
Lymphoma & related disorders
Mature B cell neoplasms
Large B cell lymphomas-special subtypes
ALK+ LBCL
Editorial Board Member: Patricia Tsang, M.D., M.B.A.
Deputy Editor-in-Chief: Genevieve M. Crane, M.D., Ph.D.


Last author update: 21 December 2020
Last staff update: 23 August 2022
Copyright: 2001-2024, PathologyOutlines.com, Inc.
PubMed Search: ALK positive OR ALK+ large B cell lymphoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Dcunha NJ, Manipadam MT. ALK+ LBCL. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lymphomaALKpositive.html. Accessed April 18th, 2024.
Definition / general
- WHO defines this entity as an aggressive lymphoma composed of ALK (anaplastic lymphoma kinase) positive monomorphic large immunoblast-like B cells, which usually have a plasma cell phenotype (Blood 2016;127:2375, Swerdlow: WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th Edition, 2017)
- Lymphoma composed of large lymphoid cells of B lineage, positive for ALK immunohistochemical stain and negative for CD20 and CD30
Essential features
- Aggressive B cell lymphoma with monomorphic large immunoblast / plasmablast-like B cells, usually having plasma cell phenotype
- Positive for ALK immunohistochemistry with granular cytoplasmic restriction and negative for CD20 and CD30
- ALK gene is translocated and activated; most frequent cytogenetic abnormality is t(2;17) responsible for CLTC (clathrin)-ALK fusion protein
Terminology
- Large B cell lymphoma expressing ALK kinase and lacking t(2;5) translocation (obsolete)
- ALK positive plasmablastic B cell lymphoma (obsolete)
ICD coding
- ICD-O: 9737/3 - ALK positive large B cell lymphoma
Epidemiology
- It is a very rare lymphoma
- Occurs in immunocompetent, HIV negative young men, although reported in a wide age range and both genders
- M:F = 5:1
- Age range of 9 - 85 years; median age of 43 years (J Clin Oncol 2009;27:4211)
Sites
- Common sites include lymph nodes and mediastinum
- Other rare sites include nasopharynx, tongue, stomach, duodenum, bone, soft tissue, liver, spleen and skin (Hum Pathol 2004;35:1285, Exp Ther Med 2014;8:409, Am J Dermatopathol 2019;41:602)
Pathophysiology
- Translocation of ALK gene on chromosome 2 with a fusion gene partner
- ALK oncogenic protein overexpression and related activation of STAT3 pathway
- MYC expression in the absence of MYC translocations or amplifications, probably due to transcriptional activation downstream of STAT3 (Mod Pathol 2013;26:1329)
- No known association with immunosuppression
Etiology
- Not specified
- Normal counterpart: a postgerminal center B cell with plasmablastic differentiation
Clinical features
- Most patients present with generalized lymphadenopathy
- 60% of cases present in advanced stage (III / IV) and bone marrow infiltration is seen in 25% of cases (J Clin Oncol 2009;27:4211)
Diagnosis
- Based on a combination of light microscopy and immunohistochemical markers
Prognostic factors
- Generally, this lymphoma has a poor prognosis
- However, factors for a good prognosis include localized disease (stage I and II) and lymphoma occurring in childhood
Case reports
- 28 year old man with right submandibular lymphadenopathy (Int J Clin Exp Pathol 2017;10:11219)
- 50 year old man with mediastinal lymphadenopathy (Pathology 2019;51:S81)
- 54 year old man with right neck mass (Case Rep Hematol 2018;2018:5320590)
Treatment
- Most cases treated with chemotherapy regimens of CHOP or E-POCH / CHOEP; a few patients are also given additional radiotherapy (PLoS One 2017;12:e0178416)
- Since most cases are negative for CD20 and CD30, rituximab and brentuximab vedotin are not given
- There is a single case report of complete response to nivolumab (Clin Lymphoma Myeloma Leuk 2020;20:e113)
Microscopic (histologic) description
- Tumor arranged as diffuse sheets, sinusoidal infiltrate or a mixture of diffuse and sinusoidal patterns
- Tumor composed of monomorphic large immunoblast-like cells containing a large central nucleolus and abundant cytoplasm
- Some cases show plasmablastic differentiation, which can be either an exclusive population of plasmablasts or a spectrum of morphology from plasmacytes to plasmablasts
- Anaplastic / pleomorphic morphology has also been described in a few cases (Am J Surg Pathol 2017;41:25)
- Atypical multinucleated tumor giant cells may be seen (Am J Surg Pathol 2017;41:25)
Microscopic (histologic) images
Contributed by Marie Therese Manipadam, M.B.B.S., M.D.
