
Mandible & maxilla
Giant cell lesions & nonepithelial bone cysts
Central giant cell granuloma
Editorial Board Member: Marc Pusztaszeri, M.D.
Deputy Editor-in-Chief: Kelly Magliocca, D.D.S., M.P.H.


Last author update: 19 March 2024
Last staff update: 26 March 2024
Copyright: 2004-2024, PathologyOutlines.com, Inc.
PubMed Search: Central giant cell granuloma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Haidari M, Abdul-Ghafar J, Ud Din N. Central giant cell granuloma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/mandiblemaxillacentralgiantcellgranuloma.html. Accessed April 20th, 2024.
Definition / general
- Benign, nonodontogenic lesion of the jaw, osteoclastic in origin, with unknown etiology (StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024], Indian J Otolaryngol Head Neck Surg 2013;65:192)
- Can be locally aggressive and destructive (StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024])
Essential features
- Sharply demarcated radiolucency with sclerotic margins, sometimes extends between the displaced tooth roots
- 80% of cases involve the region anterior to the first premolar
- Localized and lobulated but sometimes lytic and aggressive
- Vascular connective tissue is observed, with a patchy distribution of multinucleated giant cells in the surrounding stroma
Terminology
- Giant cell granuloma, central (CGCG)
- Not recommended: reparative giant cell granuloma, central giant cell lesion
ICD coding
Epidemiology
- Population incidence is thought to be 0.0001% (StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024])
- Peak age is between 5 and 15 years; rarely develops after 30 years old (J Oral Maxillofac Pathol 2020;24:413, StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024])
- Most common in female patients (2:1) (J Oral Maxillofac Pathol 2020;24:413)
- Both jaw bones can be affected; 80% of cases involve the region anterior to the first premolar (J Oral Maxillofac Pathol 2020;24:413)
- Multiple cases revealed association with the RAS / MAPK pathway (J Oral Maxillofac Pathol 2020;24:413)
Sites
- Comprises close to 7% of all intraosseous lesions in the jaw (J Clin Med 2022;11:4239)
- Both jaws are affected (J Oral Maxillofac Pathol 2020;24:413)
- 80% of cases involve the region anterior to the first premolar (J Oral Maxillofac Pathol 2020;24:413)
- Mandible involvement is 2x more common than maxilla (Imaging Sci Dent 2022;52:123)
Pathophysiology
- Altered bone microenvironment can be a possible reason for deregulation of the cell cycle (J Oral Maxillofac Pathol 2020;24:413, StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024])
- CGCG arises from osteoclast precursors in the mononuclear stroma, induced by RANKL, VEGF and b-FGF; the last amplifies the resorptive action of parathyroid hormone
- Sporadic CGCG has low tumor mutation burden, lacks fusions and is driven by mutually exclusive somatic mutations in KRAS (more often affecting codon 12), FGFR1 (either p.C381R or p.N330I) and TRPV4 (p.M713V/I) that occur in 70% of cases, leading to MAPK pathway activation (Nat Commun 2018;9:4572)
