
Nasal cavity, paranasal sinuses, nasopharynx
Benign tumors
Salivary gland anlage tumor
Editorial Board Member: Bin Xu, M.D., Ph.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 3 September 2020
Last staff update: 8 October 2020
Copyright: 2004-2024, PathologyOutlines.com, Inc.
PubMed Search: Salivary gland anlage tumor
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Electron microscopy description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Dermawan JK, Rabinowitz LO. Salivary gland anlage tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/nasalsalivaryglandanlage.html. Accessed April 16th, 2024.
Definition / general
- Extremely rare, benign, congenital, biphasic tumor with mixed epithelial and myoepithelial elements of midline nasopharynx
Essential features
- Presents within first 6 weeks of life with a midline nasopharyngeal mass and symptoms related to airway / nasal obstruction (Pediatrics 2003;112:e66)
- Covered by nonkeratinizing squamous epithelium
- Peripheral squamous nests and duct-like structures
- Central stromal nodules consisting of uniform ovoid to spindled cells (Am J Surg Pathol 1994;18:25)
- Good prognosis; excision is curative (Int J Pediatr Otorhinolaryngol 2005;69:149)
Terminology
- Salivary gland anlage tumor (SGAT)
- Congenital pleomorphic adenoma
ICD coding
- ICD-10: D49.0 - neoplasm of unspecified behavior of digestive system
Epidemiology
- Extremely rare
- Presents in immediate neonatal period or in early infancy (by age of 6 weeks)
- Male predilection (Int J Pediatr Otorhinolaryngol 2005;69:149)
