
Mandible & maxilla
Cysts of the jaw
Glandular odontogenic cyst
Copyright: 2004-2024, PathologyOutlines.com, Inc.
PubMed Search: Glandular odontogenic cyst [title]


- Locally aggressive developmental cyst occurring within the jaws, recognized by WHO in 1992 as odontogenic in origin
- Noteworthy for locally aggressive growth, potential for recurrence and differential diagnostic considerations
- While generally accepted as odontogenic in origin, lesion demonstrates glandular features including presence of cuboidal / columnar cells, mucin production, and cilia
- Highlights pluripotentiality of odontogenic epithelium
- Glandular odontogenic cyst (GOC), accepted by WHO 1992
- Sialo-odontogenic cyst
- Polymorphous Odontogenic Cyst
- Mucoepidermoid Odontogenic Cyst
- Rare lesion, 0.2% of all odontogenic cysts
- Average age at diagnosis is 51 years
- Peak occurrence in 5th to 7th decades
- No gender predilection
- Distinct peak frequency in sixth decade, particularly in men
- Mandible is most common location, 80%
- 55% occur in anterior mandible
- Maxilla affected in 20% cases
- 88% in anterior maxilla, usually canine area
- Probable origin is rests of dental lamina
- Can present with painful swelling (most common symptom is swelling) or paresthesia
- Diagnosis made by correlating microscopic findings, location of cyst and jaw imaging studies
- Variable: unilocular or multilocular radiolucent lesions with well defined borders on plain radiography
- Scalloped borders possible, sclerotic borders less common
- Tooth displacement 50%, tooth root resorption 30%, association with unerupted tooth or teeth 11%
- Can mimic other 'classic' developmental jaw cysts
- Dentigerous cyst: radiolucent lesion associated with unerupted tooth
- Lateral periodontal cyst: radiolucent lesion located between roots of mandibular premolar-canine area
- So called "globulomaxillary" position: inverted pear shaped or inverted tear drop shaped radiolucent lesion in maxilla located between roots of canine-premolar area
Images hosted on other servers:

Large osteolytic lesion/s

Well defined unilocular radiolucent lesion

Well defined unilocular lesion

Multilocular radiolucency in anterior mandible

Large well defined radiolucency

Oval radiolucency in anterior maxilla

Well defined radiolucency

Large multilocular radiolucency

Complex lytic lesion of the anterior mandible

Destructive
multilocular
lesion of the
anterior mandible
- In some series, 20 - 50% recurrence rate
- Multiple recurrences possible
- Time to recurrence variable: may depend on initial size of lesion, method of treatment, method of postoperative surveillance (plain radiography vs cross sectional imaging)
- Interval in literature ranges 2 to 13 years
- Range of interventions described: enucleation, curettage, +/- peripheral ostectomy, marsupialization segmental mandibulectomy, marginal mandibulectomy
- More aggressive initial surgery may reduce rate of recurrence, although no definitive studies
- Treatment influenced by size of lesion, involvement of teeth, bone compromise present, cortical bone perforation, history of recurrence, proximity to vital anatomic structures, patient desires and other patient related variables
Images hosted on other servers:

Swelling over left middle third of face

Intraoral swelling over left maxilla

Well defined swelling on right side of face

Lesion still attached to floor of maxillary sinus

Fluctuant swelling extending from 19 to 29 regions
Images hosted on other servers:

