
Nasal cavity, paranasal sinuses, nasopharynx
Benign tumors
Nasopharyngeal angiofibroma
Author: Bin Xu, M.D., Ph.D.
Editorial Board Member: Kelly Magliocca, D.D.S., M.P.H.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 9 October 2020
Last staff update: 12 May 2021
Copyright: 2004-2024, PathologyOutlines.com, Inc.
PubMed Search: Nasopharyngeal angiofibroma[TI] free full text[sb]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Xu B. Nasopharyngeal angiofibroma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/nasalangiofibroma.html. Accessed April 24th, 2024.
Definition / general
- Locally aggressive fibrovascular neoplasm of the nasopharynx developed almost exclusively in adolescent and young male patients
Essential features
- Nasopharyngeal location
- Affecting adolescent or young male patients
- Histologically composed of vasculature of various sizes and cellular fibrotic stroma with fibroblasts
Terminology
- Juvenile nasopharyngeal angiofibroma, juvenile fibroma, angiofibroma
Epidemiology
- 0.05 - 0.5% of all head and neck tumors (StatPearls: Nasopharyngeal Angiofibroma [Accessed 10 June 2020])
- Occurs almost exclusively in adolescent and young males, with a median age of diagnosis of 15 years (range: 8 - 27 years) (Acta Otorrinolaringol Esp 2019;70:279, Head Neck Pathol 2018;12:52)
- Although a handful of case reports describe nasopharyngeal angiofibroma in female patients, the documentation of these cases is not convincing to represent this particular entity (Mol Clin Oncol 2018;9:702, J Laryngol Otol 2018;132:184, Eur Arch Otorhinolaryngol 2006;263:657, Indian J Dent Res 2004;15:145, AMA Arch Otolaryngol 1951;54:620)
- May occur in patients with familial adenomatous polyposis (Gastroenterology 1993;105:1550, Otolaryngol Head Neck Surg 1995;113:435, ANZ J Surg 2013;83:387)
Sites
- Arises in the nasopharynx or posterolateral wall of nasal cavity (Otolaryngol Head Neck Surg 2019;161:352)
- May be locally aggressive, show extension into paranasal sinus, pterygopalatine fossa, infratemporal fossa and orbit (Otolaryngol Head Neck Surg 2019;161:352)
- 10 - 37% have intracranial extension, usually into the middle cranial fossa (Otolaryngol Head Neck Surg 2019;161:352, StatPearls: Nasopharyngeal Angiofibroma [Accessed 10 June 2020])
Etiology
- Etiology remains unclear
- May be hormonally affected given the predilection for adolescent male
Clinical features
- Highly vascular lesion with one or more feeding arterials
- The most common feeding vessel is the internal maxillary artery, a branch of the external carotid artery (StatPearls: Nasopharyngeal Angiofibroma [Accessed 10 June 2020])
- Most frequently presents with epistaxis followed by nasal obstruction and rhinorrhea (Head Neck Pathol 2018;12:52, J Oral Maxillofac Pathol 2016;20:330)
Diagnosis
- Diagnosis is typically rendered using angiography, which allows visualization of the feeding vessels and preoperative embolization
- Given the risk of massive hemorrhage, preoperative biopsy and fine needle aspiration is strongly discouraged
Radiology description
- Angiography allows identification of a highly vascularized mass with a central feeding vessel
Radiology images
Images hosted on other servers:

Angiography
Prognostic factors
- Although considered as a benign mesenchymal neoplasm, nasopharyngeal angiofibroma is locally aggressive with approximately 20% local recurrence (Otolaryngol Head Neck Surg 2019;161:352, J Laryngol Otol 2018;132:978)
- Cranial or orbital involvement and postoperative residual vascularity on imaging study are associated with increased risk of local recurrence (Otolaryngol Head Neck Surg 2019;161:352)
Case reports
- 17 year old boy with nasopharyngeal angiofibroma extending intraorally (J Oral Maxillofac Pathol 2016;20:330)
- 18 year old man with nasal mass, recurrent epistaxis and nasal obstruction (J Clin Diagn Res 2017;11:MD03)
- 21 year old man with bilateral nasopharyngeal angiofibroma (Eur Arch Otorhinolaryngol 2016;273:3435)
- 31 year old man with Proteus syndrome and nasopharyngeal angiofibroma (Hippokratia 2017;21:147)
- 32 year old man with severe epistaxis and nasopharyngeal mass (BMJ Case Rep 2018)
Treatment
- Complete surgical resection is the treatment of choice
- Preoperative embolization through angiography may be performed
Clinical images
Images hosted on other servers:

Facial swelling
Gross description
- Polypoid firm mass
- Color varies from yellow to dark red or black, depending on the extent of intraoperative hemorrhage
Gross images
Contributed by Kelly Magliocca, D.D.S., M.P.H.