Sites
- Located or near midline in the nasopharynx or posterior nasal septum
Pathophysiology
- Congenital / developmental anomaly, likely represents hamartoma of minor salivary gland origin
Clinical features
- Obstructive symptoms manifesting as respiratory distress, feeding difficulties or nasal airway obstruction
Diagnosis
- CT or MRI of the nasal sinuses
- Diagnosis is by endoscopic biopsy / debulking or surgical resection
Radiology description
- Lobular, midline soft tissue mass in the naso-oropharynx without infiltration into surrounding structures
- T1 isointense, T2 hyperintense, homogeneously enhancing mass measuring 1 to 2 cm on MRI (Pediatr Radiol 2015;45:453, AJNR Am J Neuroradiol 2009;30:1022)
Radiology images
Contributed by Scott Poswilko, M.D.
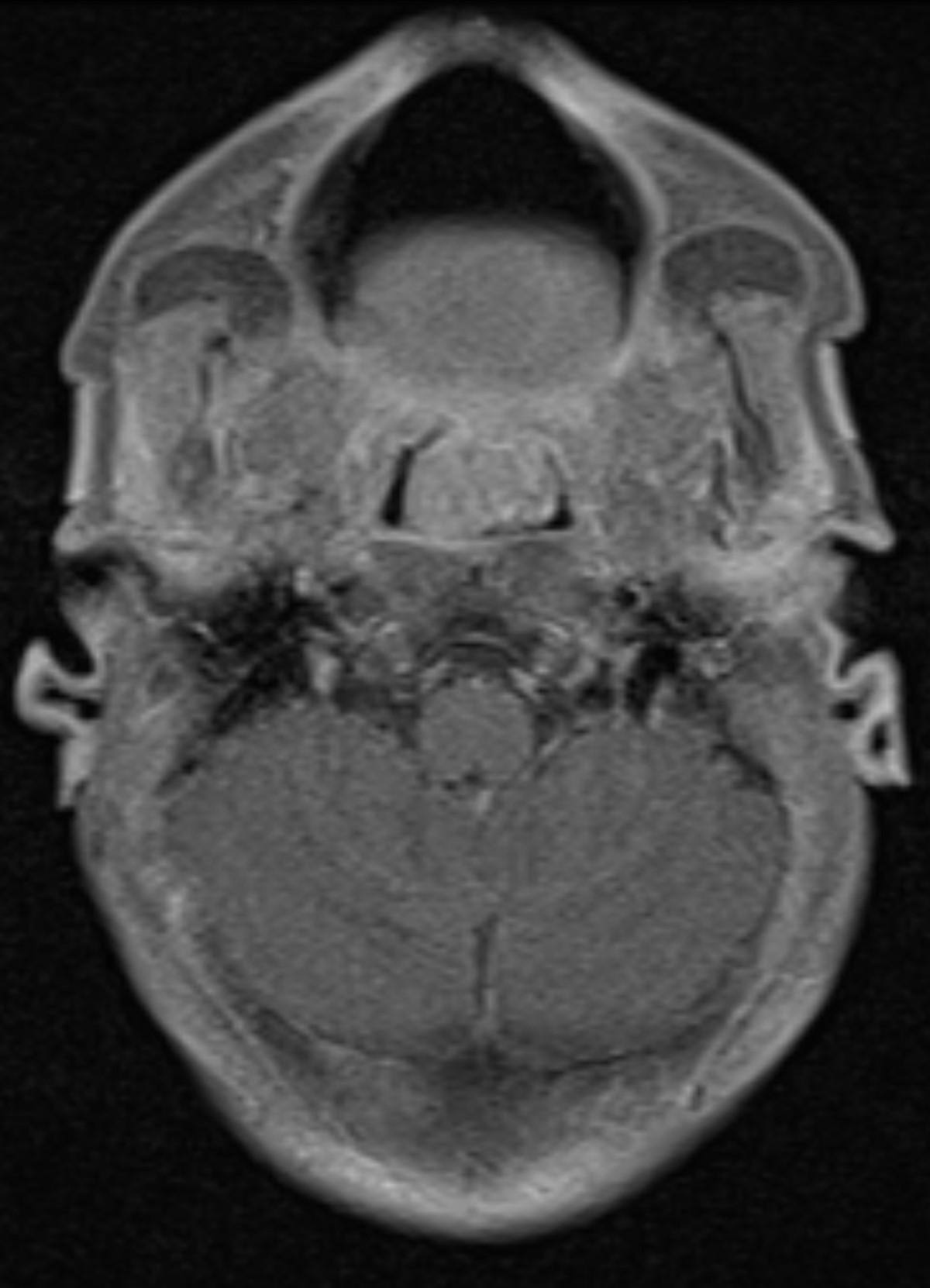
Naso-oropharyngeal mass (T1 axial)
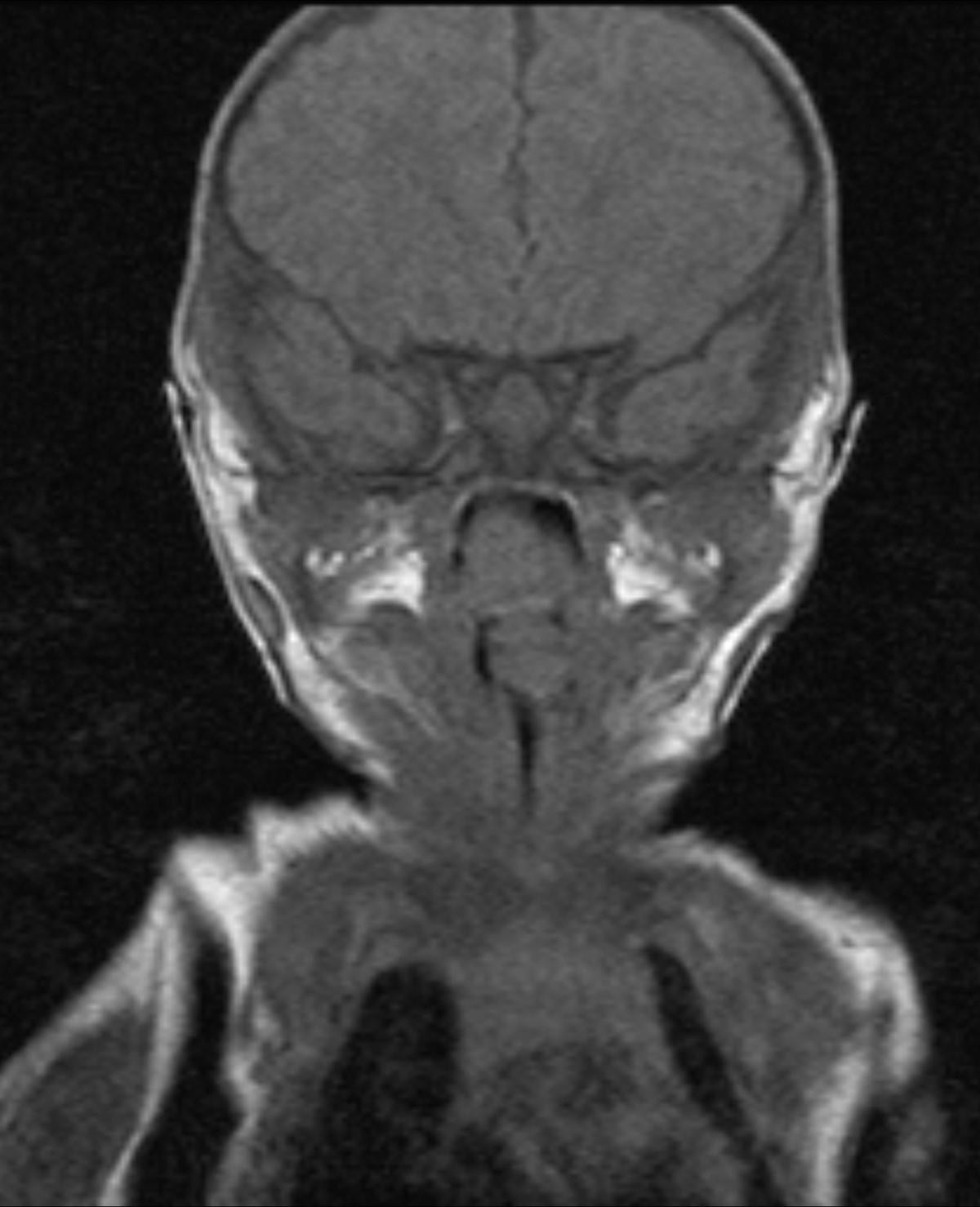
Naso-oropharyngeal mass (T1 coronal)
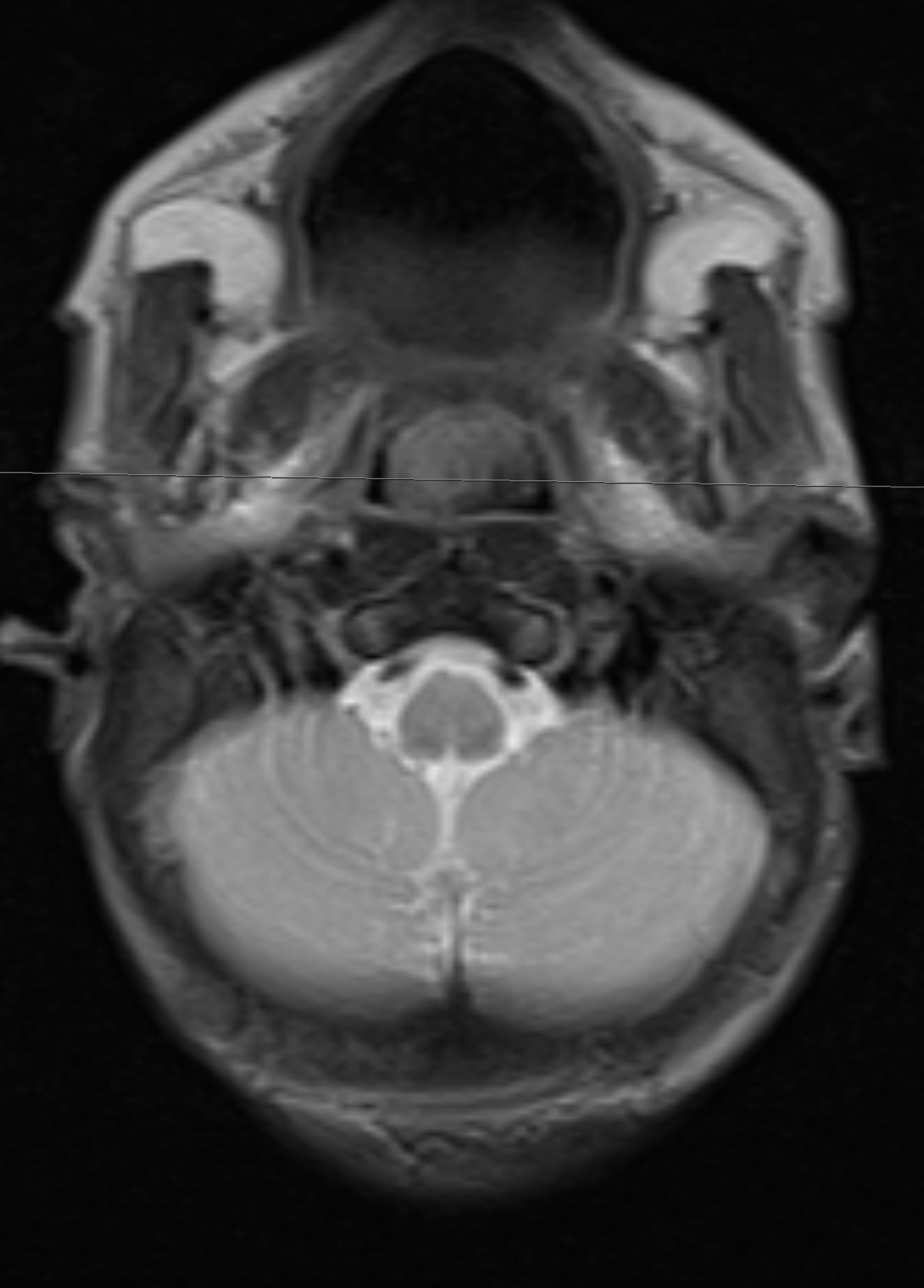
Naso-oropharyngeal mass (T2 axial)
Prognostic factors
- Excellent prognosis
- Curable by surgical resection
Case reports
- Newborn boy and 6 week old girl with nasopharyngeal mass (Fetal Pediatr Pathol 2011;30:116)
- Newborn boy with life threatening nasal obstruction (Pediatrics 2003;112:e66)
- Newborn boy with acute airway obstruction secondary to nasopharyngeal mass (Int J Pediatr Otorhinolaryngol 2005;69:149)
- 2 week old infant with difficulty breathing since birth (AJNR Am J Neuroradiol 2009;30:1022)
