

Mandible & maxilla
Cysts of the jaw
Orthokeratinized odontogenic cyst
Author: Nasir Ud Din, M.B.B.S.
Editorial Board Member: Kelly Magliocca, D.D.S., M.P.H.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 11 December 2020
Last staff update: 13 October 2023
Copyright: 2020-2025, PathologyOutlines.com, Inc.
PubMed Search: Orthokeratinized odontogenic cyst

Table of Contents
Definition / general | Essential features | Terminology | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Ud Din N. Orthokeratinized odontogenic cyst. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/mandiblemaxillaorthokeratinized.html. Accessed January 17th, 2025.
Definition / general
- A benign developmental odontogenic cyst, mostly unilocular, with a fibrous tissue wall lined predominantly or entirely by orthokeratinized stratified squamous epithelium
Essential features
- Cystic bone lesion in mandible or maxilla with compatible radiological features
- Cyst has orthokeratinized stratified squamous epithelial lining
- Cyst wall is fibrous and uninflamed
Terminology
- Previously called orthokeratinized variant of odontogenic keratocyst (OKC) (no longer recommended to use by WHO)
Epidemiology
- Comprised 10.5% of cases in series of odontogenic keratocysts (Arch Pathol Lab Med 2010;134:271)
- Comprises probably 1% of all odontogenic cysts
- Peak incidence during third and fourth decades
- More common in males (3:1) (Arch Pathol Lab Med 2010;134:271)
Sites
- Most commonly (90.16%) involves mandible (mandibular molar and ramus) (Arch Pathol Lab Med 2010;134:271)
- Maxilla involvement in 9.84% of cases
- Multiple and bilateral cases have been reported
Pathophysiology
- Thought to originate from dental lamina and its remnants; developmental in nature
Etiology
- Unknown
Clinical features
- Most present as painless asymptomatic swelling (Arch Pathol Lab Med 2010;134:271)
- Others discovered incidentally in orthodontic radiographs
Diagnosis
- Requires correlation of orthopantomogram (OPG) findings with histological features
Radiology description
- Orthopantomogram
- Well demarcated unilocular radiolucency (93%) with a corticated margin (Dentomaxillofac Radiol 2010;39:455)
- Associated with unerupted tooth in 50 - 75% of cases (Arch Pathol Lab Med 2010;134:271, Dentomaxillofac Radiol 2010;39:455)
Radiology images
Contributed by Nasir Ud Din, M.B.B.S.


Right mandible
Prognostic factors
- Overall prognosis is good
- Recurrence seen in 2% (Dentomaxillofac Radiol 2010;39:455, Arch Pathol Lab Med 2010;134:271)
Case reports
- 18 year old woman with posterior mandible calcification (J Oral Maxillofac Pathol 2018;22:S20)
- 20 and 23 year old men with multiple tumors of mandible and maxilla (Head Neck Pathol 2020;14:381)
- 41 year old man with tumor in maxilla (Turk Patoloji Derg 2017;33:81)
- 41 year old man with tumor of condylar head (Rom J Morphol Embryol 2017;58:689)
- 50 year old man with tumor of maxilla masquerading as dentigerous cyst (Int J Appl Basic Med Res 2016;6:297)
- 52 year old man with progression into squamous cell carcinoma of left mandible (World J Clin Cases 2019;7:1686)
Treatment
- Enucleation
Clinical images
Images hosted on other servers:

Extraoral swelling

Obliterated buccal sulcus
Gross description
- If an intact cyst is enucleated:
- Keratinous material filled cystic lesion
- Usually unilocular but may be multilocular
- Fibrous cyst membrane may envelope crown of molar tooth (Int J Appl Basic Med Res 2016;6:297)
- In curated specimens:
- Multiple flattened, irregular, soft to firm and pearl white to gray-white to tan-brown cystic tissue fragments
Gross images
Images hosted on other servers:

Cyst lining envelops crown of tooth
Frozen section description
- Frozen section is seldom done for odontogenic cysts
Microscopic (histologic) description
- Noninflamed fibrous cyst wall lined by thin uniform stratified squamous epithelium
- Prominent granular layer
- Thick luminal lamellated keratin (onion skin-like)
- Chevroning of lamellated keratin in some cases
- Cuboidal to flat basal layer
- No surface corrugation or basal palisading is seen
- Focal parakeratinized epithelium in case of inflammation
- Reference: Arch Pathol Lab Med 2010;134:271
Microscopic (histologic) images
Contributed by Kelly Magliocca, D.D.S., M.P.H. and Nasir Ud Din, M.B.B.S.