- TRPV4 codes a polymodal Ca2+ permeable channel and is mutated in hereditary channelopathies characterized by peripheral nervous system and skeletal changes
- Recently, CGCG has been described as one feature of a polysystemic syndrome due to germline TRPV4 mutation, expanding the spectrum of TRPV4 channelopathies (J Med Genet 2022;59:305)
Etiology
- Precise predisposing factor is yet unidentified (J Oral Maxillofac Pathol 2020;24:413)
- Altered bone microenvironment can be a possible cause (J Oral Maxillofac Pathol 2020;24:413)
Clinical features
- In general, CGCG is asymptomatic (painless swelling) in the beginning but later becomes expansile (J Oral Maxillofac Pathol 2020;24:413)
- When aggressive, it causes a rapidly enlarging painful swelling, displacing teeth, resorbing roots and the cortical plate of the alveolar ridge (StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024])
- Intraorally, a blue-brown discoloration may be seen due to thinning of the cortical plate and overlying mucosa (StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024])
- Clinical expansion occurs over a period of weeks to a couple of months (StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024])
Diagnosis
- Diagnosis of central giant cell granuloma is normally made histologically from an incisional / excisional biopsy (Ann Maxillofac Surg 2012;2:102)
- Combination of clinical, radiological and histopathological evaluations is recommended for definite diagnosis and confirmation (Ann Maxillofac Surg 2012;2:102)
- Radiologic findings alone are not sufficient for diagnosis (Ann Maxillofac Surg 2012;2:102)
Laboratory
- No specific laboratory test is available
Radiology description
- Sharply demarcated radiolucency sometimes extends between the displaced tooth roots (J Oral Maxillofac Pathol 2020;24:413)
- Sclerotic margin denoting the slow expansile nature (J Oral Maxillofac Pathol 2020;24:413)
- Faint calcifications are noticed, depicting the poorly mineralized osteoid trabeculae within the lesion, which helps to differentiate from giant cell tumors (J Oral Maxillofac Pathol 2020;24:413)
- Larger lesions may exhibit multilocularity (J Oral Maxillofac Pathol 2020;24:413)
- Cortex generally is intact but in more aggressive lesions, it may be breached (J Oral Maxillofac Pathol 2020;24:413)
Radiology images
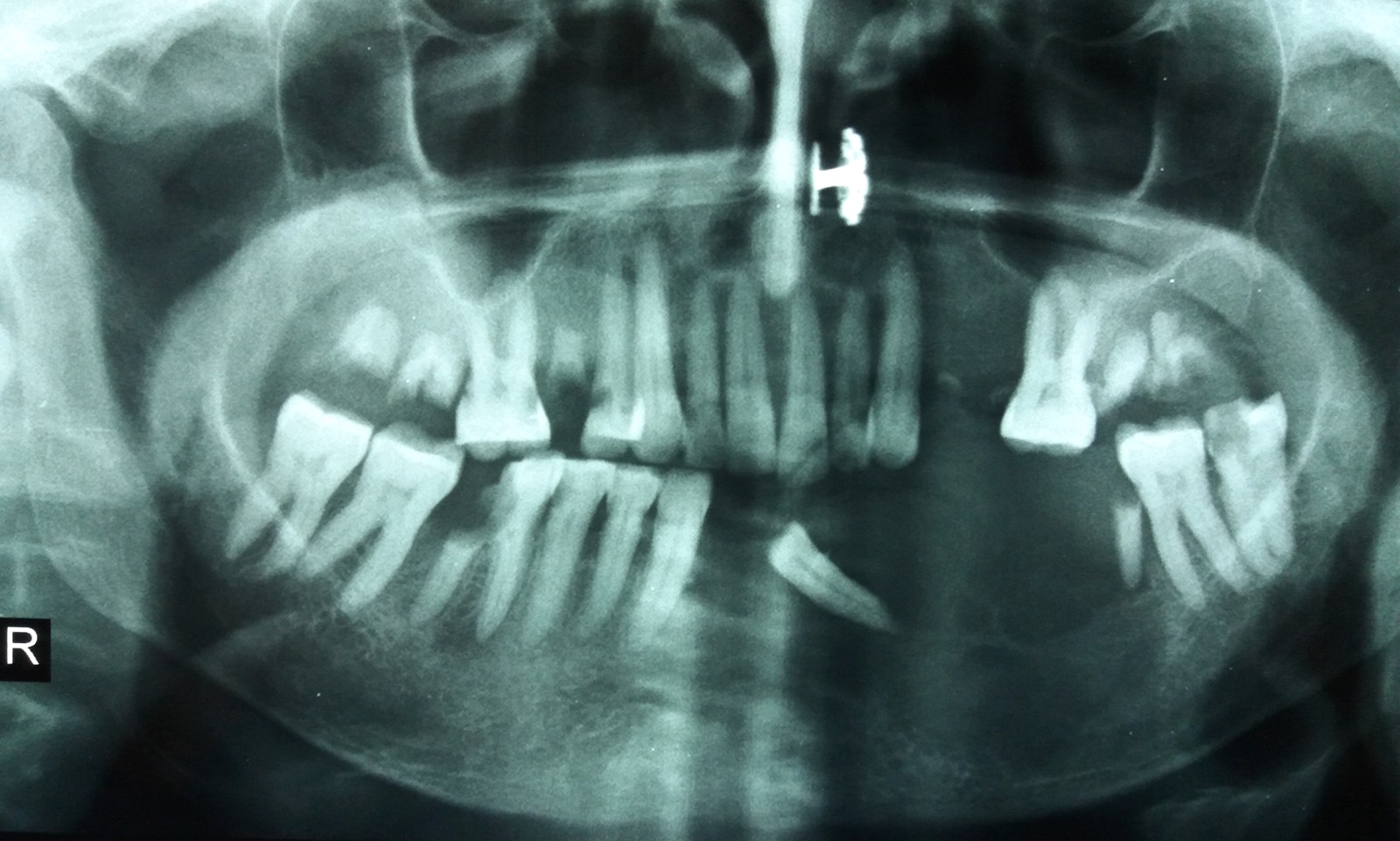
Contributed by Nasir Ud Din, M.B.B.S.
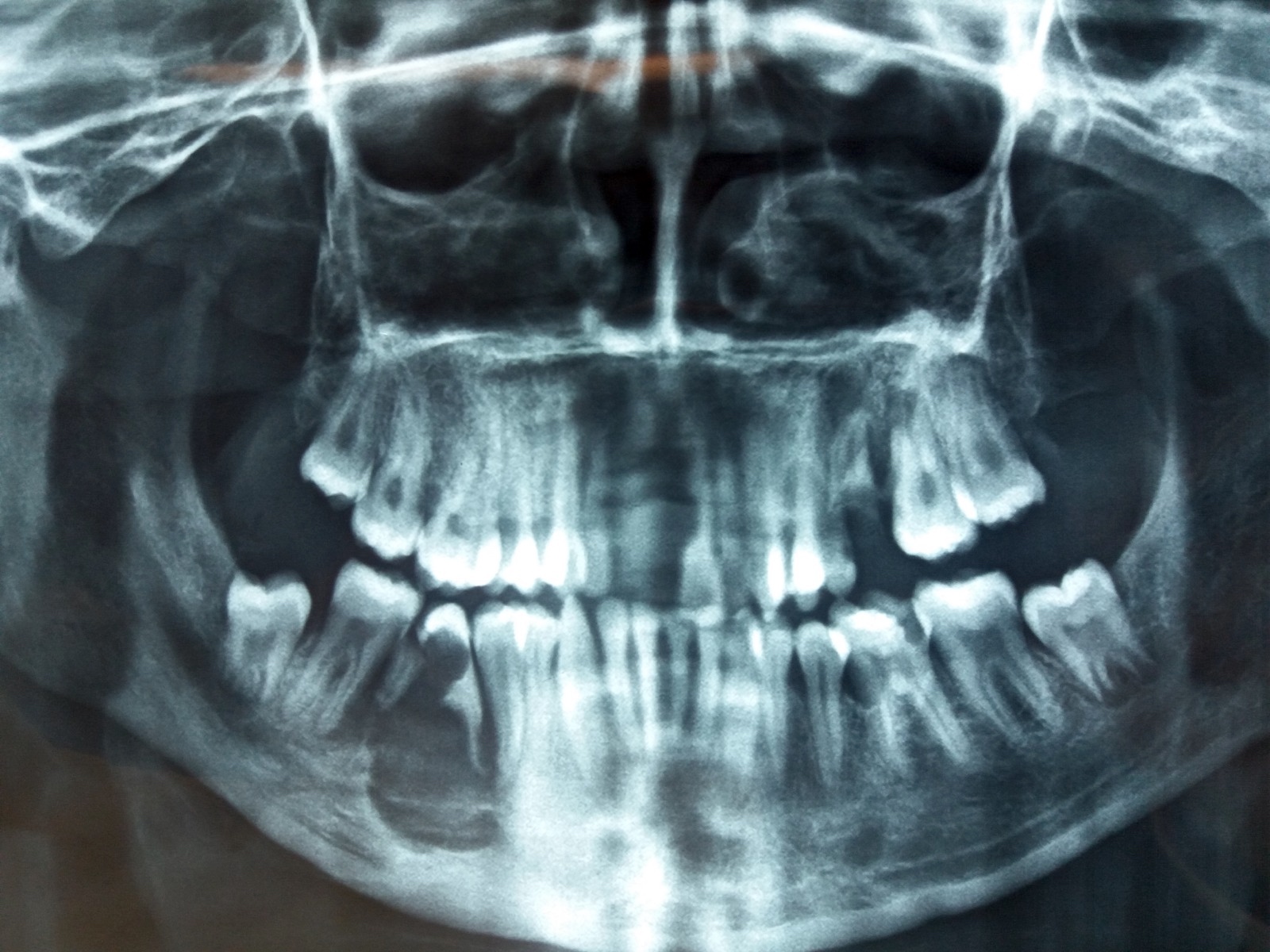
CGCG of
mandible,
premolar region
(orthopantomogram)

Mandibular body
CGCG
(orthopantomogram)
Left mandibular CGCG
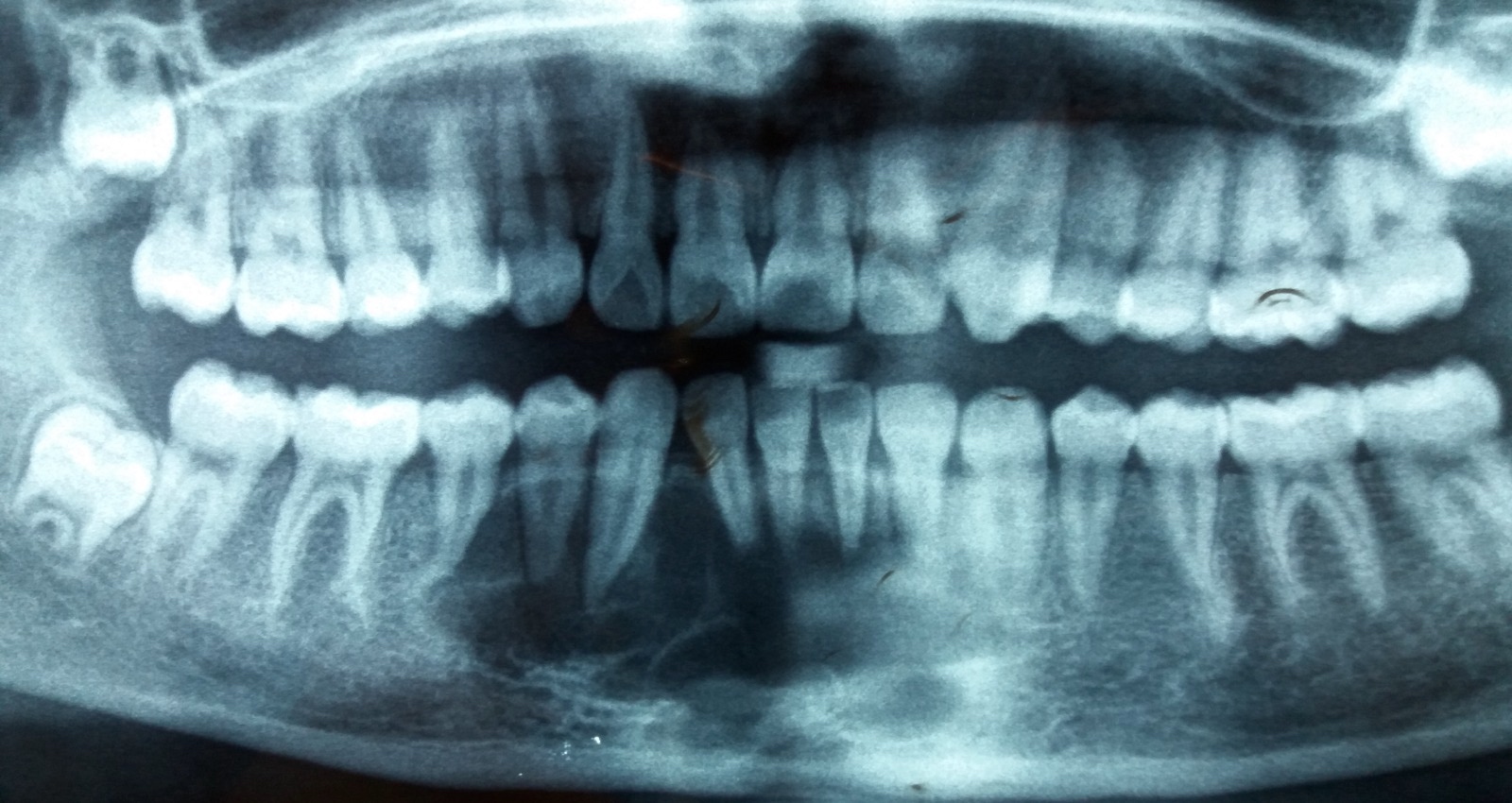
CGCG of lower incisor region
Prognostic factors
- Central giant cell granuloma can have aggressive, locally destructive behavior or may be indolent and respond to nonsurgical therapies (StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024])