- Congenital salivary gland anlage tumor causing severe neonatal respiratory distress (Fetal Pediatr Pathol 2010;29:323)
- Salivary gland anlage tumor with widespread necrosis and large cyst formation (Pathology 1996;28:128)
Treatment
- Simple surgical excision
Gross description
- Polypoid, gray, rubbery, grossly encapsulated tissue fragment with homogenous cut surface without necrosis or hemorrhage
Gross images
Images hosted on other servers:

Lobulated mass
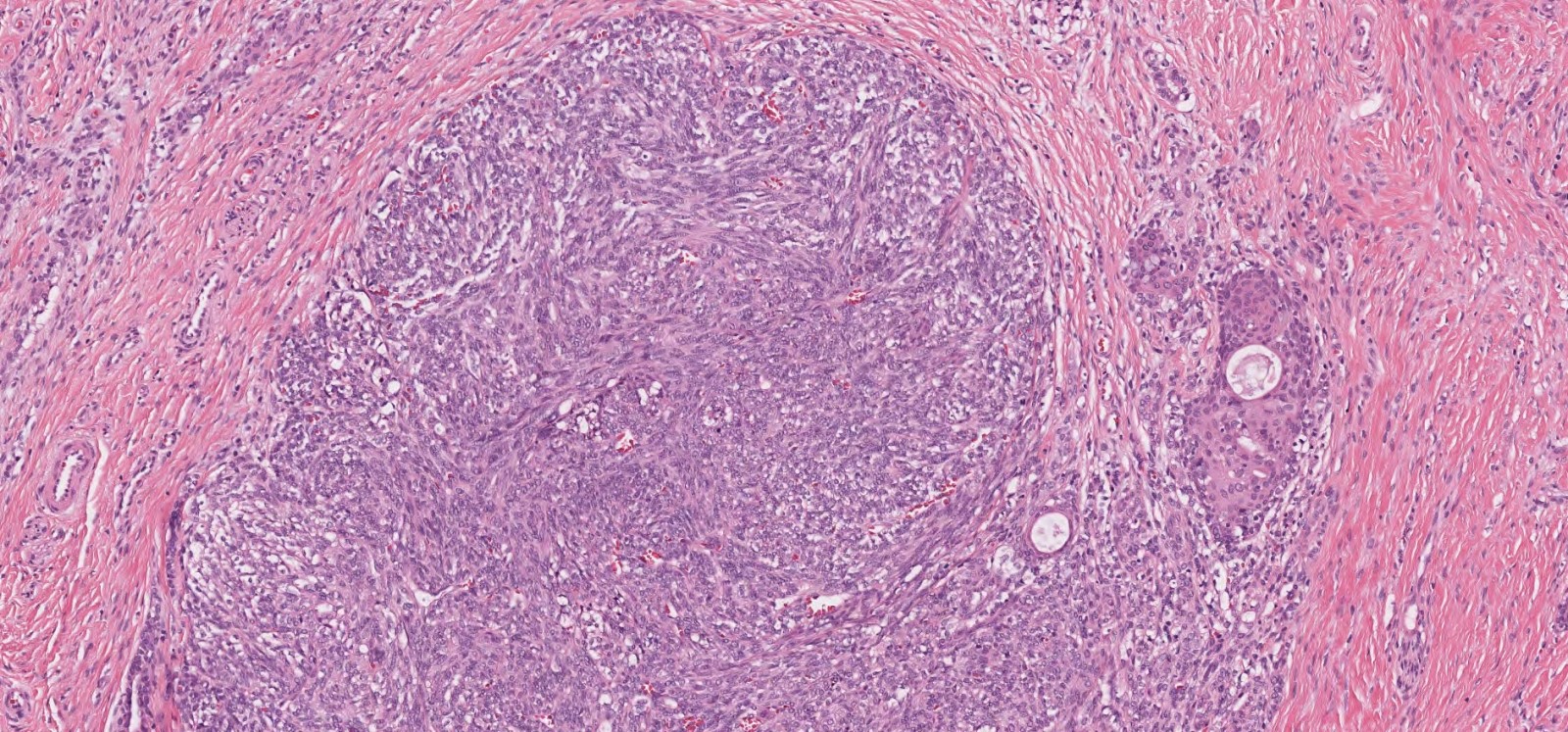
Microscopic (histologic) description
- Surface covered by nonkeratinizing squamous mucosa
- Multiple submucosal, cellular, solid stromal nodules separated by hypocellular stroma in the center
- Duct-like epithelial structures and squamous nests with variable keratinization more prominent toward periphery of stromal nodules (Int J Pediatr Otorhinolaryngol 2005;69:149)
- Internodular epithelial components blend into cellular nodules
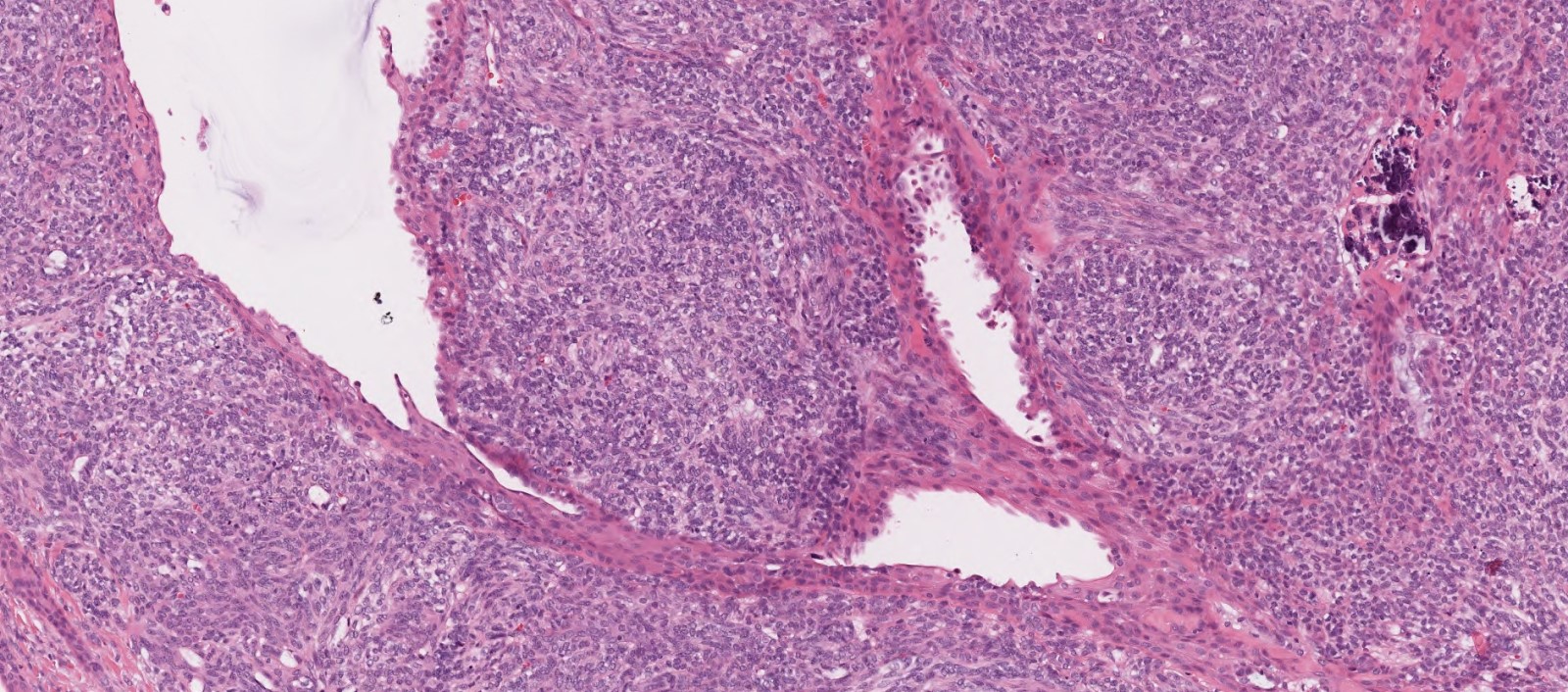
- Cellular stromal nodules composed of mesenchymal appearing, fusiform to spindled to ovoid cells forming short fascicles or trabeculae (Pediatr Pathol Lab Med 1996;16:973)
- Stromal cells are uniform and show bland cytology with dispersed chromatin, scant eosinophilic cytoplasm and indistinct cell borders (Fetal Pediatr Pathol 2011;30:116)
- Background hypocellular collagenous stroma with focal chondromyxoid areas
- Mitotic figures and hemorrhagic necrosis may be present
Microscopic (histologic) images
Contributed by Josephine K. Dermawan, M.D., Ph.D. and Laura O. Rabinowitz, M.D.
