
Lymphoma & related disorders
Mature T/NK cell disorders
Anaplastic large cell lymphoma
Anaplastic large cell lymphoma, ALK negative
Deputy Editor-in-Chief: Genevieve M. Crane, M.D., Ph.D.

Last author update: 15 February 2021
Last staff update: 16 April 2024
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed search: Anaplastic large cell lymphoma ALK negative
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Cytology images | Positive stains | Negative stains | Flow cytometry description | Flow cytometry images | Molecular / cytogenetics description | Molecular / cytogenetics images | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Balakrishna J, Jaffe ES. Anaplastic large cell lymphoma, ALK negative. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lymphomanonBanaplasticneg.html. Accessed April 25th, 2024.
Definition / general
- A CD30 positive T cell neoplasm morphologically similar to ALK positive anaplastic large cell lymphoma (ALCL) but does not express ALK protein (Swerdlow: WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th Edition, 2017)
Essential features
- T cell lymphoma
- Characteristic hallmark cells
- Morphologically indistinguishable from ALCL, ALK positive
- CD30 diffusely and strongly positive
- ALK expression negative
- ALK gene rearrangement negative
Terminology
- ALK- ALCL
ICD coding
- ICD-10:
- C84 - mature T / NK cell lymphomas
- C84.7 - anaplastic large cell lymphoma, ALK negative
- C84.70 - unspecified site
- C84.71 - lymph nodes of head, face and neck
- C84.72 - intrathoracic lymph nodes
- C84.73 - intra-abdominal lymph nodes
- C84.74 - lymph nodes of axilla and upper limb
- C84.75 - lymph nodes of inguinal region and lower limb
- C84.76 - intrapelvic lymph nodes
- C84.77 - spleen
- C84.78 - lymph nodes of multiple sites
- C84.79 - extranodal and solid organ sites
Epidemiology
- Adults (40 - 65 years), in contrast to ALCL, ALK+, which is common in children and young adults
- Slight male predominance; M:F = 1.5:1
- Prevalence unknown (Orphanet: ALK Negative Anaplastic Large Cell Lymphoma [Accessed 9 April 2020])
Sites
- Both lymph nodes and extranodal sites, including bone, soft tissue and skin (primary cutaneous ALCL needs to be distinguished)
Pathophysiology
- Arises from activated T cells
- T cell associated antigens often downregulated, with loss of CD3 and other markers
- Gene expression shows common features between ALK+ and ALK- ALCL (Leukemia 2009;23:2129, Blood 2014;123:2915)
- Gains of the 1q41-qter and 6p21 are common cytogenetic aberrations (Br J Haematol 2008;140:516)
- DUSP22::IRF4 locus on 6p25.3 (referred to as DUSP22 rearrangements); t(6;7)(p25.3;q32.3) (Blood 2011;117:915)