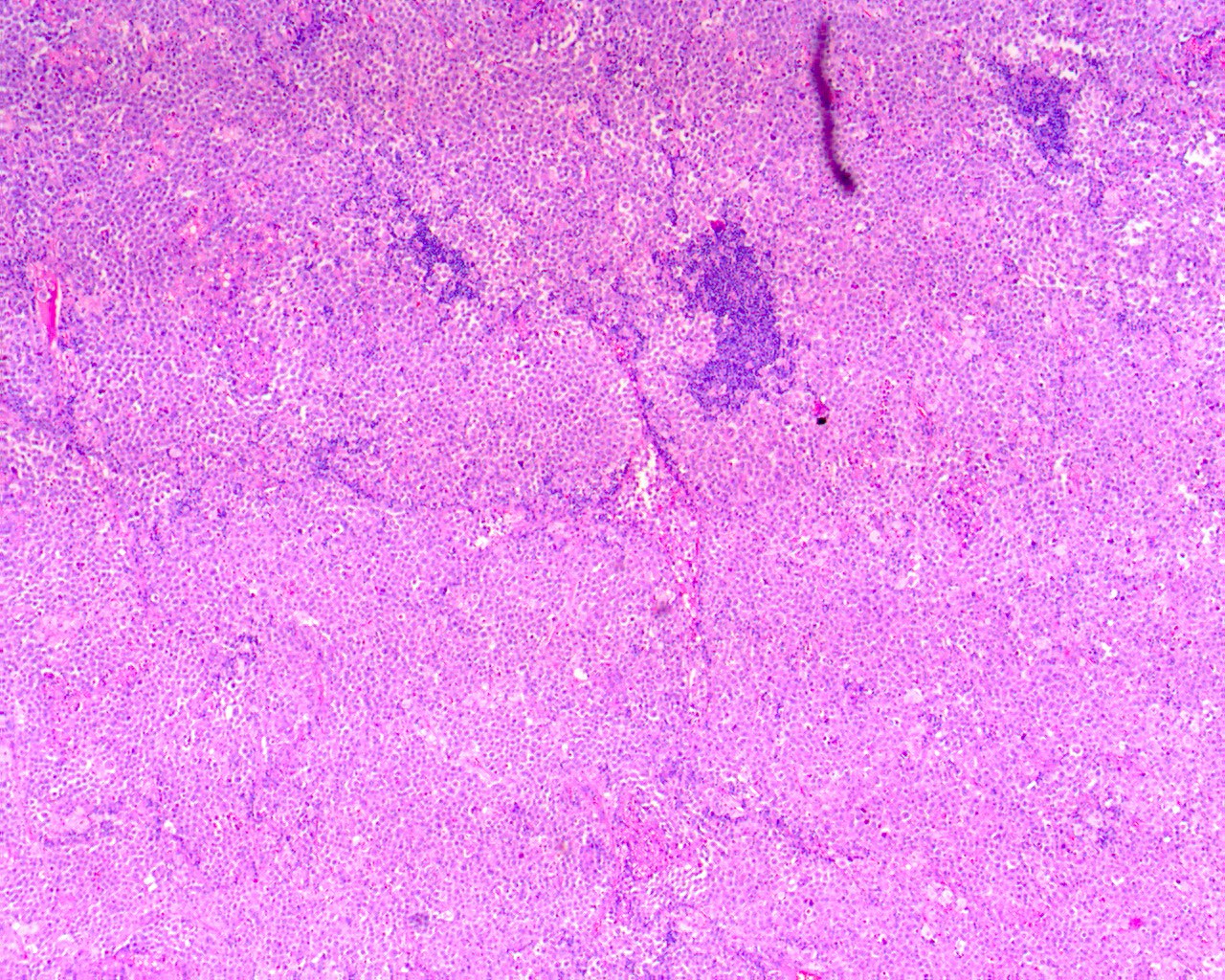
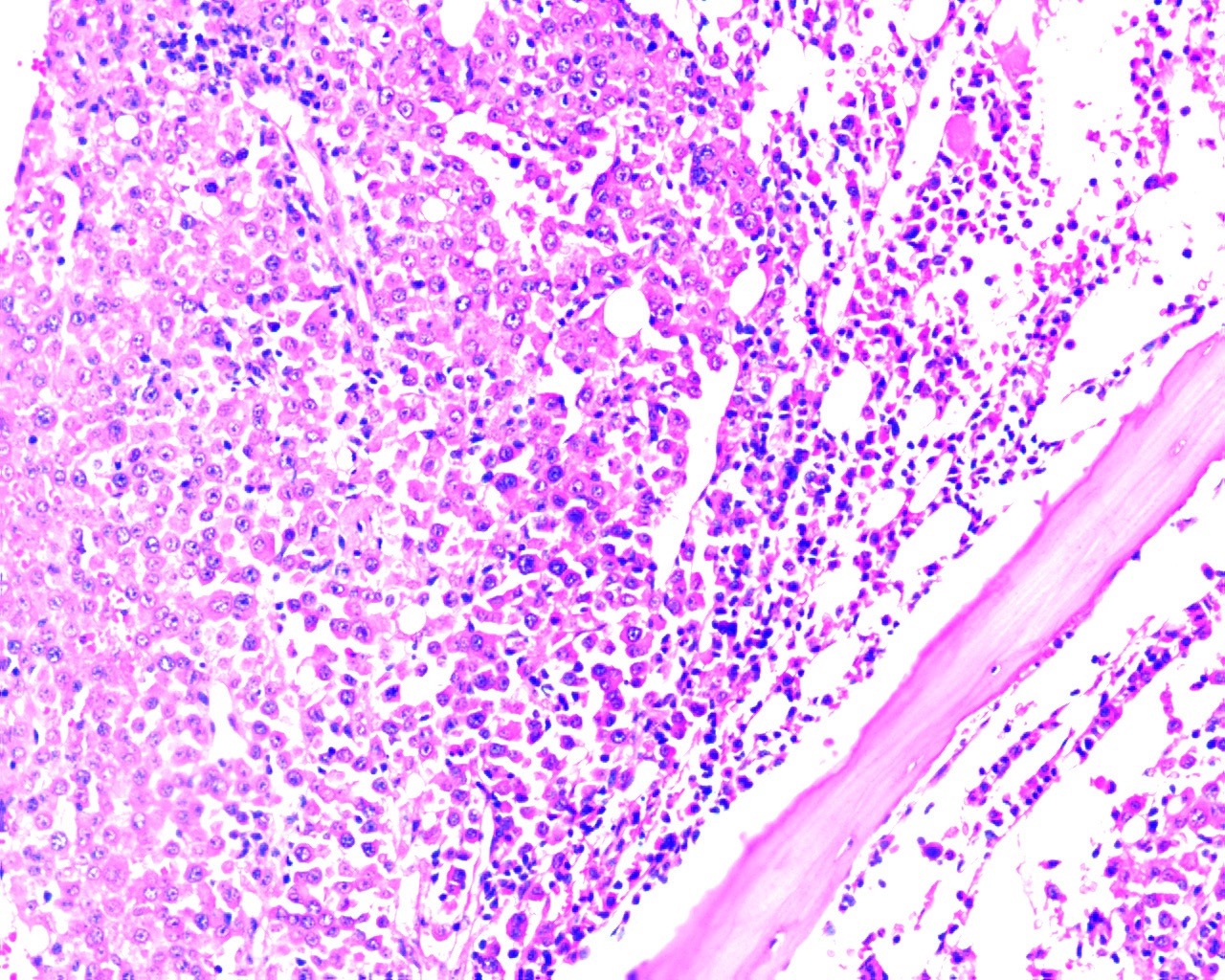
Tumor with diffuse