Claudio Luchini, M.D., Ph.D.
Editorial Board Member: Aaron R. Huber, D.O.
Deputy Editor-in-Chief: Catherine E. Hagen, M.D.

Last author update: 1 October 2021
Last staff update: 1 October 2021
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Acinar cell carcinoma[TI] pancreas[TIAB] free full text[sb]

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Luchini C. Acinar cell carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/pancreasacinar.html. Accessed December 22nd, 2024.
Definition / general
- Malignant exocrine neoplasm of the pancreas composed of cells with morphological resemblance to acinar cells and with immunohistochemistry positive for acinar markers
Essential features
- Epithelial neoplasm showing acinar differentiation
- Immunohistochemical positivity for BCL10 and trypsin (Virchows Arch 2009;454:133, Cancer Cytopathol 2013;121:459, Pathologica 2020;112:210)
Terminology
- Main category: acinar cell carcinoma
- Subtypes: acinar cell cystoadenocarcinoma, mixed acinar neuroendocrine carcinoma, mixed acinar ductal adenocarcinoma
ICD coding
- ICD-O: 8550/3 - acinar cell carcinoma
- ICD-11: 2C10.0 & XH3PG9 - adenocarcinoma of the pancreas & acinar cell carcinoma
Epidemiology
- M:F = 2.1:1 (Semin Diagn Pathol 2016;33:307, Am J Surg Pathol 2012;36:1782)
- Average age: 60 years (Semin Diagn Pathol 2016;33:307)
- 1 - 2% of all pancreatic neoplasms in adults and 15% in children (Semin Diagn Pathol 2016;33:307)
Sites
- Head of the pancreas is the most common site (Semin Diagn Pathol 2016;33:307)
Pathophysiology
- Accumulation of genetic alteration, including chromosomal instability and frequent allelic copy number variation
Etiology
- Tobacco smoking, defective DNA repair; presence of chromosomal instability and frequent allelic copy number variation (Nat Commun 2017;8:1323)
- Most cases are sporadic but a minority (< 10%) are associated with Lynch syndrome, familial adenomatous polyposis syndrome and Carney complex
Clinical features
- Presenting symptoms include abdominal or back pain, weight loss, nausea, vomiting; jaundice is more rarely observed than in ductal adenocarcinoma (Am J Surg Pathol 1992;16:815)
- In the case of extensive metastatic disease, patients may show symptoms related to lipase hypersecretion, including subcutaneous fat necrosis (Front Med (Lausanne) 2015;2:41)
Diagnosis
- CT scan and MRI are the preferred imaging modality (J Belg Soc Radiol 2019;103:43)