- Recurrent rearrangement involving the TP63 gene (Blood 2012;120:2280)
- STAT3 activating mutations (Cancer Cell 2015;27:516)
Clinical features
- Mostly presents at advanced stage (stage III - IV) and B symptoms
Diagnosis
- Biopsy of the involved lymph node with immunohistochemistry
- Morphology (see Microscopic description)
- Immunophenotype (see Positive stains)
- Detection of genetic aberrations and T cell clone (see Molecular / cytogenetics description)
Laboratory
- Elevated lactate dehydrogenase, pancytopenia, anemia, thrombocytopenia (Blood 2008;111:5496)
Radiology description
- Enlarged lymph nodes / mass lesions in extranodal sites
Prognostic factors
- Outcome poorer than ALCL, ALK positive (Histopathology 2003;43:462, J Pathol 2003;200:4)
- Prognosis depends on patient age, international prognostic index score and genetic heterogeneity
- Recent studies indicate that DUSP22 rearrangements do not confer a better prognosis, in contrast to the initial study that showed a favorable prognosis (Haematologica 2023;108:1604, Br J Haematol 2019;186:e28)
- TP63 rearrangements poor survival rates (Blood 2014;124:1473)
- Loss of PRDM1 or TP53 poor outcome (Blood 2013;122:2683)
- Survival rates better than peripheral T cell lymphoma, not otherwise specified (Blood 2008;111:5496)
Case reports