Gross appearance, cut surface

Gross appearance with ink
Images hosted on other servers:

Polypoid, beige to brown, firm, fibrotic mass
Microscopic (histologic) description
- Benign fibrovascular lesion composed of 2 components
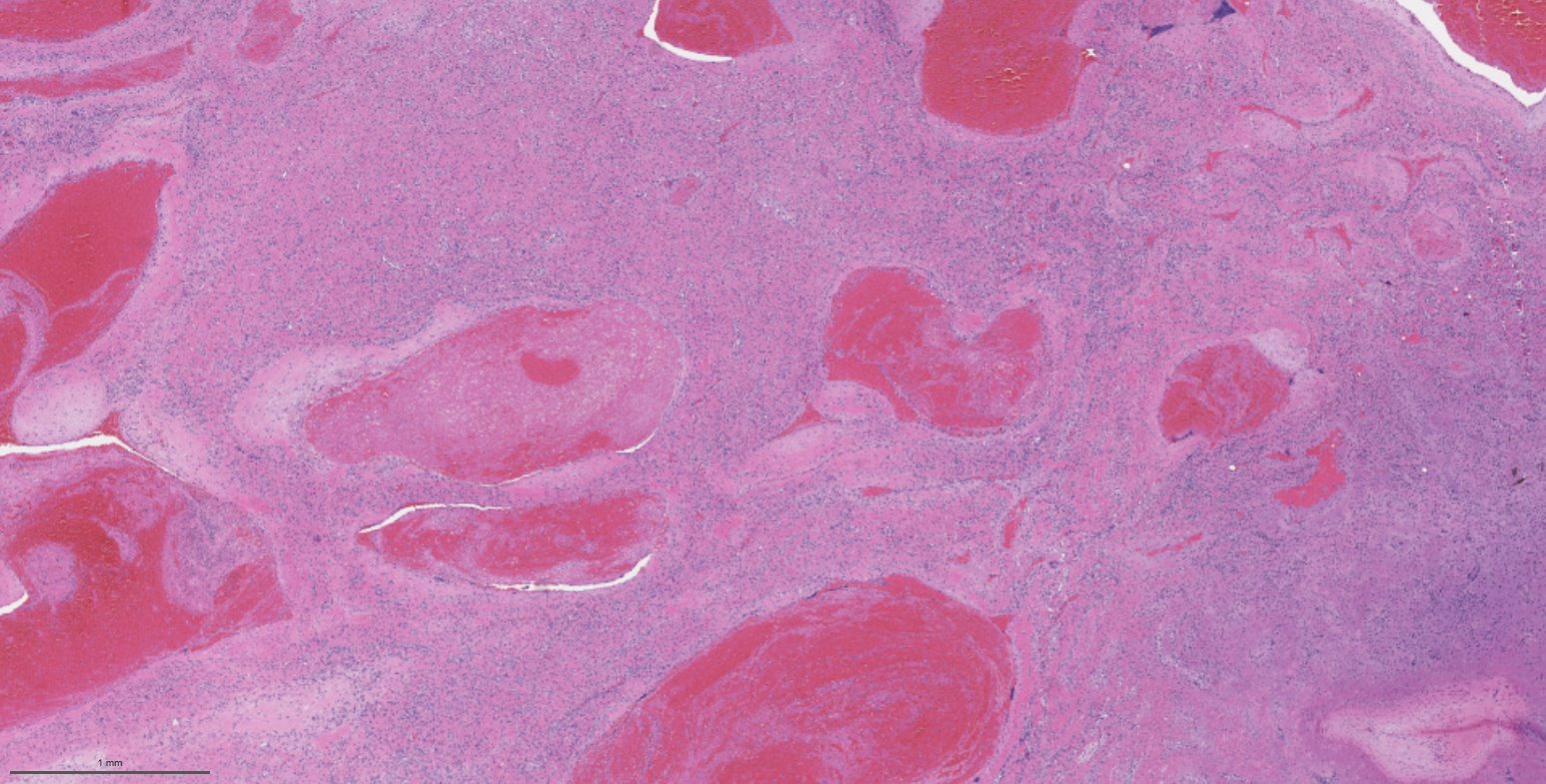
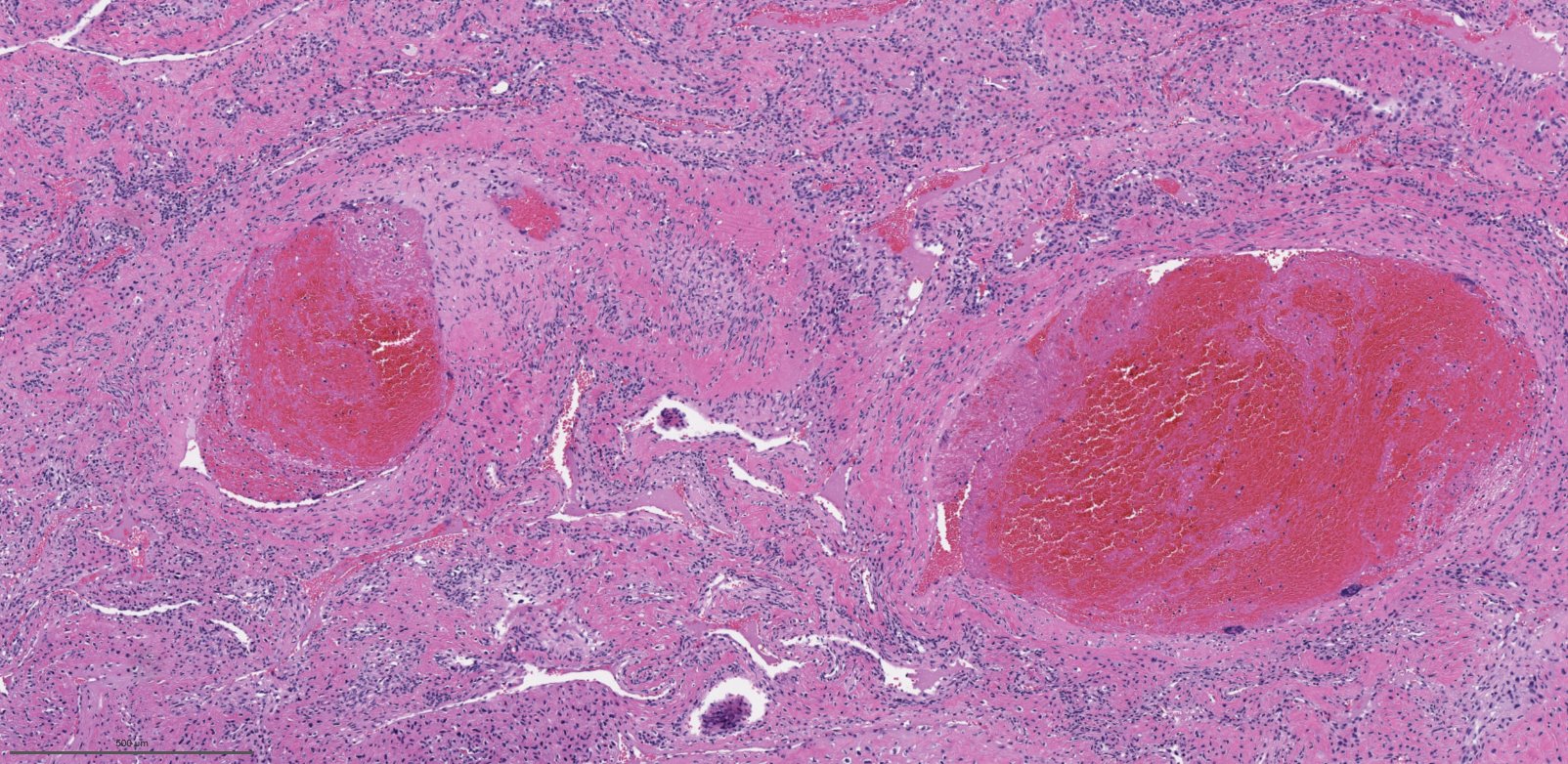
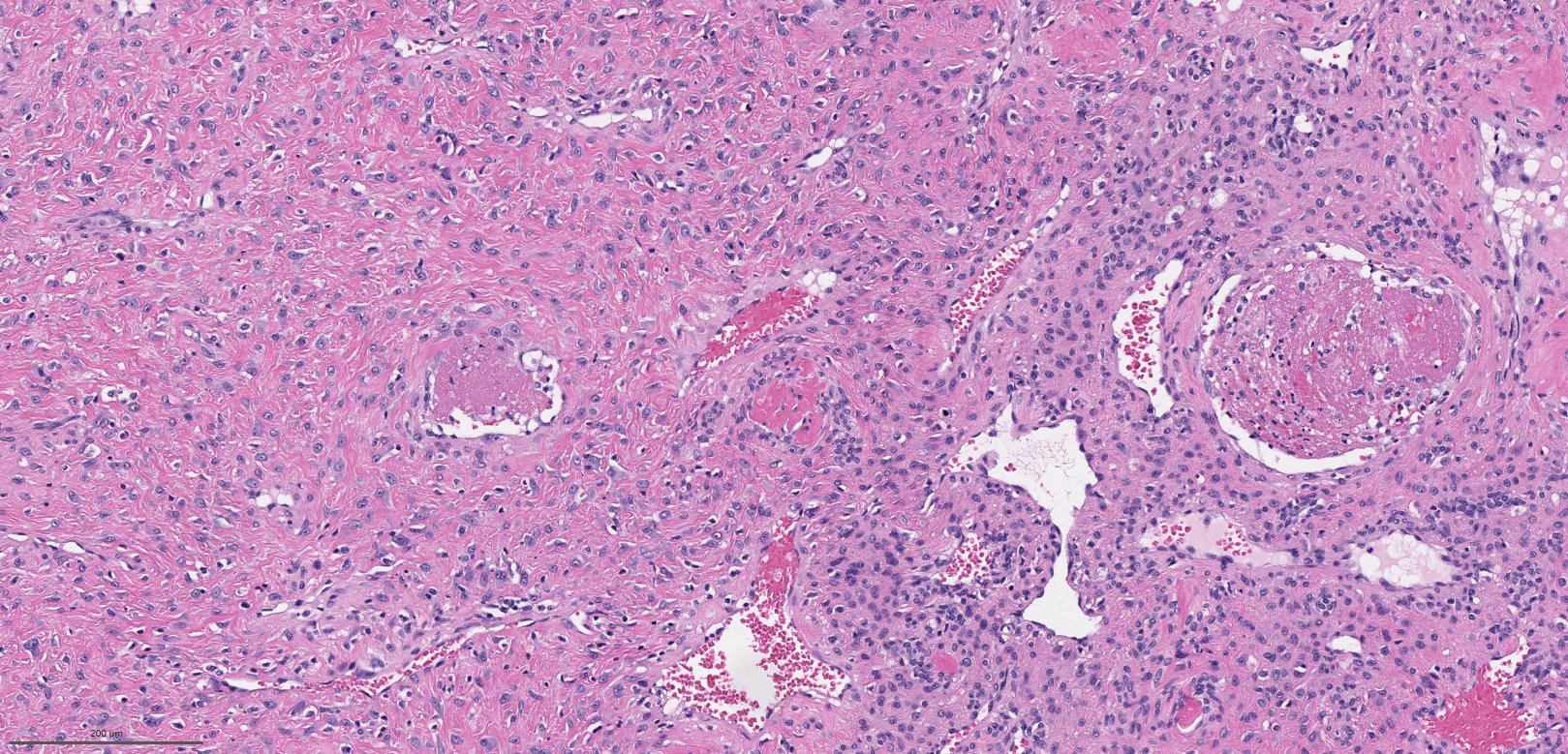
- Vascular space of various sizes, ranging from dilated branching vessel of various thickness to slit-like capillaries
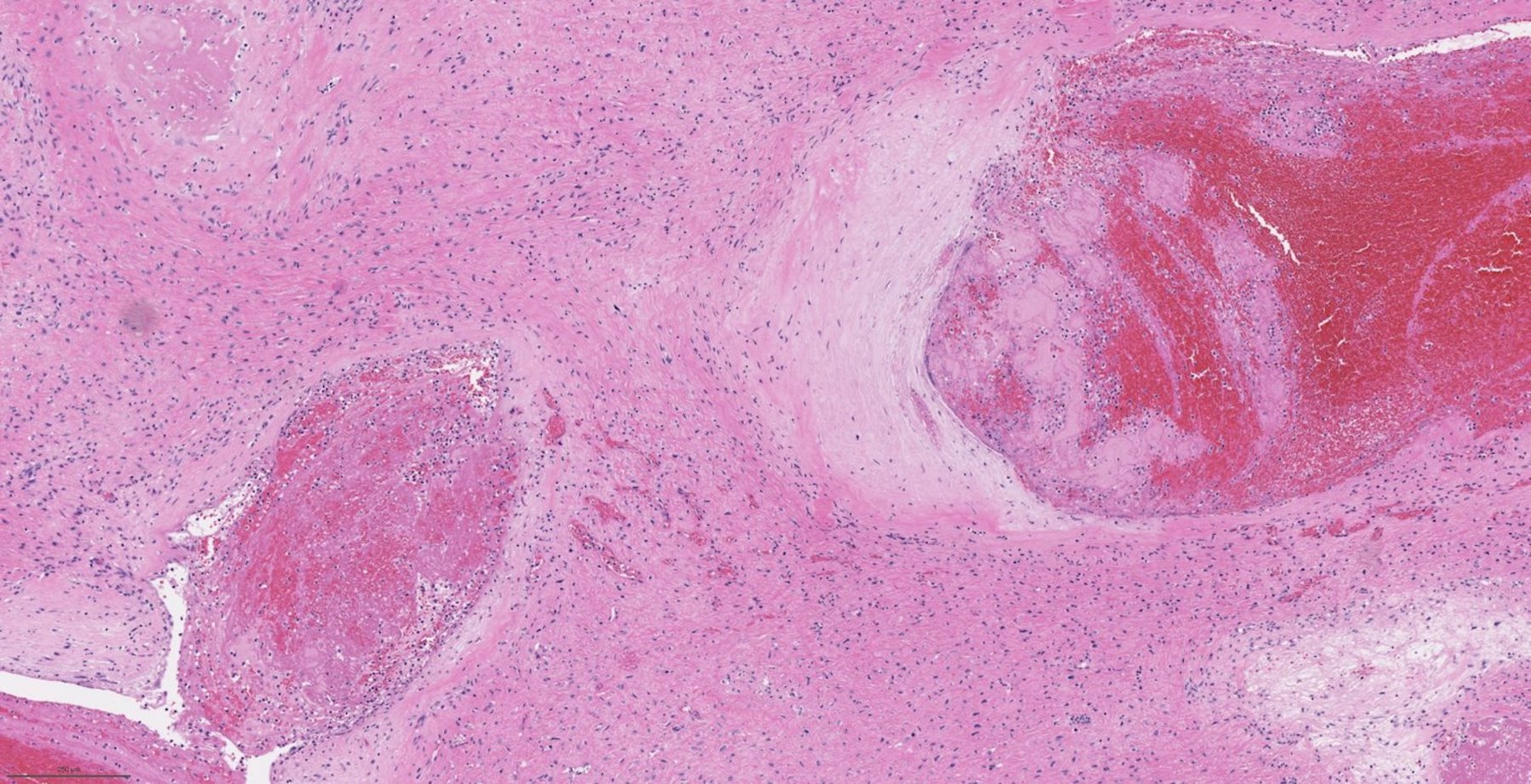
- Fibrous or collagenous stroma with fibroblasts
- Central area of the tumor is typically cellular, composed of fibroblasts or myofibroblasts with spindle, round or stellate morphology