involvement
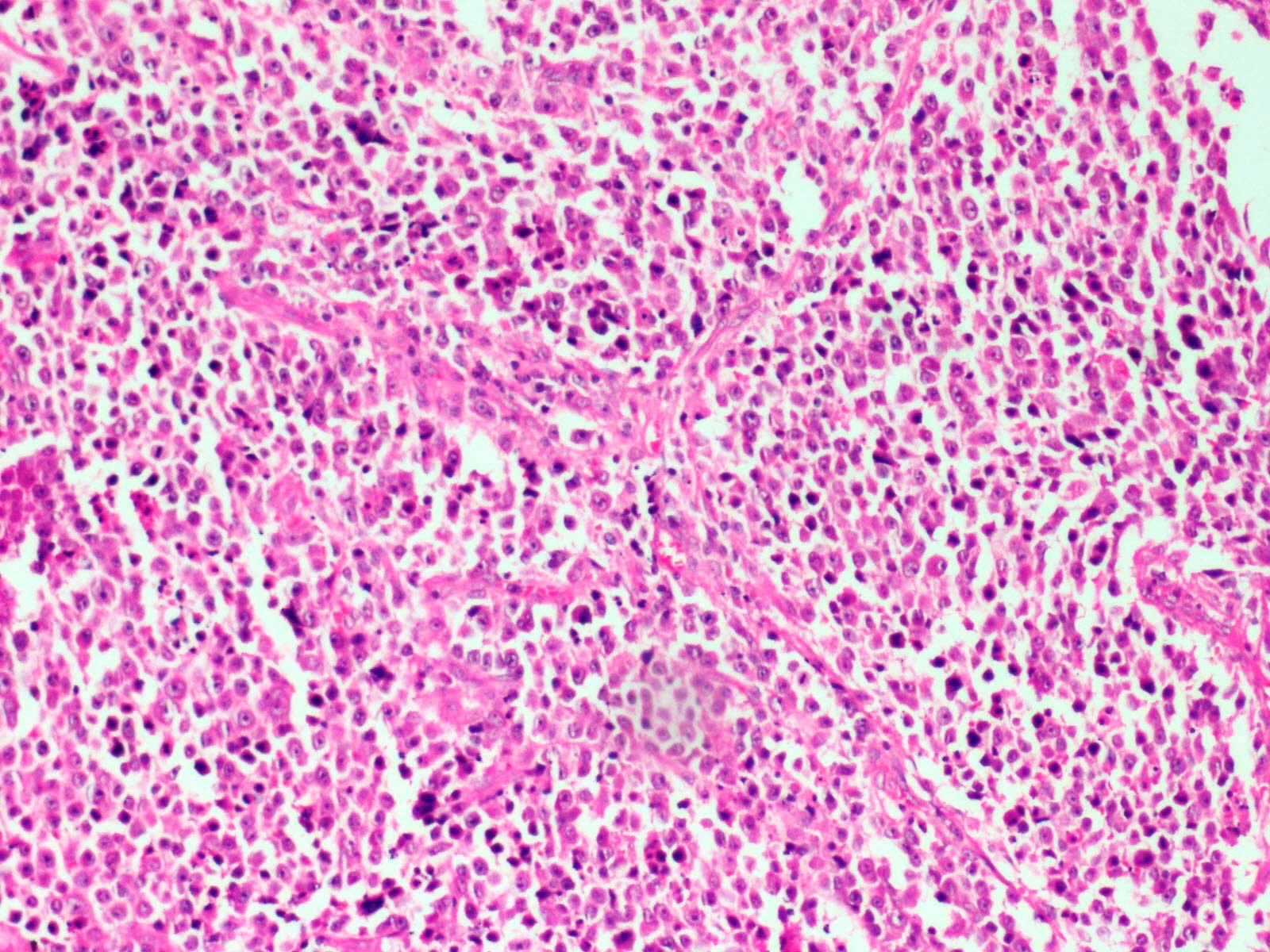
Large lymphoid tumor cells
