

Mandible & maxilla
Benign odontogenic tumors
Odontogenic myxoma / fibromyxoma
Author: Abberly Lott Limbach, M.D.
Editorial Board Member: Molly Housley Smith, D.M.D.
Deputy Editor-in-Chief: Kelly Magliocca, D.D.S., M.P.H.

Last author update: 29 November 2023
Last staff update: 29 November 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Odontogenic myxoma / fibromyxoma

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Lott Limbach A. Odontogenic myxoma / fibromyxoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/mandiblemaxillamyxoma.html. Accessed December 24th, 2024.
Definition / general
- Rare, benign odontogenic neoplasm resembling odontogenic ectomesenchyme
- Characterized by bland spindled to stellate cells in myxoid stroma
- Requires radiographic and clinical correlation to differentiate from a dental follicle / papilla
- References: Head Neck Pathol 2020;14:1021, J Oral Surg 1975;33:523, Eur J Clin Invest 2020;50:e13214, Oral Dis 2019;25:676
Essential features
- Stellate, spindle shaped, round cells arranged haphazardly in abundant, fibrillary myxoid / mucoid stroma with infiltration into surrounding bone
- Radiolucent lesion with thin, fine, coarse or wispy trabeculae of residual bone arranged perpendicular to one another (tennis racket or soap bubble appearance)
- Recurrence is common due to infiltrative nature of the neoplasm
Terminology
- Odontogenic myxoma
- Odontogenic fibromyxoma
ICD coding
- ICD-O: 9320/0 - odontogenic myxoma
- ICD-10
- ICD-11
- 2E83.0 & XH48L4 - benign osteogenic tumors of bone or articular cartilage of skull or face & odontogenic myxoma
- 2E83.1 & XH48L4 - benign osteogenic tumors of bone or articular cartilage of lower jaw & odontogenic myxoma
Epidemiology
- Incidence is 0.5 - 17.7% of all odontogenic tumors of the jaw (Head Neck Pathol 2020;14:1021, Eur J Clin Invest 2020;50:e13214, J Oral Pathol Med 2016;45:599)
- Wide age range but generally occurs in second and third decades (Head Neck Pathol 2020;14:1021, Eur J Clin Invest 2020;50:e13214)
- More common in women but may vary by population (Head Neck Pathol 2020;14:1021, Eur J Clin Invest 2020;50:e13214, Oral Dis 2019;25:676, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:101)
Sites
- More common in mandible (67%) than maxilla (33%) (Head Neck Pathol 2020;14:1021)
- In both the mandible and maxilla, more common posteriorly (Eur J Clin Invest 2020;50:e13214)
Pathophysiology
- Not well described
- May originate from the primitive mesenchymal portion of a developing tooth or periodontal membrane (J Oral Surg 1975;33:523, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:101)
- May result from myxomatous degeneration of odontogenic fibroma (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:101)
Etiology
- Unknown
Clinical features
- Often asymptomatic, incidentally discovered by imaging (Head Neck Pathol 2020;14:1021, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:101)
- Can present with slow growing swelling, rarely pain (Head Neck Pathol 2020;14:1021, Oral Dis 2019;25:676)
Diagnosis
- Diagnosis is often made by radiographical evaluation and correlated clinical and pathologic findings (Head Neck Pathol 2020;14:1021, Eur J Clin Invest 2020;50:e13214)
Radiology description
- Unilocular or multilocular radiolucency (Head Neck Pathol 2020;14:1021, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:101, Int J Dent 2021:2021:1093412)
- Variable margins from well defined and corticated to poorly defined scalloped (Head Neck Pathol 2020;14:1021)
- Characteristic radiographic finding of thin, fine, coarse or wispy trabeculae of residual bone arranged perpendicular to one another (tennis racket or soap bubble appearance) (Head Neck Pathol 2020;14:1021, Eur J Clin Invest 2020;50:e13214)
Radiology images
Images hosted on other servers:

Multilocular, radiolucent lesion

Right mandibular lateral occlusal view

Multilocular radiolucent osteolytic lesion

CT scan of mandible
Prognostic factors
- Recurrence rates are variable, 10 - 43% and related to extent of excision (Head Neck Pathol 2020;14:1021, Eur J Clin Invest 2020;50:e13214)
Case reports
- 14 year old boy with maxillary mass (BMJ Case Rep 2020;13:e234933)
- 18 year old man with maxillary mass (J Clin Diagn Res 2015;9:ZD29)
- 22 year old woman with right mandibular mass (Head Neck Pathol 2018;12:44)
- 28 year old woman and 36 year old man both with maxillary masses (Contemp Clin Dent 2015;6:131)
Treatment
- Surgical excision is mainstay of treatment (Head Neck Pathol 2020;14:1021, Eur J Clin Invest 2020;50:e13214, Oral Dis 2019;25:676, J Clin Exp Dent 2021;13:e637)
- Varies from curettage to surgical resection with 1 cm wide margin (Oral Dis 2019;25:676)
Clinical images
Images hosted on other servers:

Swelling on the right side

Mandibular right quadrant

Gray-white appearance
Gross description
- Whitish gray gelatinous loose structure (Head Neck Pathol 2020;14:1021)
Gross images
Contributed by Kelly Magliocca, D.D.S., M.P.H.