- 13 year old girl with mediastinal ALK negative anaplastic large cell lymphoma (Oxf Med Case Reports 2019;2019:omz077)
- 21 year old man with a pulmonary abscess (Clin Nucl Med 2019;44:234)
- 53 year old man with AIDS with subcutaneous nodules on the scalp and axillae and diffuse lymphadenopathy (BMJ Case Rep 2019;12:e230641)
- 54 year old man misdiagnosed with Behçet disease (World J Clin Cases 2019;7:3377)
- 56 year old Asian man with right neck swelling for 3 months with fever and weight loss (Int J Surg Pathol 2017;25:502)
- 61 year old woman with endobronchial pseudocarcinomatous hyperplasia (Histopathology 2019 Nov 9 [Epub ahead of print])
- 69 year old woman with double hit of DUSP22 and TP63 rearrangements in anaplastic large cell lymphoma, ALK negative (Blood 2020;135:700)
- 69 year old woman presented with dyspnea and malaise (Case Rep Hematol 2018;2018:3465351)
- 73 year old man with recurrent thrombosis of his infrarenal aortic prosthesis (Virchows Arch 2019;474:763)
- 80 year old Japanese man with acute exacerbation of hypercalcemia (J Clin Exp Hematop 2019;59:22)
- 82 year old man with a history of cerebrovascular disease presented with weakness and iron deficiency anemia (In Vivo 2017;31:701)
- ALK negative anaplastic large cell lymphoma with Hodgkin-like cytomorphology and nuclear expression of PAX5 (Pathol Res Pract 2020;216:152724)
Treatment
