

Muscle & peripheral nerve nontumor
Inflammatory myopathies
Inclusion body myositis
Last author update: 1 February 2016
Last staff update: 30 March 2021
Copyright: 2016-2024, PathologyOutlines.com, Inc.
PubMed Search: Inclusion body myositis [title] muscle



Table of Contents
Definition / general | Essential features | Terminology | Epidemiology | Sites | Clinical features | Diagnosis | Treatment | Laboratory | Radiology description | Prognostic factors | Case reports | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Differential diagnosisCite this page: Walsh M, Kresak J. Inclusion body myositis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/muscleinclusionbody.html. Accessed April 25th, 2024.
Definition / general
- An inflammatory myopathy of predominantly skeletal muscle usually seen in ages 50+
- The main histologic finding is rimmed vacuoles with accumulation of specific proteins of autophagy
Essential features
- Myopathic muscle with increased internal nuclei and myofiber size variation
- Inflammatory response is primarily centered around myofibers and is not perivascular
- "Rimmed vacuoles" are seen with Gomori trichrome stain and protein inclusions of autophagy with special stains
Terminology
- Inclusion body myositis (Lab Invest 1971;25:240), IBM, inflammatory myopathy with rimmed vacuoles
Epidemiology
- In North America, constitutes 16 - 28% of inflammatory myopathies
- Male to female ratio is 3:1
- Most occur in older individuals, although congenital and childhood forms have been described (reference)
- The average age is between 40s - 70s in men and slightly older in females
Sites
- Generally affects the proximal leg and distal arm musculature; however, any skeletal muscle can be involved
- Dysphagia can also occur
Clinical features
- This is a progressive muscle weakness with an insidious onset
- Patients may have other autoimmune disorders
- Generally, it affects proximal leg and distal arm musculature and patients can have asymmetry of their weakness
- The non-dominant side may be affected to a greater extent than the dominant side
- The most common complaint is quadriceps weakness
- Finger flexor and ankle dorsiflexion weakness can be noted clinically
- Dysphagia is a common symptom (J Neurol 2005;252:1448)