- Diagnosis is by biopsy or surgical resection
Laboratory
- Rarely, patients can show increased levels of AFP, especially young patients (Hum Pathol 2000;31:938)
- Patients with metastatic disease can show elevated levels of serum lipase (World J Clin Cases 2020;8:5304)
Radiology description
- Typical CT and MRI features of pancreatic acinar cell carcinoma: relatively large mass with a well defined margin, exophytic growth and heterogeneous enhancement (J Belg Soc Radiol 2019;103:43)
Prognostic factors
- The prognosis is poor, with an average survival time of about 19 months (Semin Diagn Pathol 2016;33:307)
- To date, the TNM stage can be considered the only significant prognostic moderator (Am J Surg Pathol 2012;36:1782)
- Tumors with intraductal growth display a better prognosis than conventional acinar cell carcinomas (Am J Surg Pathol 2007;31:363)
Case reports
- 41 and 77 year old men presenting with acinar cell carcinoma extensively involving the pancreas (Medicine (Baltimore) 2017;96:e7904)
- 52 year old man with acinar cell carcinoma of the pancreas harboring BRCA2 germline mutation (Cancer Biol Ther 2019;20:949)
- 69 year old man with acinar cell carcinoma of the pancreas mixed with ductal adenocarcinoma (World J Surg Oncol 2020;18:238)