- Chemotherapy with CHOP (cyclophosphamide, doxorubicin, vincristine and prednisone) or CHOP plus etoposide (CHOEP) (Curr Hematol Malig Rep 2018;13:135)
- Dose intensive regimens like hyper-CHOP and hyper-CVAD (hyperfractionated cyclophosphamide, vincristine, doxorubicin, dexamethasone, methotrexate and cytarabine) are also in use (Cancer 2005;103:2091)
- Upfront consolidative autologous stem cell transplantation at first complete remission (Blood Cancer J 2016;6:e452, J Clin Oncol 2012;30:3093)
- Brentuximab vedotin for relapsed / refractory disease (J Clin Oncol 2012;30:2190)
- Chimeric antigen receptor (CAR) T cell therapy and checkpoint inhibitors are now under evaluation (ClinicalTrials: NCT02581631 [Accessed 10 April 2020], ClinicalTrials: NCT02274584 [Accessed 10 April 2020])
Gross description
- Enlarged lymph nodes
- Firm fleshy mass
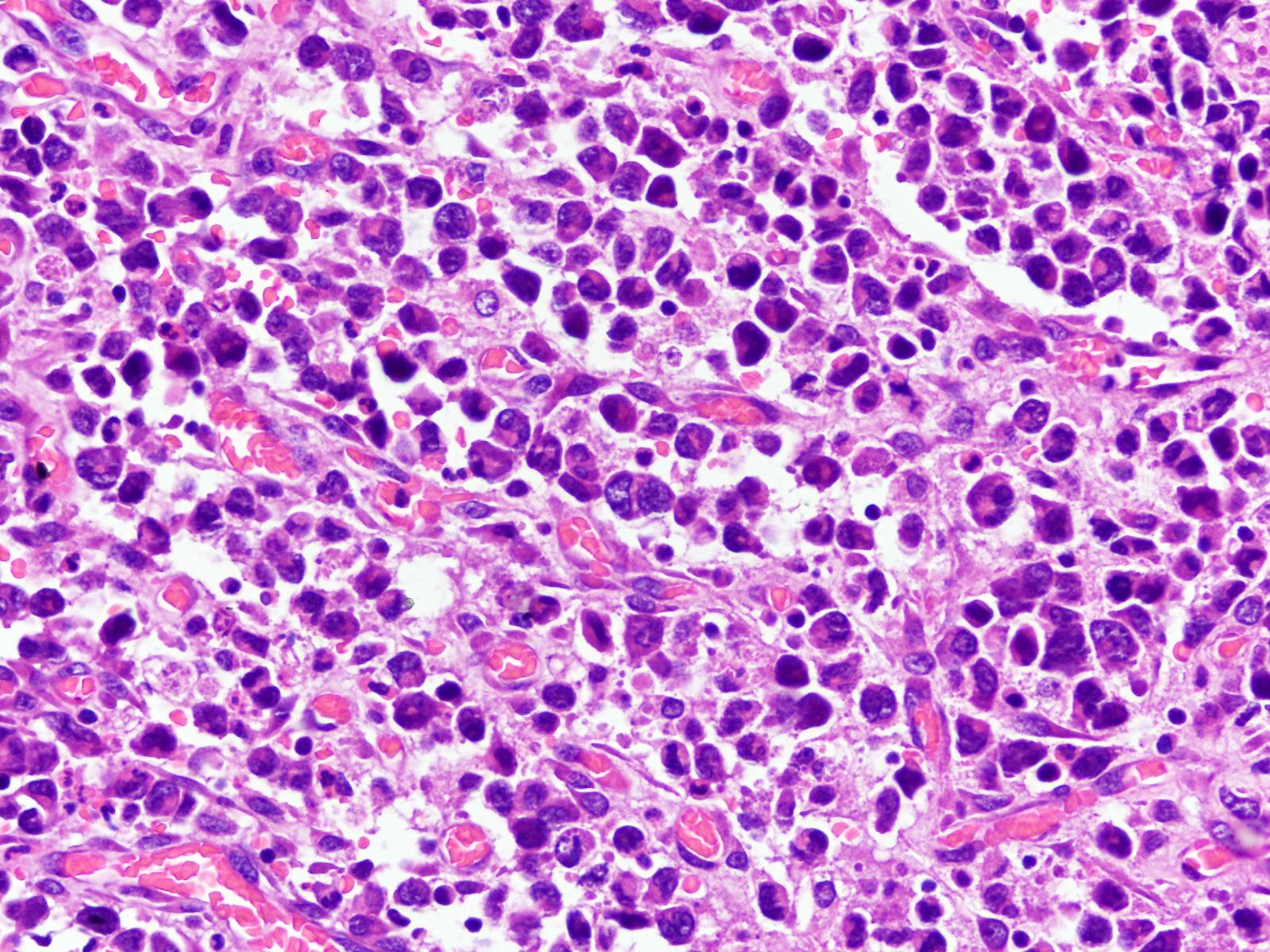
Microscopic (histologic) description
- Most of the time, morphologically indistinguishable from ALCL, ALK positive
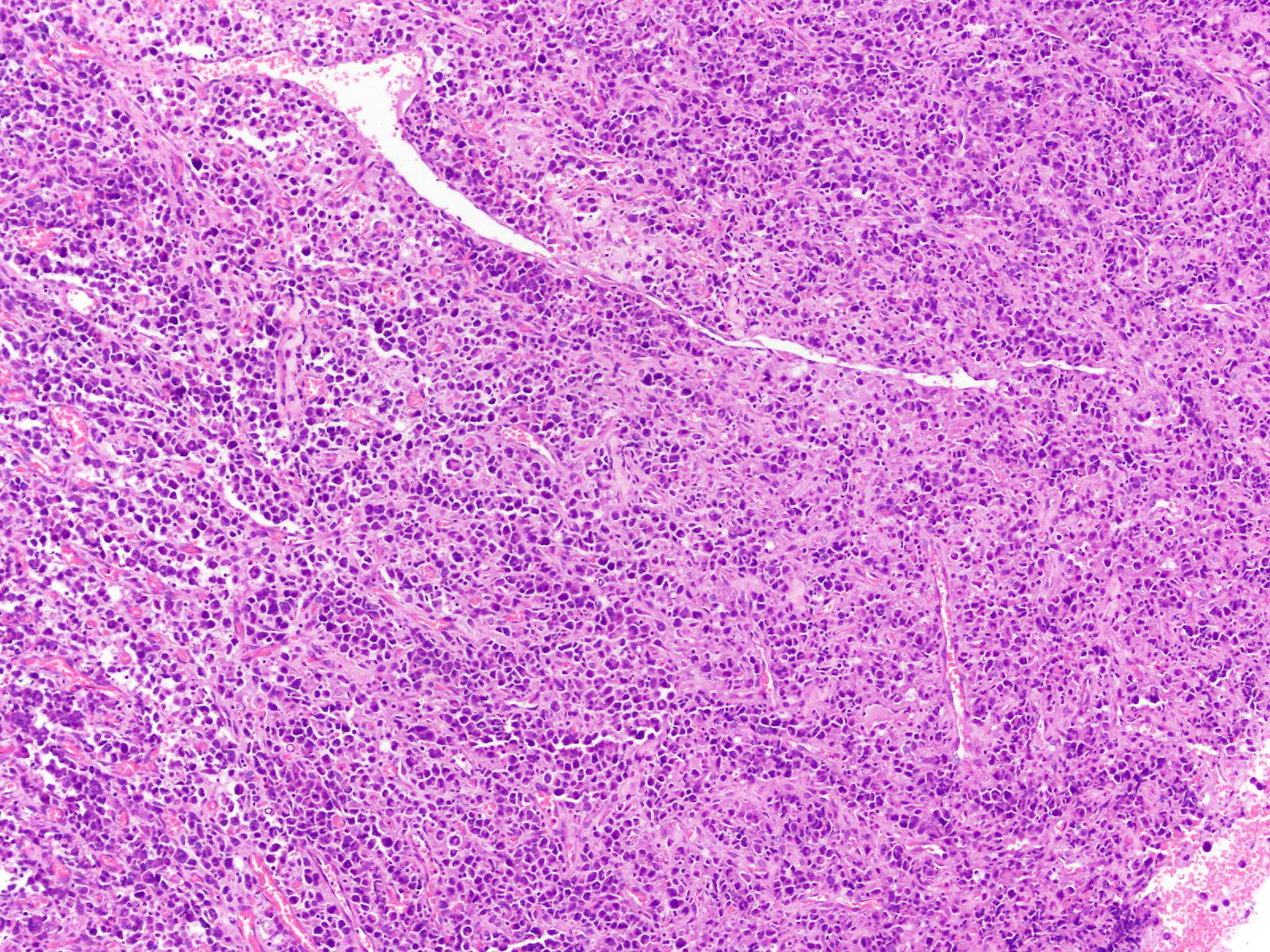
- Effaced architecture with solid, cohesive sheets of neoplastic cells
- May show preserved lymph node architecture with neoplastic cells growing intrasinusoidally or only within the T cell areas
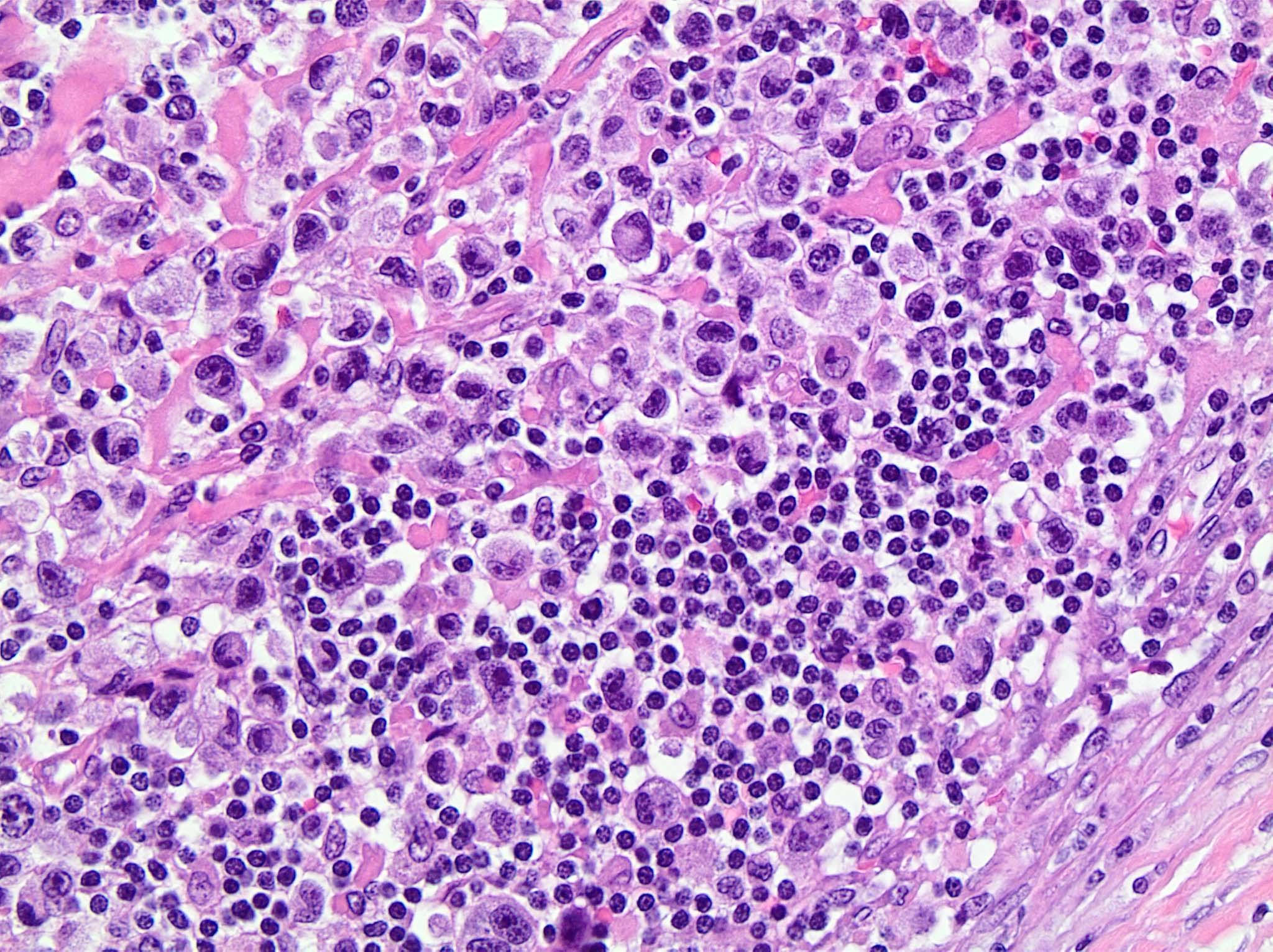
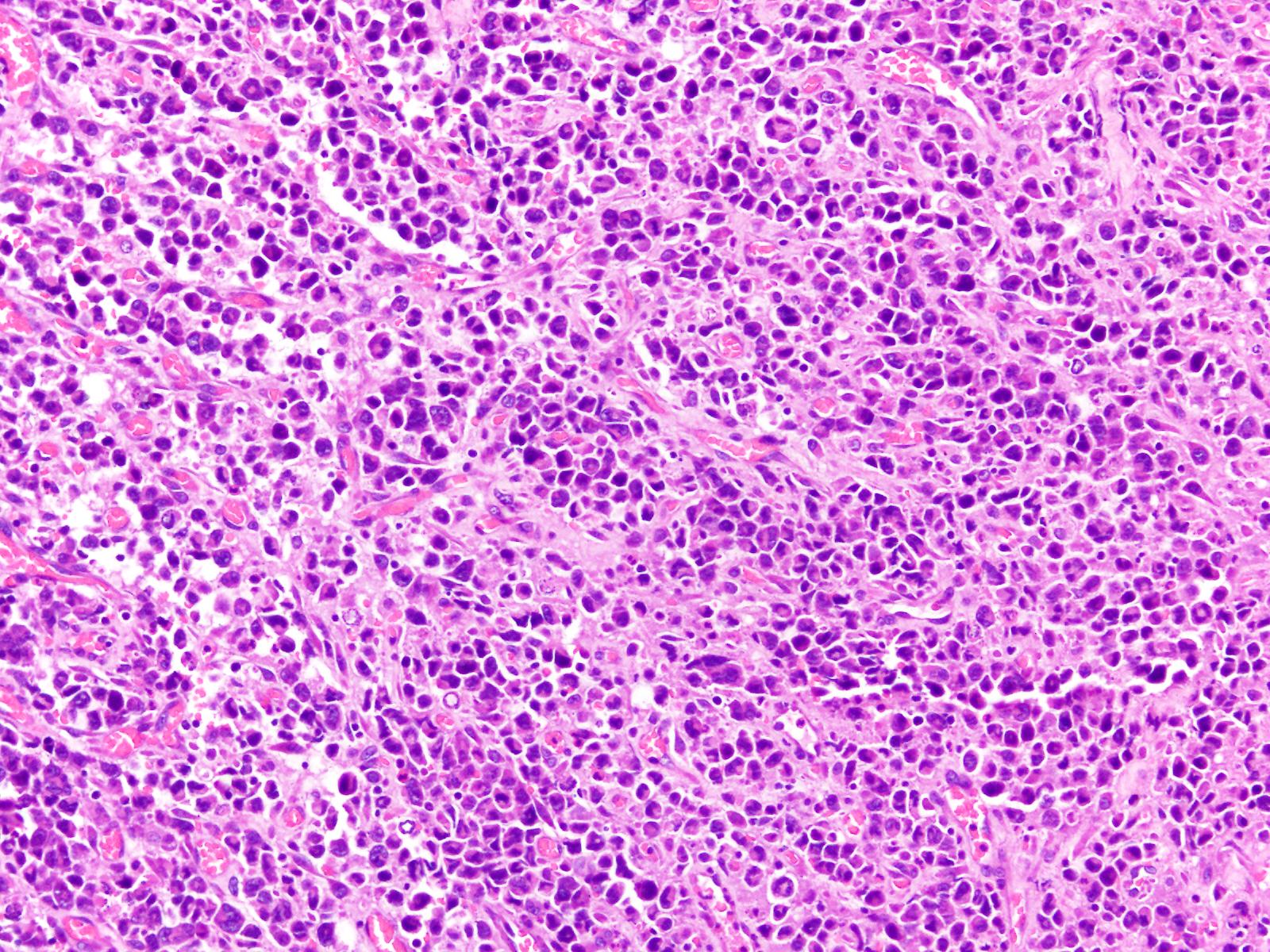
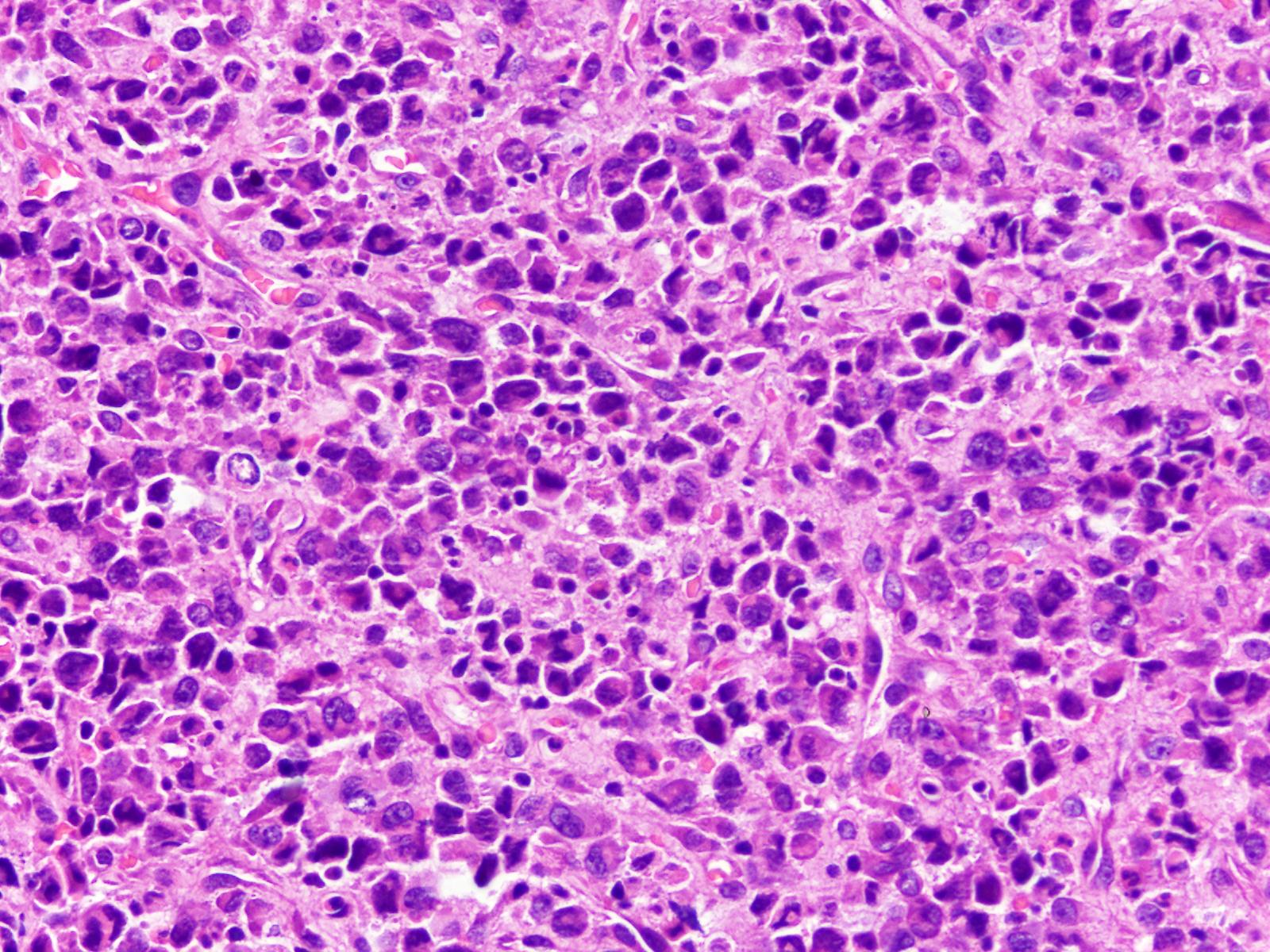