- Stroma can be fibrous, edematous or collagenized
- Fibrinous thrombi may be seen in dilated vessels
- Frequently contain (abundant) mast cells
- Mitotic figures are usually absent
- Reference: Chan: WHO Classification of Head and Neck Tumours, 4th Edition, 2017
Microscopic (histologic) images
Contributed by Bin Xu, M.D., Ph.D.
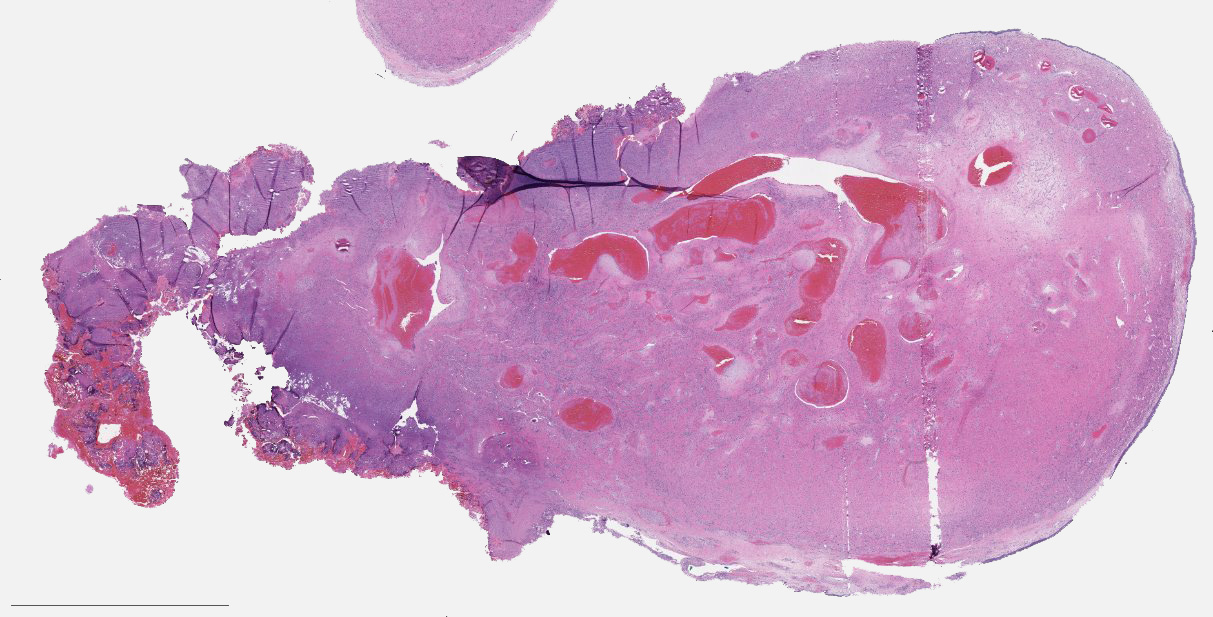
Polypoid mass
Large caliber vessels
Slit-like vasculature
Cellular stroma
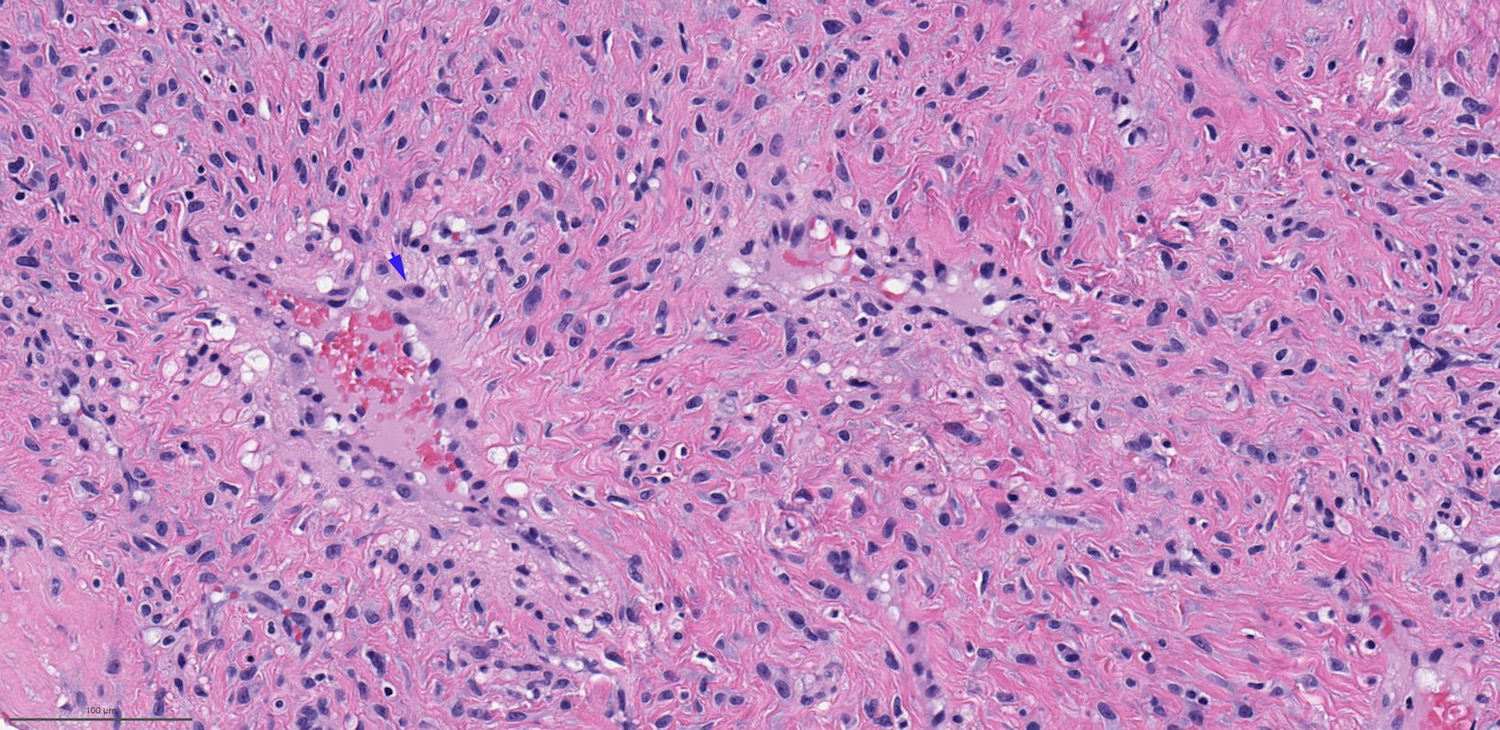
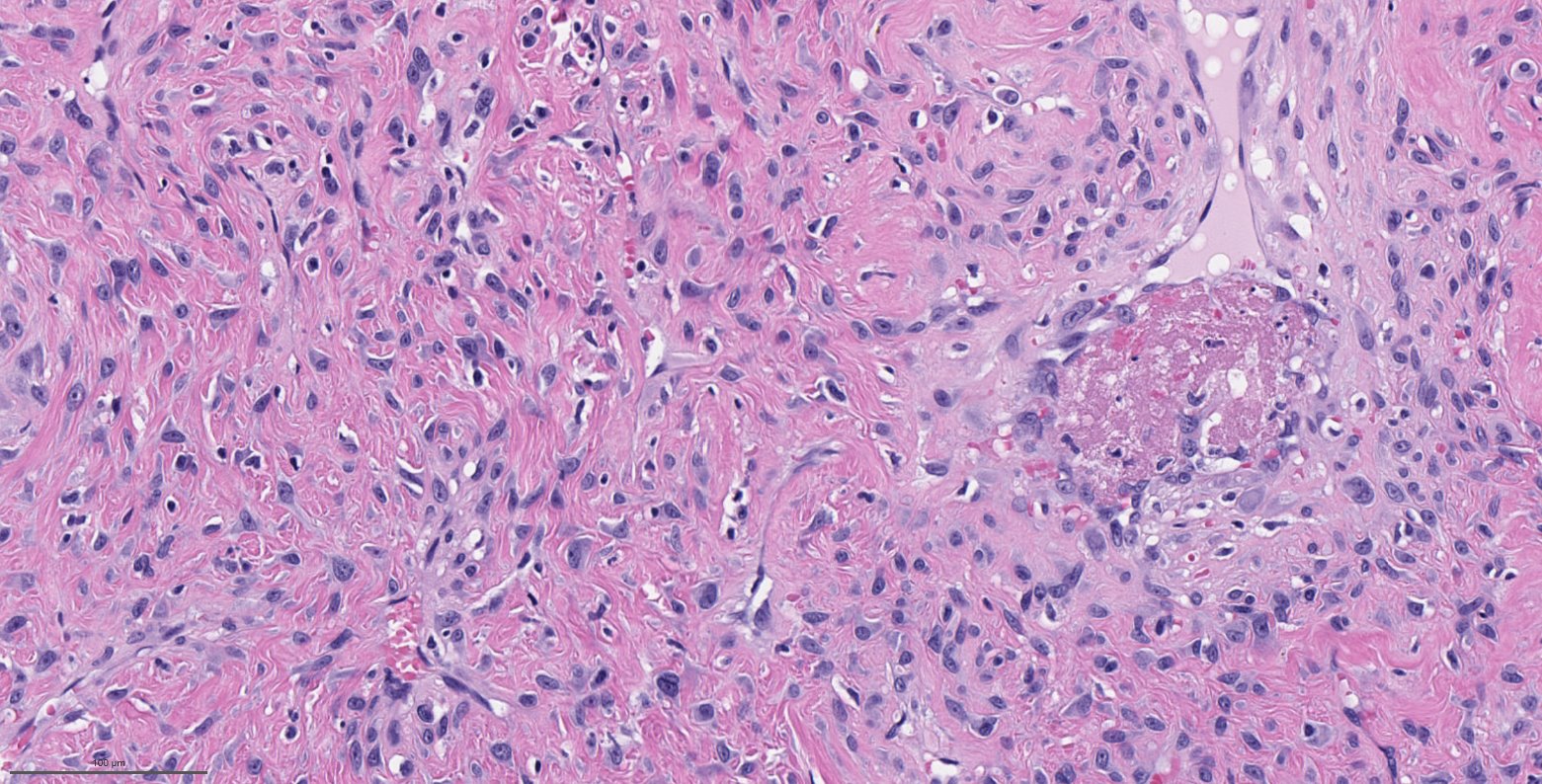
Bland fibroblasts
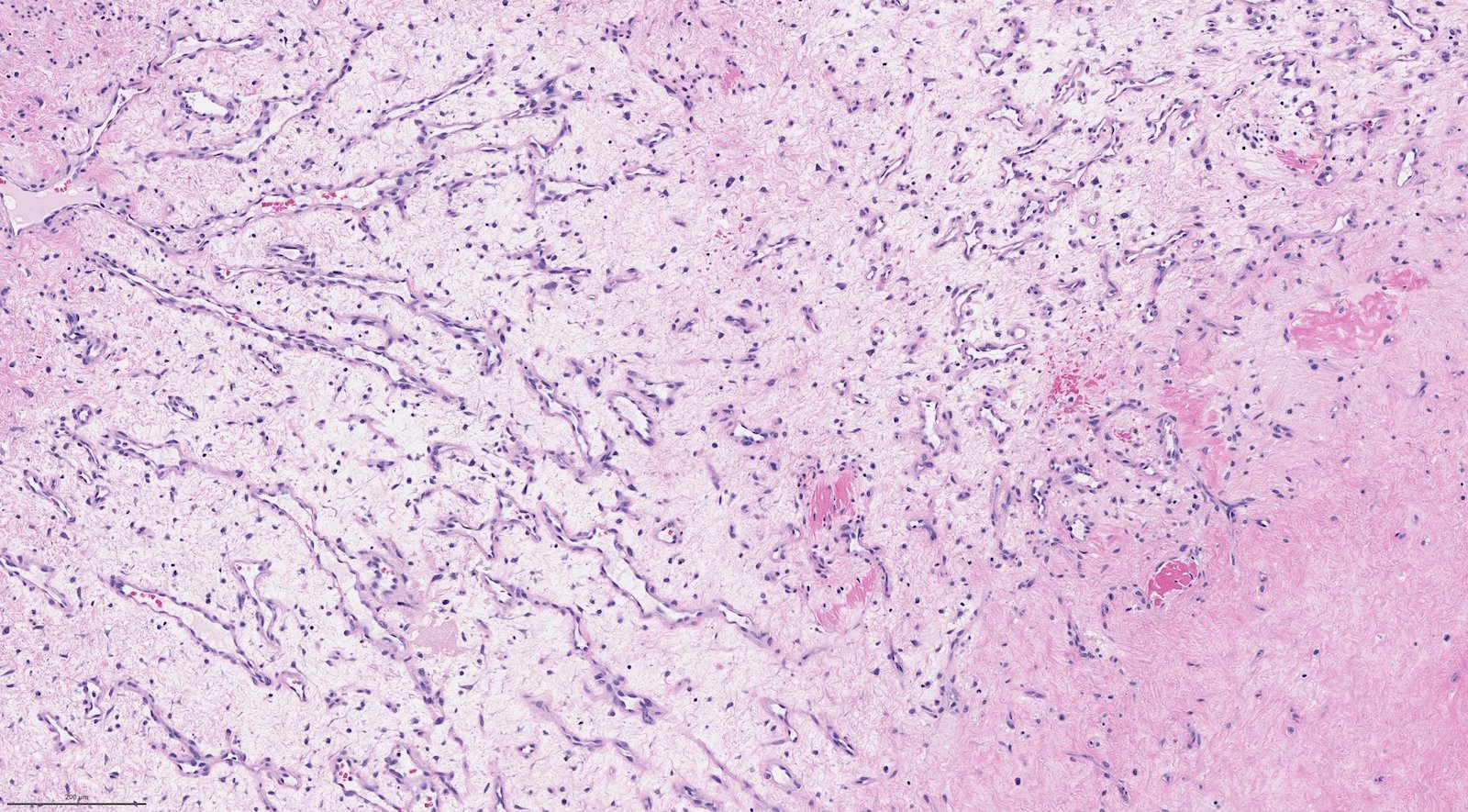
Edematous or collagenized stroma
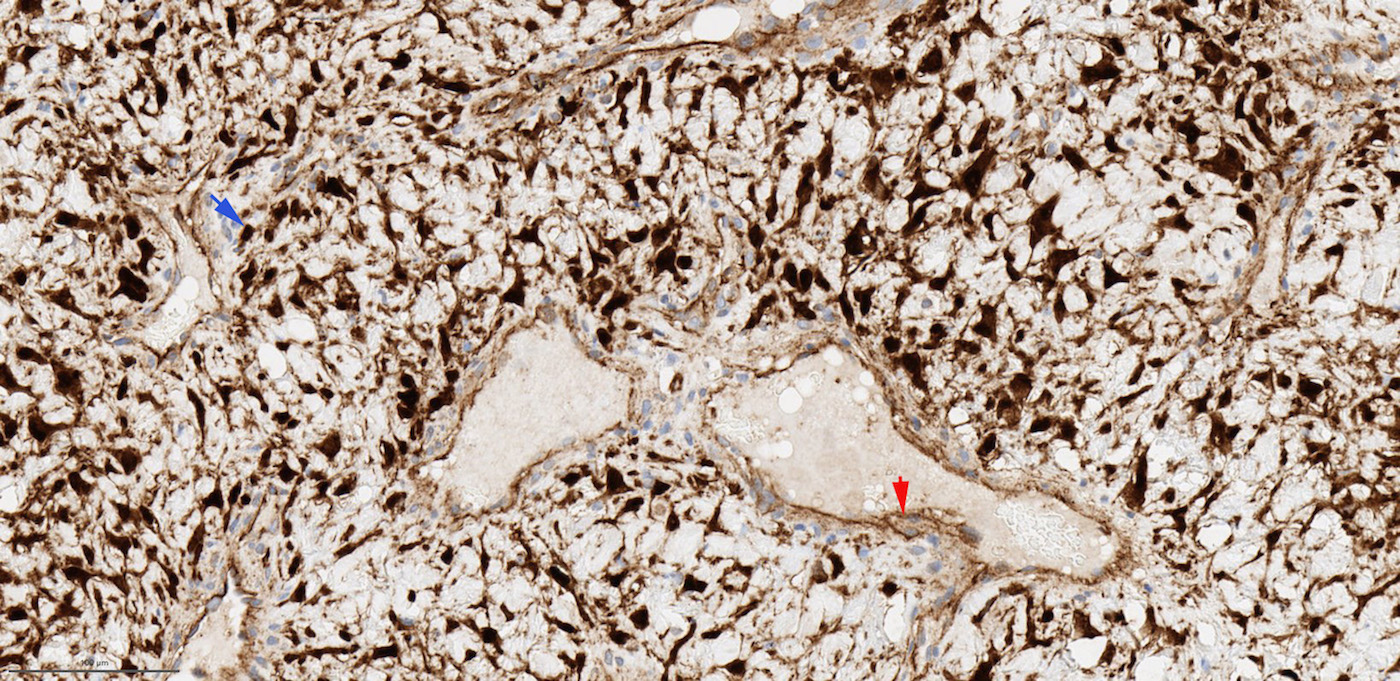
Beta catenin
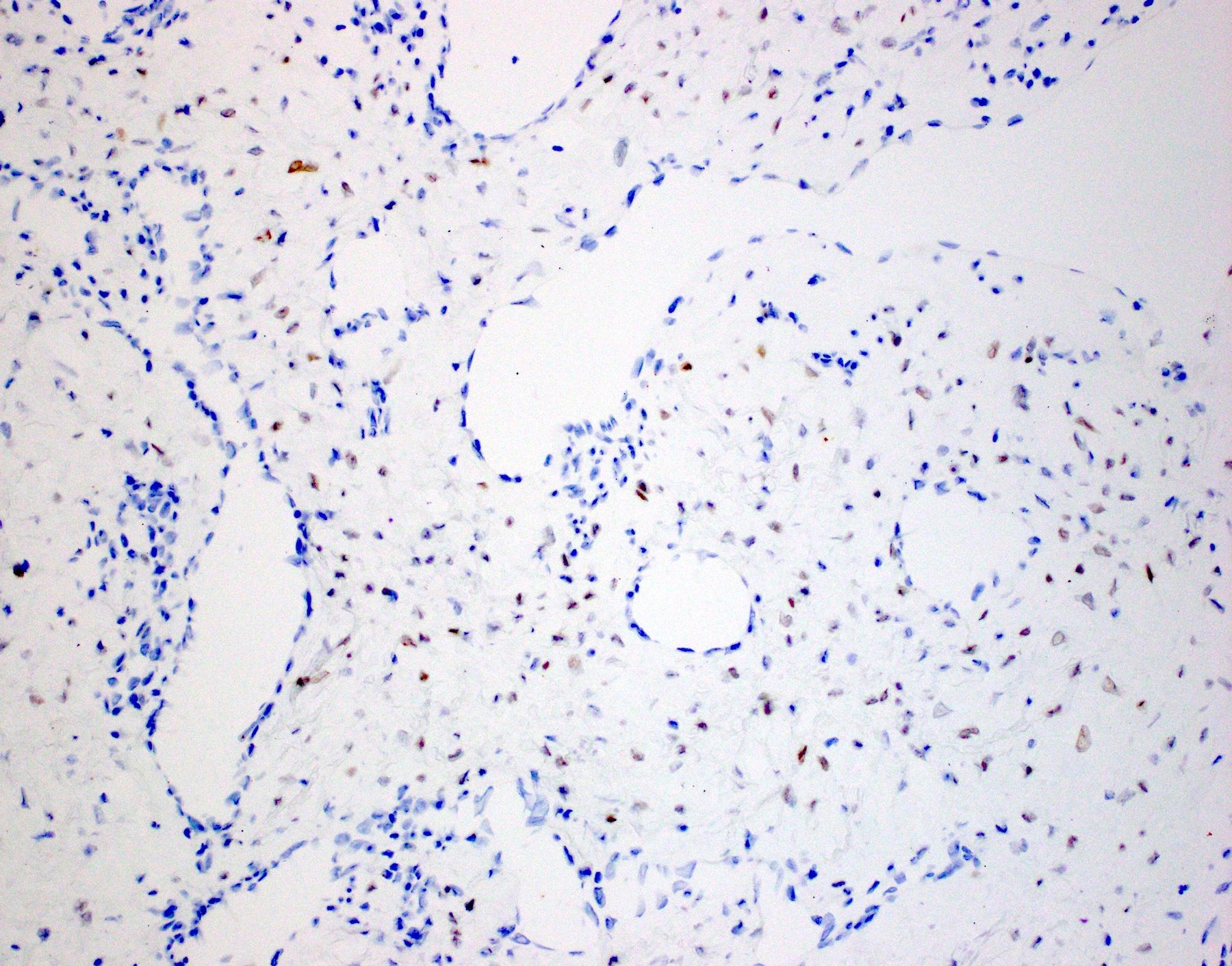