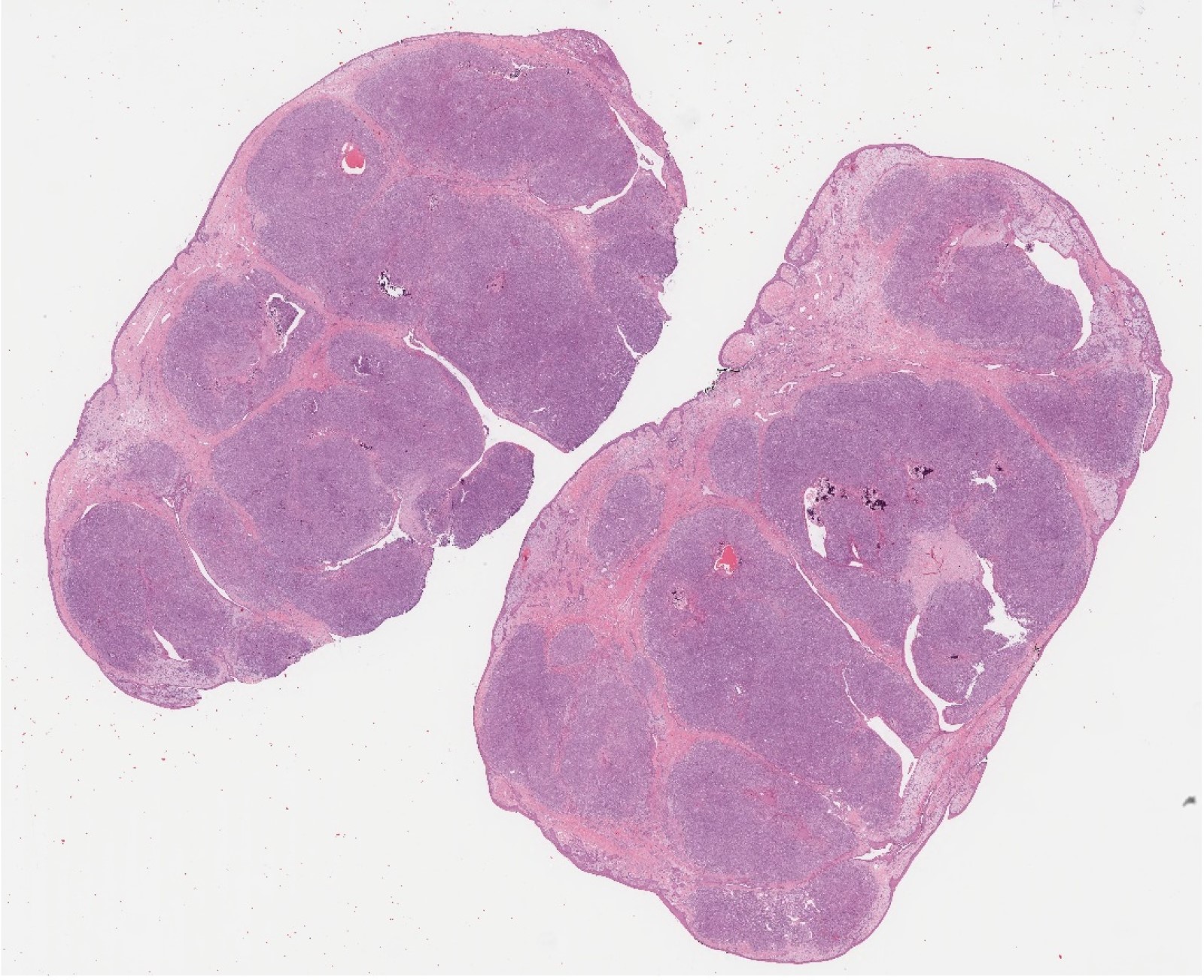
Submucosal lobular proliferation
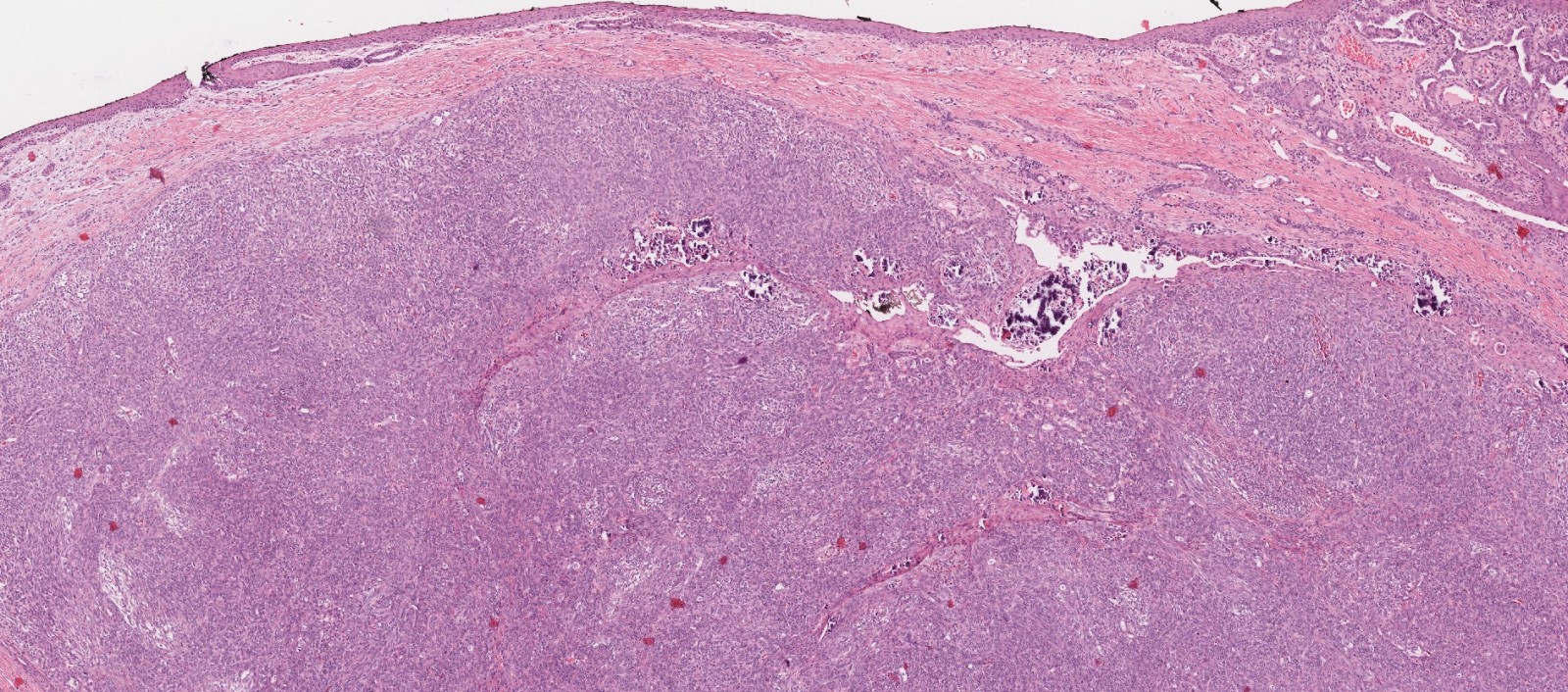
Nonkeratinizing squamous mucosa
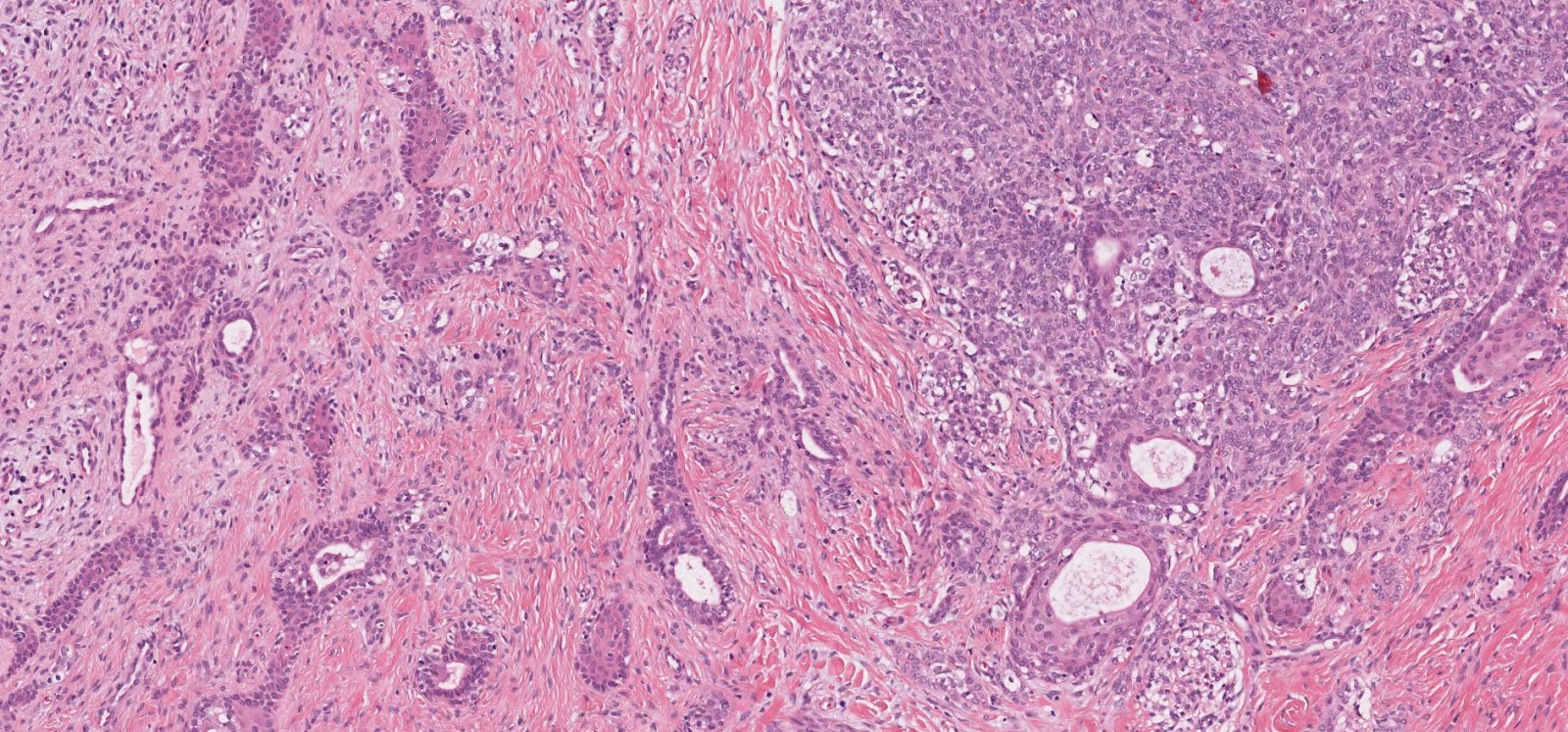
Epithelial and mesenchymal components
Duct-like structures and calcifications
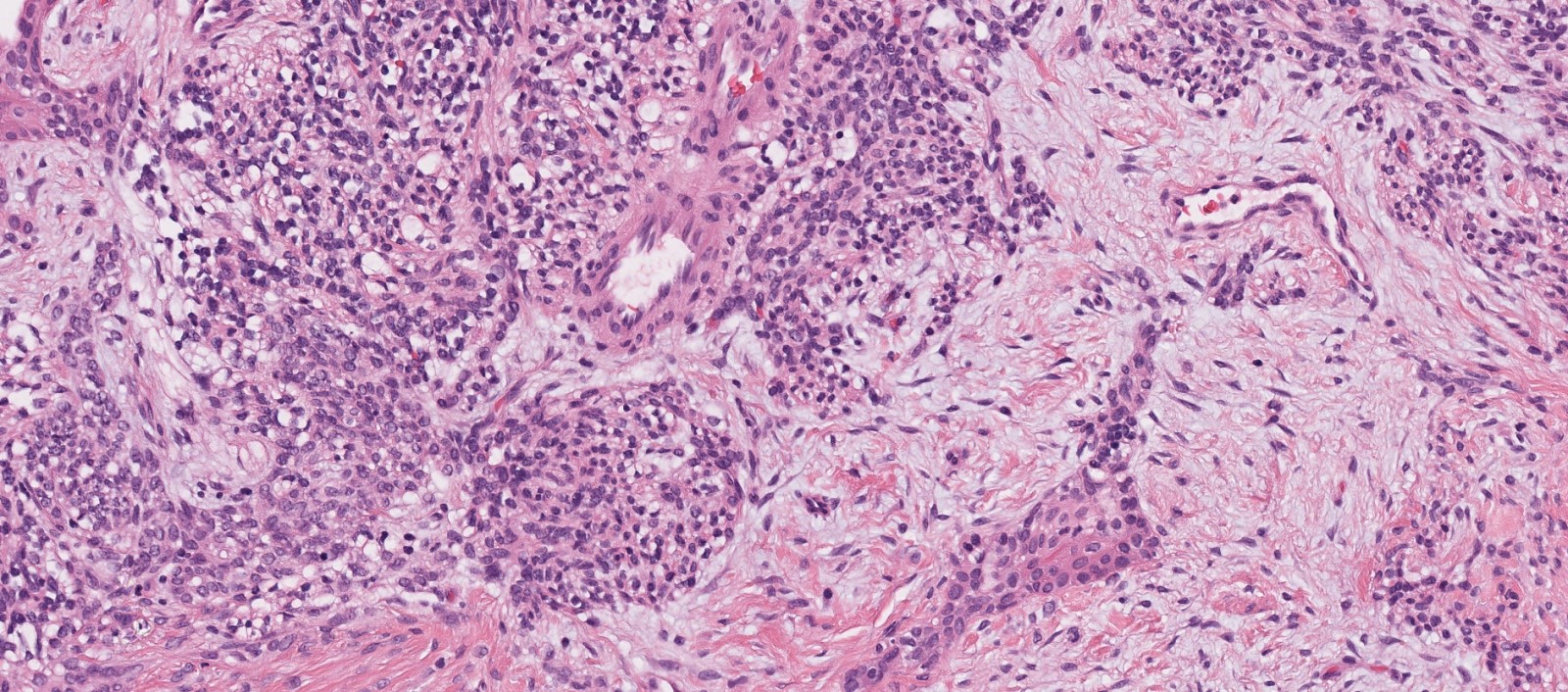
Focal chondromyxoid stroma
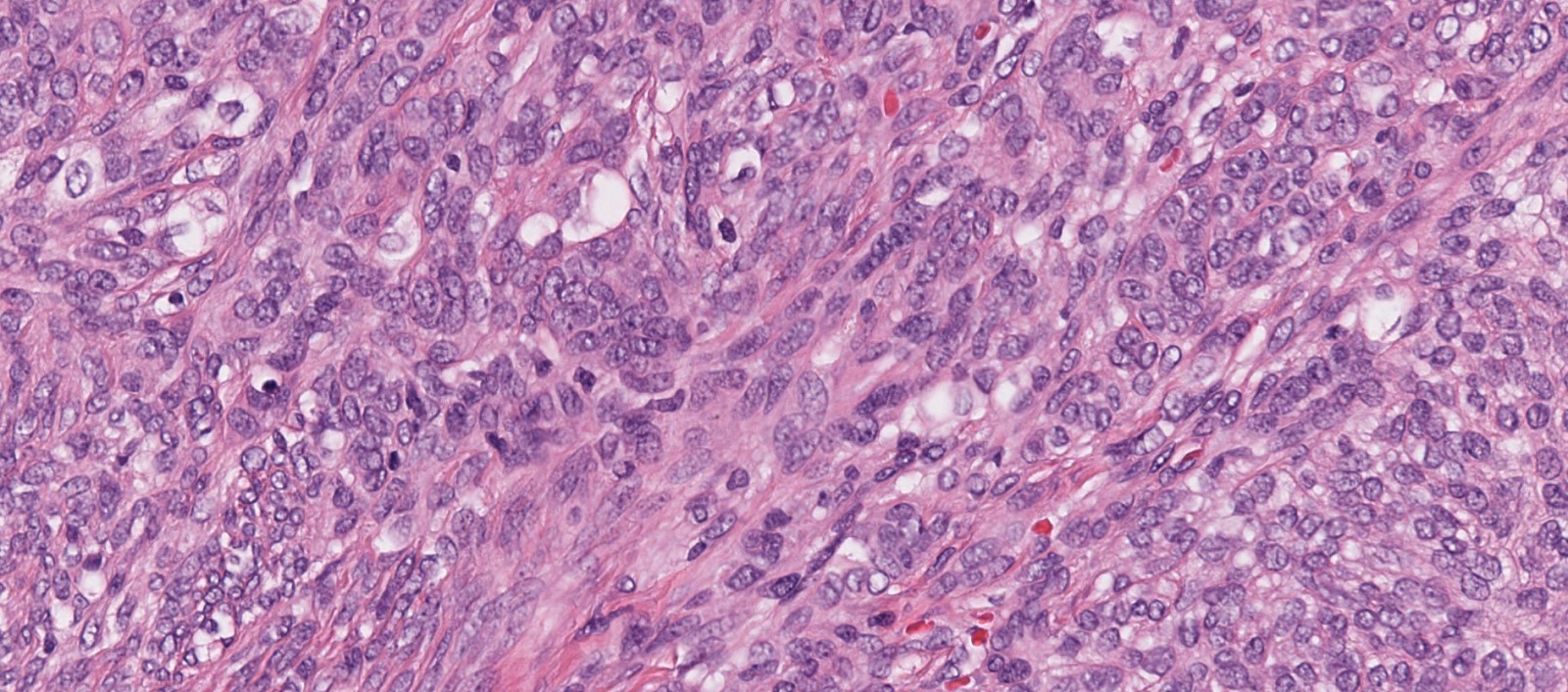
Ovoid to spindled stromal cells

Positive CK7
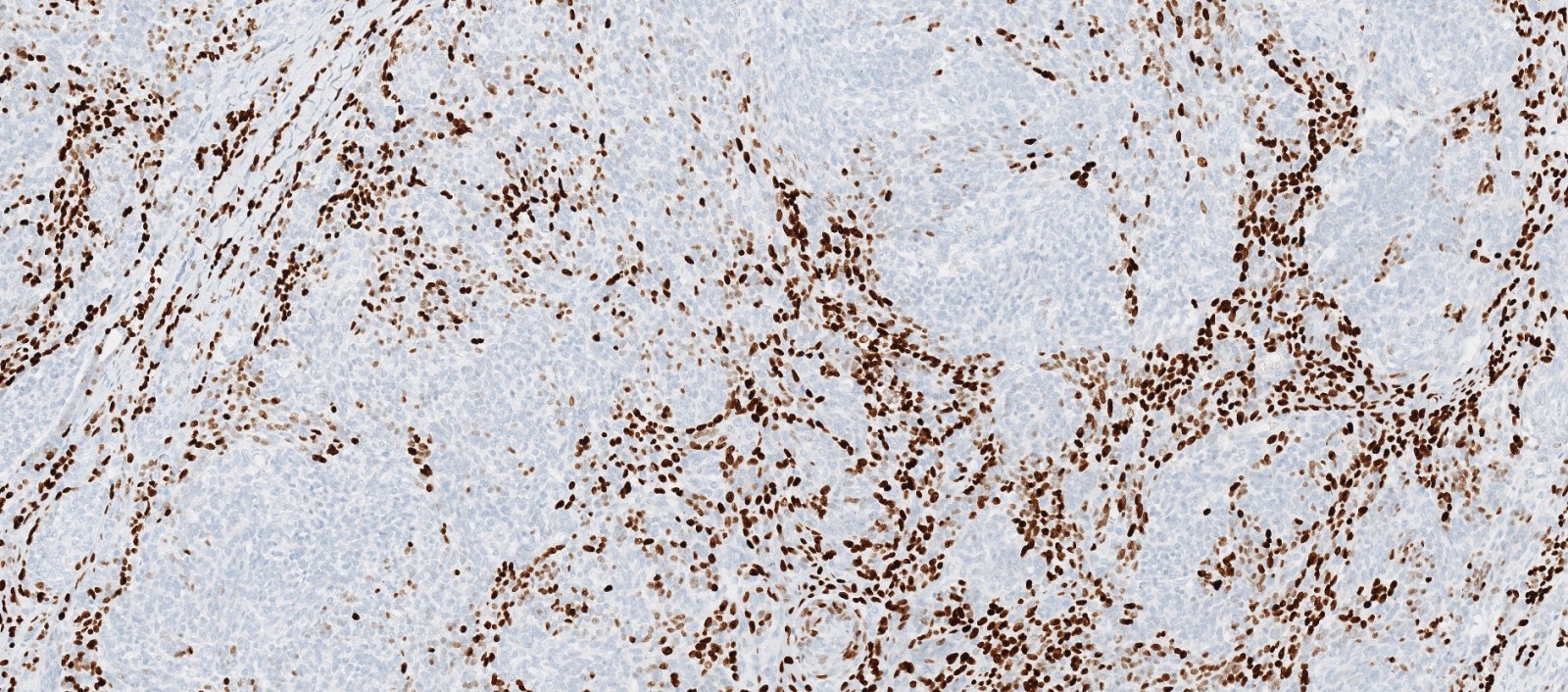
Positive p63
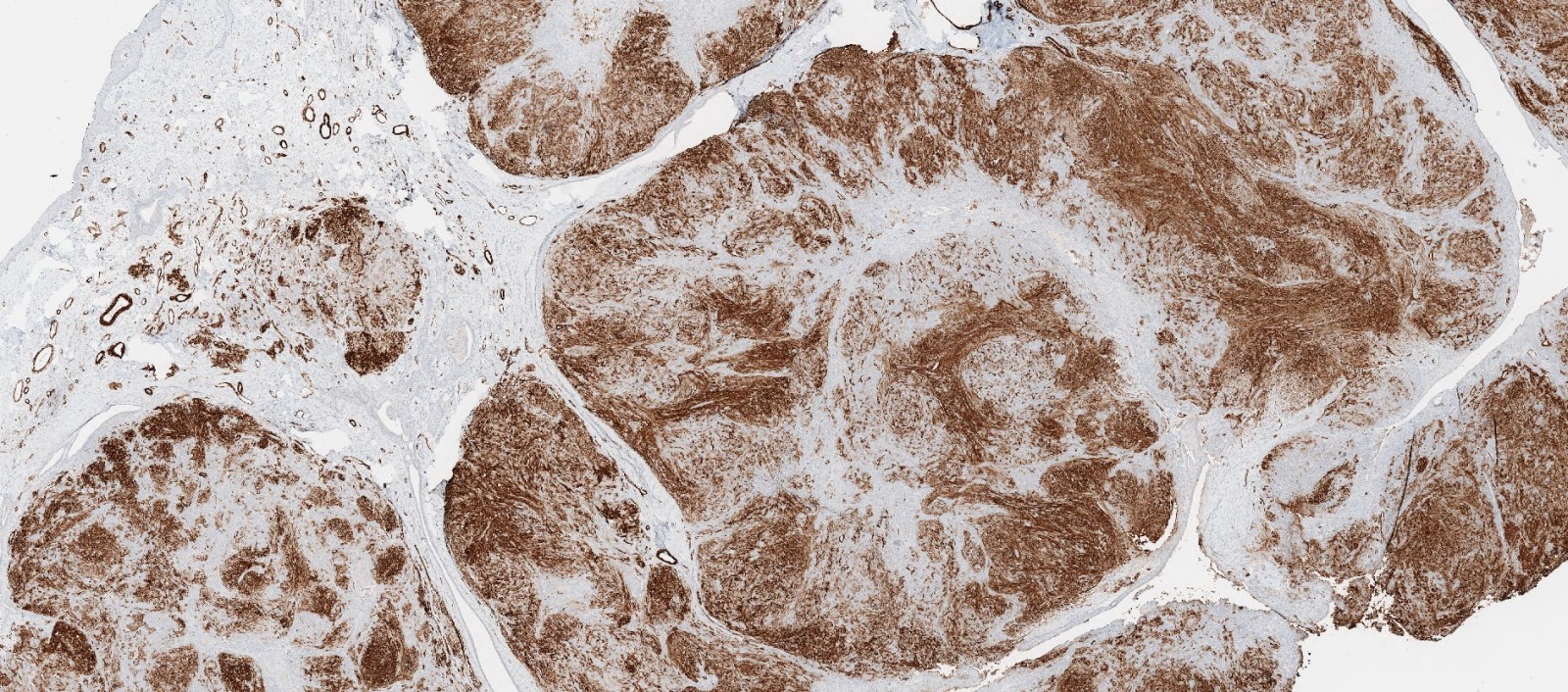
Variable SMMS1
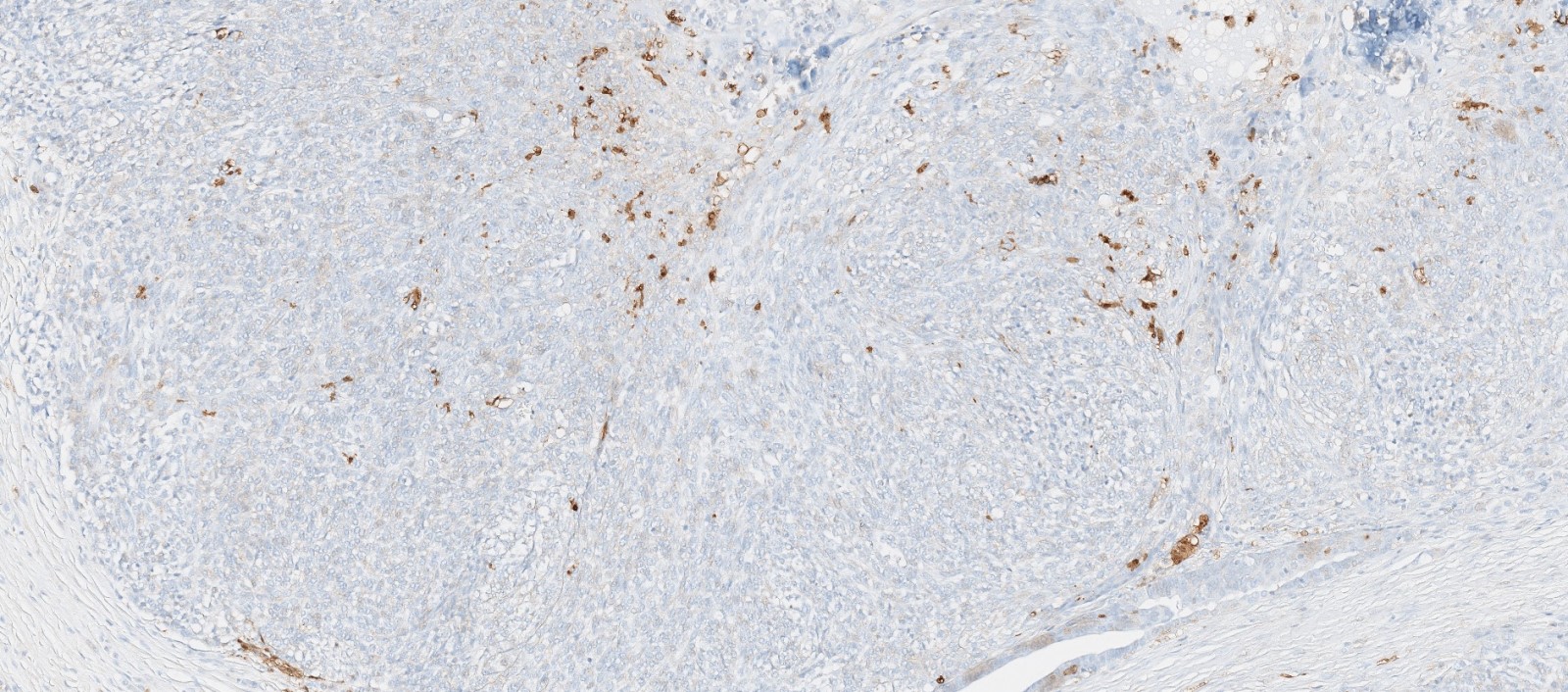
Focal S100
Positive stains
- Epithelial components:
- Cytokeratins (pancytokeratins, CK7)
- p63
- Mesenchymal components:
- Variable for cytokeratins (pancytokeratins, CK7)
- Alpha smooth muscle actin, muscle specific actin, smooth muscle myosin
- May have focal S100 (Pediatr Pathol Lab Med 1996;16:973, Am J Surg Pathol 1994;18:25)
Electron microscopy description
- Stromal-like cells have ultrastructural features of myoepithelial cells (Am J Surg Pathol 1994;18:25)
Sample pathology report