- Recurrence rate is near 15 - 20% and is higher in aggressive forms, particularly if incompletely removed (40 - 70%) (Ann Maxillofac Surg 2012;2:102)
- Recurrence normally occurs within the first 12 - 18 months (StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024])
Case reports
- 9 year old girl with hybrid CGCG within ossifying fibroma (F1000Res 2019;8:1218)
- 11 year old girl with CGCG of mandibular condyle (J Clin Med 2022;11:4239)
- 17 year old girl with coexistent CGCG and aneurysmal bone cyst (ABC) (Iran J Otorhinolaryngol 2021;33:319)
- 33 year old woman with CGCG at posterior portion of mandible (Int J Surg Case Rep 2023;112:108971)
Treatment
- Can be treated via surgical and nonsurgical means (Ann Maxillofac Surg 2012;2:102)
- Surgery varies depending on the location, size and aggressiveness of the lesion and can range from curettage to large scale resection and reconstruction (StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024])
- Nonsurgical treatment is often considered for smaller, less aggressive lesions; however, some have suggested its use as neoadjuvant therapy for large lesions (StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024])
- Intralesional steroids, daily subcutaneous calcitonin and interferon alpha for its antiangiogenic effects have all been used with some success (StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024])
Clinical images
Images hosted on other servers:

Right side submandibular swelling

Oval lesion involving left side mandible
Gross description
- Fleshy, reddish brown, hemorrhagic appearance
Gross images
Images hosted on other servers:

Fleshy, reddish brown, hemorrhagic appearance
Microscopic (histologic) description
- Unencapsulated, localized, lobulated and can have osteolytic proliferations (StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024])
- Primary cells of the CGCG are fibroblasts and secondary cells are multinucleated giant cells; accessory cells are macrophages, dendrocytes and endothelial cells (J Oral Maxillofac Pathol 2020;24:413)
- Vascular connective tissue is observed, with a patchy distribution of multinucleated giant cells in the surrounding stroma (StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024])
- Multinucleated giant cells are unevenly distributed and form clearly recognizable clusters separated by scar-like stromal tissue (J Oral Maxillofac Pathol 2020;24:413)
- Clustering is particularly evident in areas of hemorrhage (J Oral Maxillofac Pathol 2020;24:413)
- Extravasated erythrocytes and hemosiderin deposits are frequently seen, highlighting multifocal hemorrhage (StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024])
- More aggressive versions have been shown to have more numerous, larger giant cells with a greater surface area density (StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024])
Microscopic (histologic) images
Contributed by Nasir Ud Din, M.B.B.S.