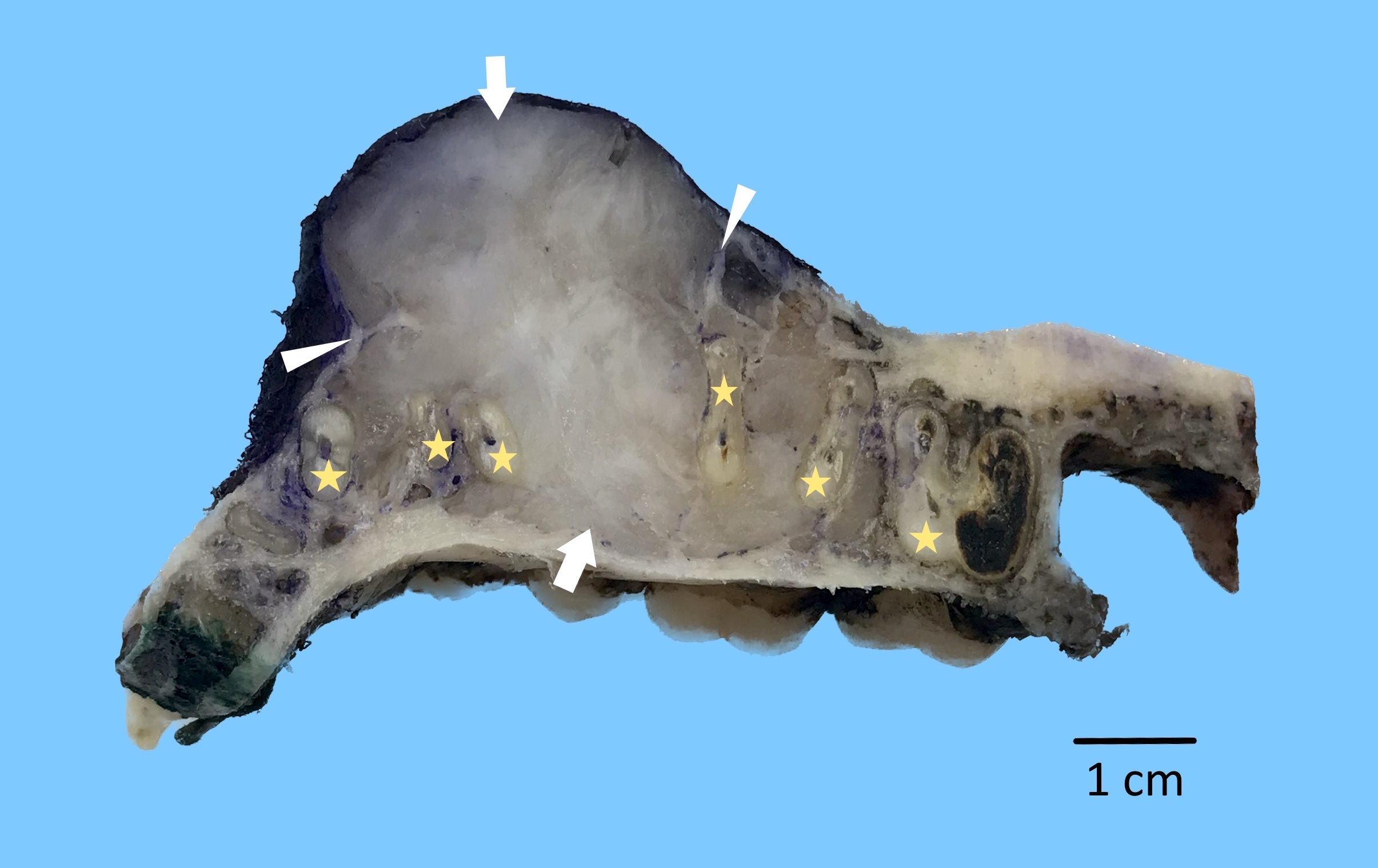
Mandibular myxoma resection
Images hosted on other servers:

Jelly-like appearance
Microscopic (histologic) description
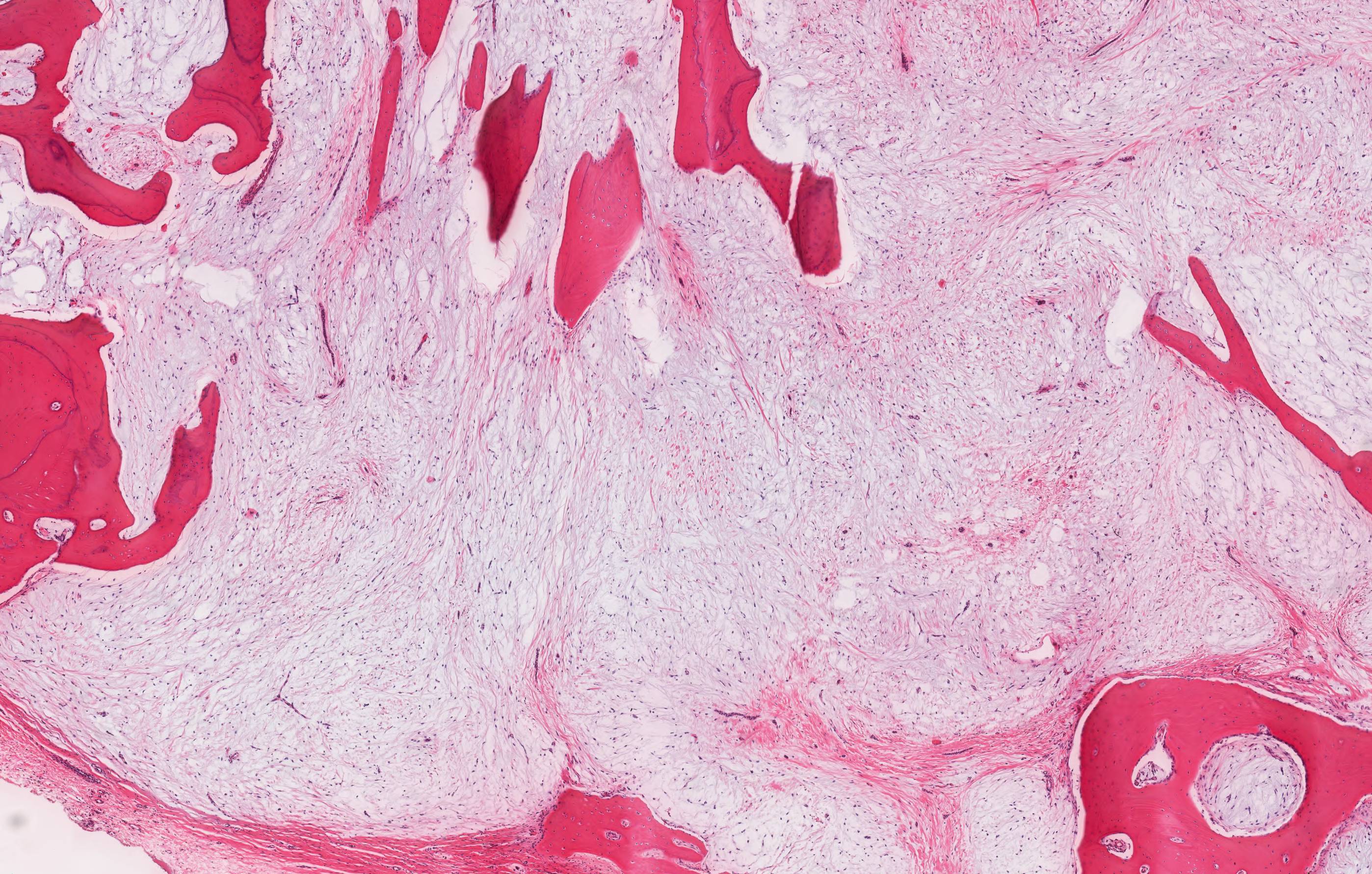
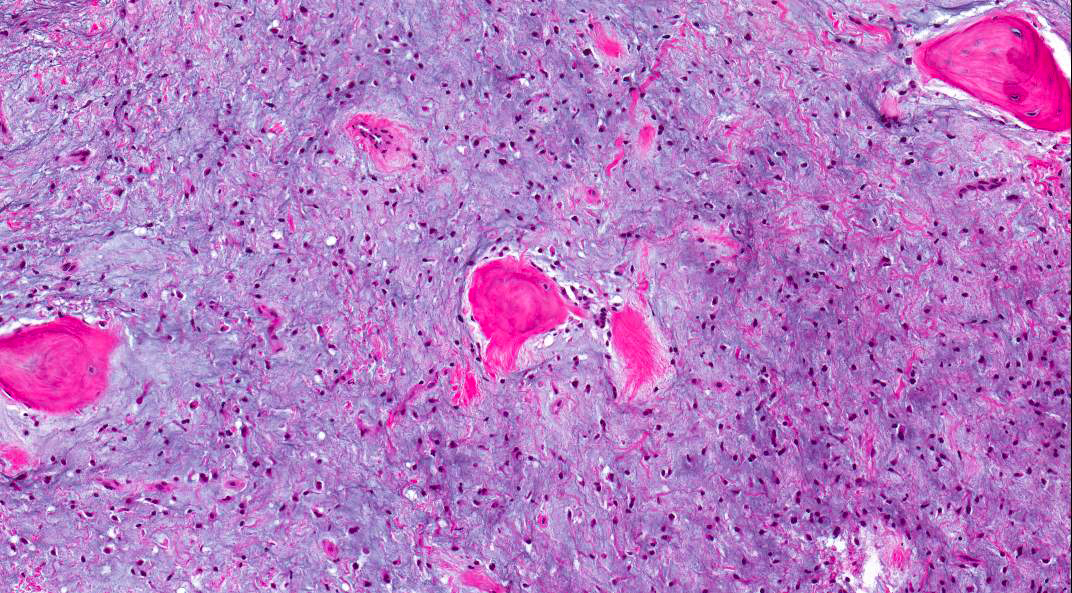
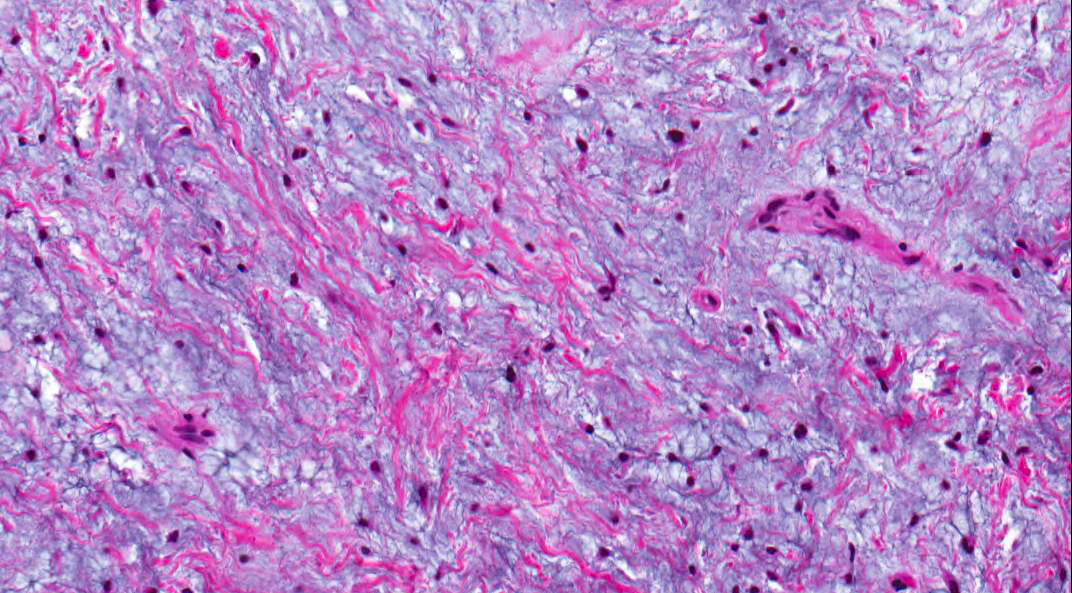
- Stellate, spindle shaped, round cells arranged haphazardly in abundant, fibrillary myxoid / mucoid stroma (Head Neck Pathol 2020;14:1021)
- Infiltrates surrounding bone (Eur J Clin Invest 2020;50:e13214)
- Small islands of inactive odontogenic epithelial rests can be seen (Head Neck Pathol 2020;14:1021)
- If abundant collagen is present, the term fibromyxoma is used (Head Neck Pathol 2020;14:1021, Eur J Clin Invest 2020;50:e13214)
Microscopic (histologic) images
Contributed by Abberly Lott Limbach, M.D. and Kelly Magliocca, D.D.S., M.P.H.