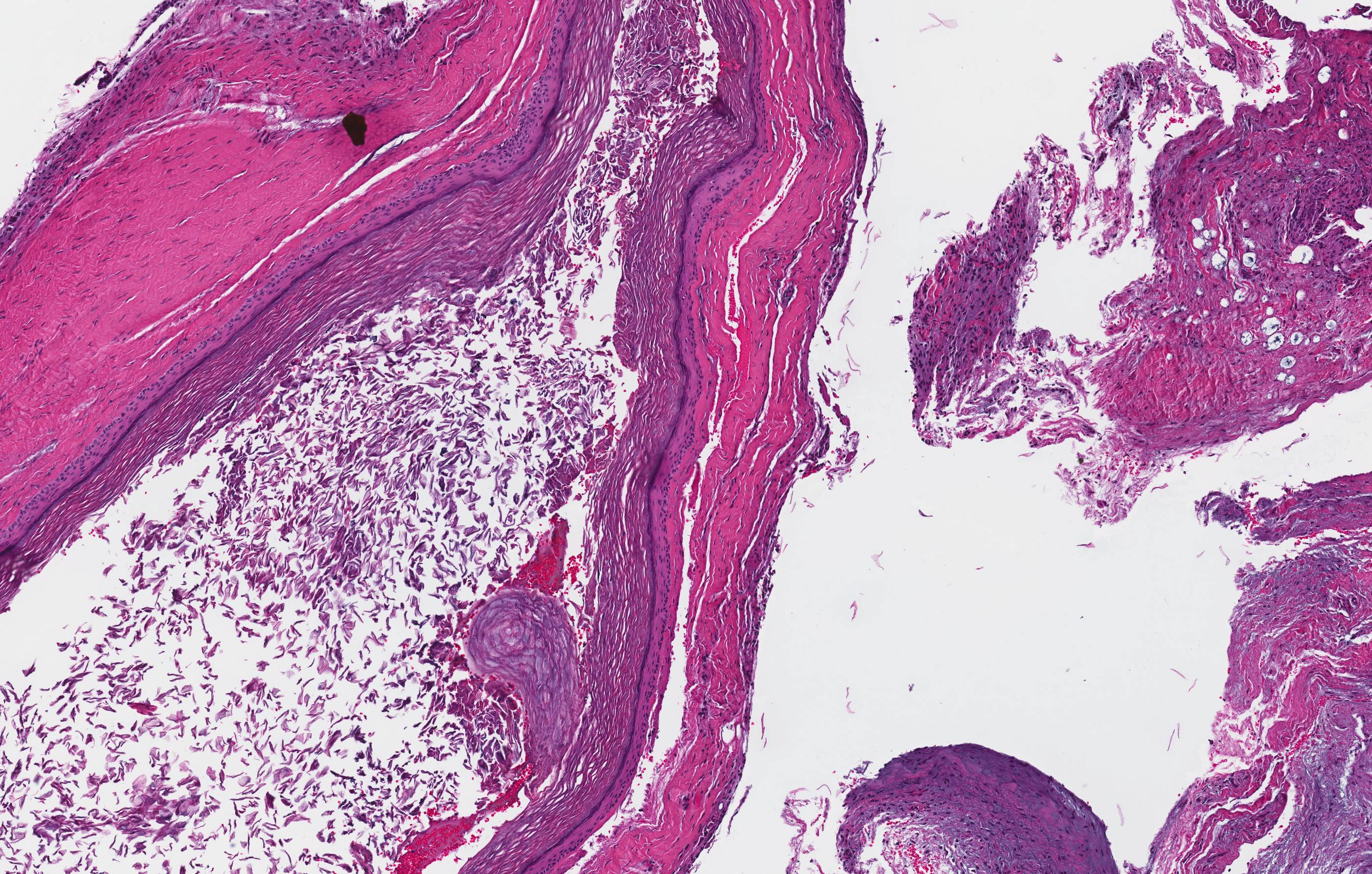
Orthokeratinized odontogenic cyst
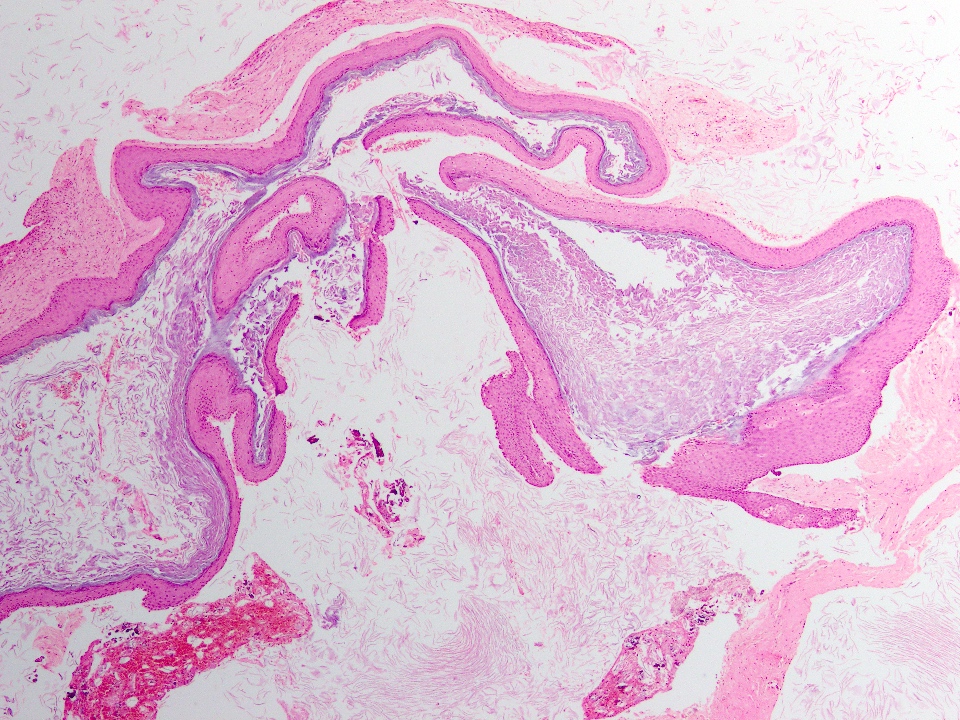
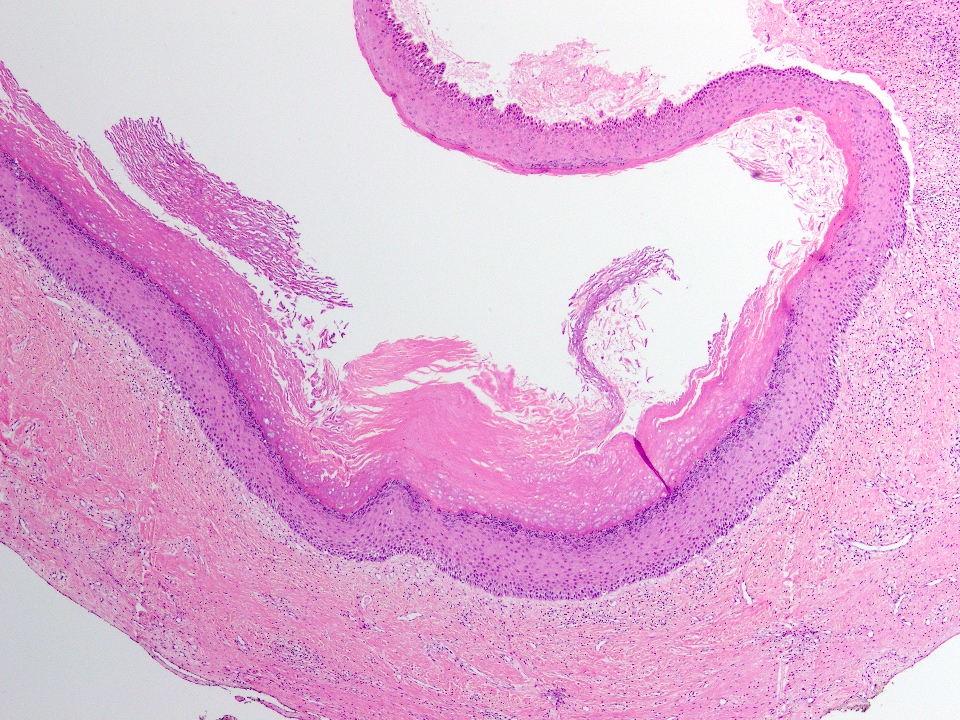
Cyst wall fragments
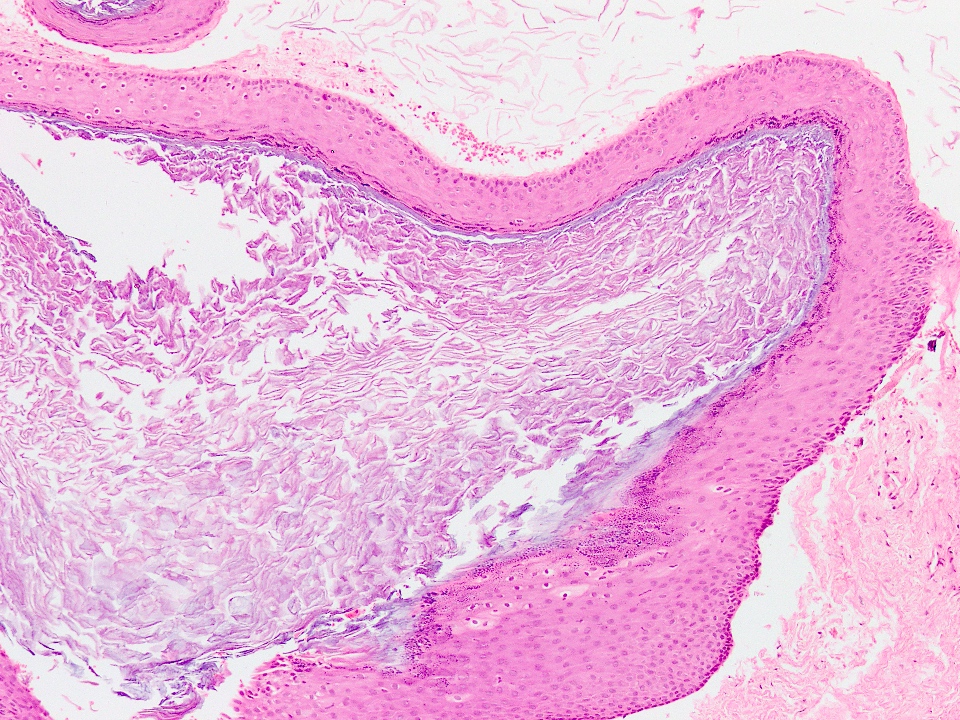
Cyst wall lumen
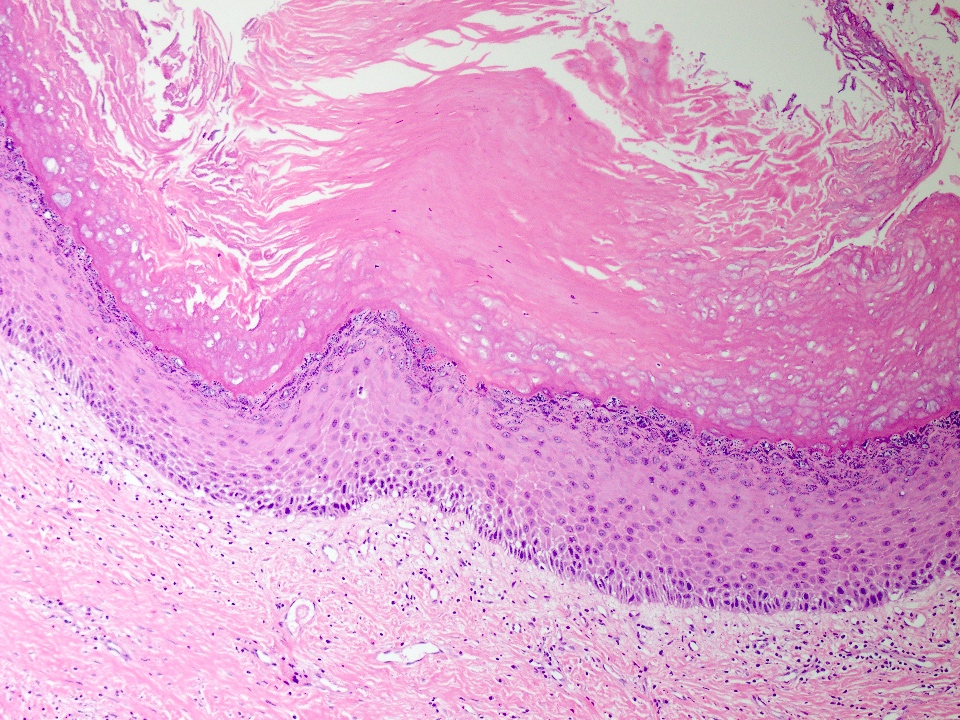
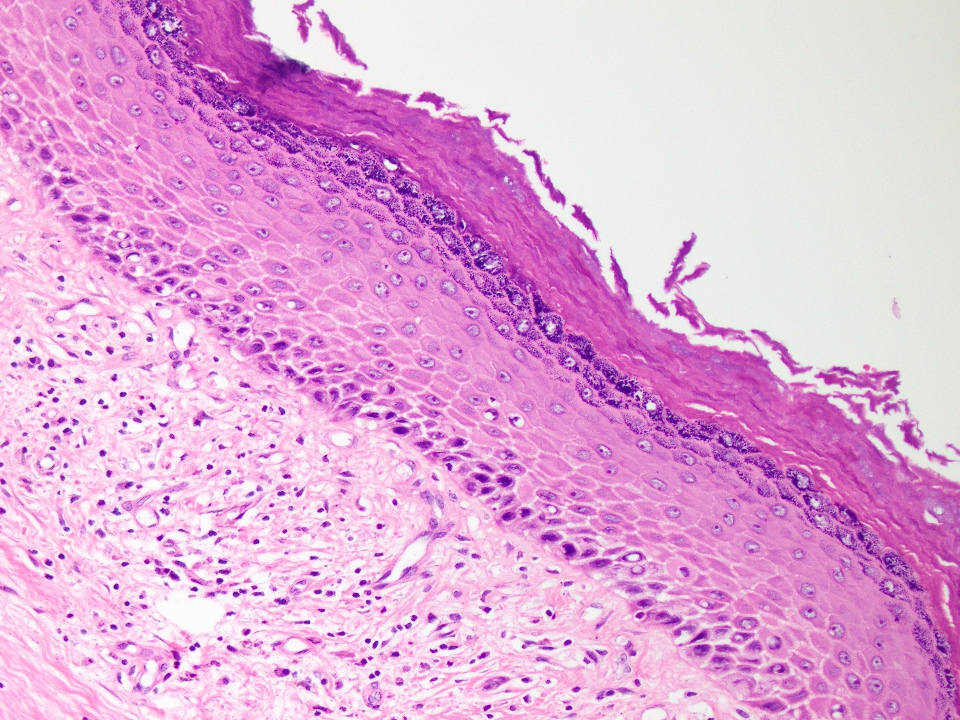
Cyst lining
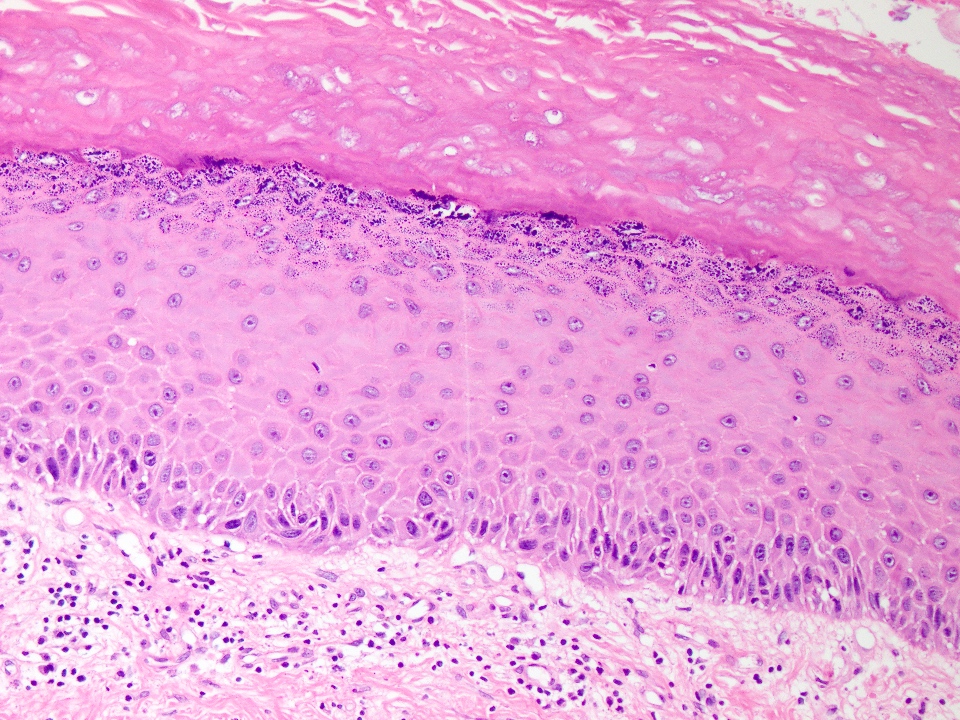
Cyst lining
Positive stains
- Immunohistochemical stains are not usually used for diagnostic purpose
- Decreased Ki67 index and p53 staining when compared with odontogenic keratocyst (Arch Pathol Lab Med 2010;134:271)
- Reduced expression of BCL2, bax, p53 and TGFα as compared with odontogenic keratocyst (Oral Oncol 2009;45:e41, Dent Res J (Isfahan) 2012;9:S39)