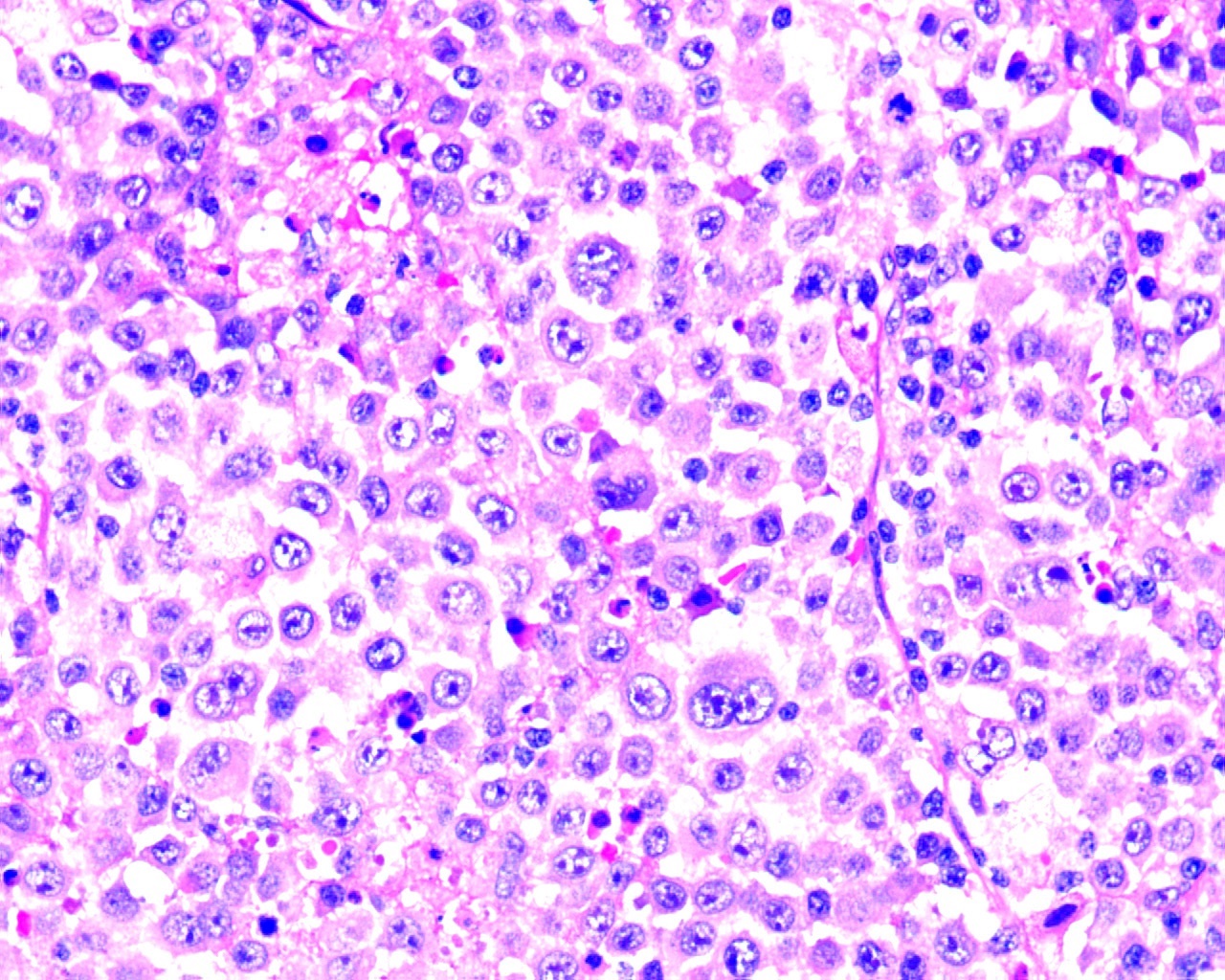
Immunoblast-like
tumor cells and
few plasmablasts
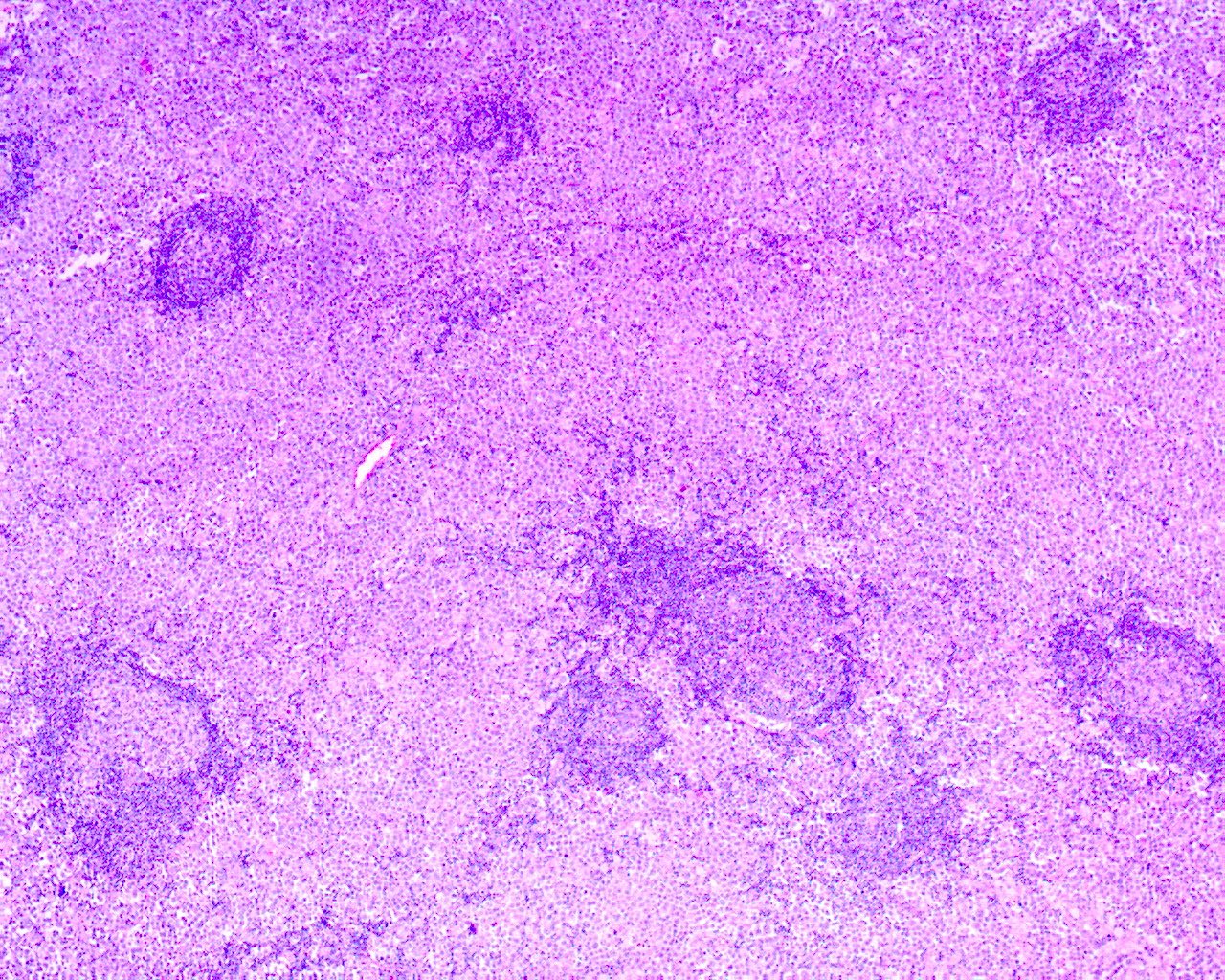