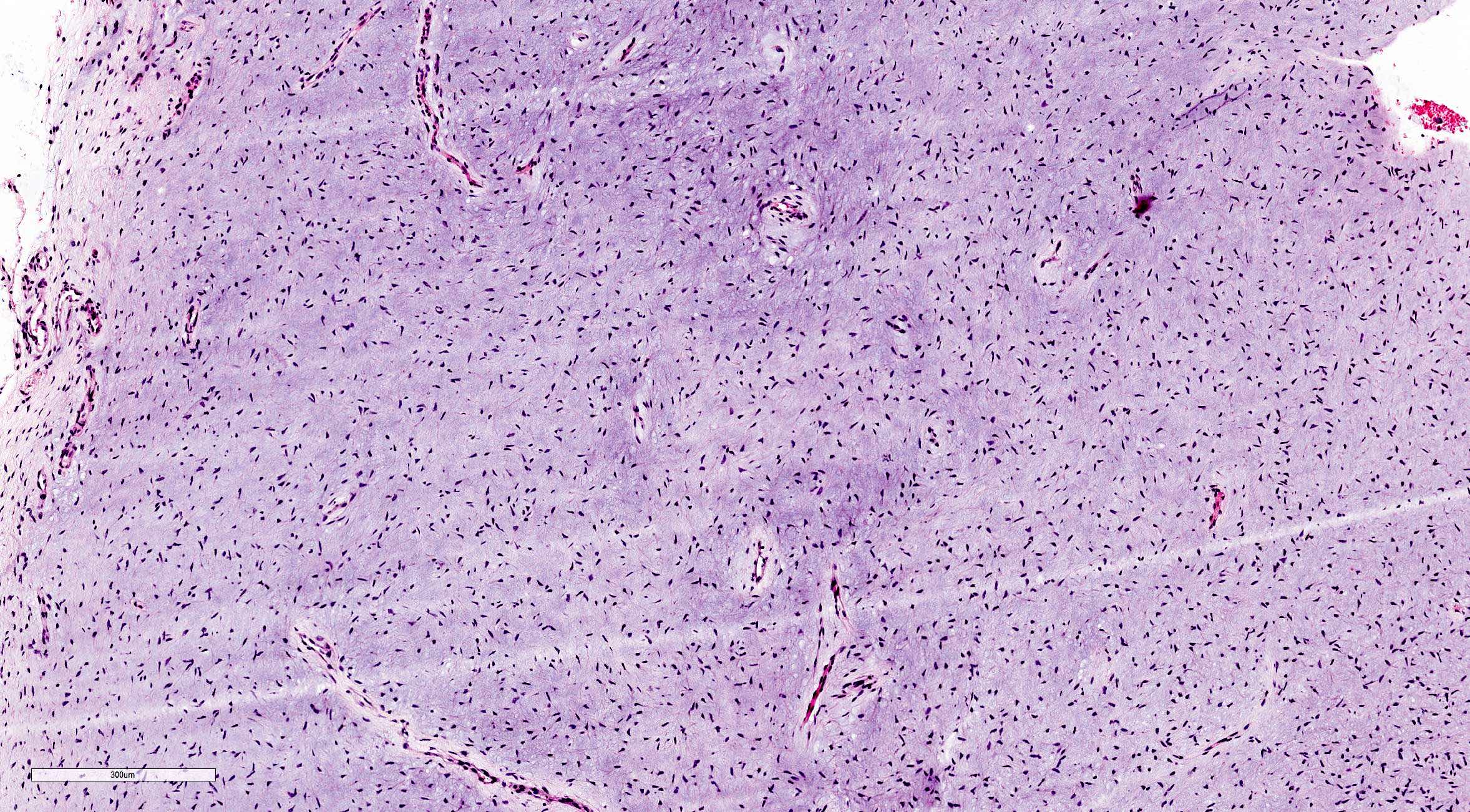
Myxoid background with bland spindle cells
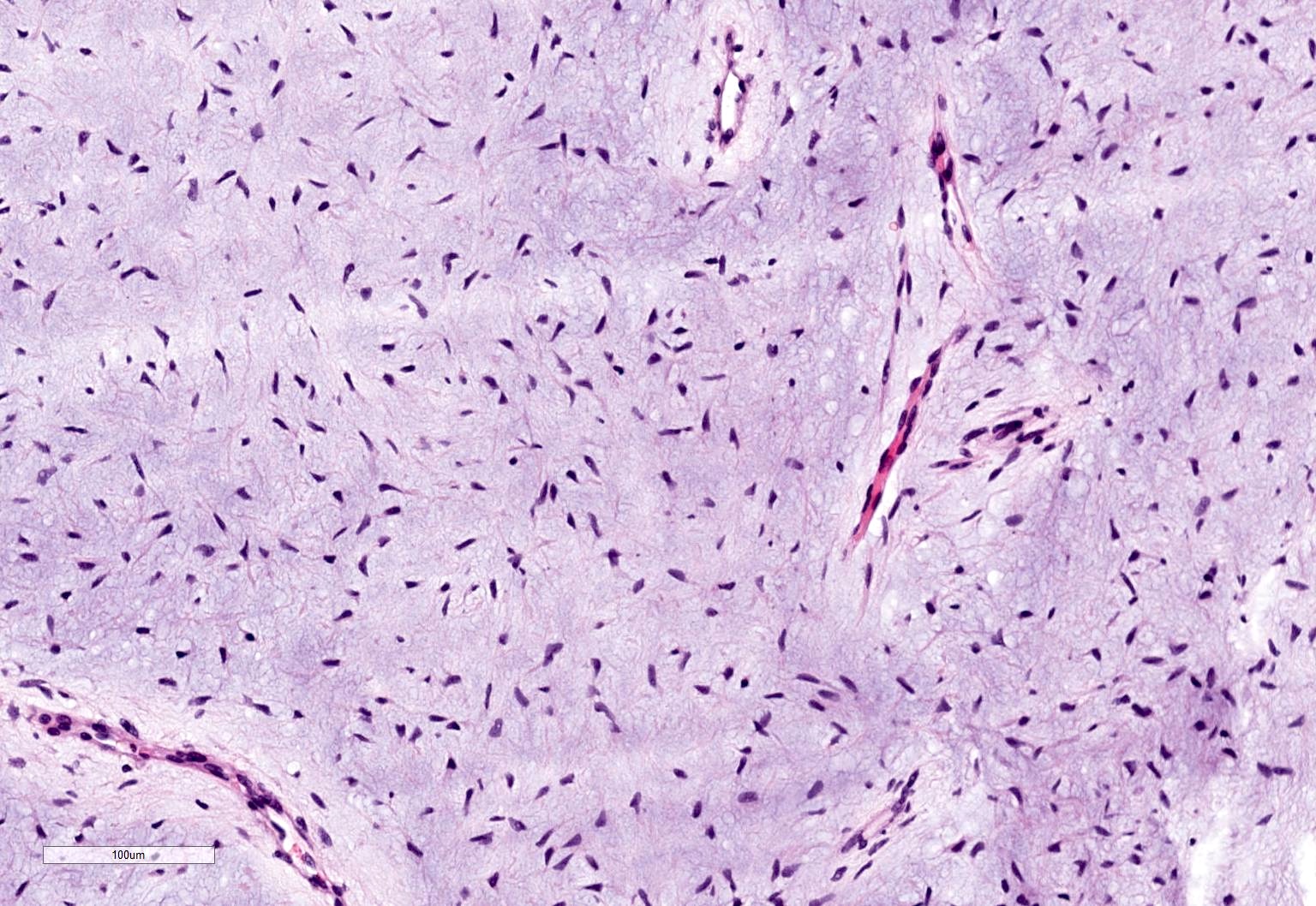
Bland spindle cells in myxoid stroma
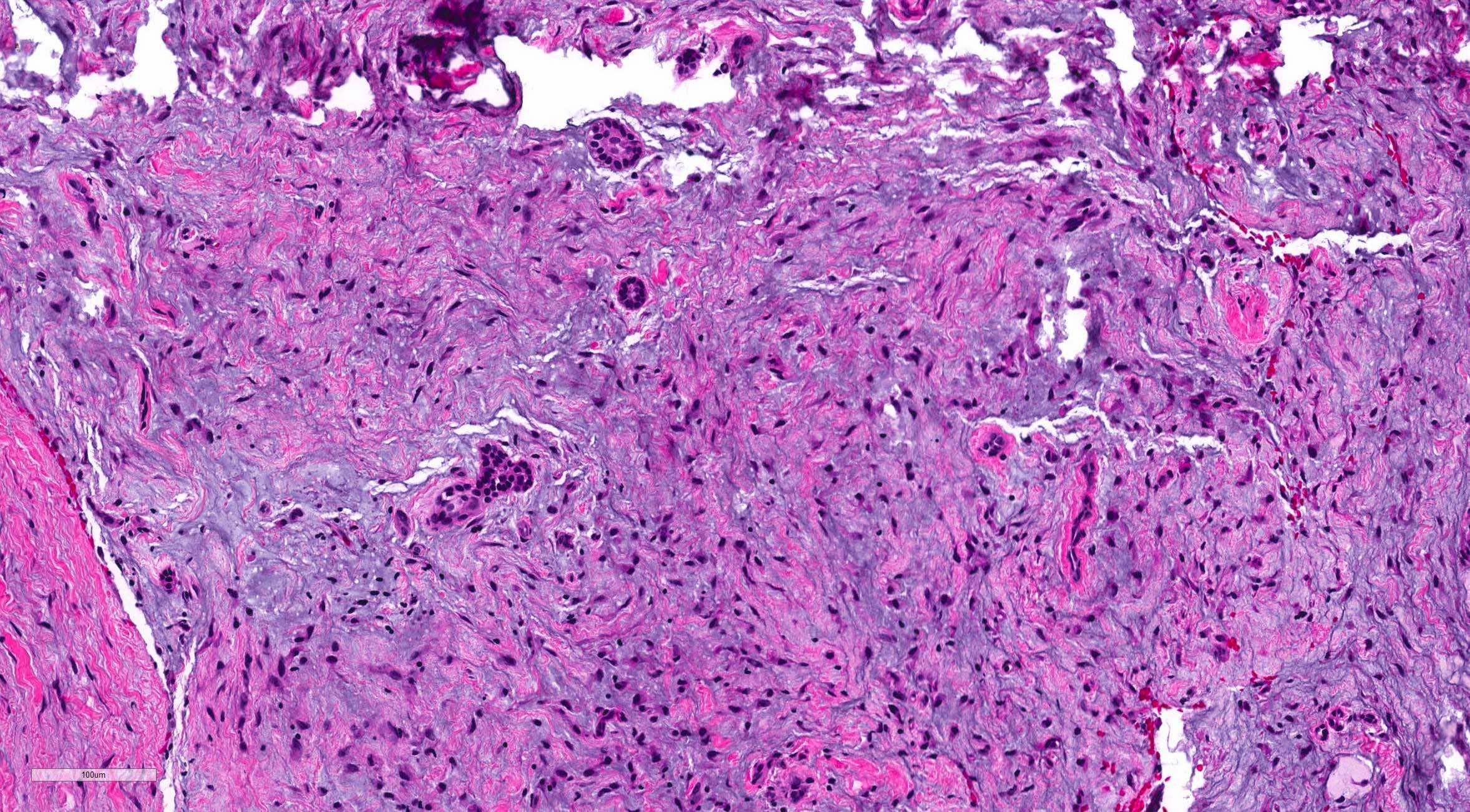
Inactive odontogenic rests
Maxilla neoplasm
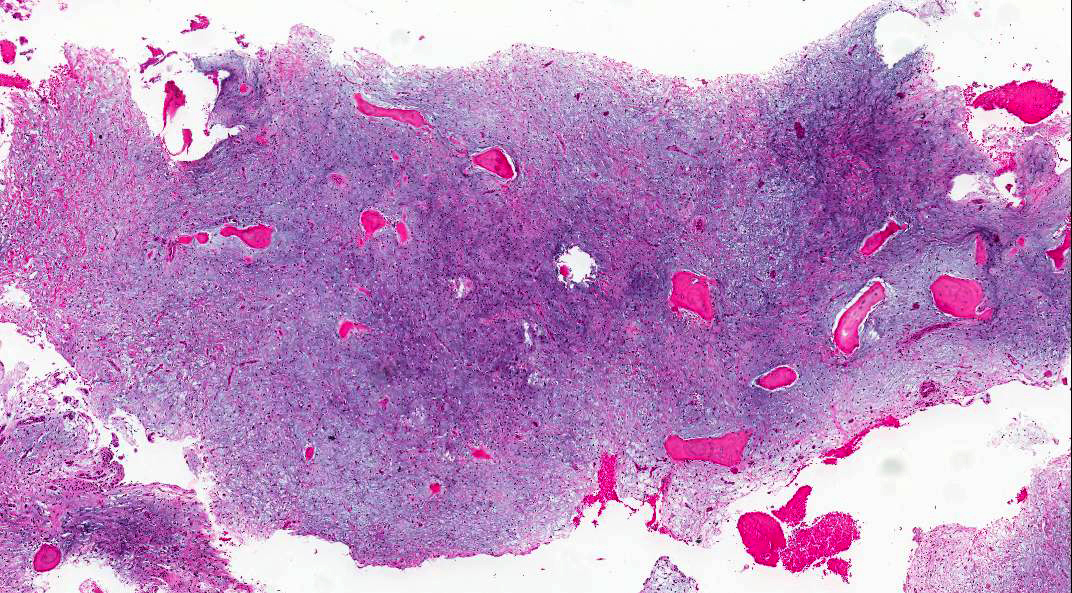
Mandibular lesion
Mandibular lesion
Virtual slides
Images hosted on other servers:

Odontogenic myxoma in mandible
Positive stains
- SMA
- β catenin: nuclear positive staining is rarely reported (Am J Surg Pathol 2023;47:1301)
Negative stains
Molecular / cytogenetics description
- MAPK / ERK pathway activation (Oral Oncol 2011;47:325)
Sample pathology report
- Mandible, segmental resection:
- Odontogenic myxoma
- Margins of excision negative
Differential diagnosis
- Dental papilla or dental follicle:
- Immature dental pulp or follicle from a developing tooth
- Often requires clinical and radiographic correlation to differentiate from myxoma