- Large cells with round to indented nuclei, deeply staining cytoplasm, with prominent Golgi zone
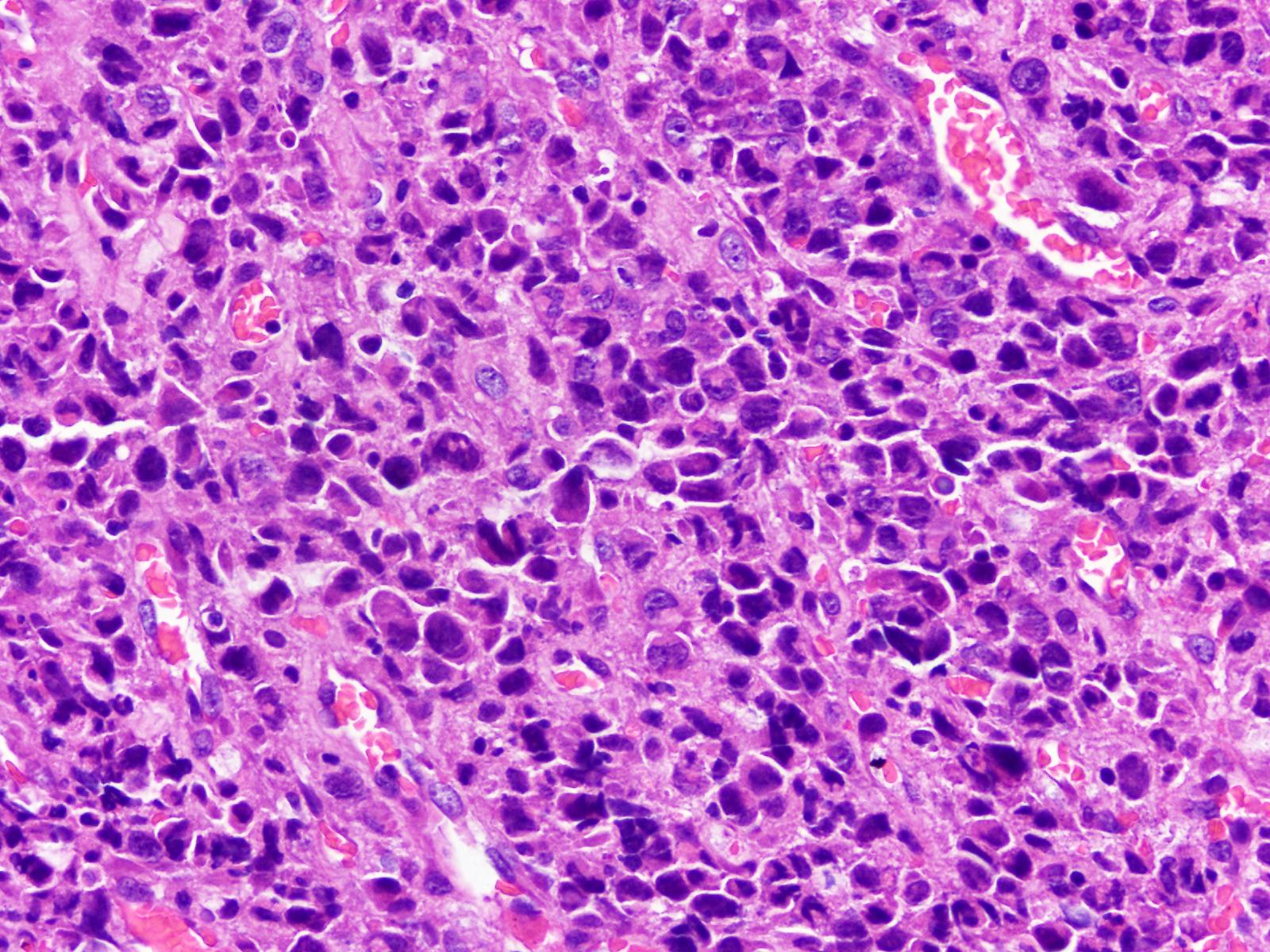
- Hallmark cells (cells with eccentric, horseshoe or kidney shaped nuclei)
- Small cells, as described in the small cell or lymphohistiocytic variant of ALCL, ALK positive, are uncommon
- Cases with DUSP22 rearrangements show smaller, monomorphic cells with prominent nucleoli and central nuclear pseudoinclusions (doughnut cells) (Haematologica 2019;104:e158)
- Cases positive for DUSP22 rearrangements lack a cytotoxic phenotype
- Cases with ERBB4 and COL29A1 expression show Hodgkin-like morphology (Blood 2016;127:221)
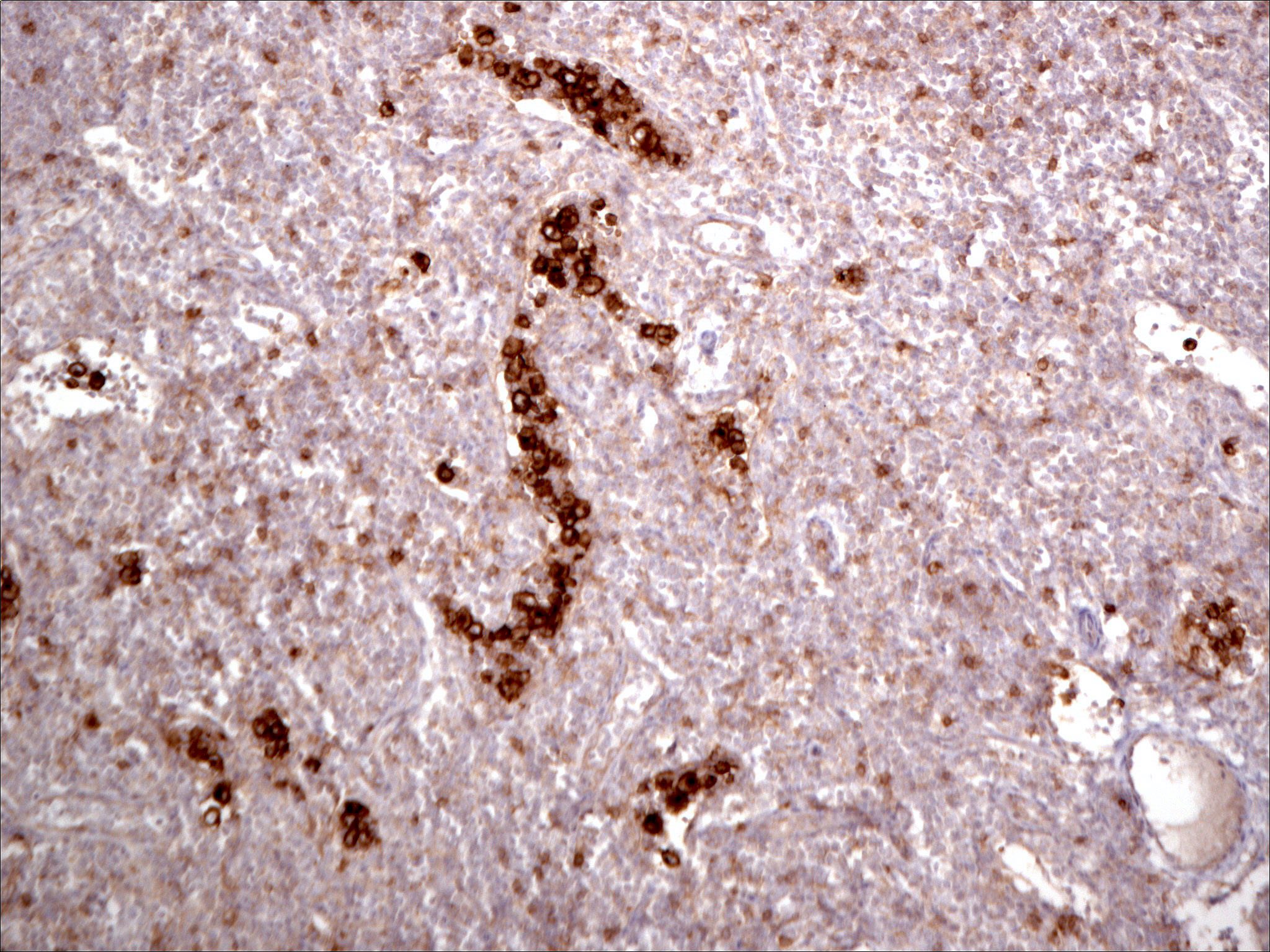
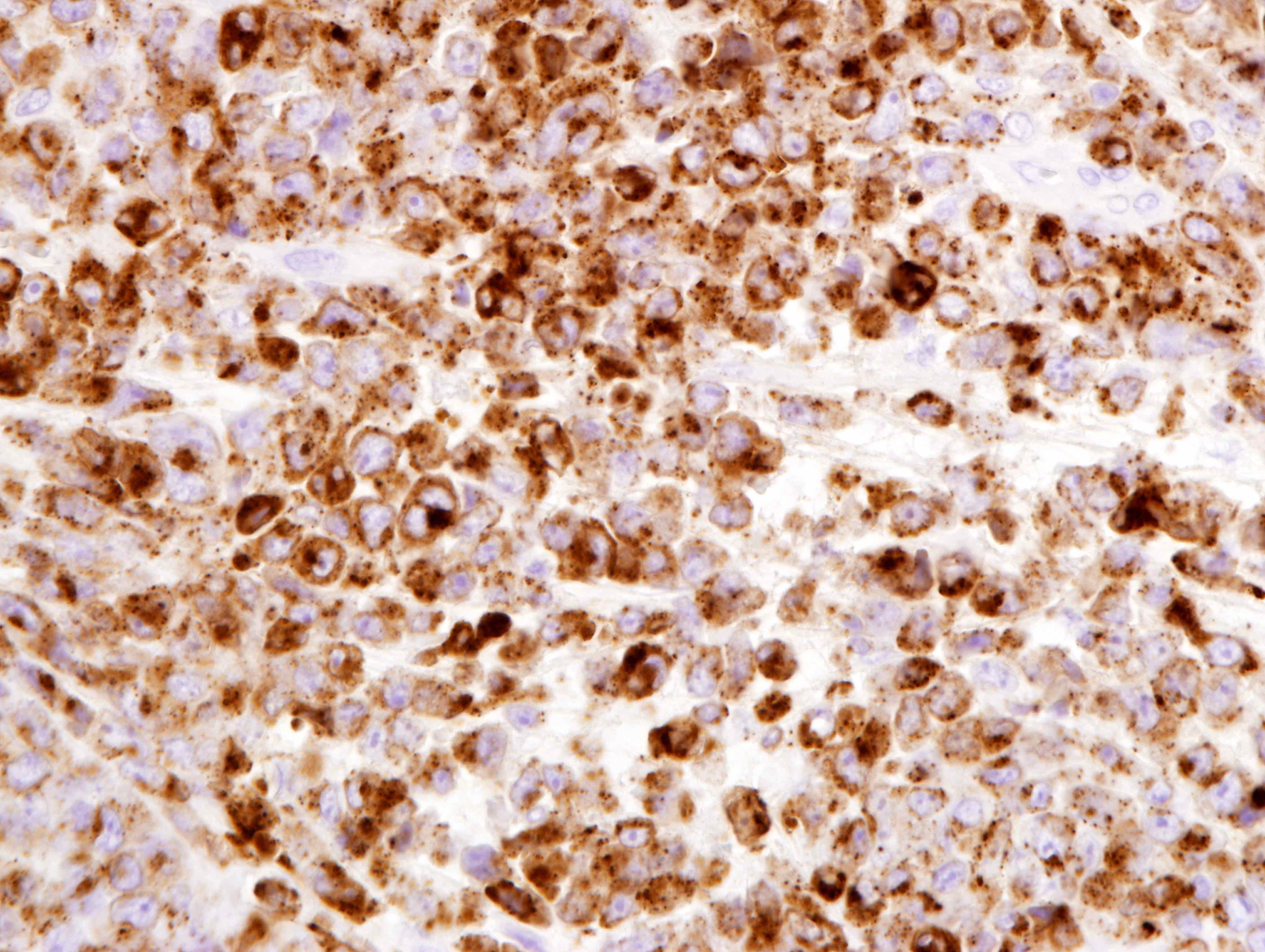
Microscopic (histologic) images
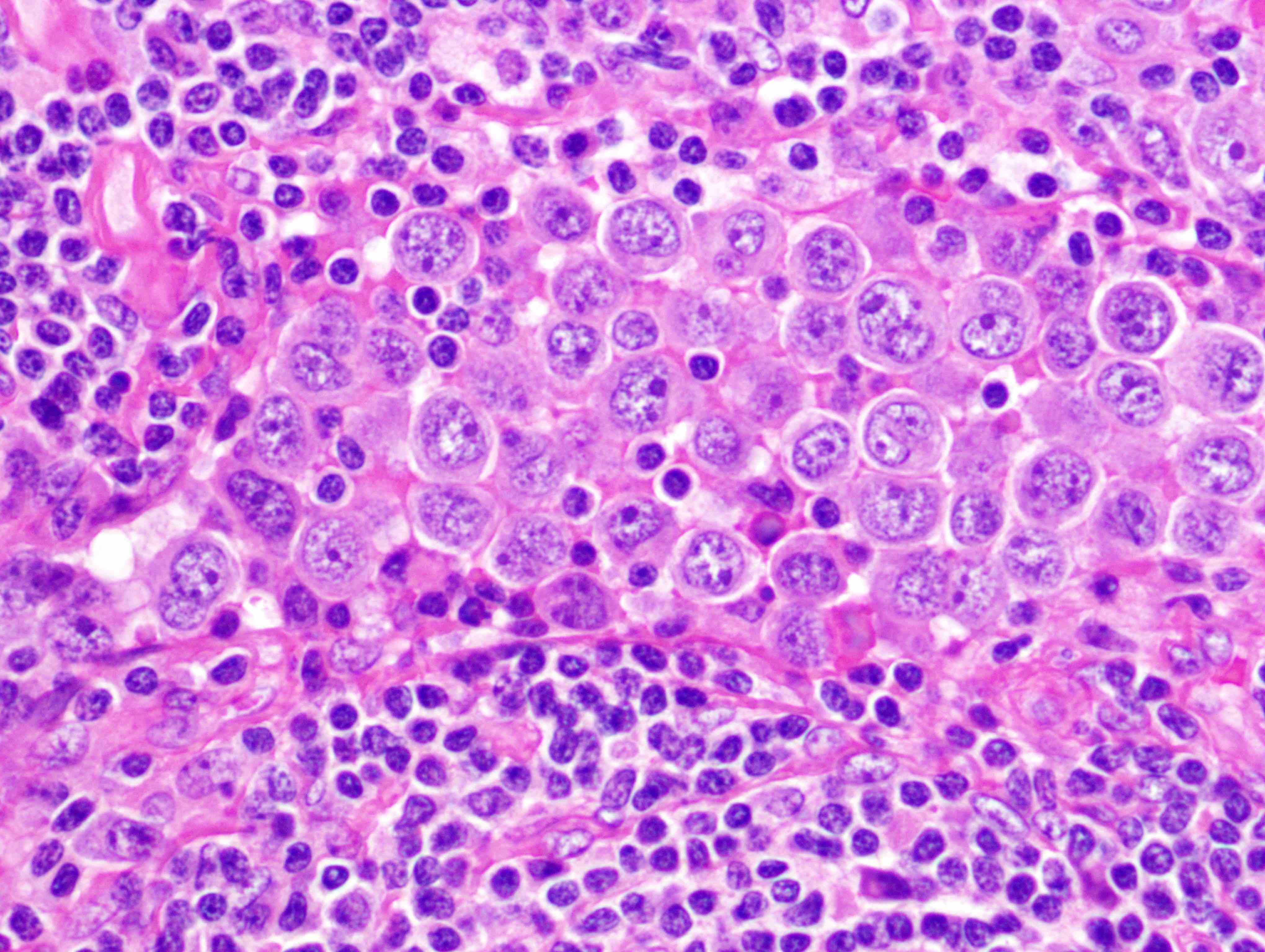
Contributed by Jayalakshmi Balakrishna, M.D. and Elaine S. Jaffe, M.D.
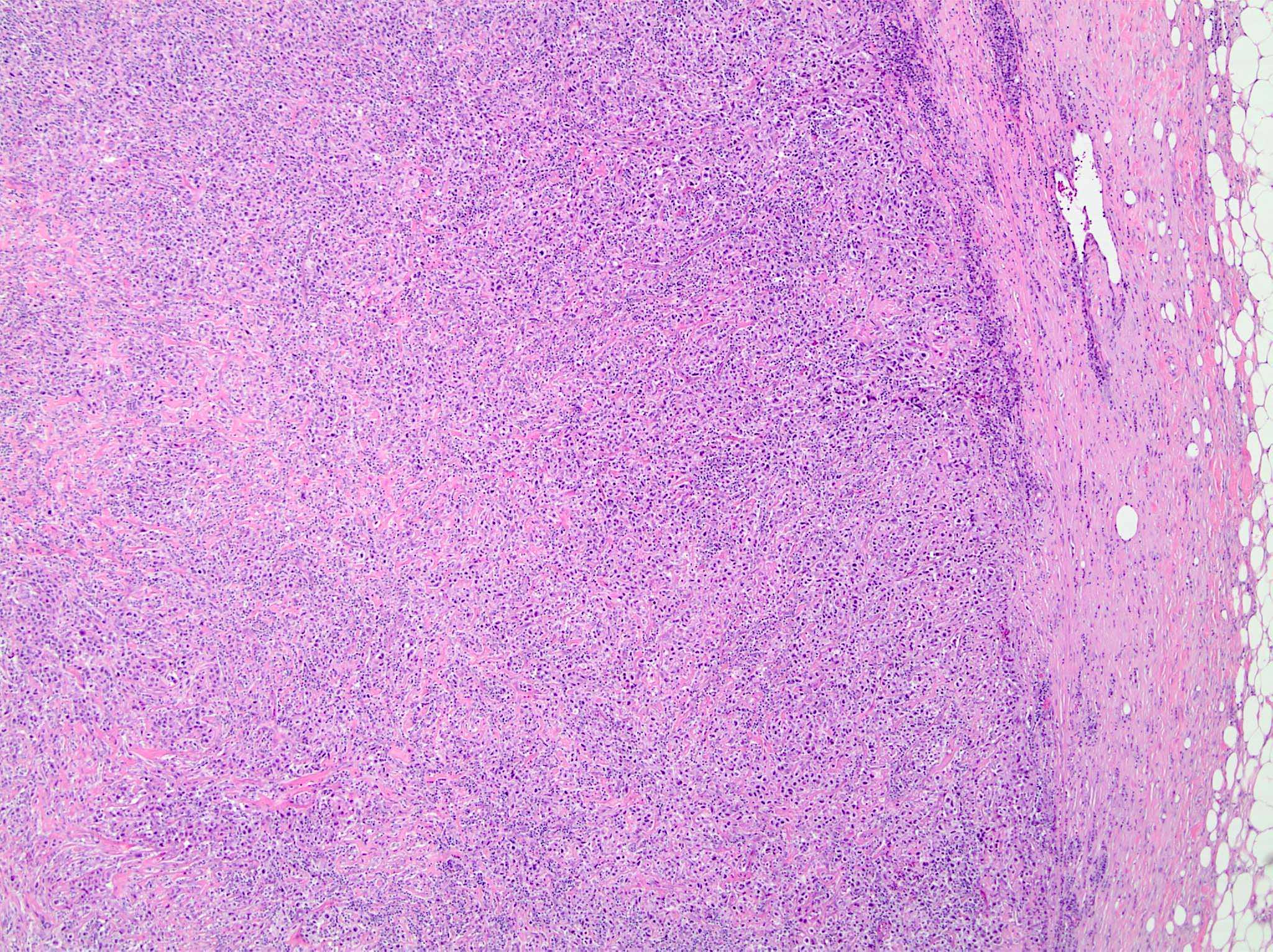
Diffuse infiltrate
Invasion of sinus
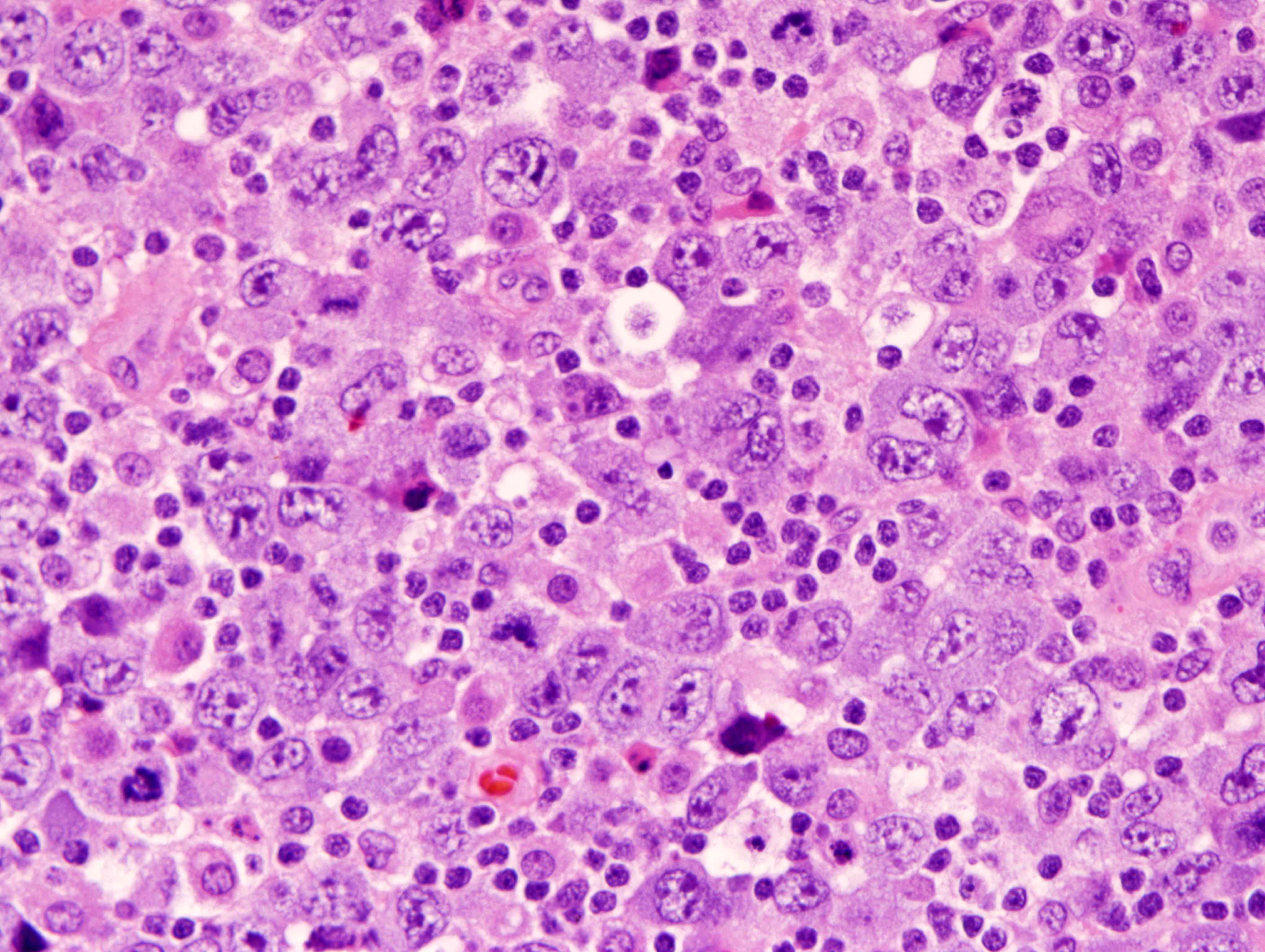
Large atypical cells
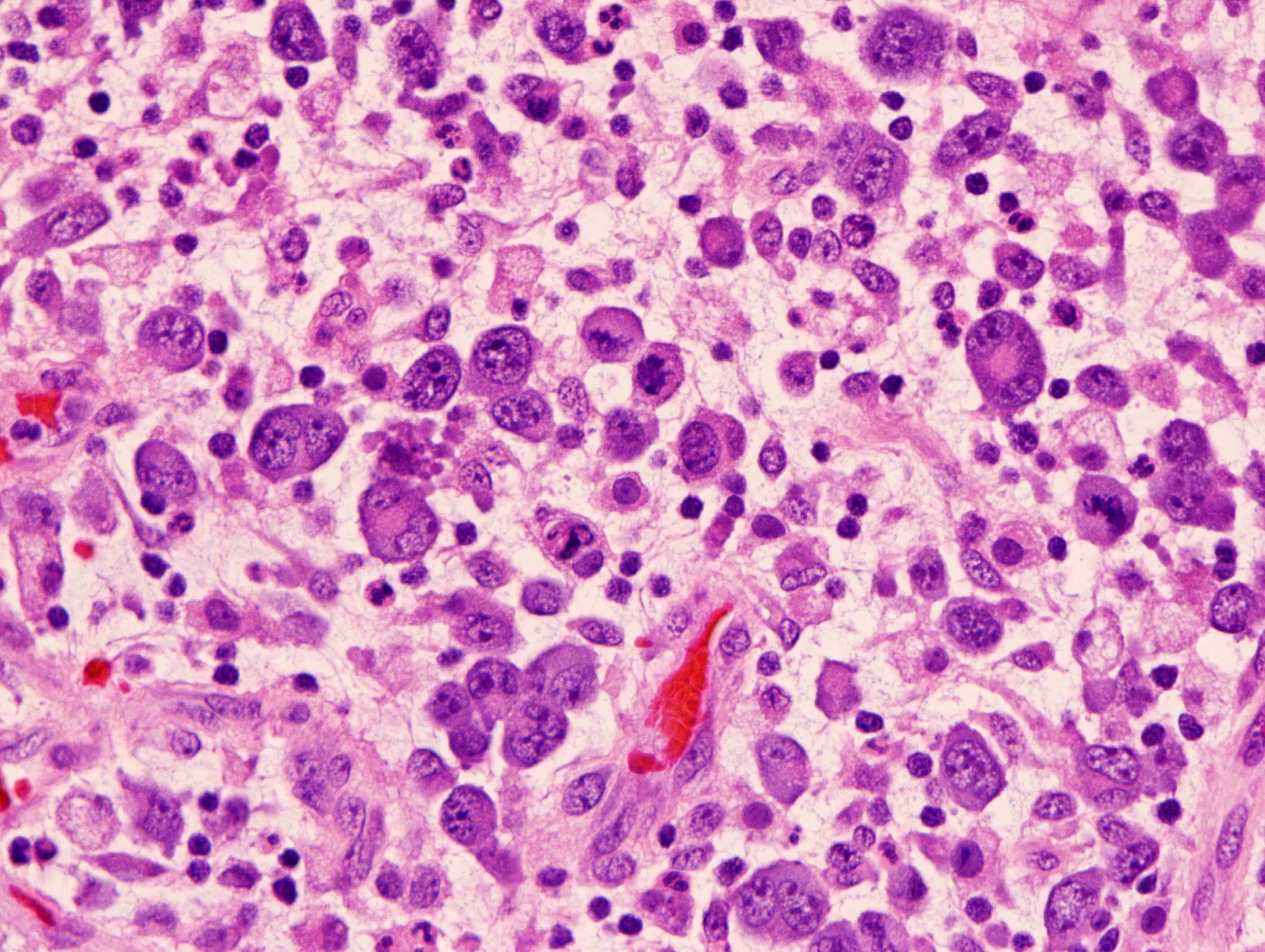
Mitotic figures and apoptotic bodies
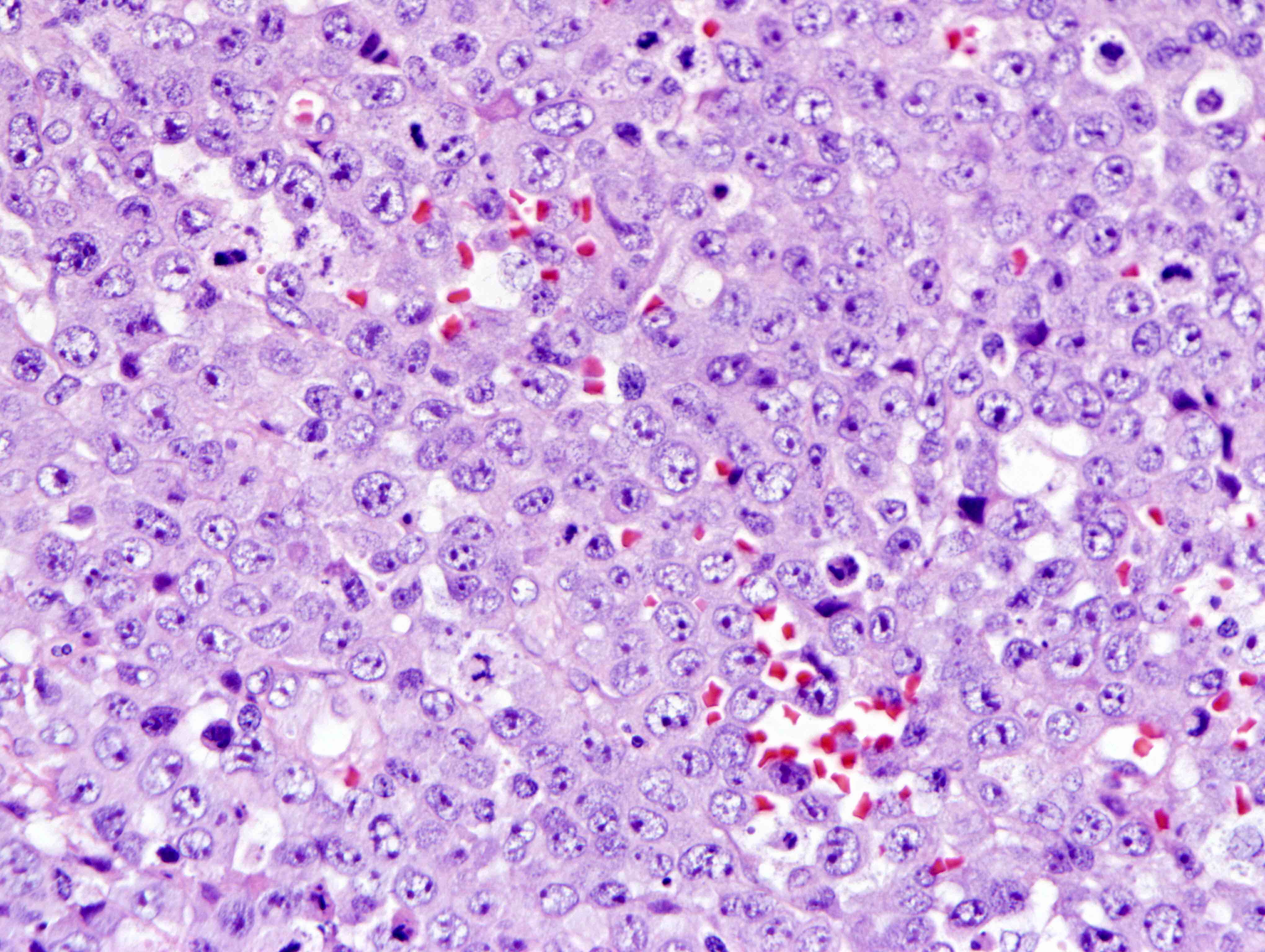
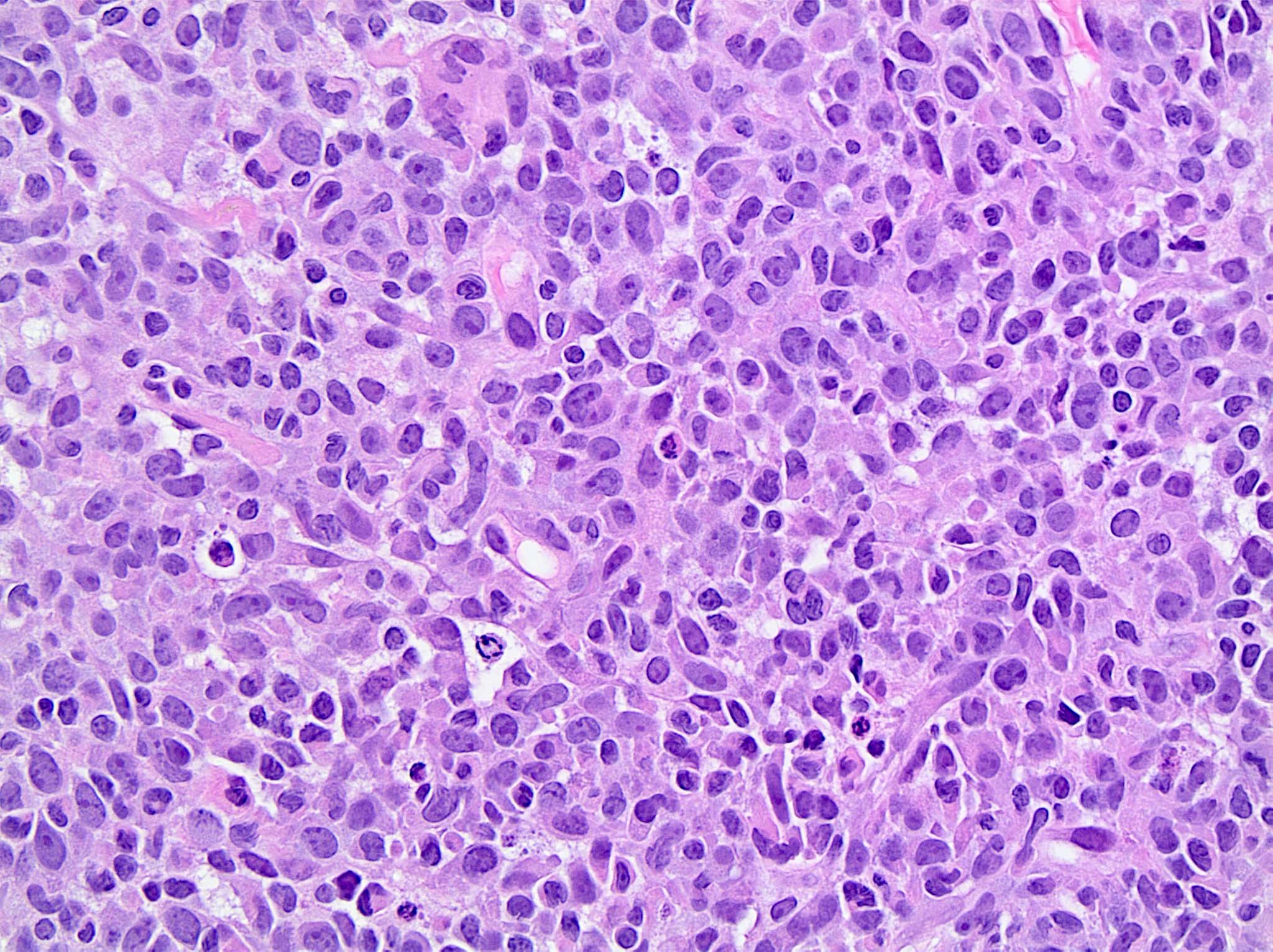
Large atypical cells
Large atypical cells
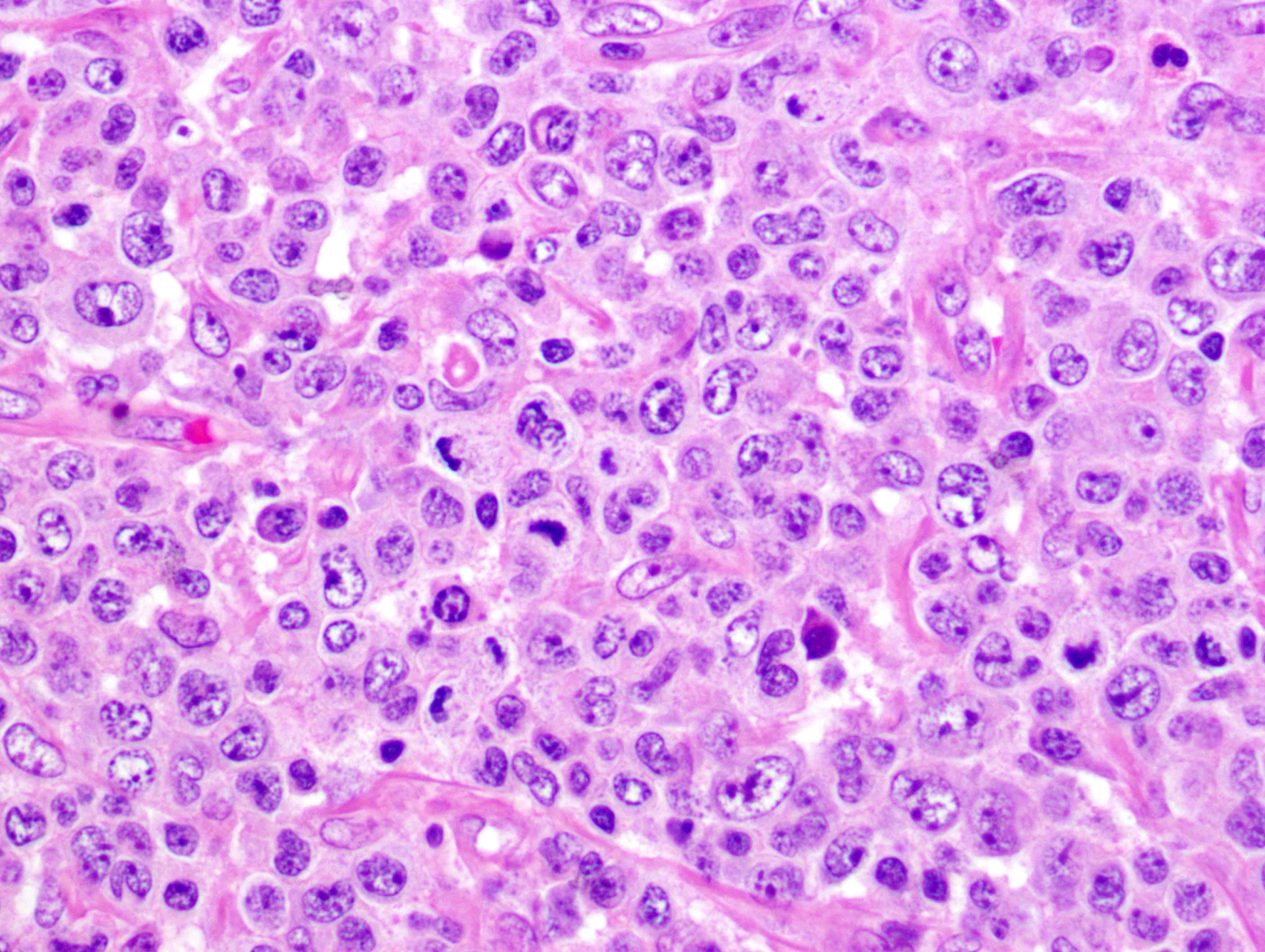
Hallmark cells
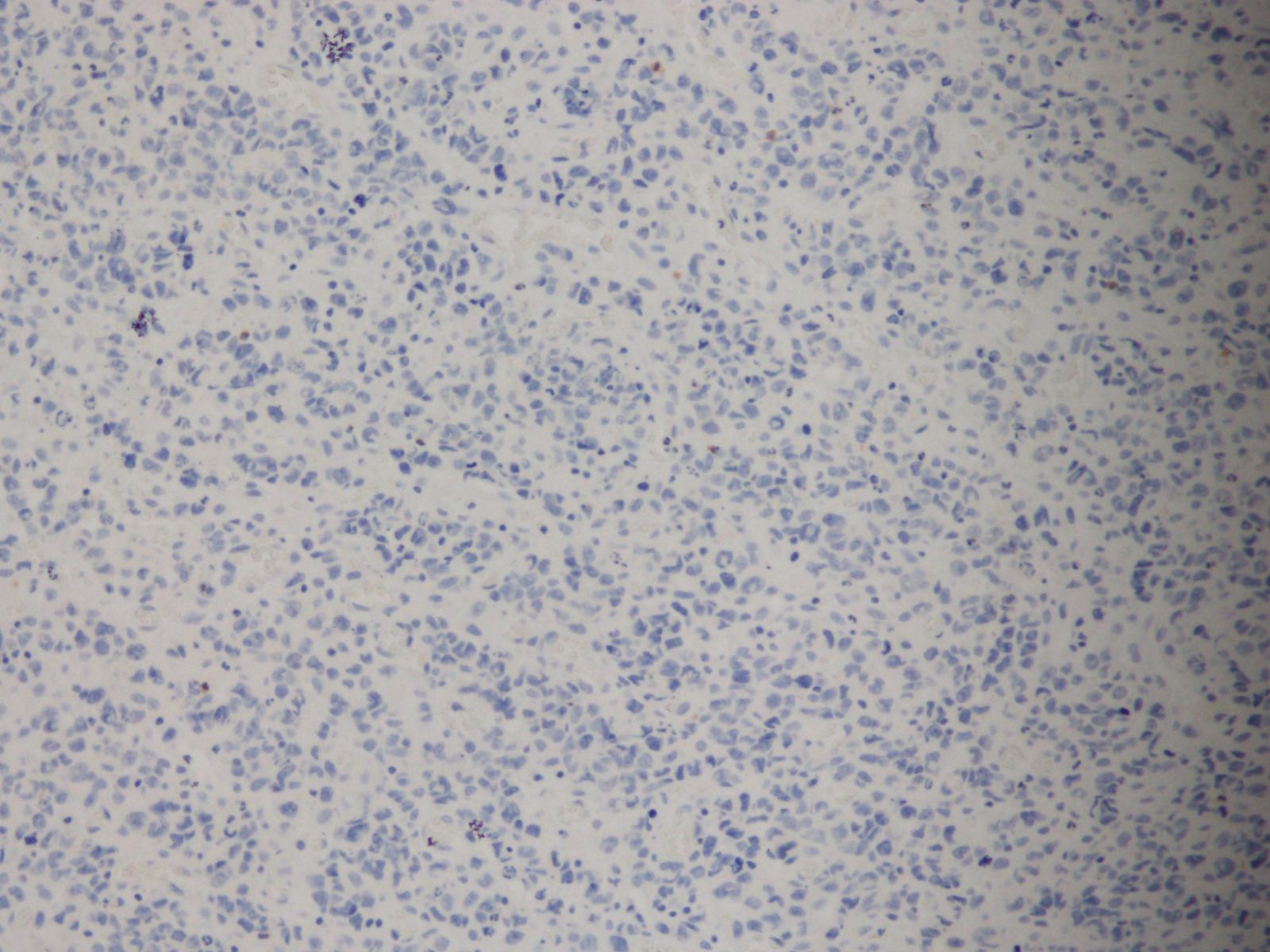