- Generally, patients do not report myalgias (muscle pain or cramps)
Diagnosis
- Muscle biopsy
- Serum creatine kinase (CK) can be normal or elevated
- Typically, patients do not have autoantibodies
Treatment
- Physical therapy and occupational therapy (exercise program) may be of some assistance (J Rehabil Med 2003;34:31)
- Recalcitrant to steroid therapy and will progress despite high dose steroids, in contrast to polymyositis, which generally responds to steroid therapy
Laboratory
- CK, aldolase and AST levels can be elevated (all are non-specific markers of muscle damage)
Radiology description
- Has a limited role for diagnosis
Prognostic factors
- Refractory to steroids or immunotherapy
- Generally, weakness slowly progresses, although complete wheelchair dependence occurs in only 3% (J Neurol 2005;252:1448)
Case reports
- 53 year old man with associated collagen vascular disease (J Neurol Neurosurg Psychiatry 1985;48:270)
- 62 year old man with dermatomyositis (Br J Dermatol 1999;141:926)
- Inclusion body myositis in connective tissue disorders (Clin Rheumatol 2003;22:324)
- Inclusion body myositis with cricopharyngeus muscle involvement and severe dysphagia (Muscle Nerve 1991;14:470)
- Macrophagic myofasciitis associated with inclusion body myositis (Neuromuscul Disord 2001;11:452)
- Creutzfeldt-Jakob disease and inclusion body myositis (Ann Neurol 2004;55:121)
- Sporadic inclusion body myositis in a patient with HTLV1 associated myelopathy (Clin Infect Dis 2001;32:510)
Microscopic (histologic) description
- Variation in myofiber sizes with small angulated myofibers, either individually or in groups
- Hypertrophied myofibers can also be seen
- An increase in internal nuclei (normal muscle can have up to 3% of myofibers having internal nuclei) can be seen
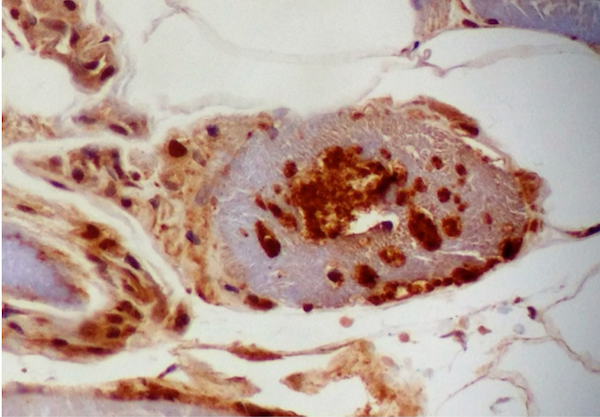
- There can be a brisk inflammatory response including CD8+ lymphocytes, which may invade non-necrotic myofibers
- Occasional myofibers undergoing phagocytosis by CD68+ macrophages can be identified
- Regenerating, basophilic myofibers can be seen
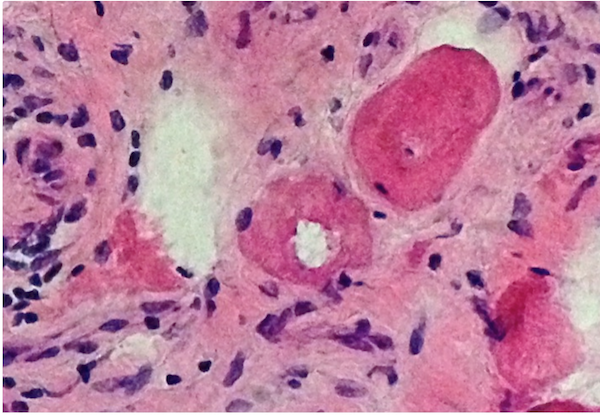
- The Gomori Trichrome stain shows "rimmed vacuoles", although the extent of myofibers having classic rimmed vacuoles varies (Dubowitz: Muscle Biopsy: A Practical Approach, 2013, 4th Edition)