- 71 year old man with acinar cell carcinoma of the pancreas, with extension into the main pancreatic duct (Surg Case Rep 2021;7:90)
- 81 year old man with acinar cell carcinoma of the pancreas harboring NTRK fusion gene, with exceptional response to molecularly based target therapy (J Natl Compr Canc Netw 2021;19:10)
Treatment
- Surgical resection if possible, gemcitabine based chemotherapy / radiofrequency ablation, molecularly based target therapy in the case of actionable alterations (World J Clin Cases 2020;8:1241)
Gross description
- Well circumscribed mass, at least partially encapsulated, solid and large, with fleshy consistency
Gross images
AFIP images
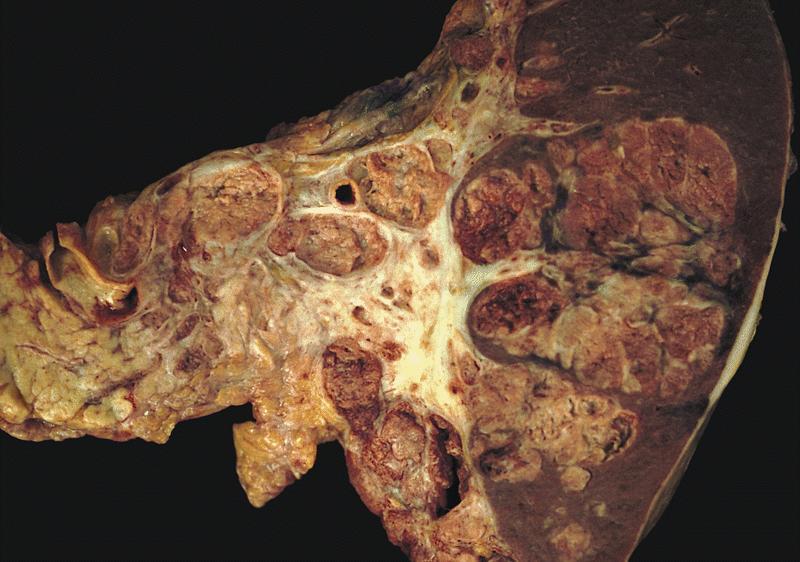
Cut surface displays large nodules
Frozen section description
- Hypercellular neoplasm with acinar resembling cells
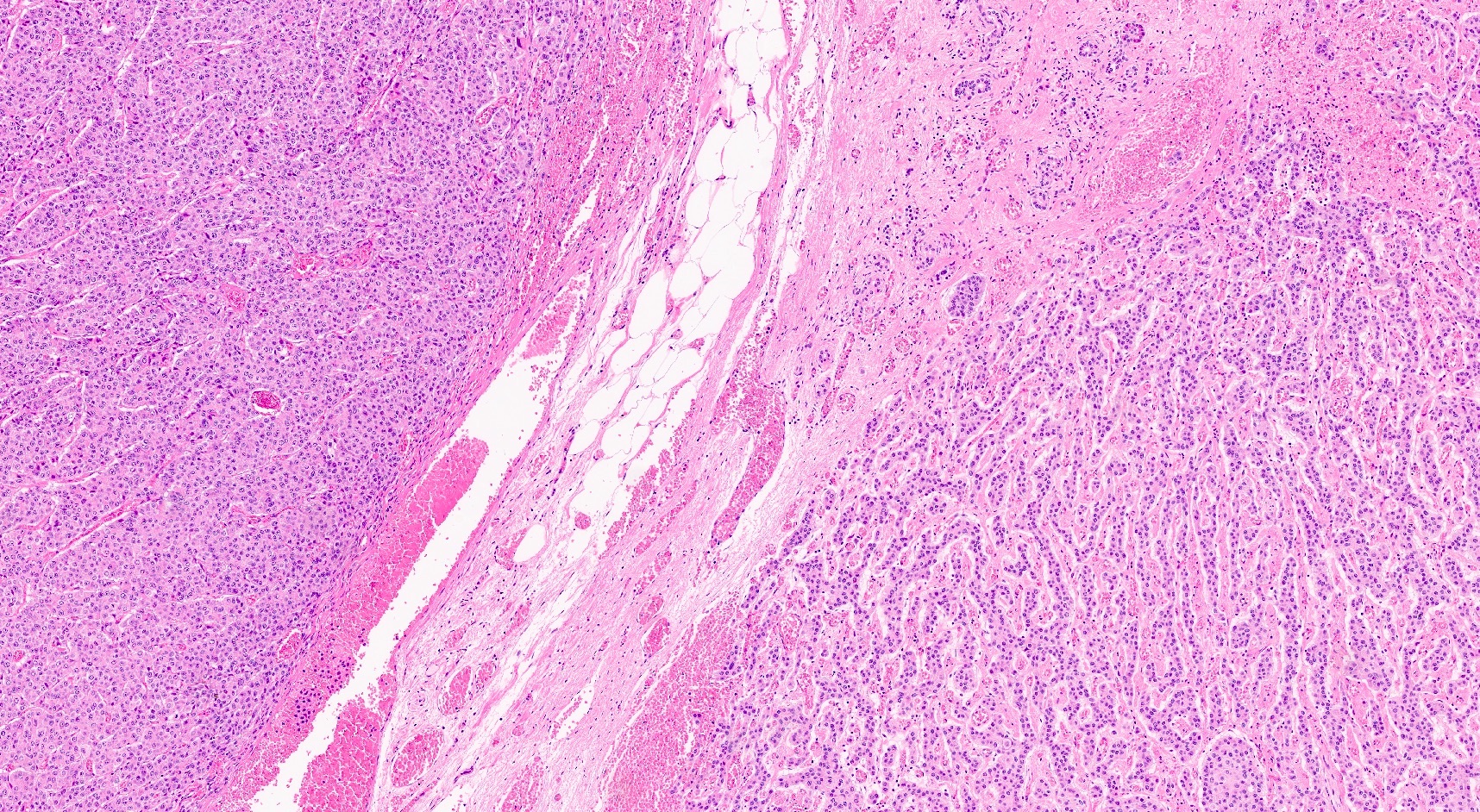
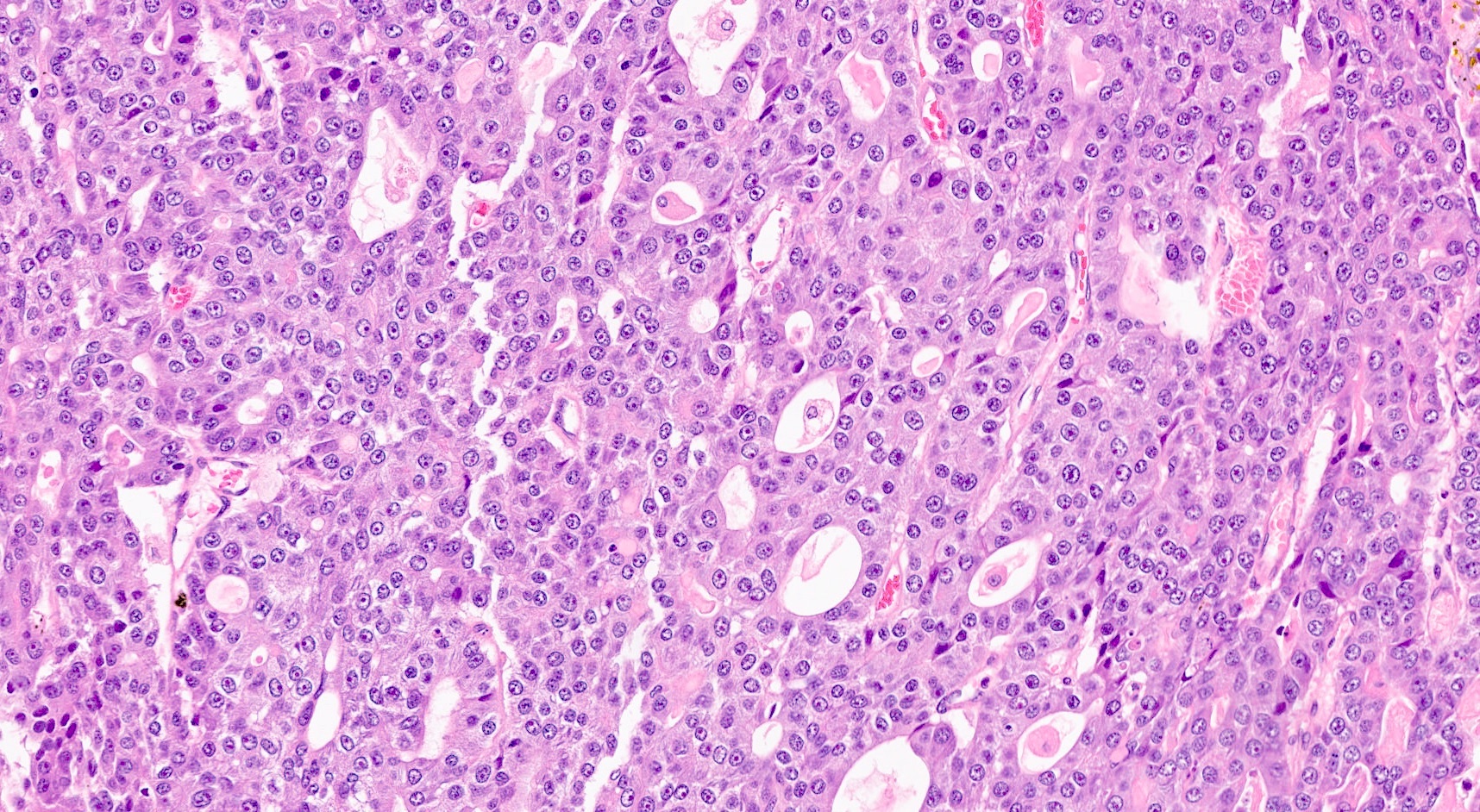
Microscopic (histologic) description
- Unlike conventional ductal adenocarcinoma, this tumor is highly cellular and with scant fibrous stroma
- Cells show moderate amounts of granular eosinophilic cytoplasm containing PAS positive diastase resistant zymogen granules