- Cytokeratin 10 positivity with variable expression of cytokeratin 13 and 14 (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;94:732)
- Expression of cytokeratin 1, 2, 10 and loricrin
- This profile suggests differentiation toward normal epidermis (Hum Pathol 2010;41:1718)
Sample pathology report
- Right posterior mandible, enucleation:
- Orthokeratinized odontogenic cyst (see comment)
- Comment: Histologic and radiologic features support the diagnosis.
Differential diagnosis
- Odontogenic keratocyst (OKC):
- Peak incidence in second and third decades
- Mostly solitary, unilocular, well demarcated radiolucency
- Multiple cysts in 10% of cases
- Much more common
- Associated with nevoid basal cell carcinoma syndrome
- Associated with aggressive behavior (28 - 30% recurrence)
- Thin uniform lining of parakeratinized squamous epithelium
- Corrugated layer of parakeratin on its luminal surface
- Palisaded layer of columnar basal cells (reverse polarity)
- No keratohyalin granules
- Lumen may contain keratinaceous debris
- Frequent separation of the epithelial lining from underlying connective tissue
- Dental lamina rests and microcysts occasionally present in capsule wall
- Dentigerous cyst (DC):
- Radiologically similar as both are associated with unerupted molar tooth of mandible
- Much more common
- Peak incidence in second to fourth decades of life
- Noninflamed lining is thin; 2 - 3 layers of regular nonkeratinizing stratified squamous epithelium