Interfollicular expansion by tumor cells

Intrasinusoidal growth of tumor
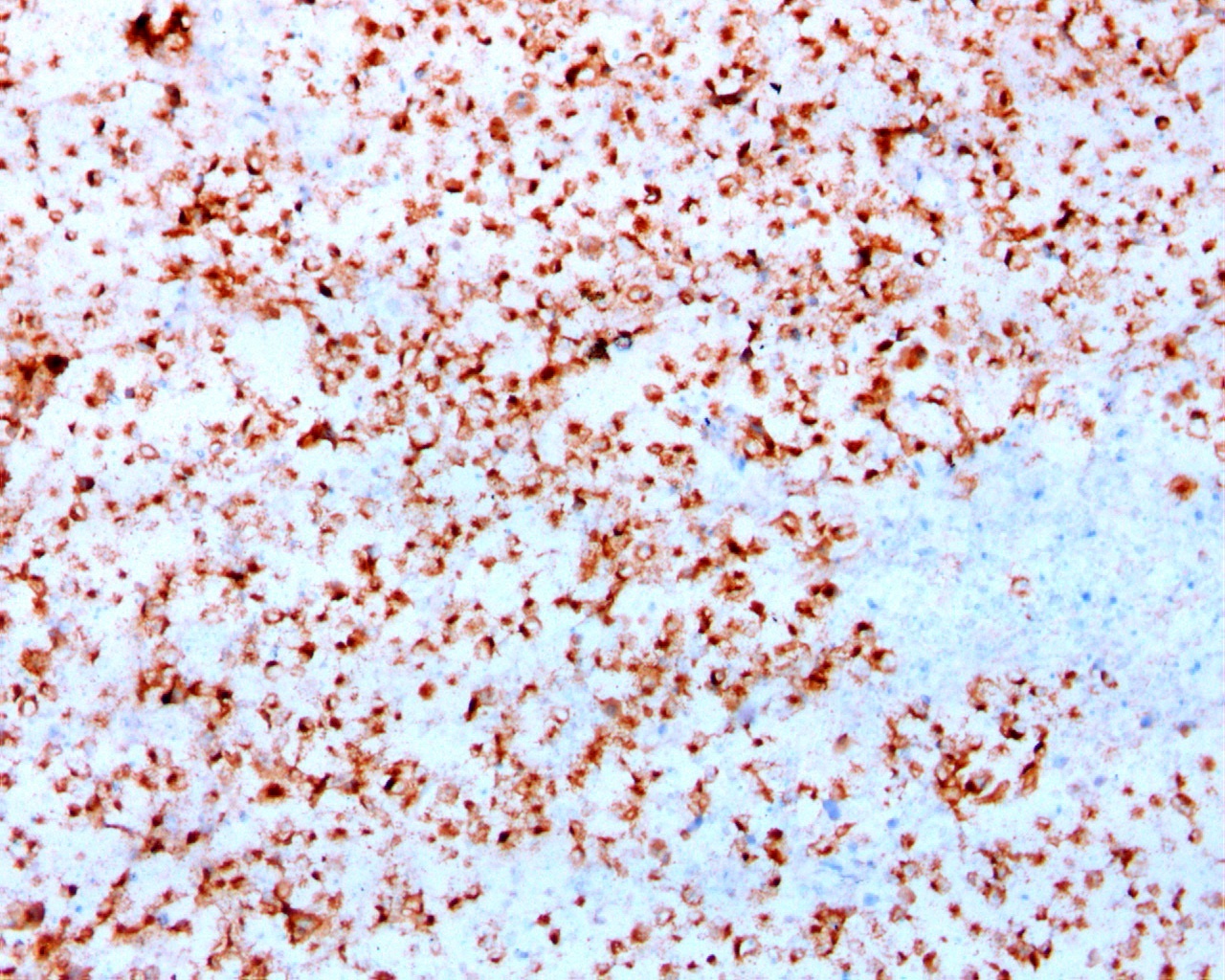
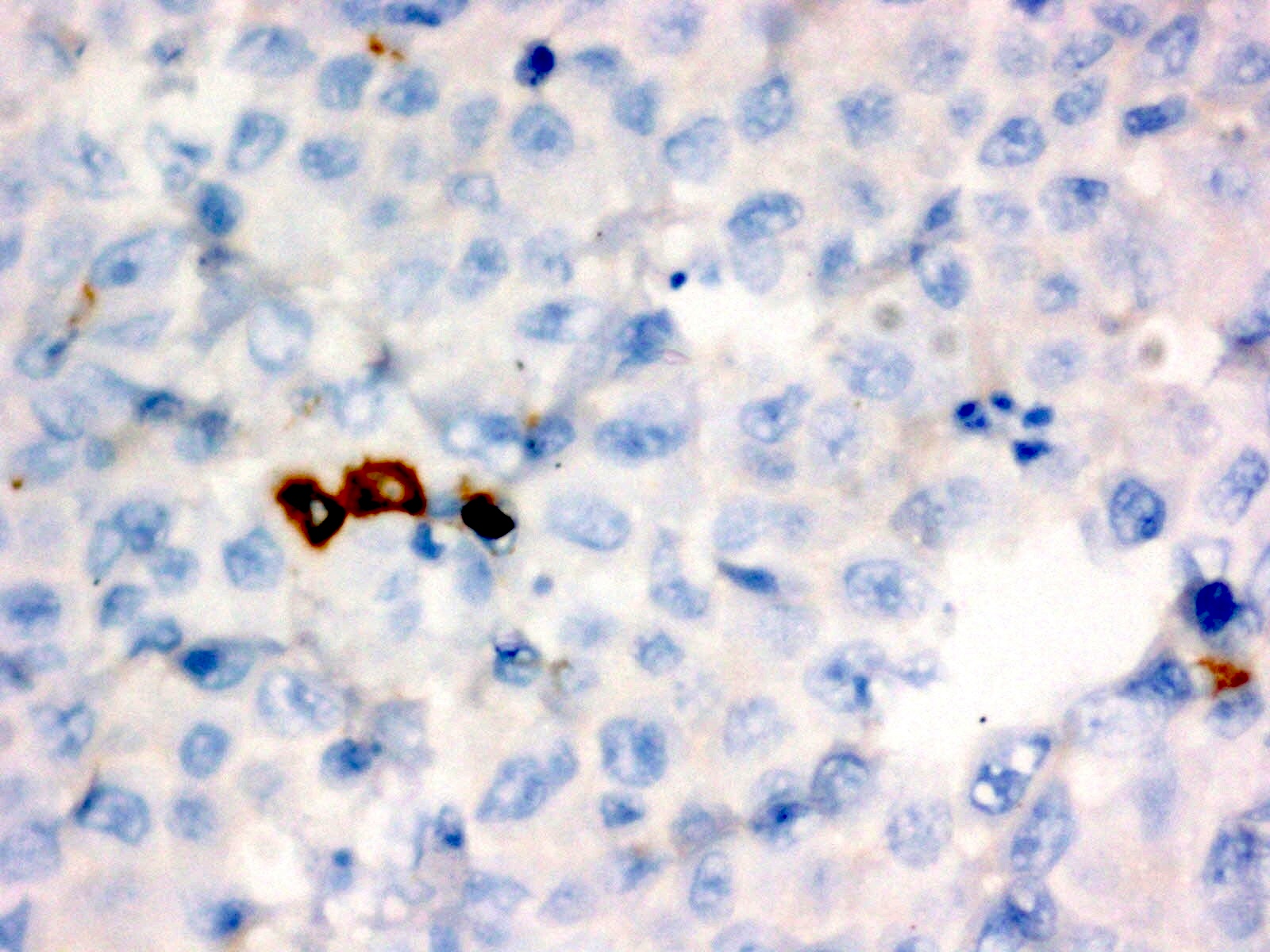