- Nuclei are uniform with a typically present, single and prominent nucleolus (Semin Diagn Pathol 2016;33:307)
- Perineural invasion and vascular invasion are very common
- Can have different architectures and growth patterns, including cystic, acinar, glandular and intraductal
- Nonneuroendocrine component of mixed neuroendocrine nonneuroendocrine neoplasms (MiNEN) in the pancreas can be represented by acinar cell carcinoma; MiNEN diagnosis should be based on both morphology and immunohistochemistry
Microscopic (histologic) images
Contributed by Claudio Luchini, M.D., Ph.D.
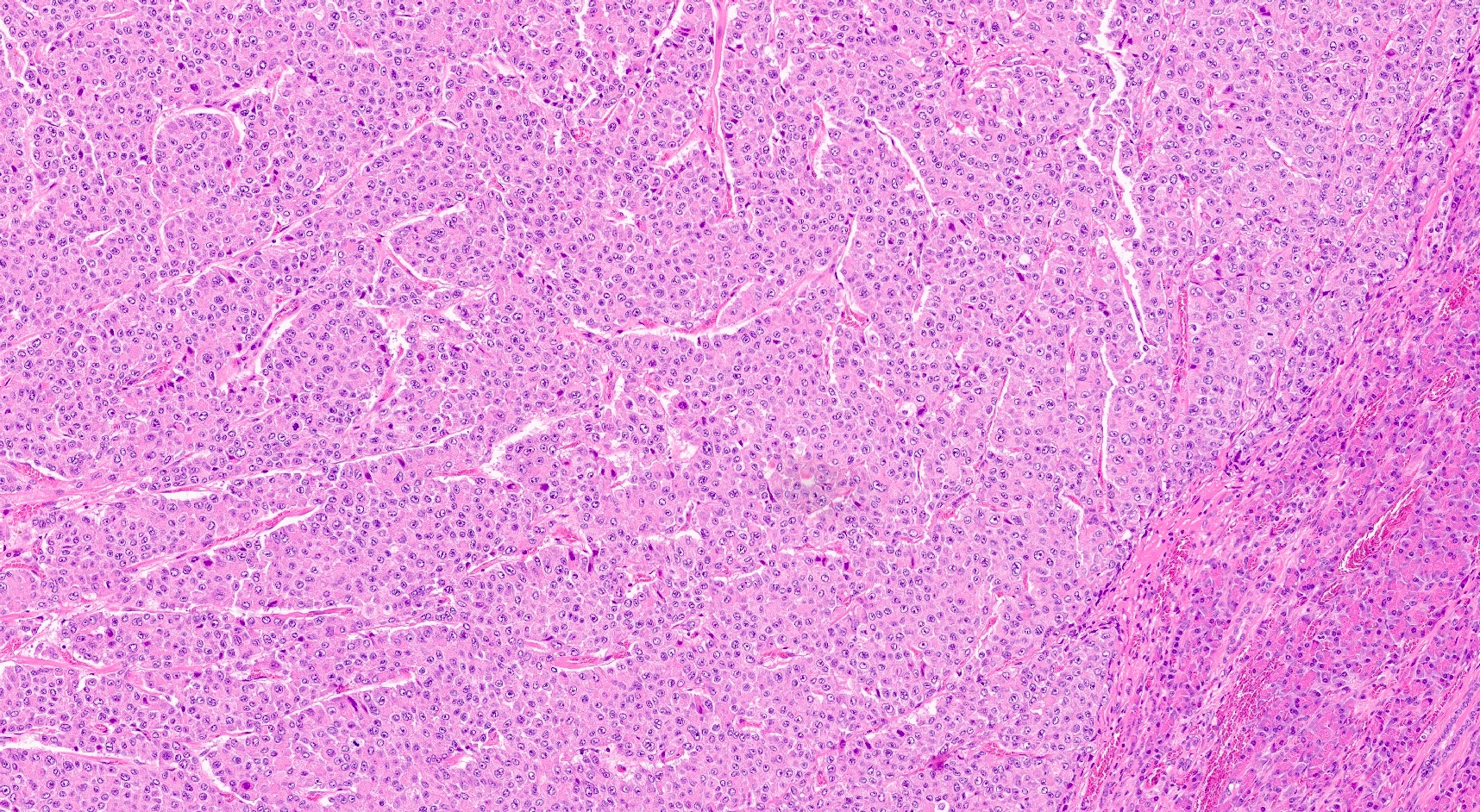
Typical histology
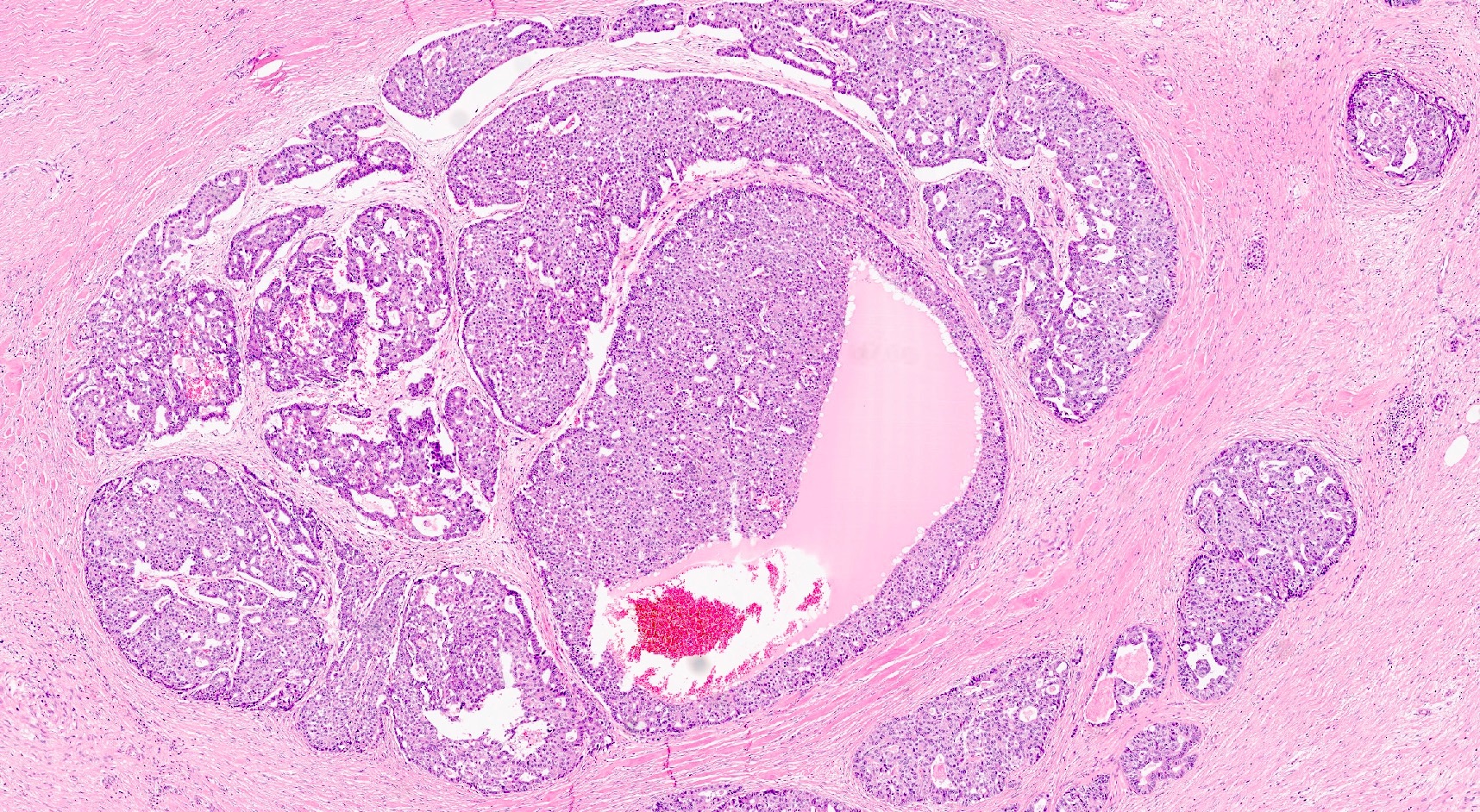
Intraductal growth
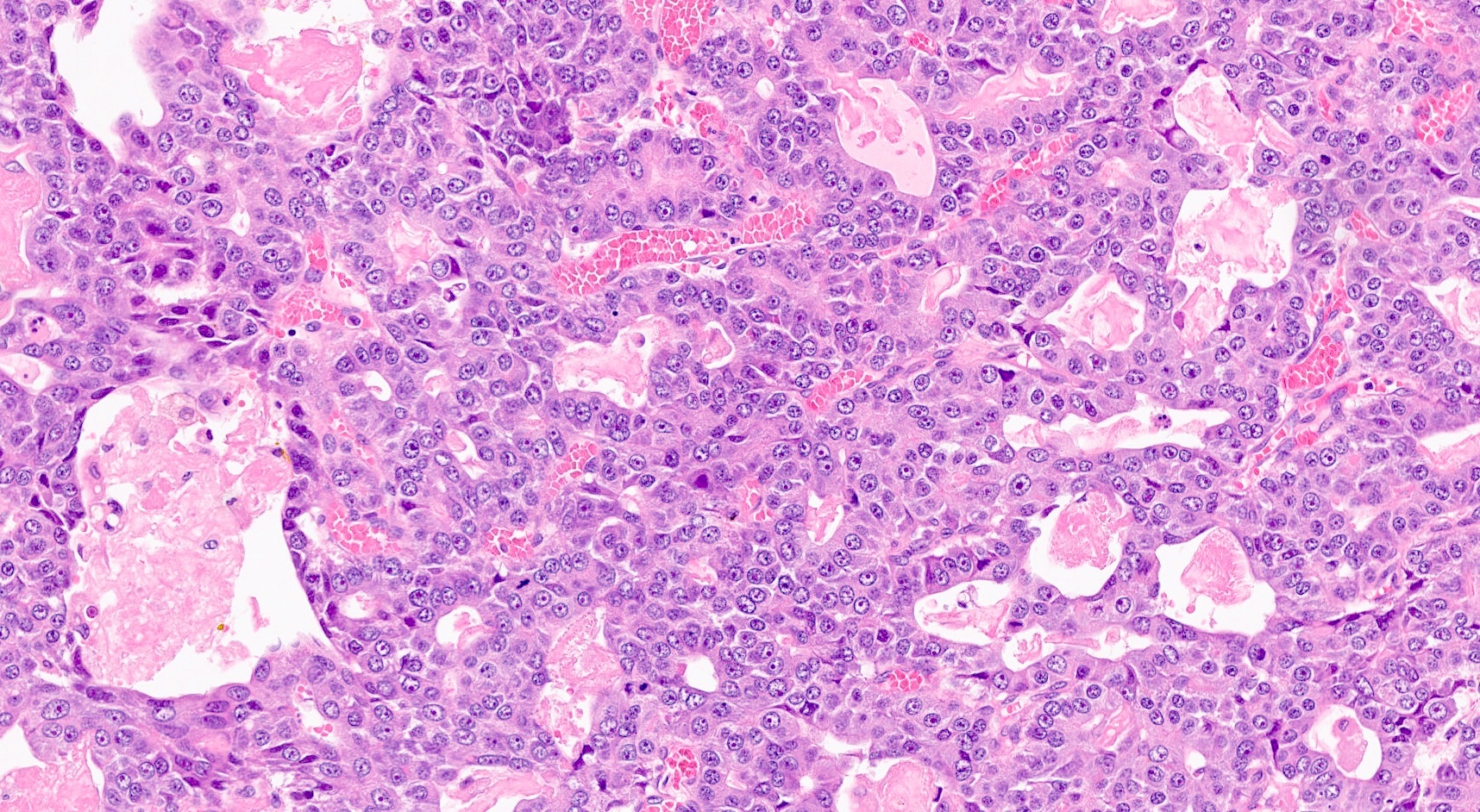
Cell detail
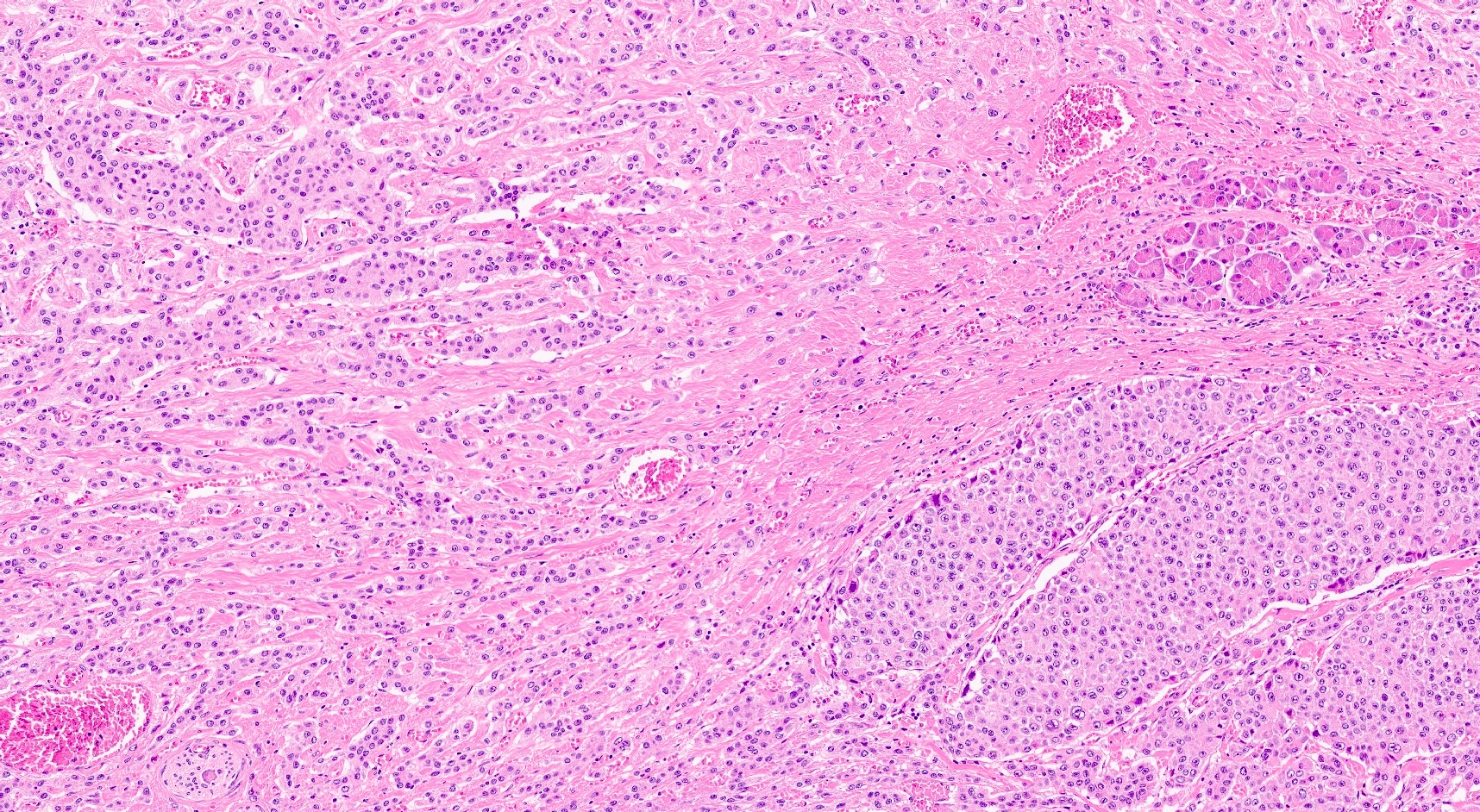
Association with neuroendocrine tumors
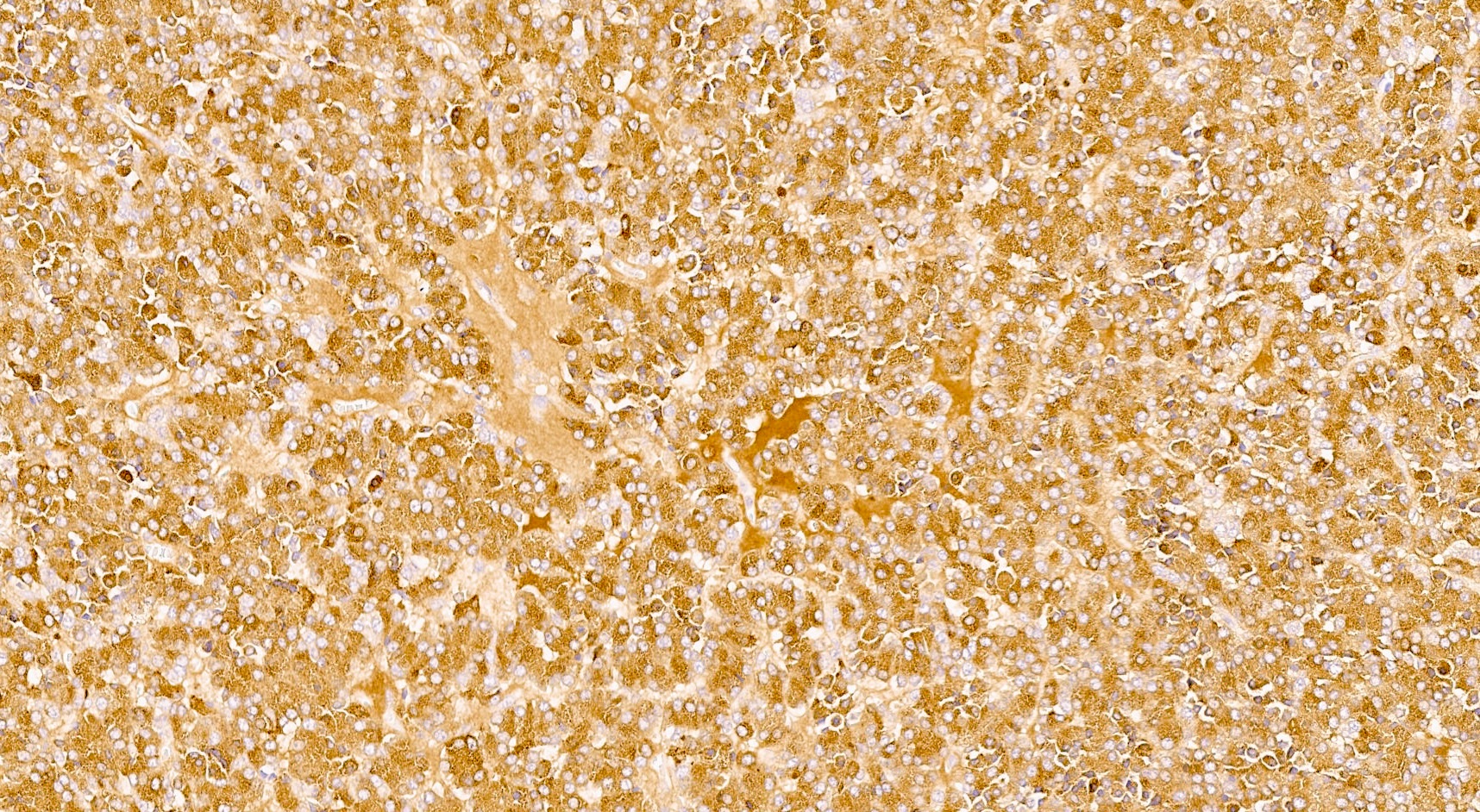
BCL10 expression pattern
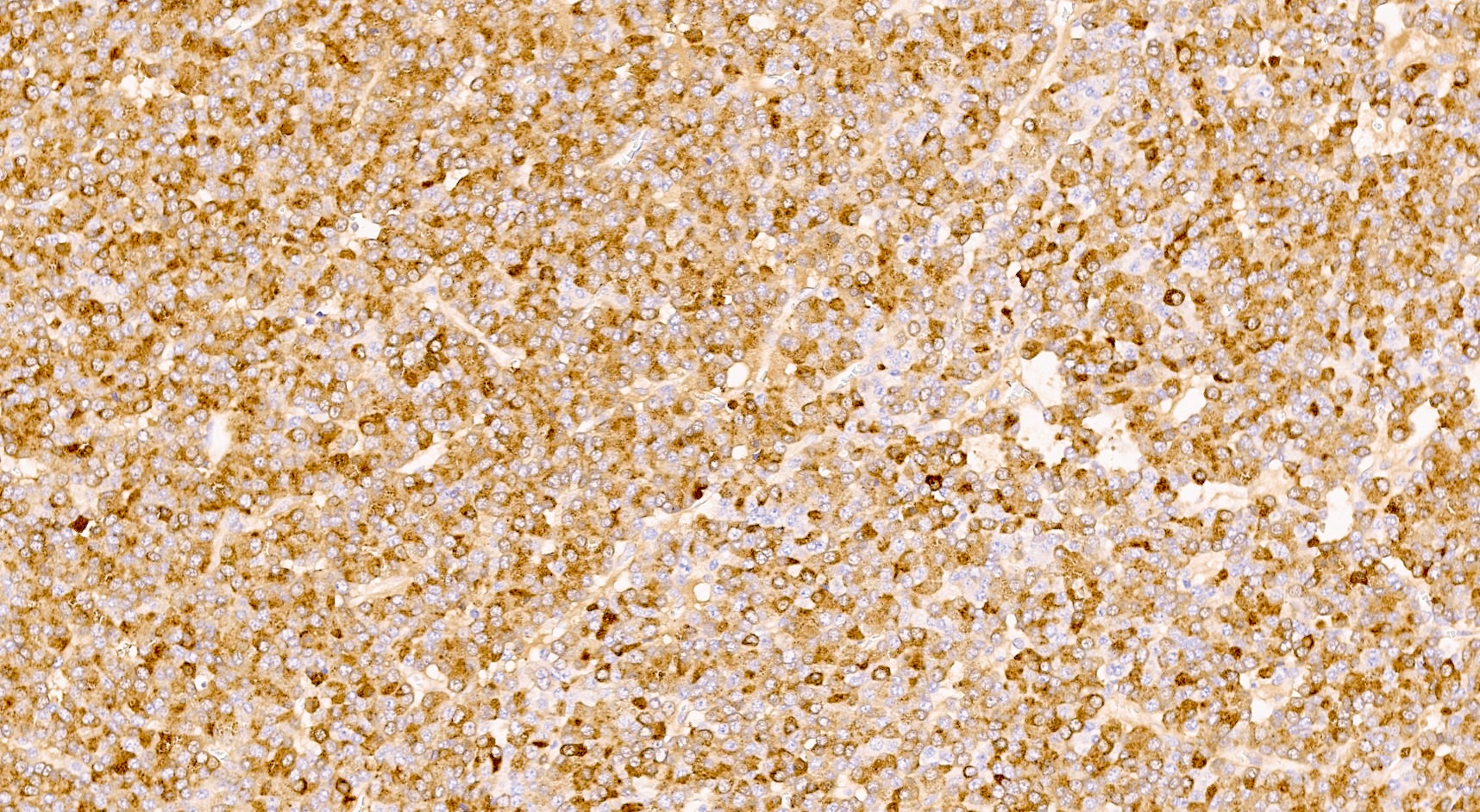
Trypsin expression pattern
Cytology description
- Hypercellular / moderately cellular neoplasm, monomorphic nuclei with prominent nucleoli (Diagn Cytopathol 2017;45:247)
Cytology images
Contributed by Claudio Luchini, M.D., Ph.D.