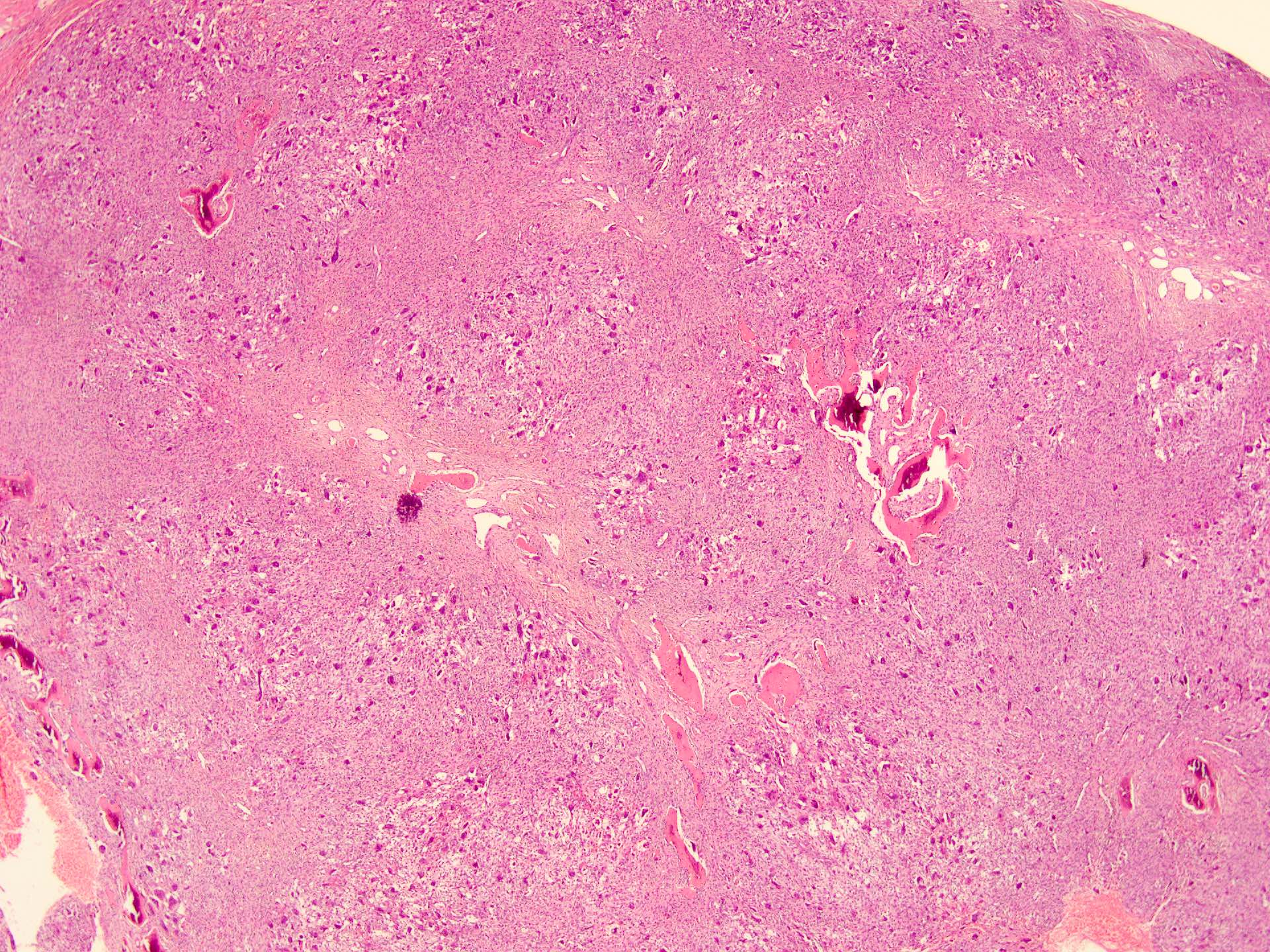
Lobulated architecture
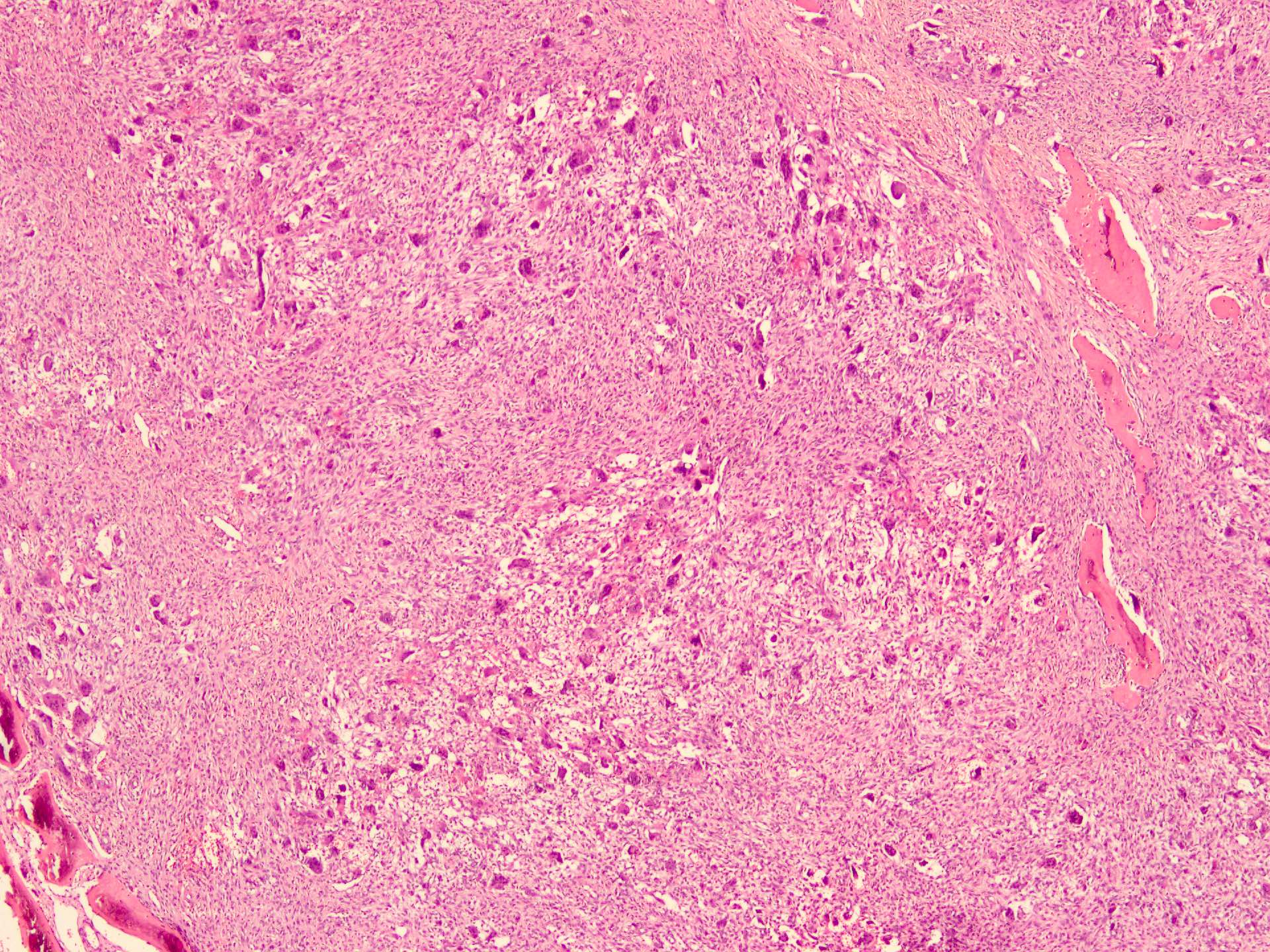
Lobulation
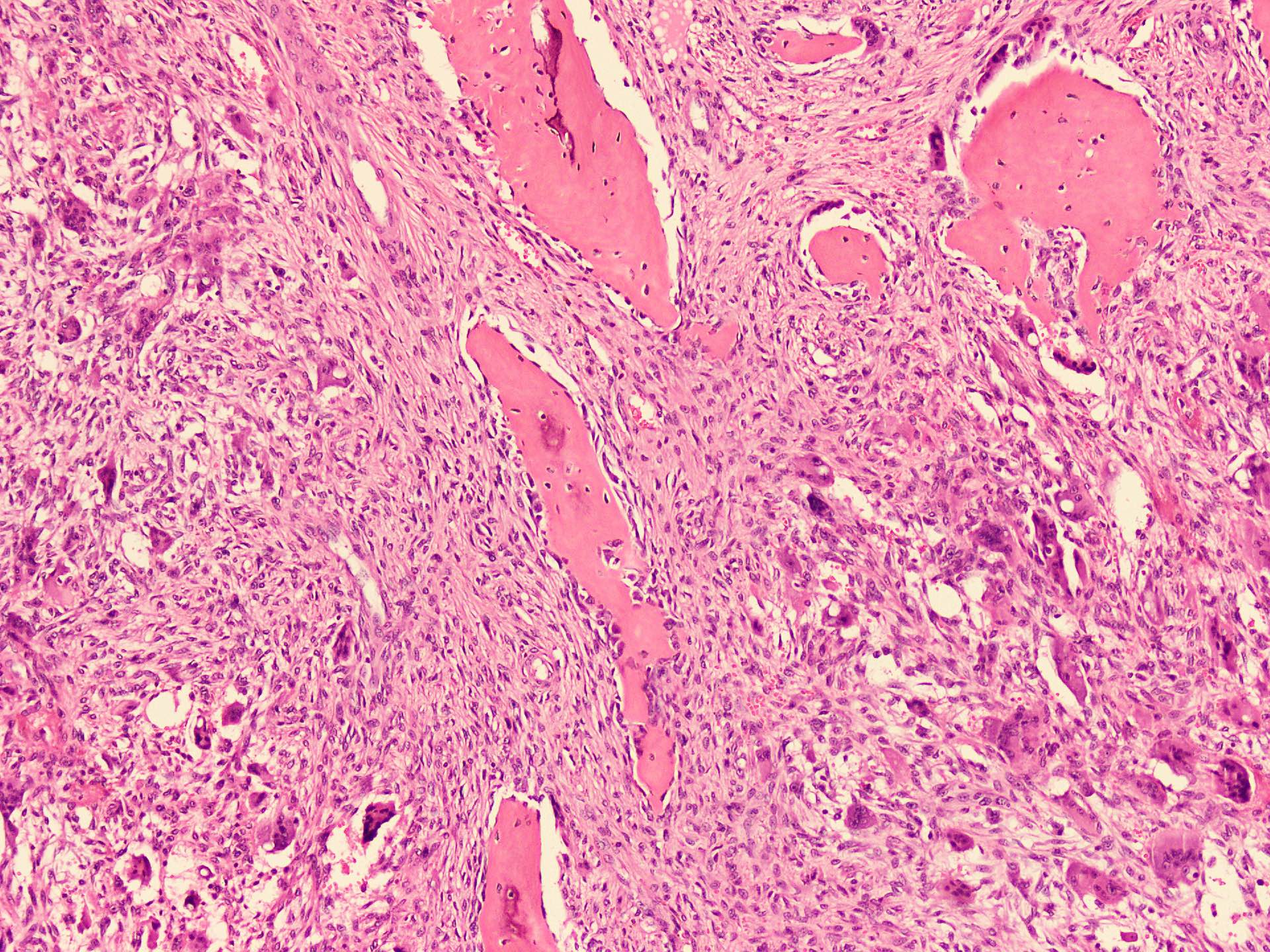
Periphery of lobule
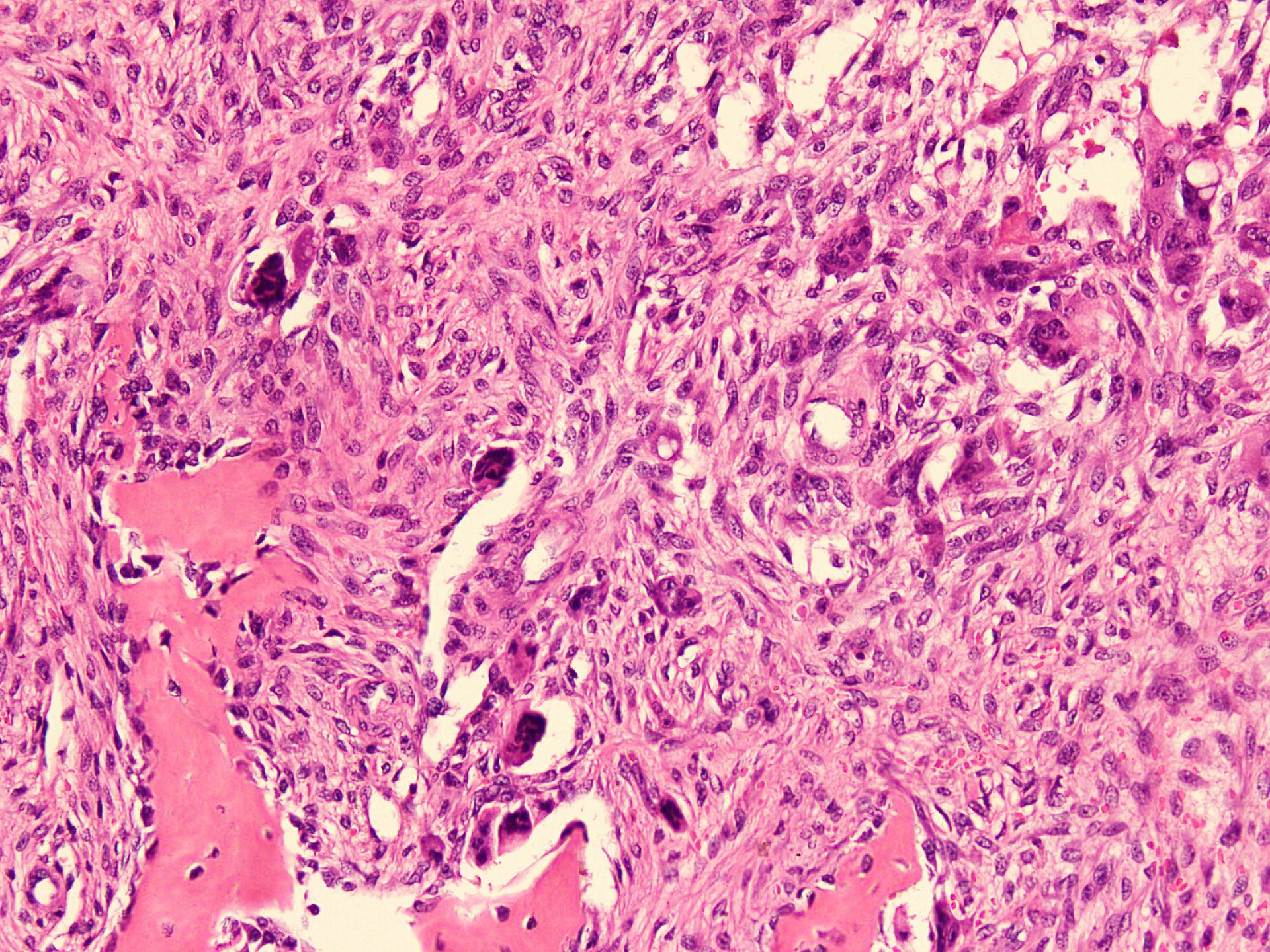
Woven bone
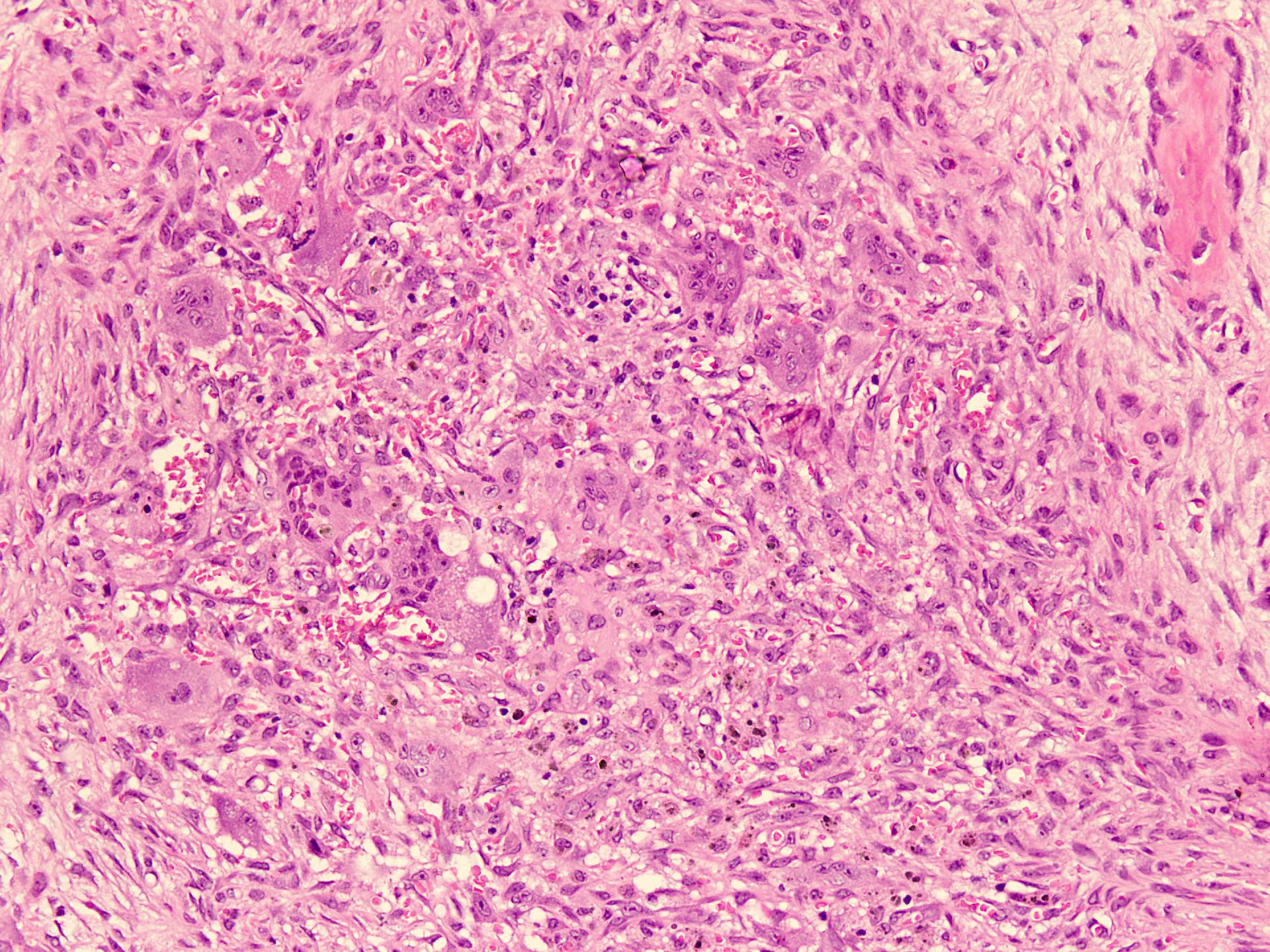
Lobule center
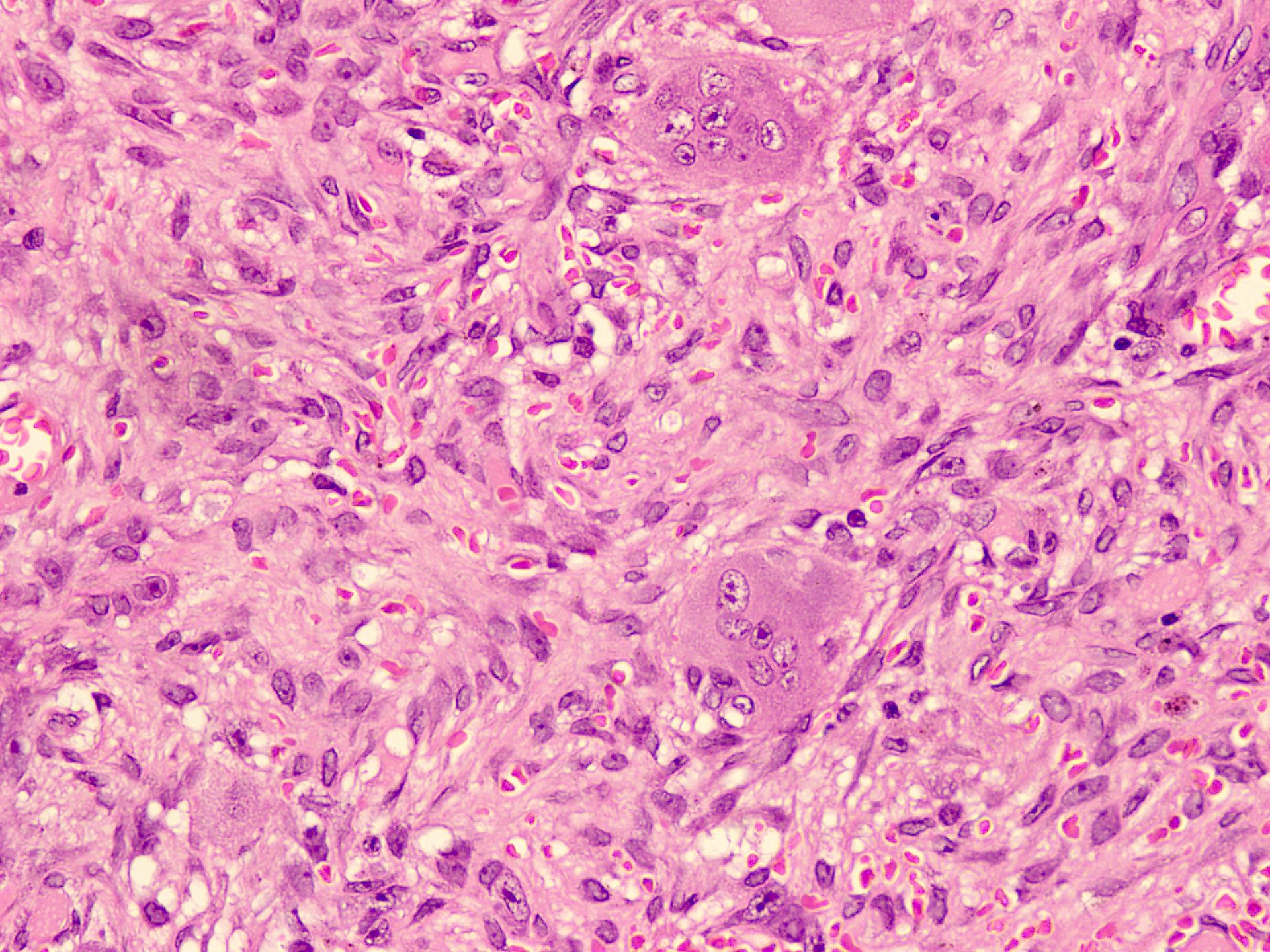
Fibroblast and giant cells
Virtual slides
Images hosted on other servers:

Central giant cell granuloma
Cytology description
- Cohesive monolayered clusters of round to oval mononuclear cells with dispersed single cells and