- Soft tissue mass, nasopharynx, excision:
- Salivary gland anlage tumor (see comment)
- Comment: Histologic sections demonstrate a lobulated nasopharyngeal proliferation which shows mixed epithelial and myoepithelial components. The tumor shows tubules and ducts with variable keratinization with attachment to surface squamous epithelium and multiple cellular spindle cell nodules. Focal chondromyxoid matrix is noted. The epithelial component shows diffuse, strong immunoreactivity for cytokeratin and CK7. The spindle cells show variable to strong immunoreactivity with CK7, p63, SMMS and S100 (rare cells).
Differential diagnosis
- Dermoid cyst:
- Cystic lesion lined by keratinizing squamous epithelium
- Epithelium associated with skin adnexal structures, such as sebaceous glands
- Craniopharyngioma:
- Nests and cords of squamoid cells
- Peripheral palisaded nuclei
- Calcification and keratin material
- Leiomyoma or leiomyosarcomas:
- Spindle cell rhabdomyosarcoma:
- Synovial sarcoma:
- Variable positivity for cytokeratins and TLE1
- Negative for SMA and MSA
- Characterized by t(X;18) SS18-SSX1/2 fusions
- Respiratory epithelioid adenomatoid hamartoma (REAH):
- Noninvasive epithelial proliferation with surface invaginations with thickened basement membrane and ciliated respiratory epithelium
- Lack of spindle cell proliferation
Board review style question #1
- A neonate presents with respiratory distress shortly after delivery. Direct laryngoscopy shows an obstructing nasopharyngeal mass. An MRI of the nasal sinus shows a 1.8 cm, polypoid mass in the in the naso-oropharynx. Histology reveals a biphasic, epithelial and mesenchymal neoplasm with ducts and squamous nests and cellular stromal nodules consisting of spindle cells with a myoepithelial immunophenotype. What is the best management for this tumor?
- Close observation
- Cryotherapy
- Neoadjuvant chemotherapy followed by surgical resection
- Radiation therapy
- Simple endoscopic or surgical resection
Board review style answer #1
E. Simple endoscopic or surgical resection
Salivary gland anlage tumor is a benign tumor with excellent prognosis following simple surgical resection. Of all the cases that have been reported, none has recurred following surgical excision.