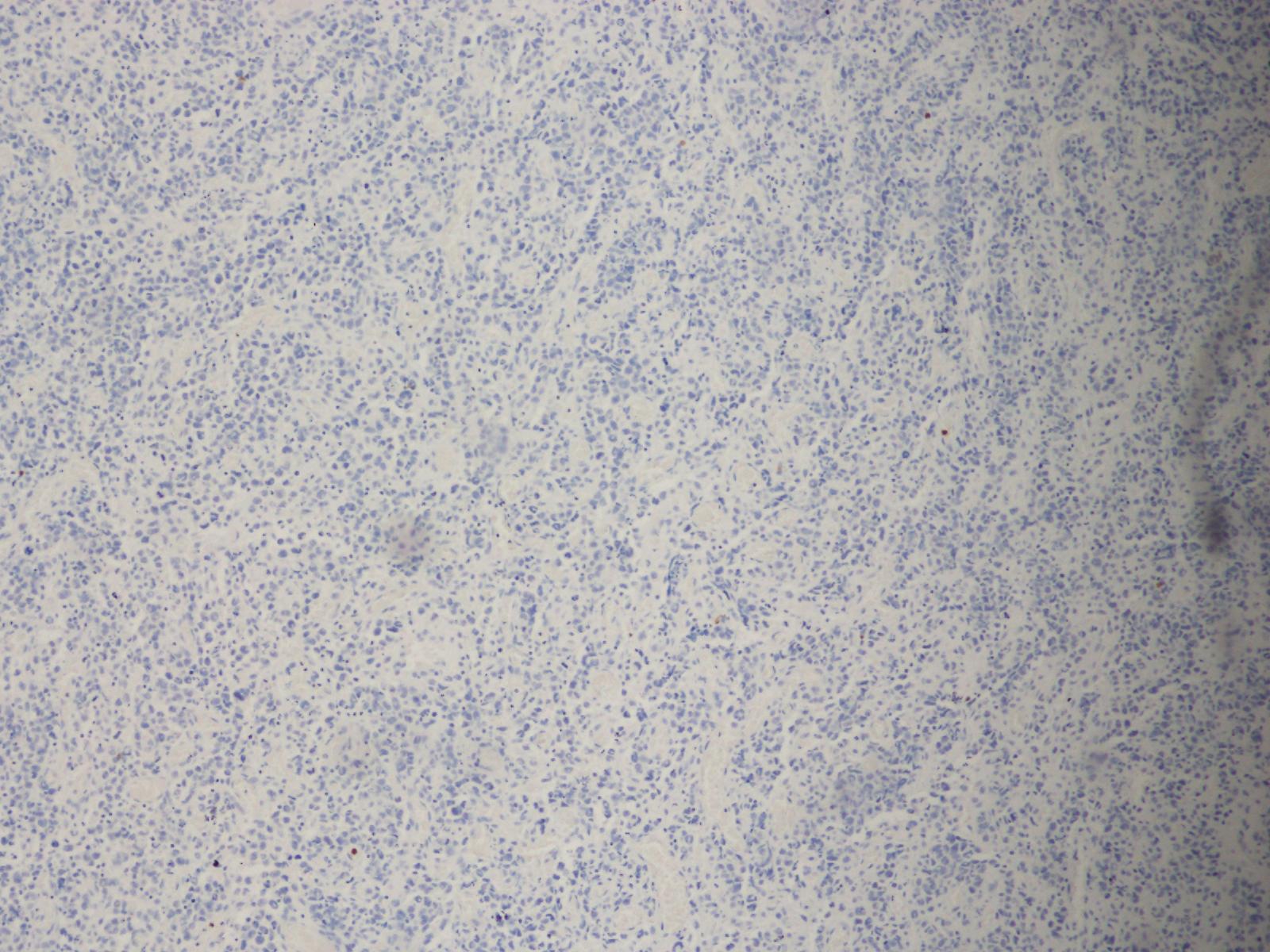
IHC stain, CD3
IHC stain, CD4
IHC stain, CD3
IHC stain, CD25
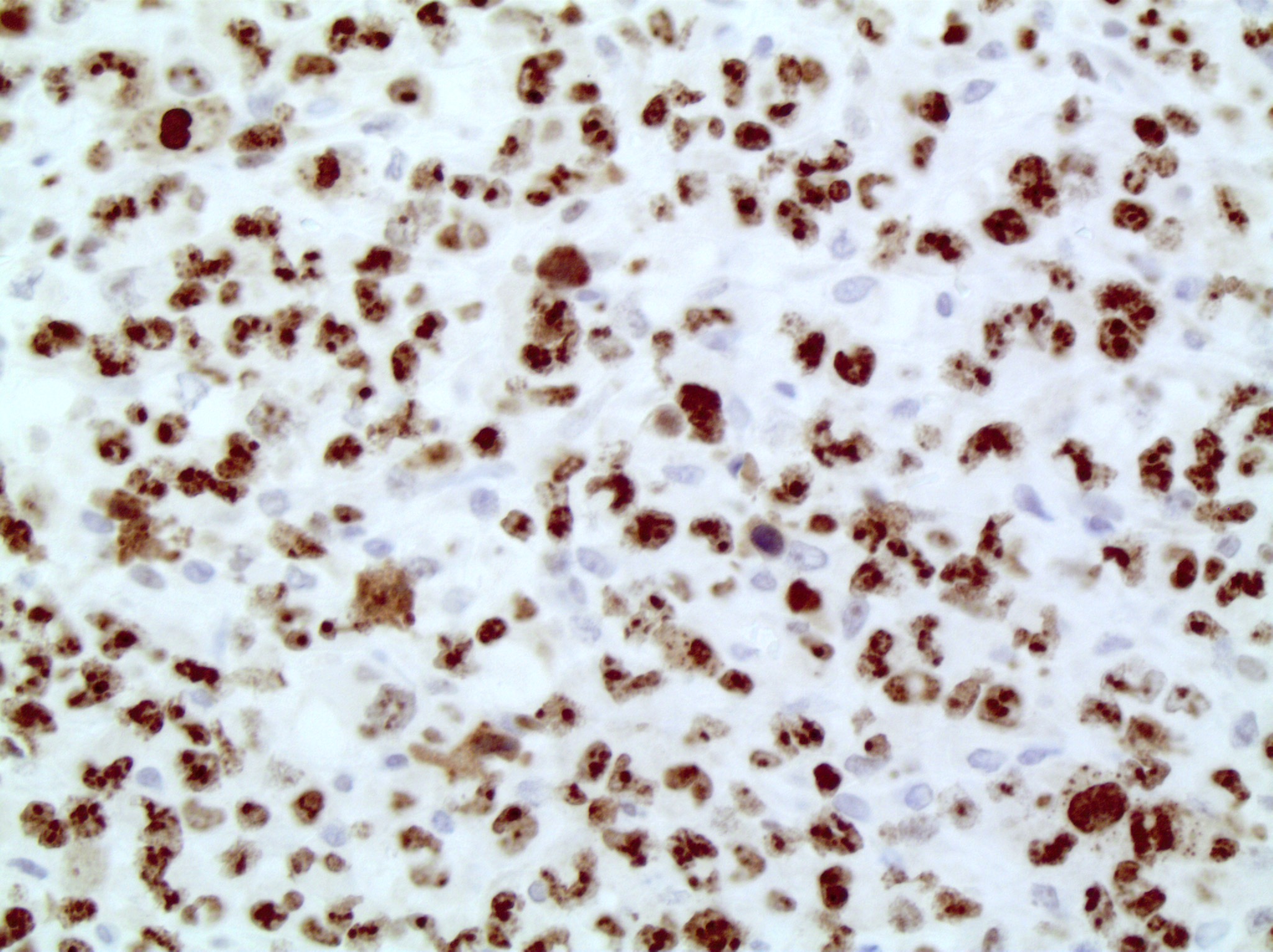
IHC stain, Ki67

IHC stain, CD2
IHC stain, perforin
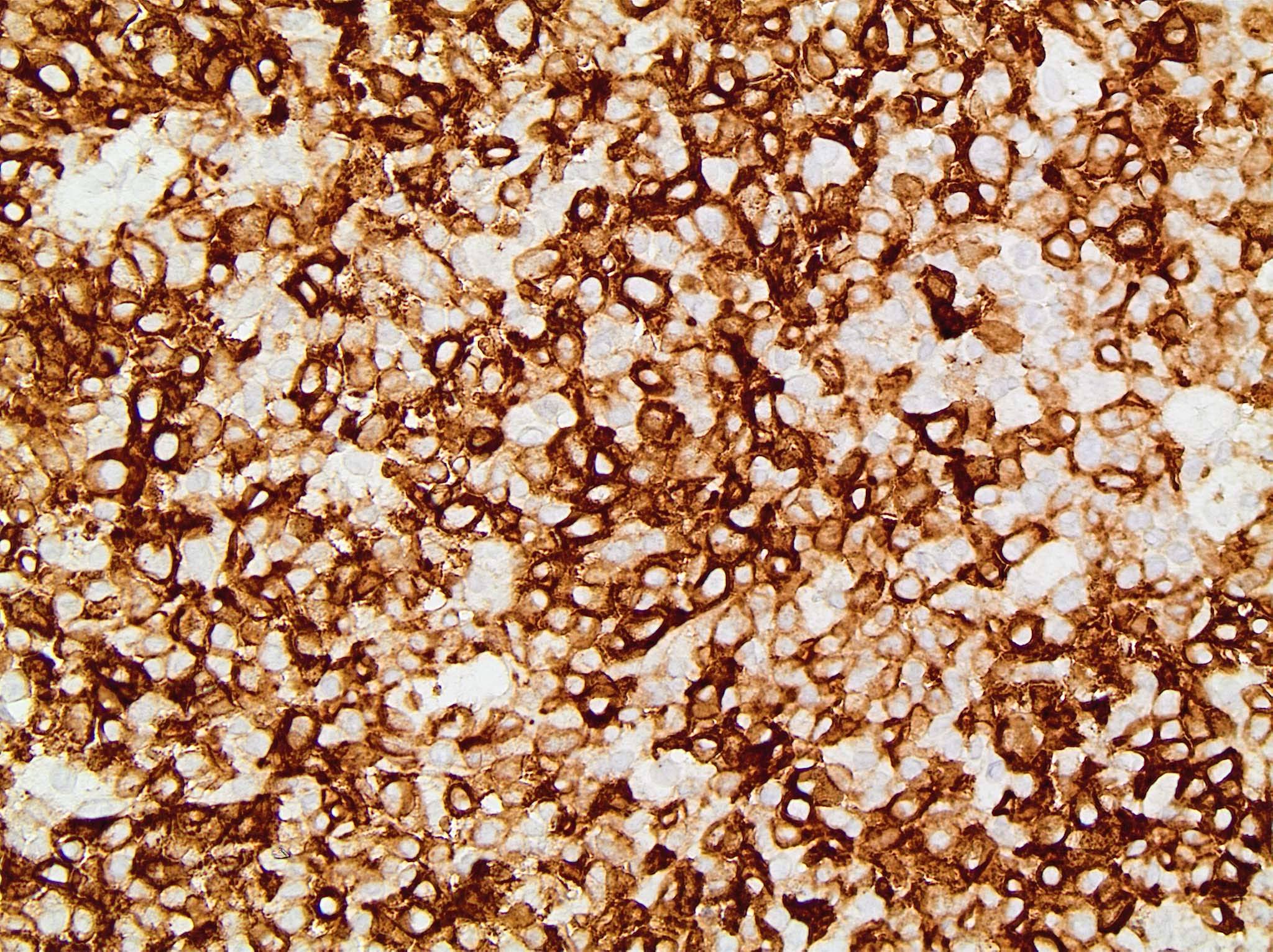
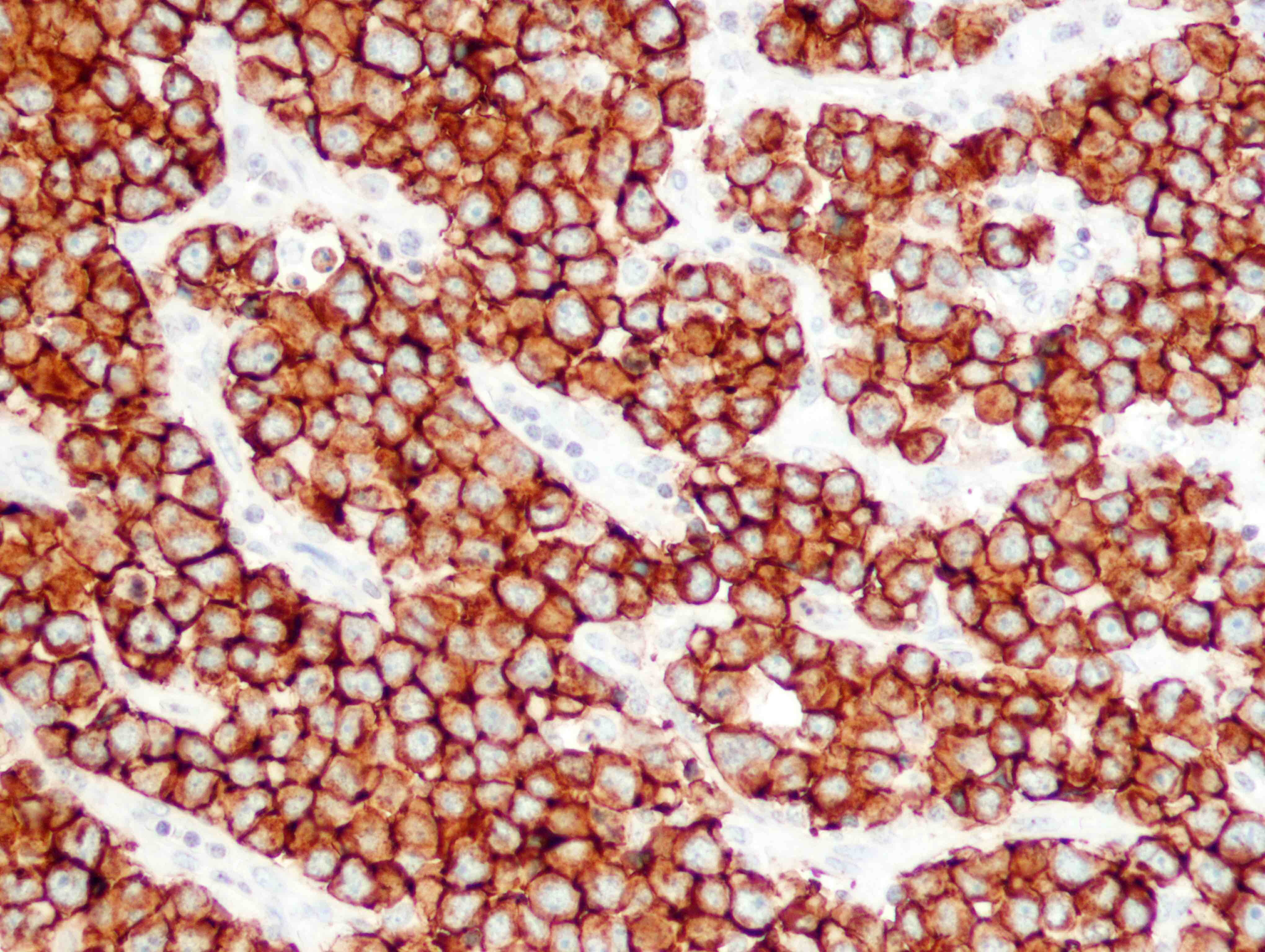
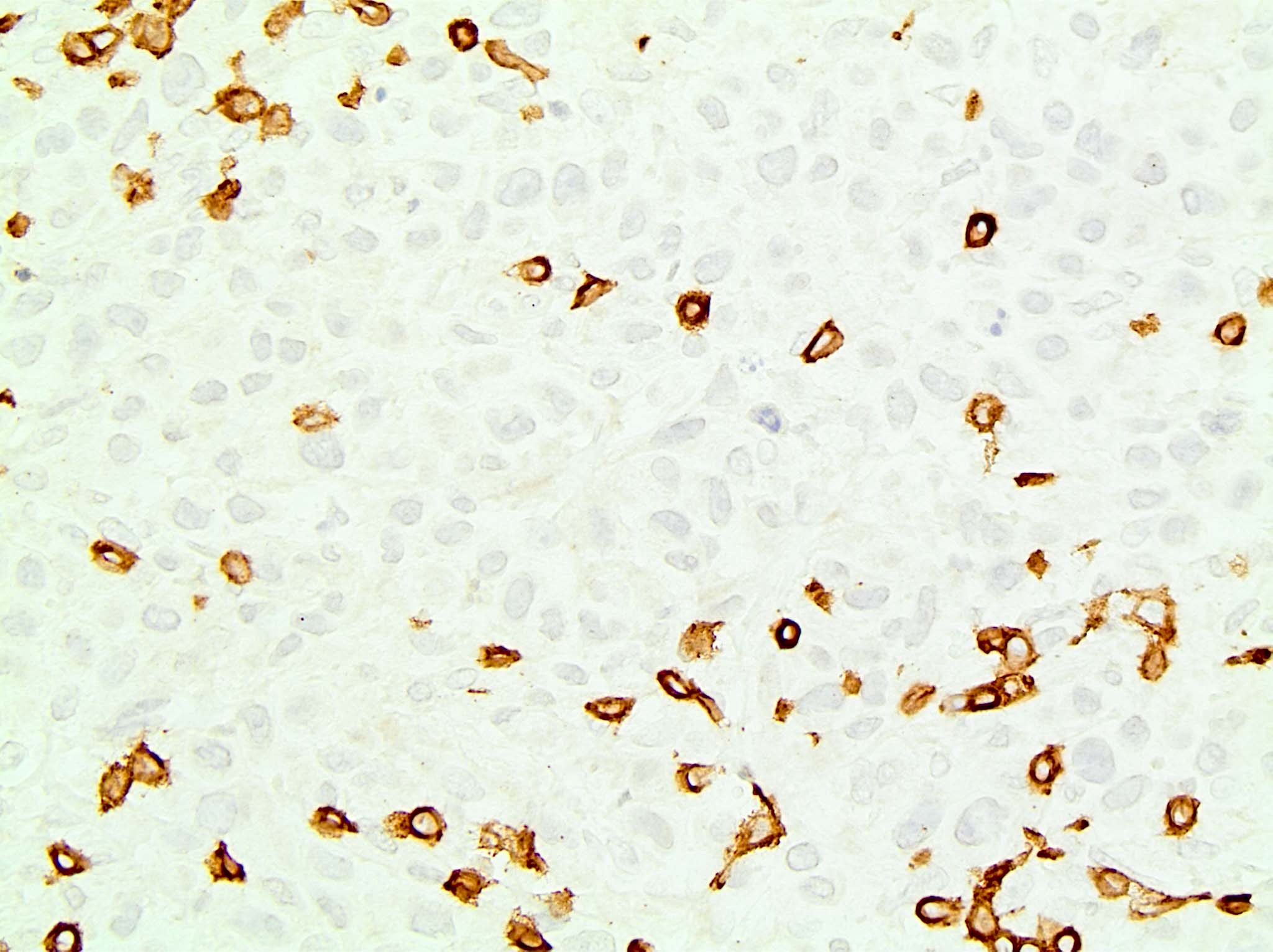
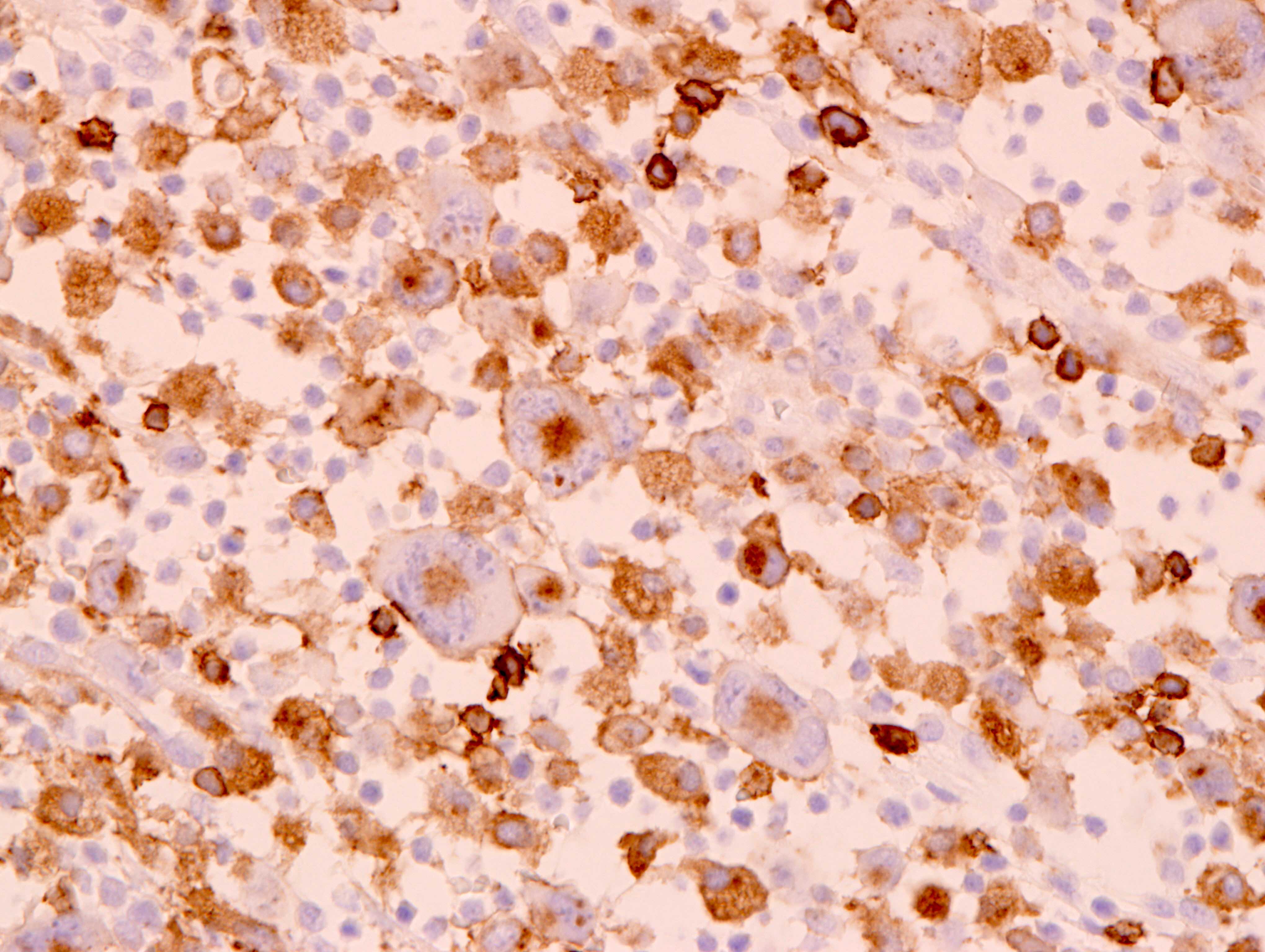
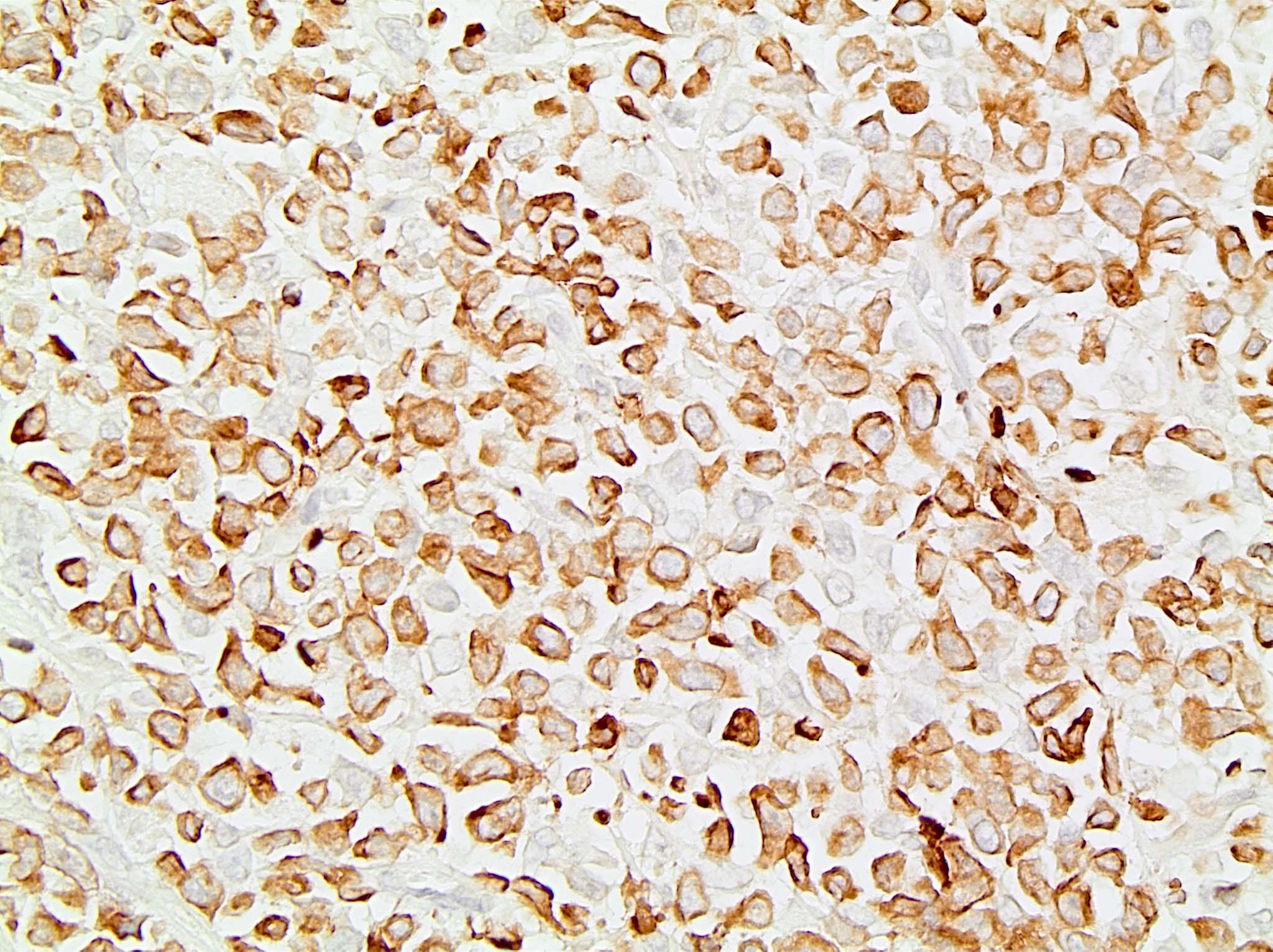
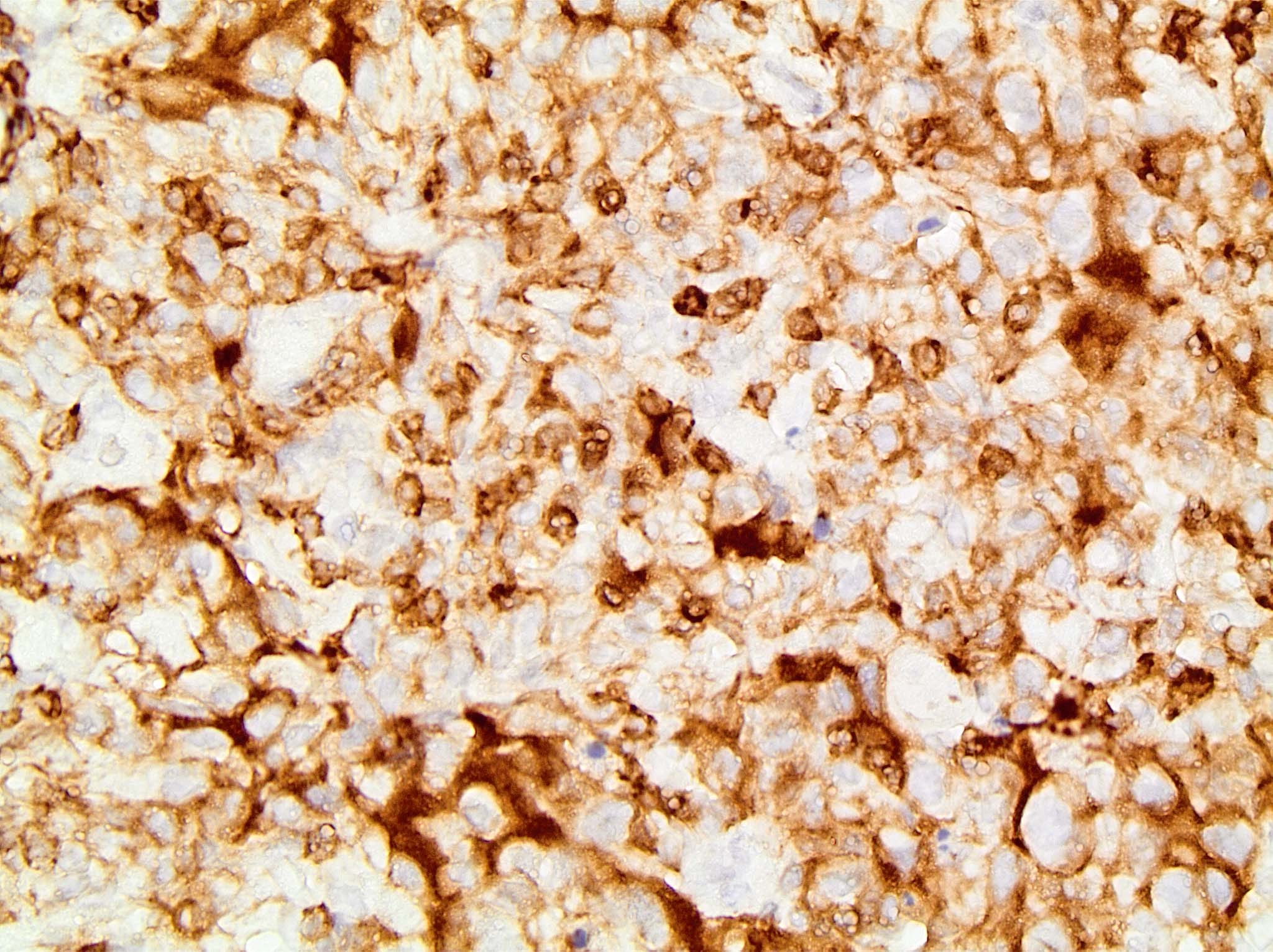
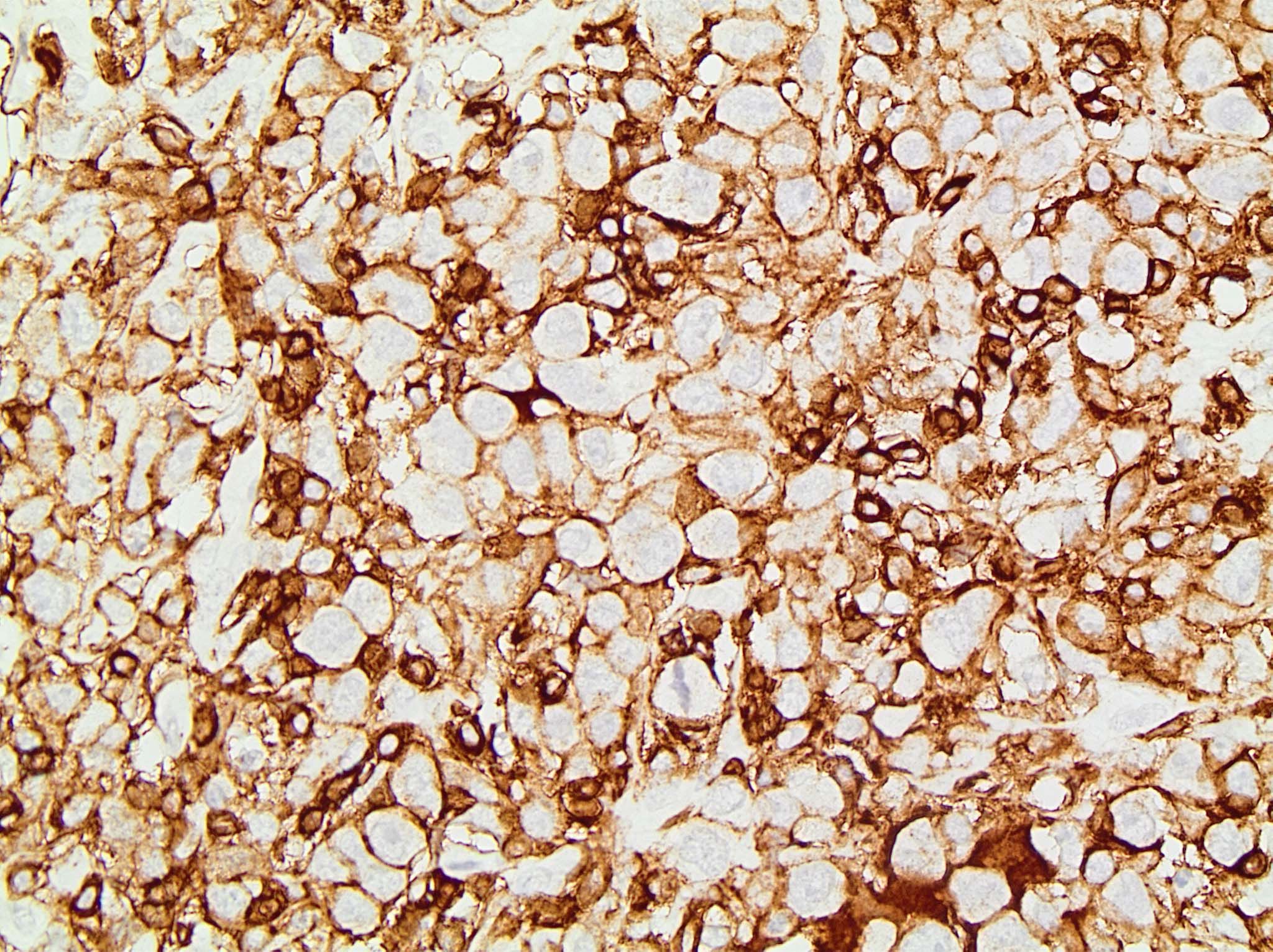
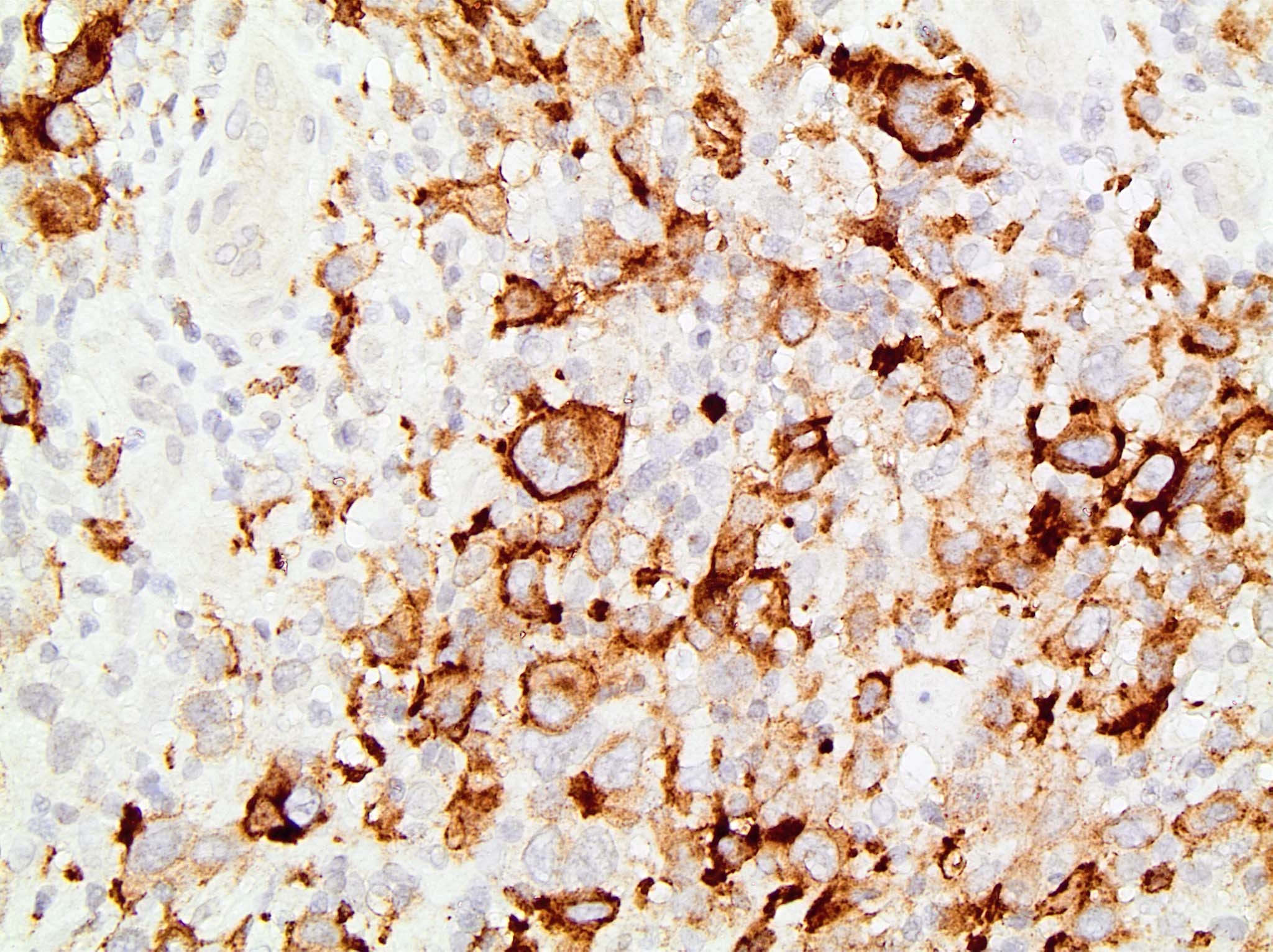
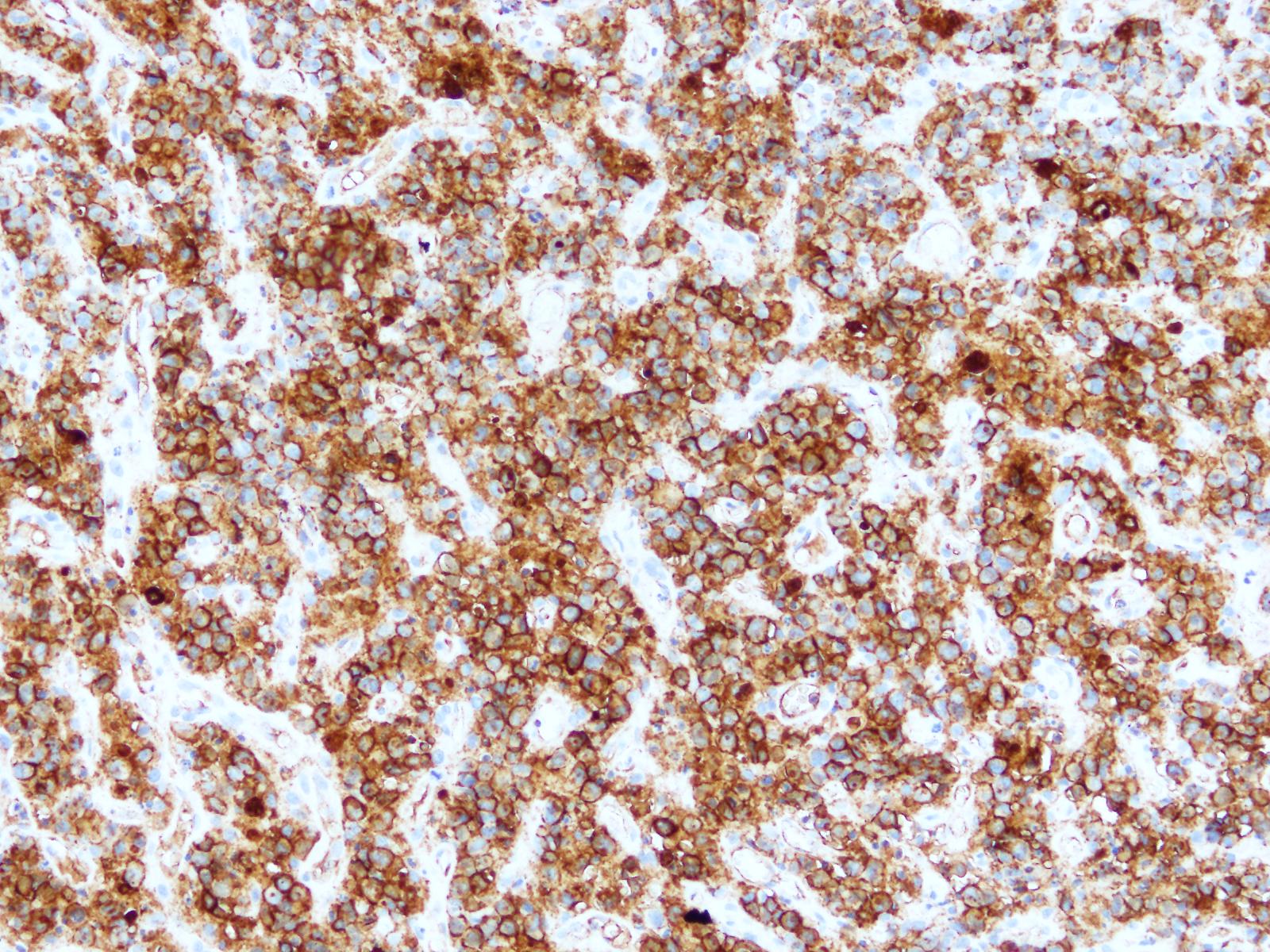
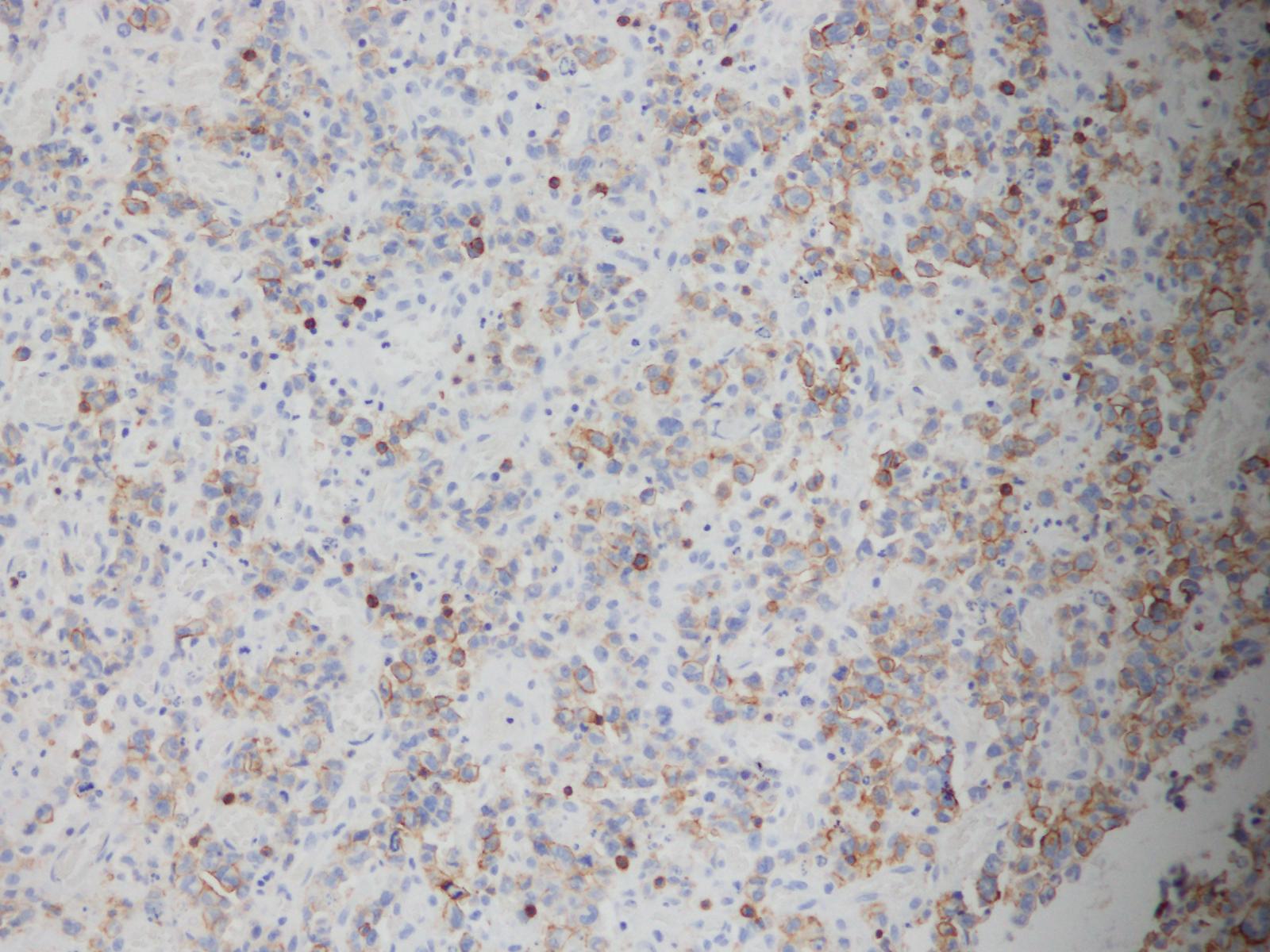
IHC stain, CD30
IHC stain, CD43
IHC stain, CD45
IHC stain, EMA

IHC stain, granzyme
Contributed by Doan Minh Khuy, M.D.
23 year old man with a cervical lymphoid nodule, no B symptoms
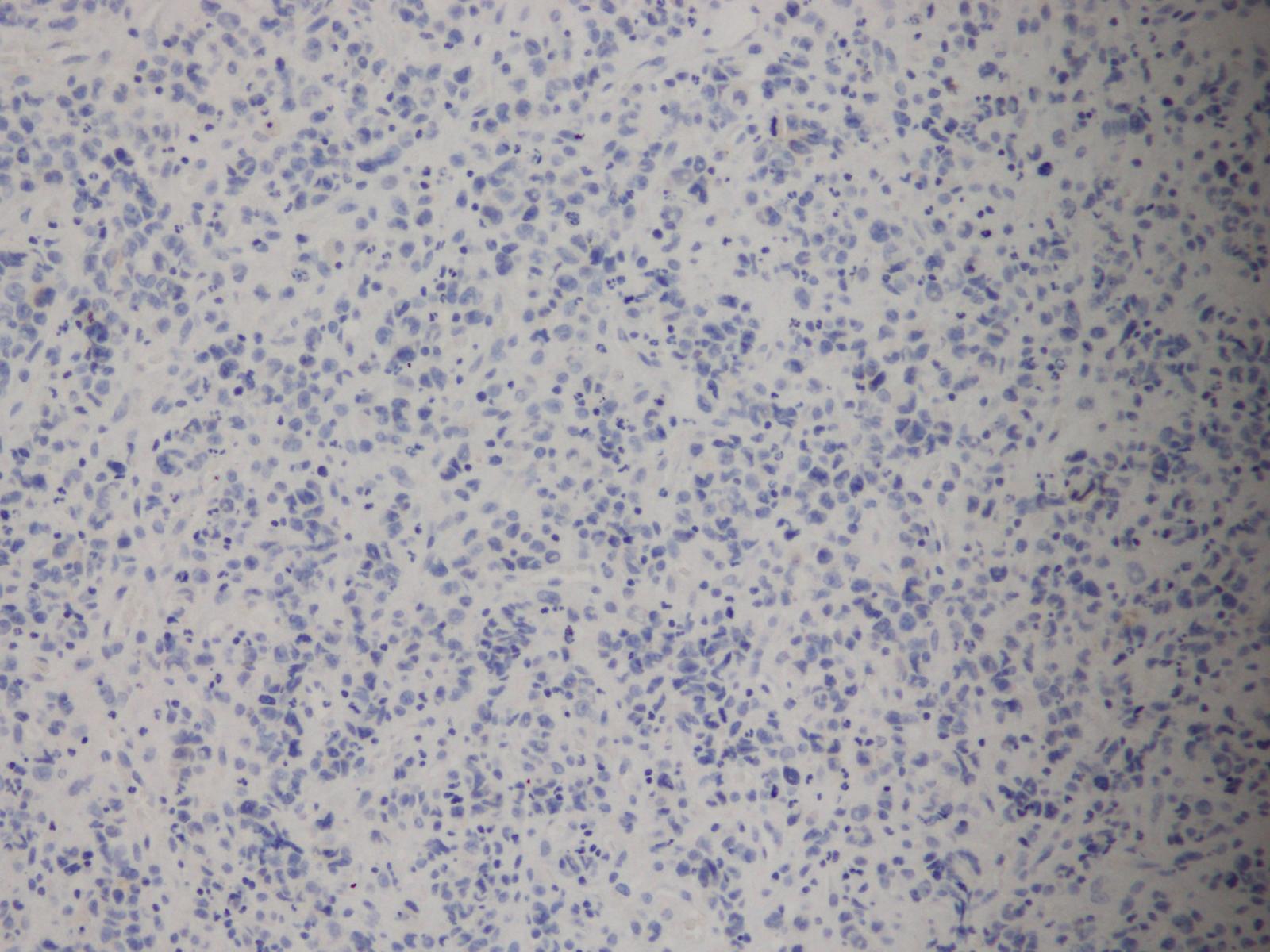
CK-
EMA+
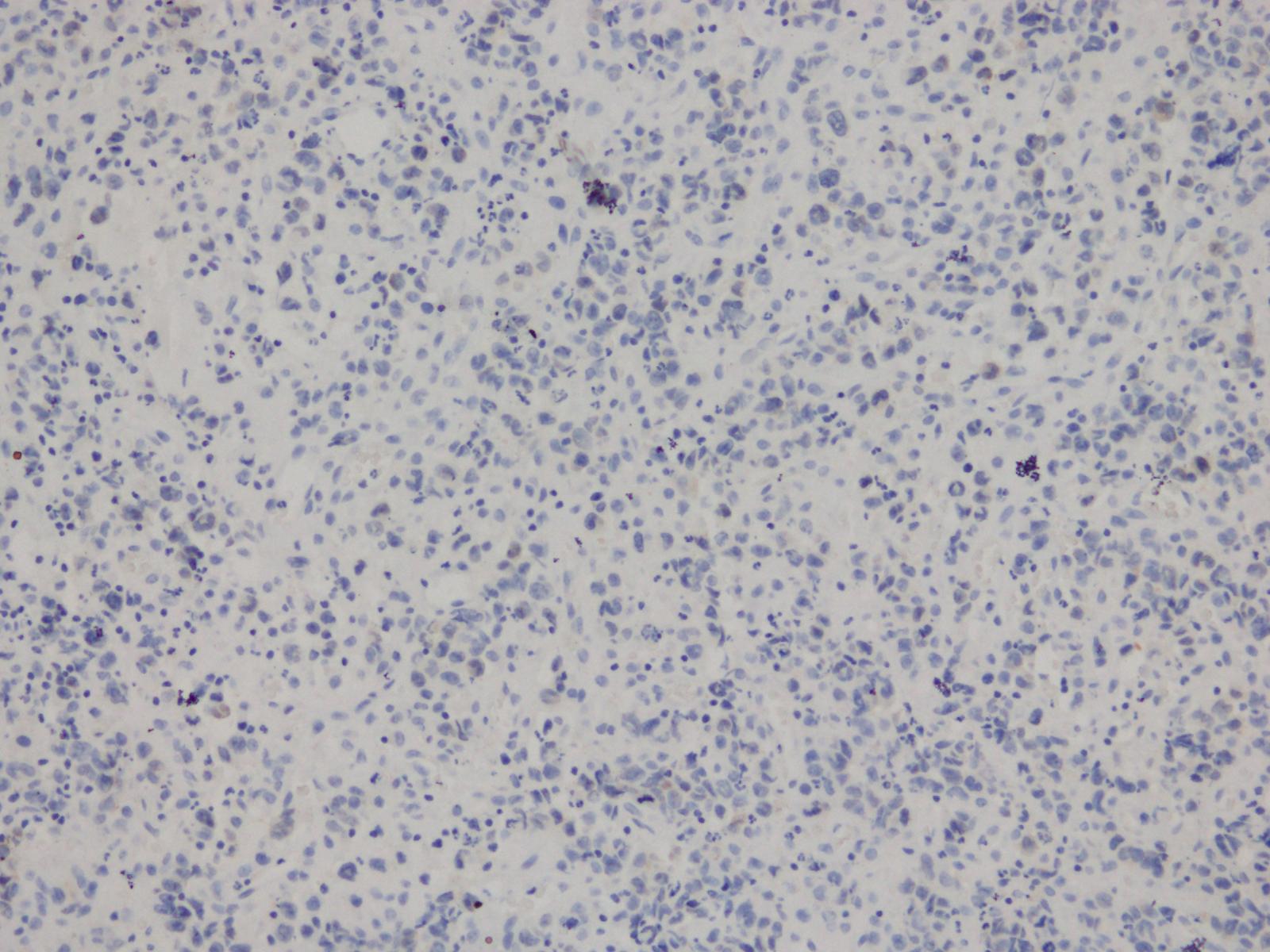
ALK-
CD15-
CD20-
CD5+
Virtual slides
Images hosted on other servers:

ALCL, ALK-, ALK1

ALCL, ALK-, CD30

ALCL, ALK-, H&E

ALCL, ALK+, ALK1

ALCL, ALK+, CD30

ALCL, ALK+, H&E
Cytology description
- Large atypical neoplastic cells, multinucleation / multilobated nuclei, prominent Golgi zone, basophilic cytoplasm
- Basophilic nucleoli, generally less prominent than seen in Hodgkin Reed-Sternberg cells
Cytology images
Contributed by Jayalakshmi Balakrishna, M.D.