randomly distributed multinucleated giant cells in the background (Acta Cytol 1994;38:475)
- Round to ovoid nuclei with fine chromatin and inconspicuous nucleoli (Acta Cytol 1994;38:475)
- Hemosiderin laden macrophages and inflammatory cells can also be present (Acta Cytol 1994;38:475)
- Absence of mitotic figures and cellular pleomorphism (Acta Cytol 1994;38:475)
Cytology images
Images hosted on other servers:

Giant cell with occasional
spindle cells and
hemorrhagic background
Positive stains
Molecular / cytogenetics description
- KRAS, TRPV4 and FGFRI can be seen in CGCG, which is histologically similar to nonossifying fibroma of long bones (J Oral Maxillofac Pathol 2020;24:413)
- Multiple giant cell lesions occur in syndromes, including neurofibromatosis type 1, osteoglophonic dysplasia, Noonan, cardiofaciocutaneous, oculoectodermal, LEOPARD, Schimmelpenning-Feuerstein-Mims and Jaffe-Campanacci, most of which are caused by MAPK pathway gene mutations (J Pathol 2020;250:126)
Videos
Central giant cell granuloma
Sample pathology report
- Mandible, anterior portion lytic lesion, excisional biopsy:
- Features suggest central giant cell granuloma (CGCG) (see comment)
- Comment: Histologically an unencapsulated spindle cell lesion with unevenly distributed clusters of osteoclast type giant cells in a hemorrhagic background along with bland fibroblasts and peripheral woven bone formation. Immunohistochemically the multinucleated giant cells are positive for CD68 and negative for H3 G34W. This constellation of morphological and immunohistochemical features strongly supports the diagnosis of central giant cell granuloma.