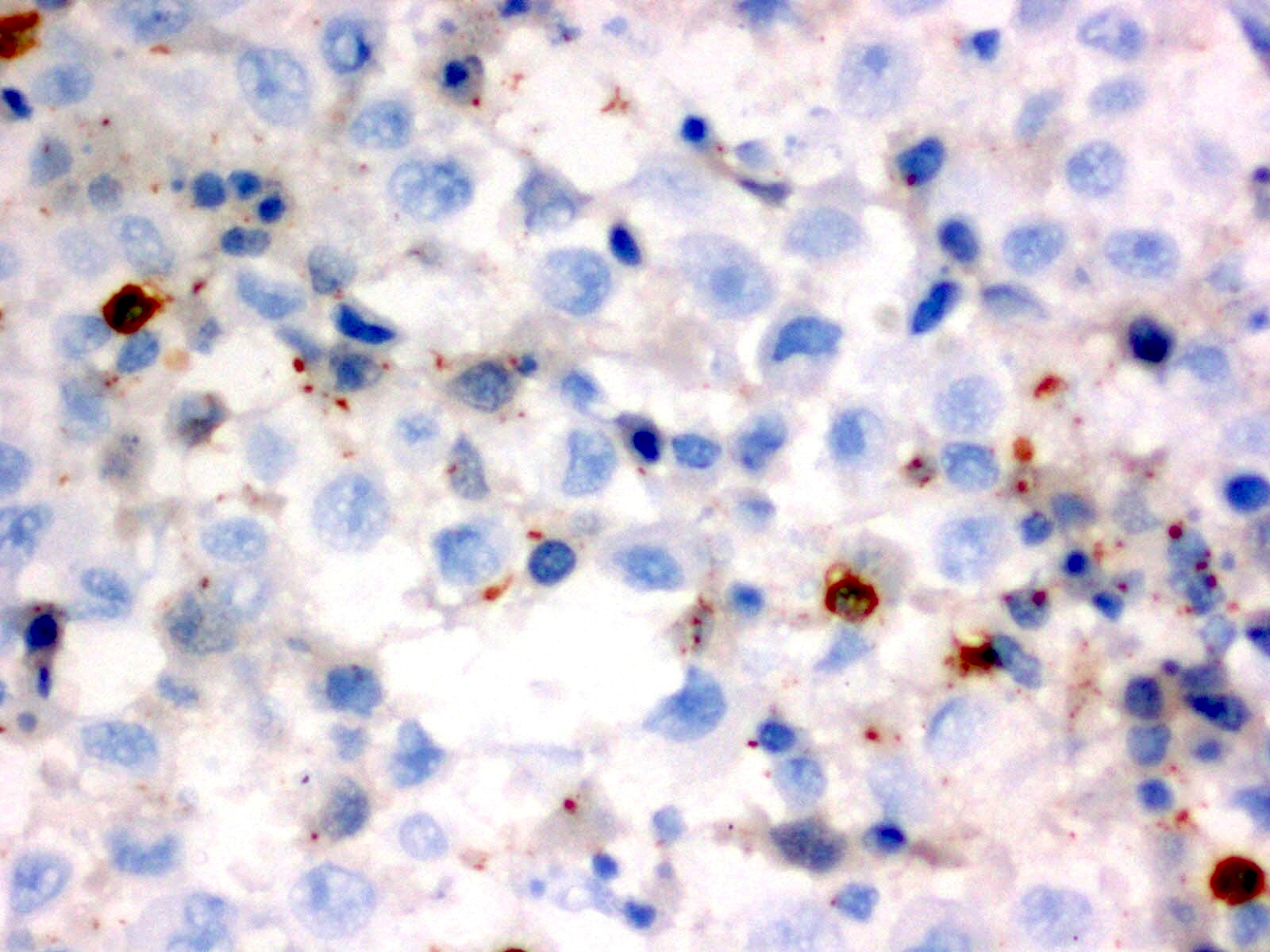
Cytoplasmic granular ALK positivity

MUM1 positivity
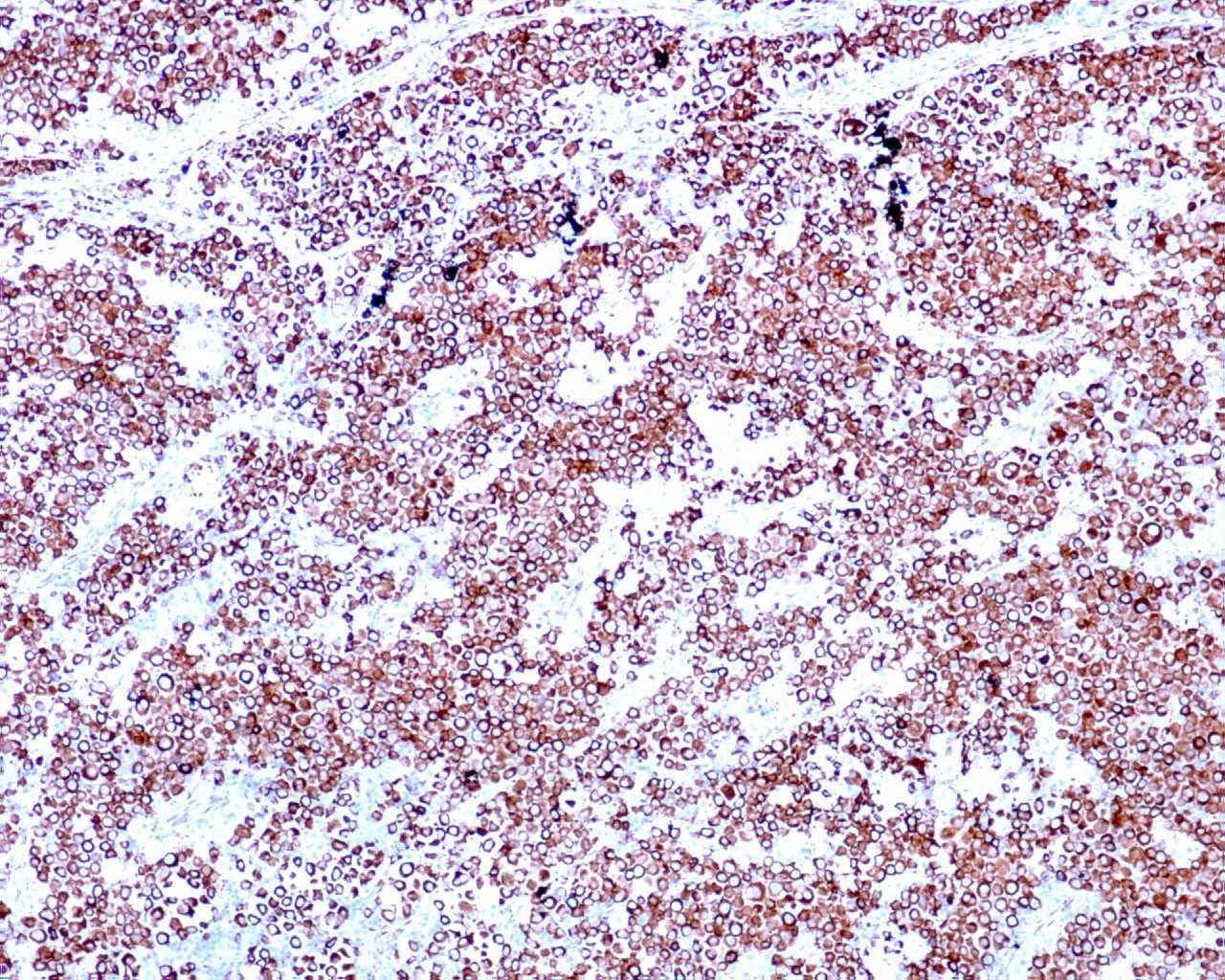