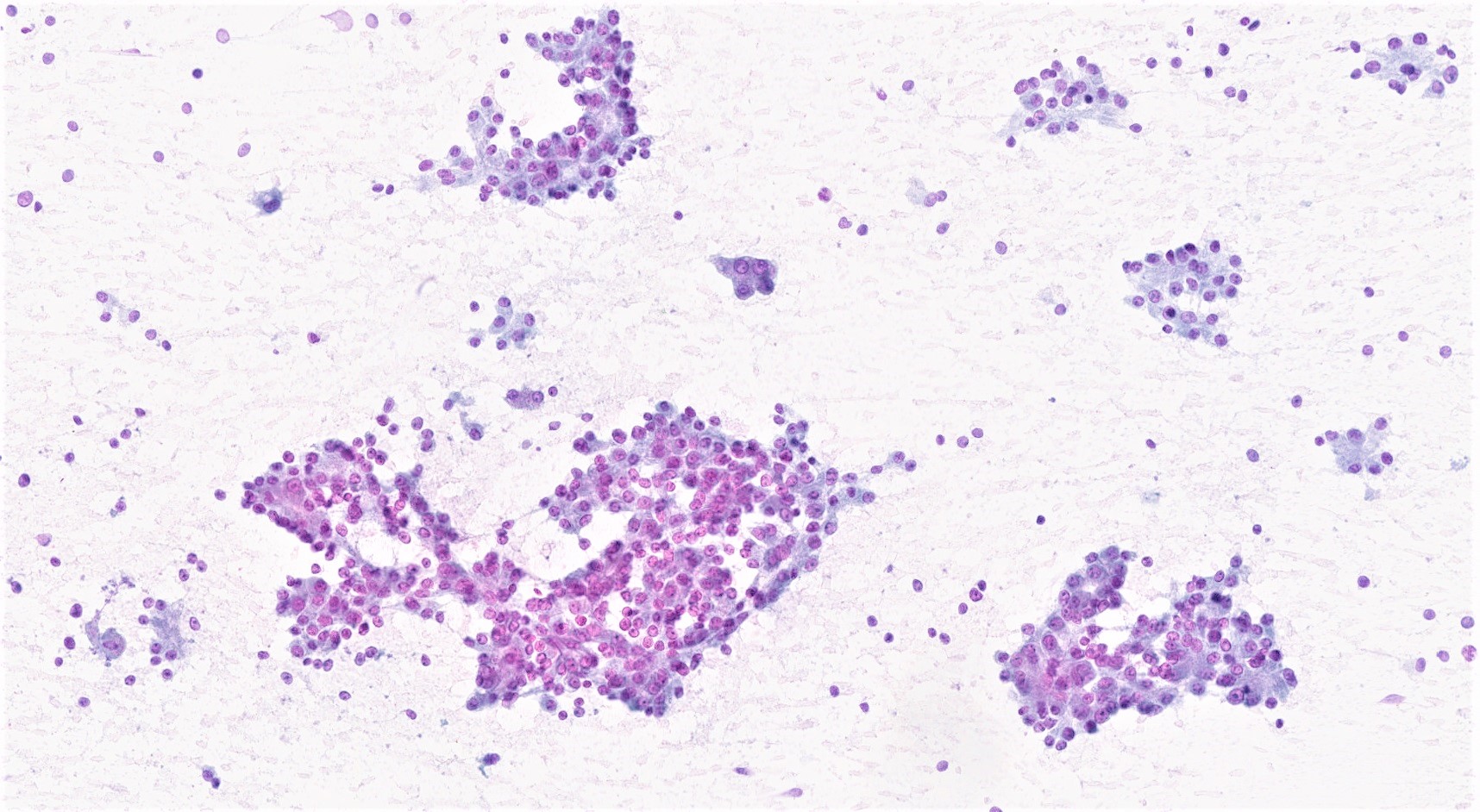
Cytological aspects
Positive stains
- Keratins (particularly CK7 and CK8 / CK18 / CK19), BCL10 (particularly the clone 331.3) and trypsin (Virchows Arch 2009;454:133, Cancer Cytopathol 2013;121:459, Pathologica 2020;112:210)
- Nuclear expression of beta catenin and CD200 expression is found in about 10% of cases (Am J Surg Pathol 2012;36:1782, Virchows Arch 2019;474:105)
Negative stains
- Neoplastic cells are negative for chromogranin and synaptophysin (rarely, scattered positive cells may be present)
Molecular / cytogenetics description
- Most common molecular alterations of pancreatic ductal adenocarcinoma (e.g. KRAS and SMAD4 mutations) are usually absent
- Recurrent presence of BRAF, RAF1 and RET rearrangements (Cancer Discov 2014;4:1398, Mod Pathol 2020;33:1811, Mod Pathol 2020;33:657)
- Wnt pathway alterations with APC / CTNNB1 mutations can be present in a subset of cases
Sample pathology report
- Distal stomach, duodenum and pancreatic head, pancreaticoduodenectomy (Whipple resection):
- Acinar cell carcinoma of the pancreas, 2.2 cm
- Carcinoma involves distal bile duct
- All margins negative for carcinoma
- Positive for lymphovascular invasion and perineural invasion