- Serological correlation is recommended to rule out the possibility of Brown tumor.
Differential diagnosis
- Brown tumor of hyperparathyroidism:
- Histologically indistinguishable but usually present in multiple bones and with deranged bone profile results (StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024])
- Hyperparathyroidism can be differentiated on the basis of biochemical tests, where hypercalcemia, hypophosphatasia and increased parathyroid hormone (PTH) will point toward hyperparathyroidism (J Oral Maxillofac Pathol 2020;24:413)
- Bone tunneling is a useful clue for Brown tumor
- Peripheral giant cell granuloma:
- Reactive condition involves gingiva as a nodular mass while CGCG involves bones (Indian J Med Paediatr Oncol 2017;38:440)
- More common in the fifth and sixth decades (J Oral Maxillofac Res 2019;10:e5)
- Rarely bone or osteoid formation is seen (J Oral Maxillofac Res 2019;10:e5)
- Giant cell tumor:
- Difficult to differentiate, especially when the CGCG is of the aggressive type (J Oral Maxillofac Pathol 2020;24:413)
- Giant cell tumors have larger giant cells, greater numbers of nuclei and generalized distribution of giant cells and absence of osteoid formation (J Oral Maxillofac Pathol 2020;24:413)
- Practically, the occurrence of giant cell tumor in the jawbones is very rare and cases have been reported where patients are already suffering from Paget disease (J Oral Maxillofac Pathol 2020;24:413)
- Positive H3 G34W and p63 staining in mononuclear cells (Cancer Cytopathol 2018;126:552)
- Cherubism:
- Autosomal dominant disorder, most commonly caused by a mutation in SH3P2
- Widespread and multiple osteolytic lesions of primarily the posterior mandible (StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024])
- Onset is in childhood, producing a classical, symmetric full cheek appearance (StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024])
- Nonossifying fibroma:
- Fibrohistiocytic stroma with a storiform pattern and prominent xanthogranulomatous reaction (J Oral Maxillofac Pathol 2020;24:413)
- Maxillofacial involvement is very rare
- Aneurysmal bone cysts (ABC) (StatPearls: Non-Odontogenic Tumors of the Jaws [Accessed 28 February 2024]):
- ABCs show blood filled cystic spaces (J Pathol Transl Med 2023;57:81)
- Common in the metadiaphysis of long bones and vertebral bones (J Pathol Transl Med 2023;57:81)
- ABCs have a rearrangement of the USP6 gene (J Pathol Transl Med 2023;57:81)
Additional references
Board review style question #1
A 20 year old woman presents with a single large painless mass at the anterior portion of the mandibular bone. Excisional biopsy shows a fleshy hemorrhagic mass. Microscopically it shows a lesion composed of mononuclear spindle cells and clusters of osteoclast type multinucleated giant cells set in a vascular and hemorrhagic background. The multinucleated giant cells are positive for CD68. The mononuclear cells are negative for p63 and H3 G34W. No hypercalcemia or hypophosphatasia noted and parathyroid hormone (PTH) level is in normal range.
Which of the following is true regarding the above scenario?
- Features favor Brown tumor
- Findings are compatible with giant cell tumor of jaw
- Findings are in favor of central giant cell granuloma
- Findings are in favor of peripheral giant cell granuloma
- The neoplasm rarely involves the anterior portion of the mandible
Board review style answer #1
C. Findings are in favor of central giant cell granuloma. The histologic image reveals an unencapsulated spindle cell lesion with unevenly distributed clusters of osteoclast type giant cells in a hemorrhagic background along with bland fibroblasts and peripheral woven bone formation. Answer B is incorrect because p63 and H3 G34W are positive in giant cell tumor. Answer D is incorrect because the lesion is in between the bone. Answer A is incorrect because no hypercalcemia, hypophosphatasia or increased PTH were noted. Answer E is incorrect because CGCG mostly involves the anterior portion of the mandible.
Comment Here
Reference: Central giant cell granuloma
Comment Here
Reference: Central giant cell granuloma
Board review style question #2
Which of the following is true about central giant cell granuloma (CGCG)?
- Benign lesion that can be locally aggressive
- It is common in males and complete excision is the only treatment
- Multinucleated giant cells are evenly distributed in CGCG
- Primary cells of CGCG are giant cells
- Spindle cell component is positive for CD68
Board review style answer #2
A. Benign lesion that can be locally aggressive. Answer D is incorrect because primary cells of the CGCG are fibroblasts and secondary cells are multinucleated giant cells. Answer C is incorrect because in CGCG, one of the important histologic findings is the uneven distribution of multinucleated giant cells. Answer E is incorrect because the giant cells are positive for CD68, not the spindle cells, which are fibroblastic in nature. Answer B is incorrect because CGCG is more common in females and can have other treatment methods (nonsurgical treatment is often considered for smaller, less aggressive lesions; however, some have suggested its use as neoadjuvant therapy for large lesions).
Comment Here
Reference: Central giant cell granuloma
Comment Here
Reference: Central giant cell granuloma