AR
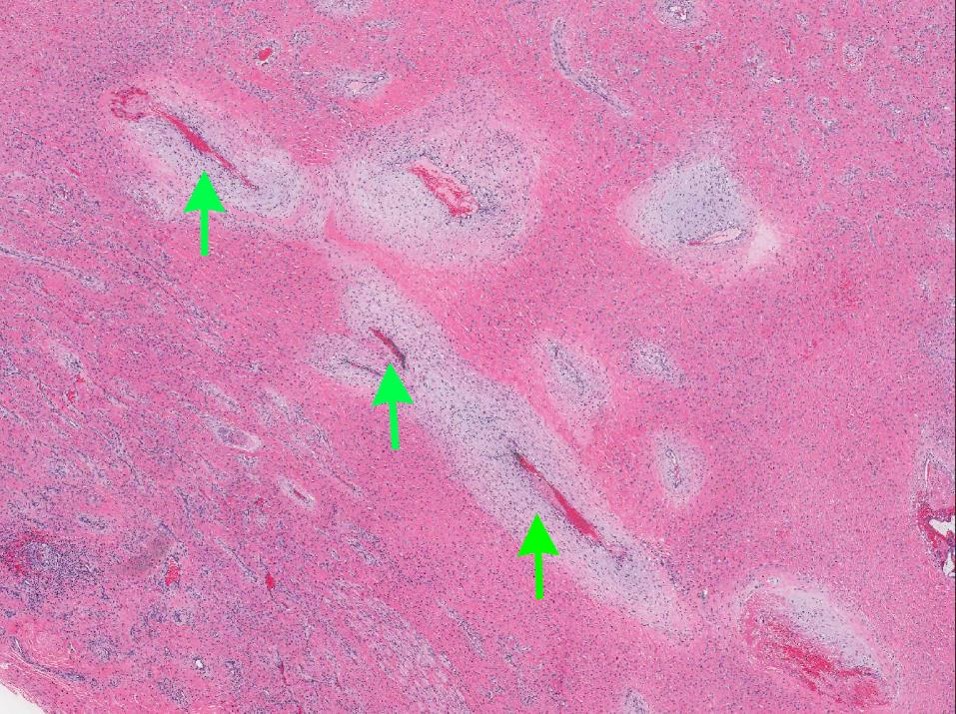
Contributed by Kelly Magliocca, D.D.S., M.P.H.
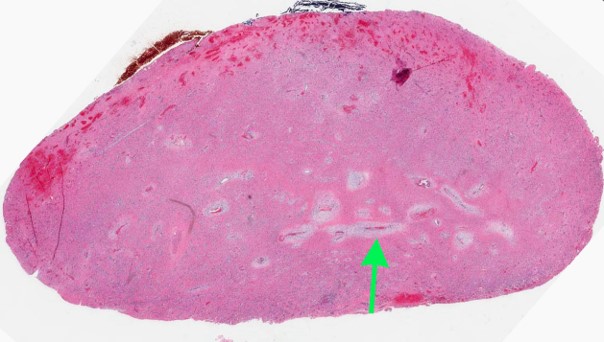
Correlate to "Gross appearance with ink"
Vascular channel, low magnification

Vascular channel, higher magnification
Cytology description
- Given the nasopharyngeal location and the highly vascular nature of the lesion, fine needle aspiration should be avoided
Positive stains
- SMA, HHF35 / h-caldesmon in smooth muscle wall of large vasculature (Pathology 2008;40:396, Head Neck Pathol 2018;12:52)
- CD31, CD34 and ERG highlight endothelial cells of vasculature
- AR is positive in stroma cells in 40 - 75% cases; the expression may be focal and weak (Acta Otolaryngol 2015;135:51, Am J Clin Pathol 2006;125:832, Mod Pathol 1998;11:1122)