- Metastatic carcinoma involving 1 of 27 lymph nodes
- Portion of benign stomach and duodenum with no significant pathologic change
Differential diagnosis
- Neuroendocrine neoplasms:
- BCL10 negative, chromogranin and synaptophysin positive
- Salt and pepper chromatin
- No evident nucleoli
- Pancreatoblastoma:
- Pancreatic neoplasm with acinar differentiation: the presence of squamoid nests is diagnostic for pancreatoblastoma
- Intraductal tubulopapillary neoplasm (ITPN):
Additional references
Board review style question #1
A high magnification field of a tumor within the pancreas is shown above. Can the diagnosis of acinar cell carcinoma be based on morphology alone or are other analyses required?
- No, morphology alone is always sufficient
- Yes, electron microscopy is of great help to rule out a neuroendocrine tumor and is always required
- Yes, in addition to morphology, the immunohistochemical demonstration of the acinar differentiation represents the diagnostic gold standard
- Yes, molecular analysis is mandatory
- Yes, the demonstration of a BRAF rearrangement is required for the diagnosis
Board review style answer #1
C. Yes, in addition to morphology, the immunohistochemical demonstration of the acinar differentiation represents the diagnostic gold standard. Morphology and immunohistochemistry represent the 2 most important tools for the diagnosis. The acinar differentiation seen at histology should be supported with BCL10 and trypsin positivity. Tumor cells are also positive for PASD.
Comment Here
Reference: Acinar cell carcinoma
Comment Here
Reference: Acinar cell carcinoma
Board review style question #2
Is it important to report the intraductal growth pattern of pancreatic acinar cell carcinoma?
- No, it is only a descriptive finding
- No, this pattern does not belong to the morphological spectrum of acinar cell carcinoma
- Yes, this pattern is associated with a better prognosis
- Yes, this pattern is associated with a very poor prognosis
- Yes, this pattern is associated with intraductal papillary mucinous neoplasm
Board review style answer #2
C. Yes, this pattern is associated with a better prognosis. This pattern represents a potential diagnostic pitfall with intraductal neoplasms (above all, intraductal tubulopapillary neoplasm) and is associated with a better prognosis.
Comment Here
Reference: Acinar cell carcinoma
Comment Here
Reference: Acinar cell carcinoma