- Dental papillae may show a rim of odontoblasts
- Myxoid neurofibroma:
- S100 positive
- Chondromyxoid fibroma:
- Presence of chondroid / mature cartilaginous component
- Odontogenic fibroma:
- More cellular and fibrocollagenous
- Strands or islands of odontogenic epithelium more prominent
- Infantile sinonasal myxoma (Am J Surg Pathol 2023;47:1301):
- Short, intersecting fascicles of bland, stellate to spindle cells
- Prominent stromal vessels and variably myxoid to collagenous stroma
- Neoplastic cells exhibited bipolar to stellate, fibroblastic cytomorphology, with pale pink cytoplasm, vesicular nuclei and small, distinct nucleoli
- Pushing border rather than infiltrative growth
- No dystrophic calcifications
- No rests of odontogenic epithelium
- Mitotic index low (median < 1 per 10 HPF)
- Strong and diffuse nuclear β catenin in majority of cases, rare SMA positive
- Negative for S100 protein, CD34 and desmin
- Molecular level: most tumors harbor CTNNB1 mutations (D32Y, G34E, G34R and I35S) on exon 3 or APC alterations consistent with biallelic inactivation
- Combination of patient age, tumor site and strong and diffuse nuclear β catenin expression generally distinguished infantile sinonasal myxomas from odontogenic myxoma
Board review style question #1
The tumor shown above is found in the posterior mandible. What is the best diagnosis?
- Chondromyxoid fibroma
- Intraosseous mucoepidermoid carcinoma
- Odontogenic keratocyst
- Odontogenic myxoma
Board review style answer #1
D. Odontogenic myxoma. The image shows scant spindle cells in a myxoid background consistent with odontogenic myxoma. Answer B is incorrect because intraosseous mucoepidermoid carcinoma would have an epidermoid component and lack spindle cells. Answer A is incorrect because chondromyxoid fibroma contains cartilage (not seen in the image). Answer C is incorrect because odontogenic keratocyst is lined by a squamous type epithelium and lacks significant myxoid change.
Comment Here
Reference: Odontogenic myxoma / fibromyxoma
Comment Here
Reference: Odontogenic myxoma / fibromyxoma
Board review style question #2
Odontogenic myxomas have been shown to have which of the following molecular alterations?
- BRAF mutations
- GNAS mutations
- KRAS mutations
- MAPK / ERK pathway activation
Board review style answer #2
D. MAPK / ERK pathway activation. Odontogenic myxomas have been shown to have activation of the MAPK / ERK pathway. Answer A is incorrect because BRAF mutations can be seen in ameloblastomas. Answer B is incorrect because GNAS mutations are seen in fibrous dysplasia. Answer C is incorrect because KRAS mutations can be seen in adenomatoid odontogenic tumors.
Comment Here
Reference: Odontogenic myxoma / fibromyxoma
Comment Here
Reference: Odontogenic myxoma / fibromyxoma