- Reported positive rate of ER is highly variable, ranging from 0% to over 90% partially depending on the subunits stained (Acta Otolaryngol 2015;135:51, Am J Clin Pathol 2006;125:832)
- Beta catenin: nuclear staining in stromal cells (fibroblasts) in 70 - 90% of cases, membranous / cytoplasmic staining in endothelial cells (J Laryngol Otol 2016;130:907)
Negative stains
Molecular / cytogenetics description
- Somatic mutation of CTNNB1 (beta catenin) gene in 75% of cases (Ann Otol Rhinol Laryngol 2019;128:1061)
Sample pathology report
- Nasopharynx, resection:
- Nasopharyngeal angiofibroma, 1.8 cm, margin negative for tumor (see comment)
- Comment: Immunostain shows that the tumor is focally positive for AR. There is abnormal nuclear accumulation of beta catenin. The immunoprofile supports the diagnosis.
Differential diagnosis
- Hemangioma:
- May affect both genders, any age and is not limited to nasopharynx
- Lacks cellular stroma enriched with fibroblasts
- Vessels are typically uniform in size, whereas angiofibroma usually contains central large caliber vessels and peripheral slit-like vascular space
- Does not show AR immunopositivity or nuclear beta catenin
- Inflammatory sinonasal polyp:
- May contain fibrous to edematous stroma but usually hypocellular
- Lack rich vasculature seen in angiofibroma