- Inflamed lining is hyperplastic with elongated rete ridges
- Mucus metaplasia and cilia are also seen
Additional references
Board review style question #1
The most important histological feature to differentiate orthokeratinized odontogenic cyst (see image) from odontogenic keratocyst is
- Absence of parakeratin
- Orthokeratinized squamous epithelium with prominent granular layer
- Presence of luminal lamellated keratin
- Thick stratified squamous epithelium
- Uninflamed fibrous cyst wall
Board review style answer #1
B. Orthokeratinized squamous epithelium with prominent granular layer
Comment Here
Reference: Orthokeratinized odontogenic cyst
Comment Here
Reference: Orthokeratinized odontogenic cyst
Board review style question #2
Which of the following cysts most closely mimics orthokeratinized odontogenic cyst radiologically?
- Calcifying epithelial odontogenic cyst
- Dentigerous cyst
- Lateral periodontal cyst
- Odontogenic keratocyst
- Radicular cyst
Board review style answer #2
Board review style question #3
The most important histological feature to differentiate orthokeratinized odontogenic cyst from dentigerous cyst is
- Absence of basal palisading
- Elongated rete ridges
- Orthokeratinzed granular squamous epithelium
- Thick stratified squamous epithelium
- Uninflamed fibrous wall
Board review style answer #3
C. Orthokeratinzed granular squamous epithelium
Comment Here
Reference: Orthokeratinized odontogenic cyst
Comment Here
Reference: Orthokeratinized odontogenic cyst