Excised lesion showing the cystic lining
- Nonkeratinized or slightly basaloid epithelial cyst lining which may exhibit a number of microscopic parameters
- The combination of specific microscopic parameters is important in making an accurate diagnosis
- Presence of 7 or more microscopic parameters predictive of diagnosis; see Table 1 - Head Neck Pathol 2011;5:364
- Most helpful microscopic parameters: Table 2 - Head Neck Pathol 2011;5:364
- Intraepithelial microcysts, crypts or duct-like spaces:
- Most commonly lined by a single layer of cuboidal to columnar cells similar to surface cells, less commonly lined by mucous goblet cells
- Microcysts:
- May contain mucous pools, eosinophilic material, or appear empty
- May open onto surface of lining epithelium
- May give glandular or pseudoglandular structure appearance
- Epithelial spheres or plaque-like thickenings:
- Epithelium in these plaques exhibits swirling or spherule formation
- May protrude into cyst lumen or extend into underlying connective tissue wall
- Identical to structures present in lateral periodontal cysts or botryoid odontogenic cysts or soft tissue odontogenic cyst, gingival cyst of adult
- Multiple cyst compartments:
- Multiple cystic spaces similar to those seen in botryoid odontogenic cysts
- Variable thickness of the cyst lining
- Papillary projections or "tufting" of epithelium into cyst lumen:
- Papillary projections may be formed by several microcysts opening onto luminal surface of the cyst lining or be formed independent of microcysts
- Clear or vacuolated cells:
- Cells with clear cytoplasm which may be present in basal or parabasal layers
- In areas of attenuated cyst lining, clear basal cells may be directly subjacent to the surface eosinophilic cuboidal cells
- Surface eosinophilic cuboidal cells (hobnail cells):
- Present on luminal surface of cyst lining; resemble cuboidal cells of the reduced enamel epithelium that lines dental follicles and dentigerous cysts
- May demonstrate cilia
- Not specific for GOC diagnosis
- Apocrine snouting of hobnail cells:
- Hobnail cells may demonstrate "pinching off" of surface similar to decapitation secretion seen in cells that line apocrine gland ducts
- Mucous goblet cells:
- Present individually or in small clusters on cyst lumen surface or within cyst lining
- May also line microcysts
- Not specific for GOC diagnosis
- Ciliated cells:
- True cilia may be present on surface of eosinophilic cuboidal cells
- Are distinct from apocrine snouting
- Solid islands of odontogenic epithelium in connective tissue wall:
- May have microcyst formation present
- Intraepithelial microcysts, crypts or duct-like spaces:
Contributed by Kelly Magliocca, D.D.S., M.P.H.
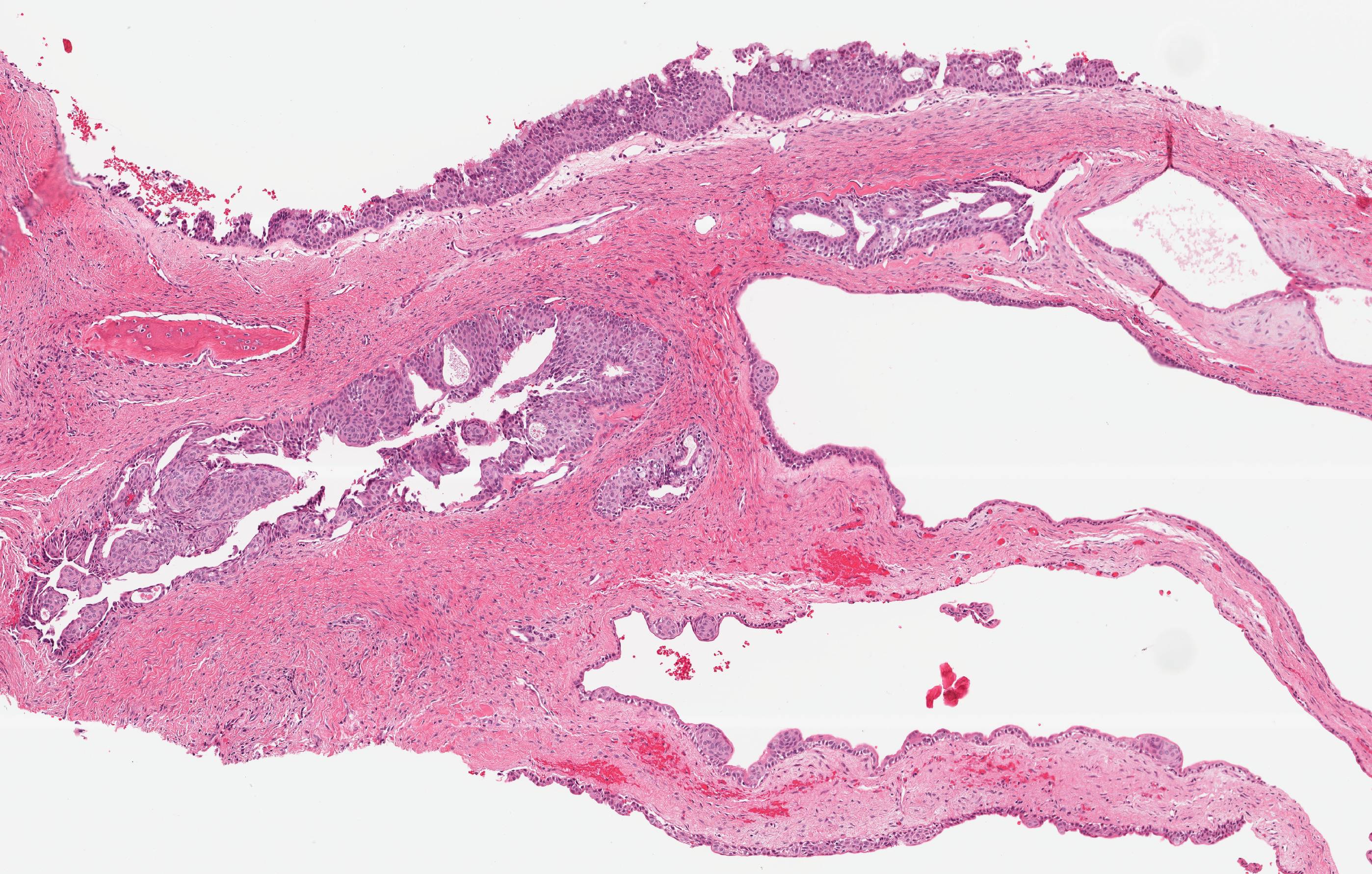
Glandular odontogenic cyst
Images hosted on other servers:

Complex cyst lining

Cystic lining with connective tissue stroma

Pseudostratified squamous epithelium

Islands of epithelium

Mucous cells, epidermoid cells, and clear cells

Glandular cystic lining

Mucicarmine positive mucus cells


Mucus cells (mucicarmine positive)

Parakeratinized squamous epithelial lining

Eosinophilic cuboidal cells

Vacuolated area in lining of a dentigerous cyst

Mucoepidermoid carcinoma-like islands in cyst wall
- Helpful to consider microscopic parameters in combination with radiographic and clinical / historical data:
- Associated with unerupted tooth / teeth, no prior history of cyst removed from same area, no prior history of major oral surgery in same anatomic area:
- Associated with the root of erupted tooth / teeth, no prior history of odontogenic cyst removed from same area:
- Radicular cysts: can have mucous cell metaplasia
- Odontogenic keratocyst/KOT
- Central mucoepidermoid carcinoma
- Botryoid cyst/lateral periodontal cyst
- Surgical ciliated cyst
- Edentulous area or associated with the root of erupted tooth / teeth, positive history of odontogenic cyst removed from same area:
- Odontogenic keratocyst/KOT
- Central mucoepidermoid carcinoma
- Botryoid cyst
- Recurrent glandular odontogenic cyst