- Does not show AR immunopositivity or nuclear beta catenin
- Occurs in nasal cavity or paranasal sinuses, rather than nasopharynx
- Nasal turbinate:
- Normal nasal turbinate is vascular rich, containing large caliber blood vessels with muscle wall
- Lacks hypercellular stroma and slit-like vasculatures of angiofibroma
Board review style question #1
- A 15 year old boy underwent resection of nasopharyngeal mass. Which of the following statements is true?
- It is commonly S100+ and desmin+
- It is locally aggressive with 20% risk of local recurrence
- It is typically diagnosed preoperatively using endoscopic biopsy
- It often harbors PAX3 translocation
Board review style answer #1
B. It is locally aggressive with 20% risk of local recurrence
Comment Here
Reference: Nasopharyngeal angiofibroma
Comment Here
Reference: Nasopharyngeal angiofibroma
Board review style question #2
- Which of the following statements of nasopharyngeal angiofibroma is true?
- It generally affects adolescent women
- It has a hormonal profile of ER+, PR+, AR+
- It is a benign lesion that can be safely managed by long term observation even when large
- The most frequent molecular alteration in this lesion is CTNNB1 somatic mutation
Board review style answer #2
D. The most frequent molecular alteration in this lesion is CTNNB1 somatic mutation
Comment Here
Reference: Nasopharyngeal angiofibroma
Comment Here
Reference: Nasopharyngeal angiofibroma