- The vacuoles disrupt the myofiber architecture and can lack NADH-TR staining (Dubowitz: Muscle Biopsy: A Practical Approach, 2013, 4th Edition)
Microscopic (histologic) images
Contributed by Meggen Walsh, D.O., M.S., P.A.
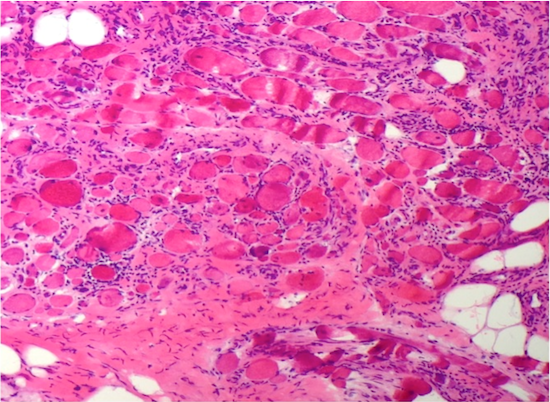
Myopathic features
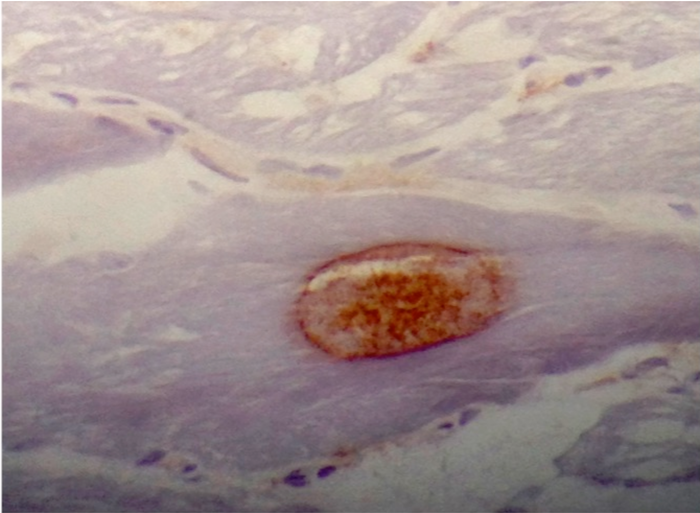
Ubiquitin
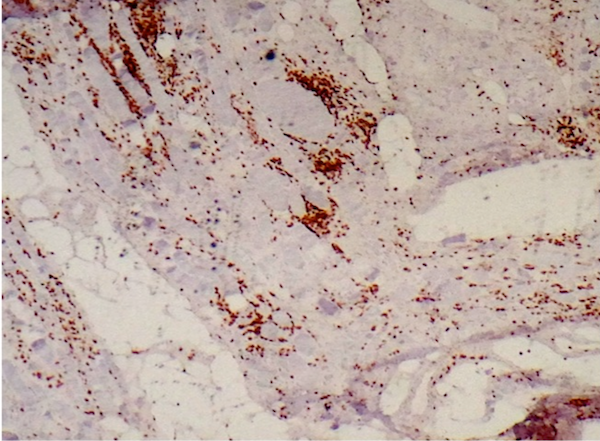
CD3
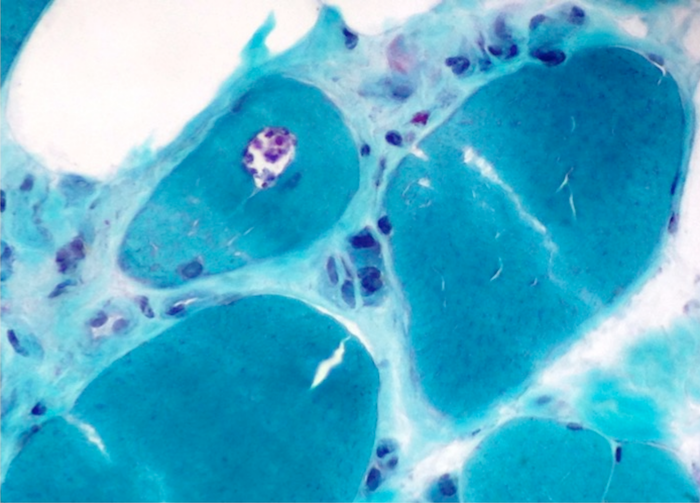
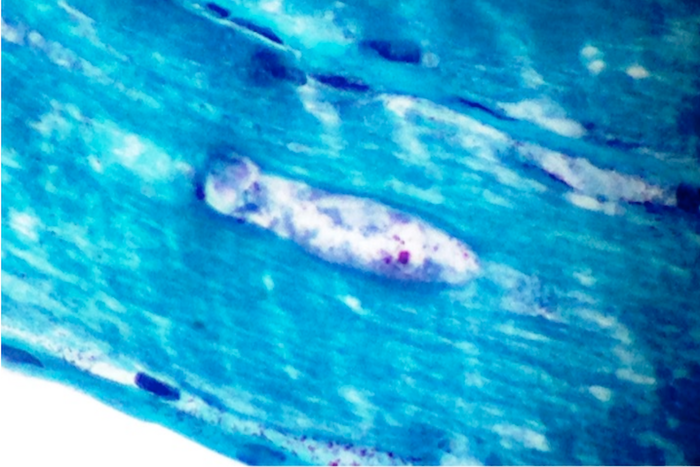
Gomori trichrome
Cytology description
- Cytology is of limited to no benefit - muscle needle biopsy may not provide a large enough sample to obtain myofibers with rimmed vacuoles
Positive stains
- Gomori trichrome shows rimmed vacuoles and can show ragged red fibers in areas
- Congo Red (amyloid) positive "apple-green" birefringence positive inclusions (Arch Neurol 1991;48:1229)
- Ubiquitin and LC3B highlight the inclusions
- Ubiquitin, B-amyloid, B-amyloid precursor protein (APP), α-synuclein, tau, TDP43, and LC3B can be seen in the inclusion bodies
- CD8+ T lymphocytes highlight the inflammatory response and infiltrate non-necrotic myofibers
Negative stains
- Rarely, cytochrome oxidase / COX negative fibers are seen
Electron microscopy description
- 15-21 nm tubulofilaments in sarcoplasm
- Mitochondria may be structurally abnormal (Yachnis: Neuropathology: A Volume in the High Yield Pathology Series, 2013, 1st Edition)
Molecular / cytogenetics description
- Associated with HLA-DR3, DR52 and B8 (Yachnis: Neuropathology: A Volume in the High Yield Pathology Series, 2013, 1st Edition)
- Upregulation of MHCI in myofibers (Dubowitz: Muscle Biopsy: A Practical Approach, 2013, 4th Edition)
Differential diagnosis
- Amyotrophic lateral sclerosis: progressive muscle weakness despite therapy, with predominantly, neurogenic changes on muscle biopsy and minimal to no inflammation
- Dermatomyositis: an inflammatory myositis, but inflammation is generally perivascular with CD4+ T cells and perifascicular myofiber atrophy
- Polymyositis: in the differential if rimmed vacuoles are not present in inflammatory myositis, because immunostudies for ubiquitin or LC3 show coarse granular staining which suggests inflammatory myositis