Comment Here
Reference: Salivary gland anlage tumor
Salivary gland anlage tumor is a benign tumor with excellent prognosis following simple surgical resection. Of all the cases that have been reported, none has recurred following surgical excision.
Comment Here
Reference: Salivary gland anlage tumor
Board review style question #2
- Which of the following features would favor a diagnosis of salivary gland anlage tumor?
- Diffuse S100 immunoreactivity in the spindled component
- Distant metastasis and death within several months of initial diagnosis
- Mesenchymal component with pleomorphic spindle cells showing significant cytologic atypia
- Presence of ducts and squamous nests that blend into nodules of spindled cells
- Presentation in an adolescent or young male
Board review style answer #2
D. Presence of ducts and squamous nests that blend into nodules of spindled cells
Salivary gland anlage tumor is a benign congenital tumor of infancy characterized histologically by the presence of both epithelial and mesenchymal components. Lined by nonkeratinizing squamous epithelium, in the submucosa are cellular stromal nodules composed of uniform, spindled to ovoid cells forming short fascicles, with duct-like epithelial structures and squamous nests in the periphery that blend into the cellular nodules. The spindle cells show variable to strong immunoreactivity with CK7, p63, SMMS and S100 (rare cells).
Comment Here
Reference: Salivary gland anlage tumor
Salivary gland anlage tumor is a benign congenital tumor of infancy characterized histologically by the presence of both epithelial and mesenchymal components. Lined by nonkeratinizing squamous epithelium, in the submucosa are cellular stromal nodules composed of uniform, spindled to ovoid cells forming short fascicles, with duct-like epithelial structures and squamous nests in the periphery that blend into the cellular nodules. The spindle cells show variable to strong immunoreactivity with CK7, p63, SMMS and S100 (rare cells).
Comment Here
Reference: Salivary gland anlage tumor