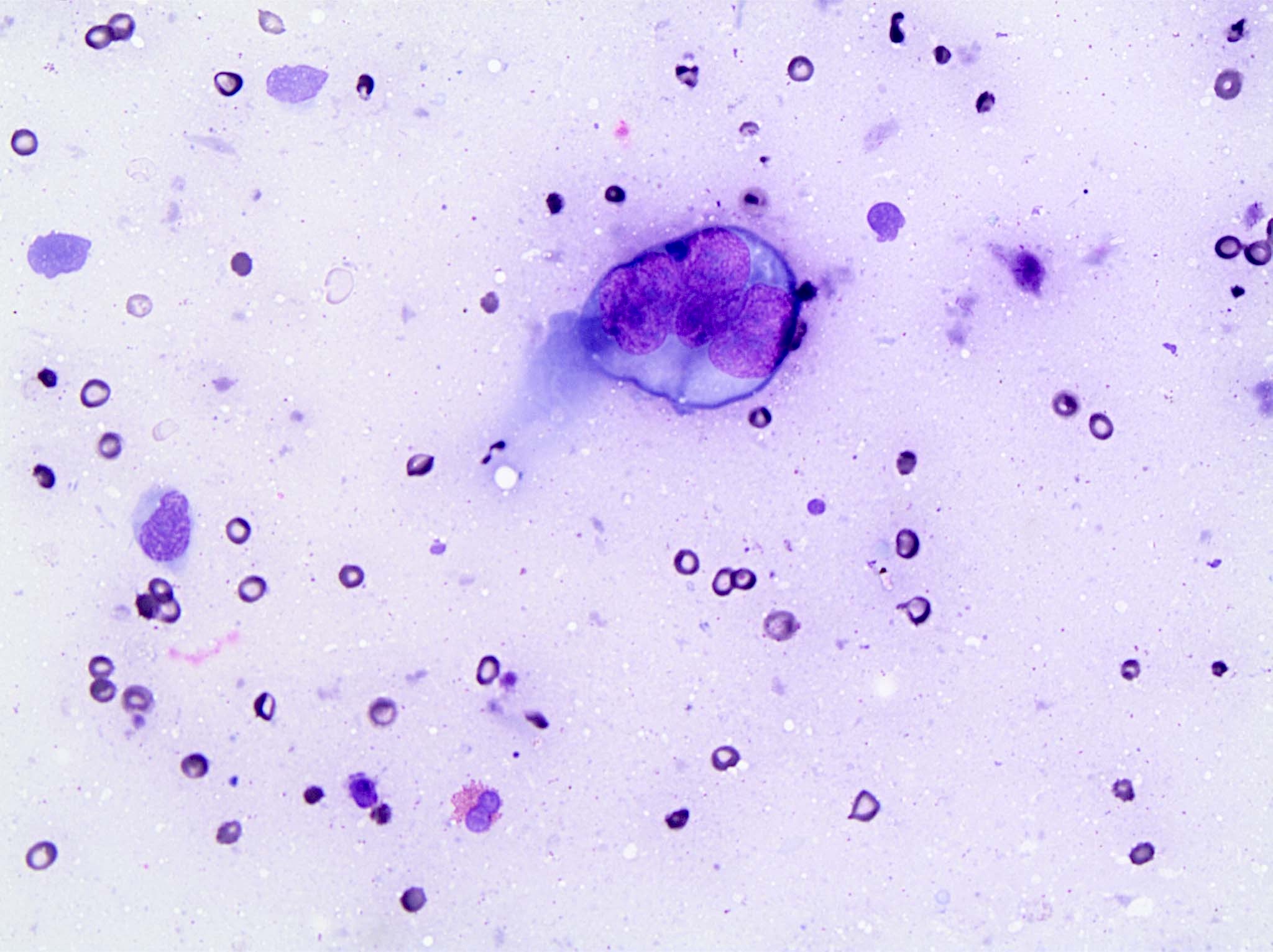
Lymph node biopsy touch preparation
Positive stains
- Strong and diffuse uniform CD30 staining in all tumor cells (membrane and Golgi zone pattern, also cytoplasmic)
- Variable expression / loss of pan-T cell antigens: CD2+ and CD3+ more often than CD5+
- Almost always CD43+ and CD45+; can be used to distinguish from carcinoma
- Often CD4+, rarely CD8+
- TIA1, granzyme B, perforin, clusterin, fascin, EMA (variable)
- Cases with DUSP22 rearrangements tend to be less frequently positive for cytotoxic markers
Negative stains
Flow cytometry description
- Flow cytometry shows the anaplastic large cell lymphoma cells with high forward and side light scatter properties (consistent with large and complex cells) and high density CD45 expression simulating monocytes
- Tumor cells express CD30 and one or more of the T cell associated antigens (Arch Pathol Lab Med 2009;133:49)
Flow cytometry images
Contributed by Sanam Loghavi, M.D.

CD45 and side light scatter
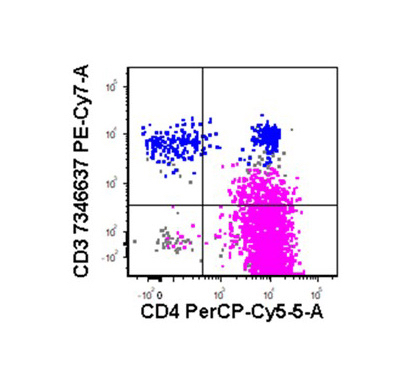
CD3 and CD4

CD4 and CD8
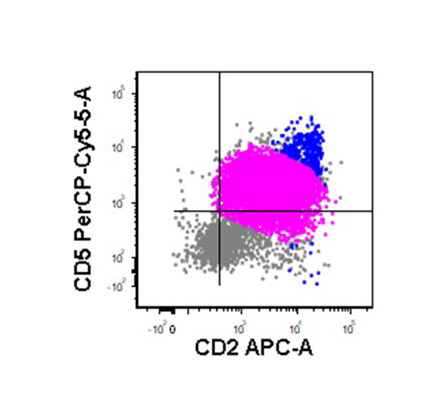
CD5 and CD2
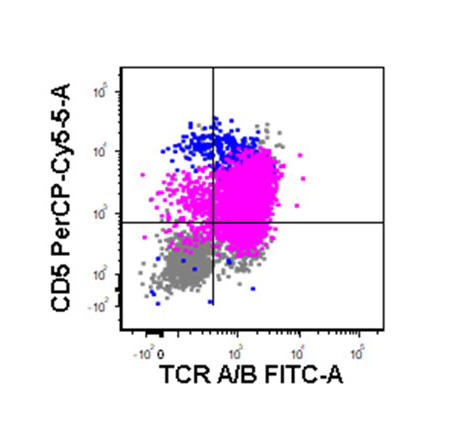
TCR A / B

CD3 and CD30
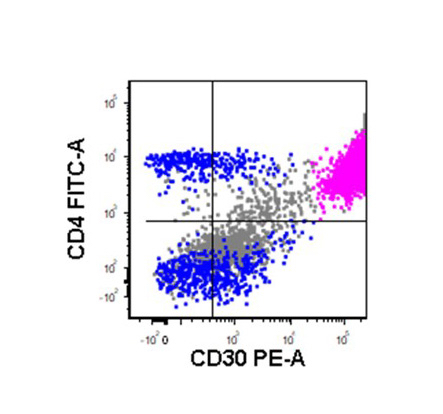
CD4 and CD30
Molecular / cytogenetics description
- T cell receptor (TCR) clonal gene rearrangement in most cases, irrespective of T cell antigen expression
- DUSP22::IRF4 locus on 6p25.3 (referred to as DUSP22 rearrangements); t(6;7)(p25.3;q32.3) (Blood 2011;117:915)
- Recurrent rearrangement involving the TP63 gene in a minority of cases (Blood 2012;120:2280)
- Gains of the 1q41-qter and 6p21 are common cytogenetic aberrations (Br J Haematol 2008;140:516)
- ERBB4 and COL29A1 are expressed in 24% of ALK- ALCL, mutually exclusive with TP63 rearrangement (Blood 2016;127:221)
- STAT3 activating mutations in a subset of cases (Cancer Cell 2015;27:516)
Molecular / cytogenetics images
Contributed by Andrew Feldman, M.D.
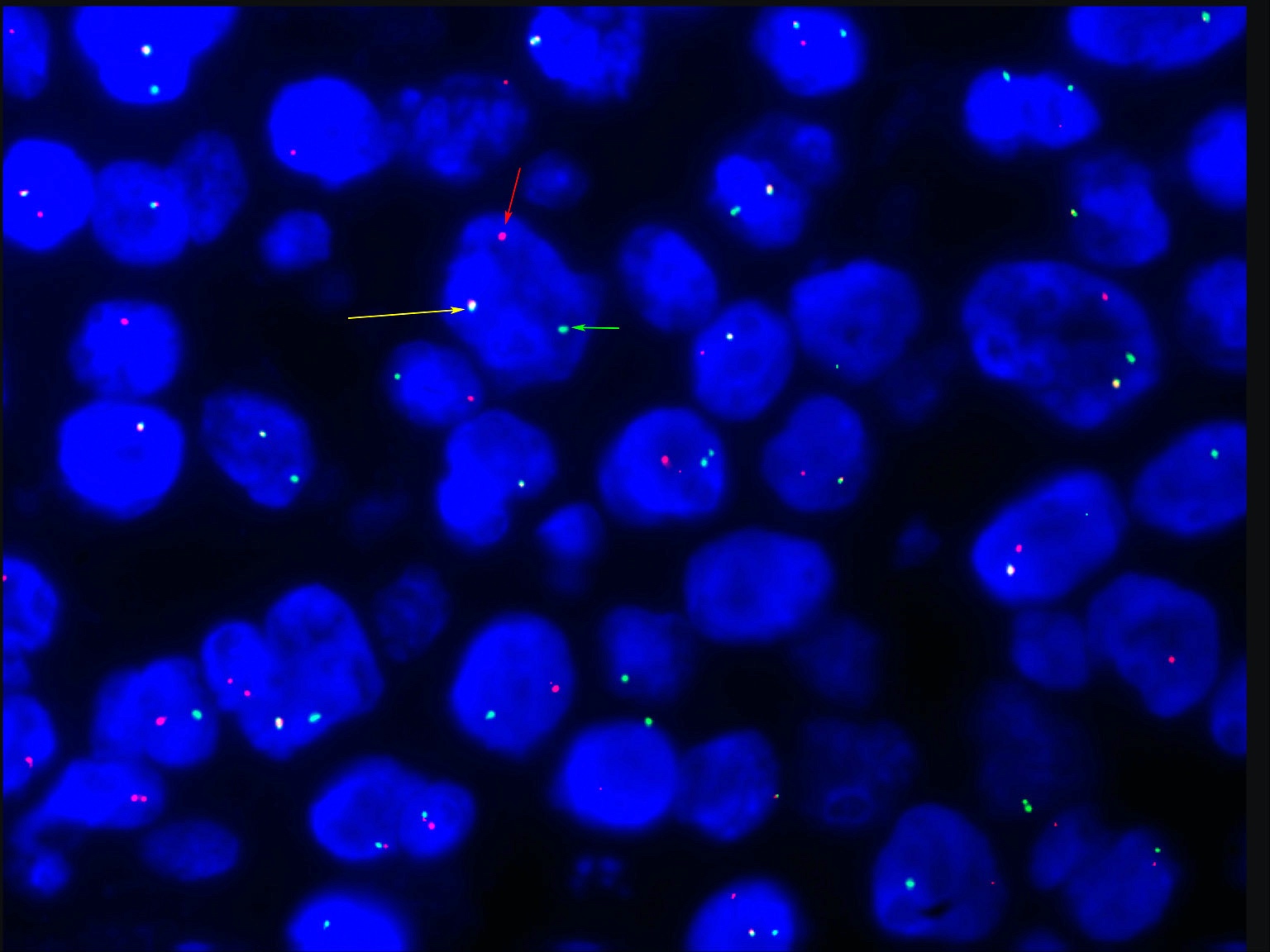
Break apart probe FISH for chromosome region 6p25.3
Sample pathology report
- Mass, left breast, excision:
- Anaplastic large cell lymphoma, ALK negative (see synoptic report)
Differential diagnosis
- ALCL, ALK positive:
- ALK+, younger age, less aggressive
- Classical Hodgkin lymphoma:
- Peripheral T cell lymphoma, NOS:
- Difficult differential, WHO recommends conservative approach (diagnose ALCL, ALK- only if very similar to ALCL, ALK+, except for ALK expression)
- Overall worse prognosis than ALCL, ALK-
- Primary cutaneous ALCL:
- Gene expression profiling shows that ALCL, ALK negative is closely related to primary cutaneous ALCL
- Much better prognosis, clinical correlation with staging necessary
- Breast implant associated ALCL:
- Breast implants, typically textured
- Triple negative genetic subtype
- Typically ALK- also
- Mycosis fungoides with CD30 expression:
- Presents as cutaneous patches and can progress to plaques, tumors and erythroderma
- Band-like papillary dermal lymphoid infiltrate
- Intraepidermal lymphocytes out of proportion with spongiosis (epidermotropism) with or without Pautrier microabscesses
Additional references
Board review style question #1
What is the morphologic characteristic of anaplastic large cell lymphoma, ALK negative with DUSP22-IRF4 rearrangement?
- Eosinophilia
- Hodgkin-like cells
- Prominent nucleoli and intranuclear inclusions (doughnut cells)
- Small cell morphology
Board review style answer #1
C. Prominent nucleoli and intranuclear inclusions (doughnut cells)
Comment Here
Reference: Anaplastic large cell lymphoma, ALK negative
Comment Here
Reference: Anaplastic large cell lymphoma, ALK negative
Board review style question #2
What is a prognostic factor in anaplastic large cell lymphoma, ALK negative?
- Age of the patient
- Gender of the patient
- Mitotic count
- Tumor necrosis
Board review style answer #2