CD138 positivity
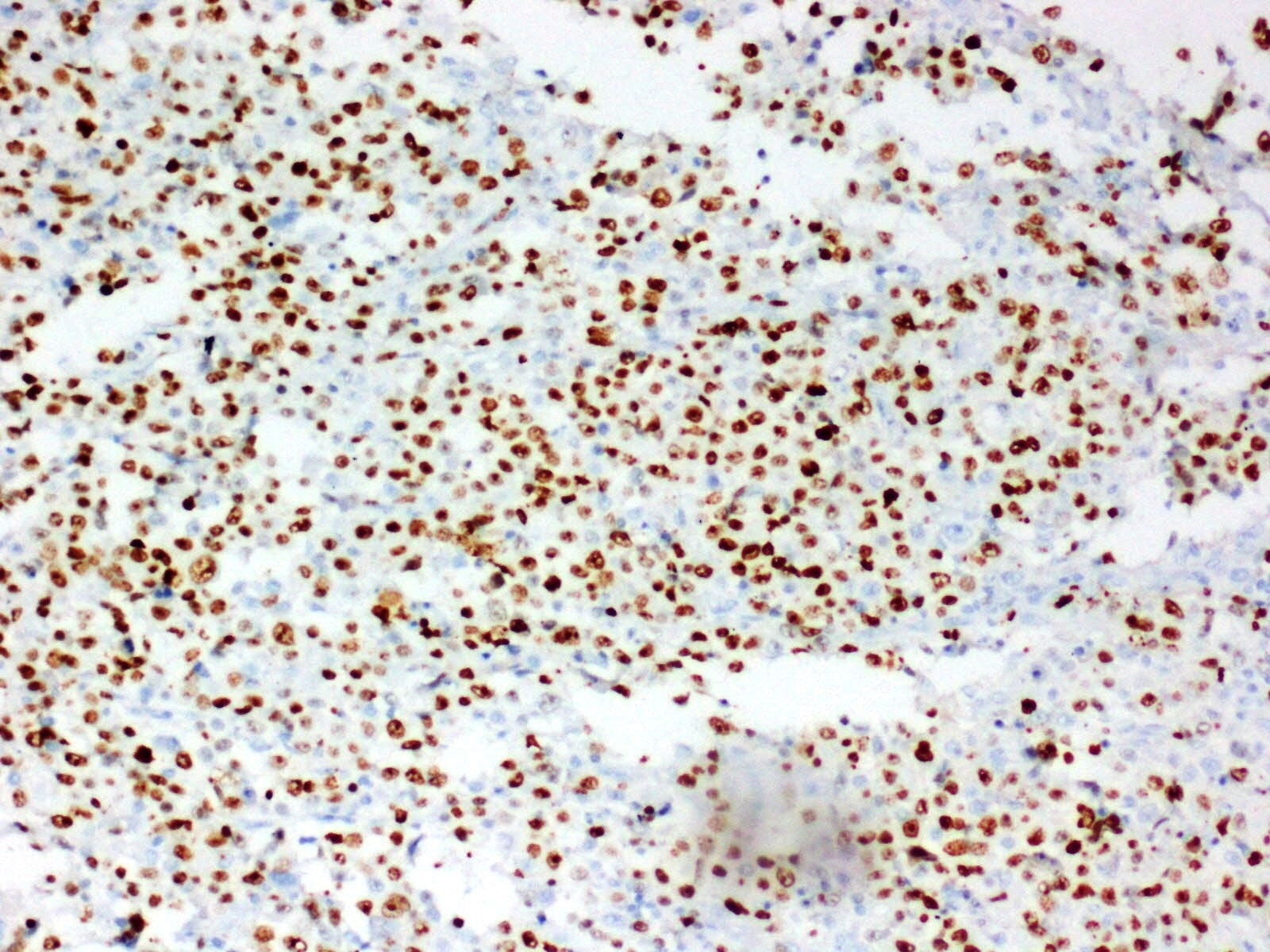
MIB1 index of 80 - 90%
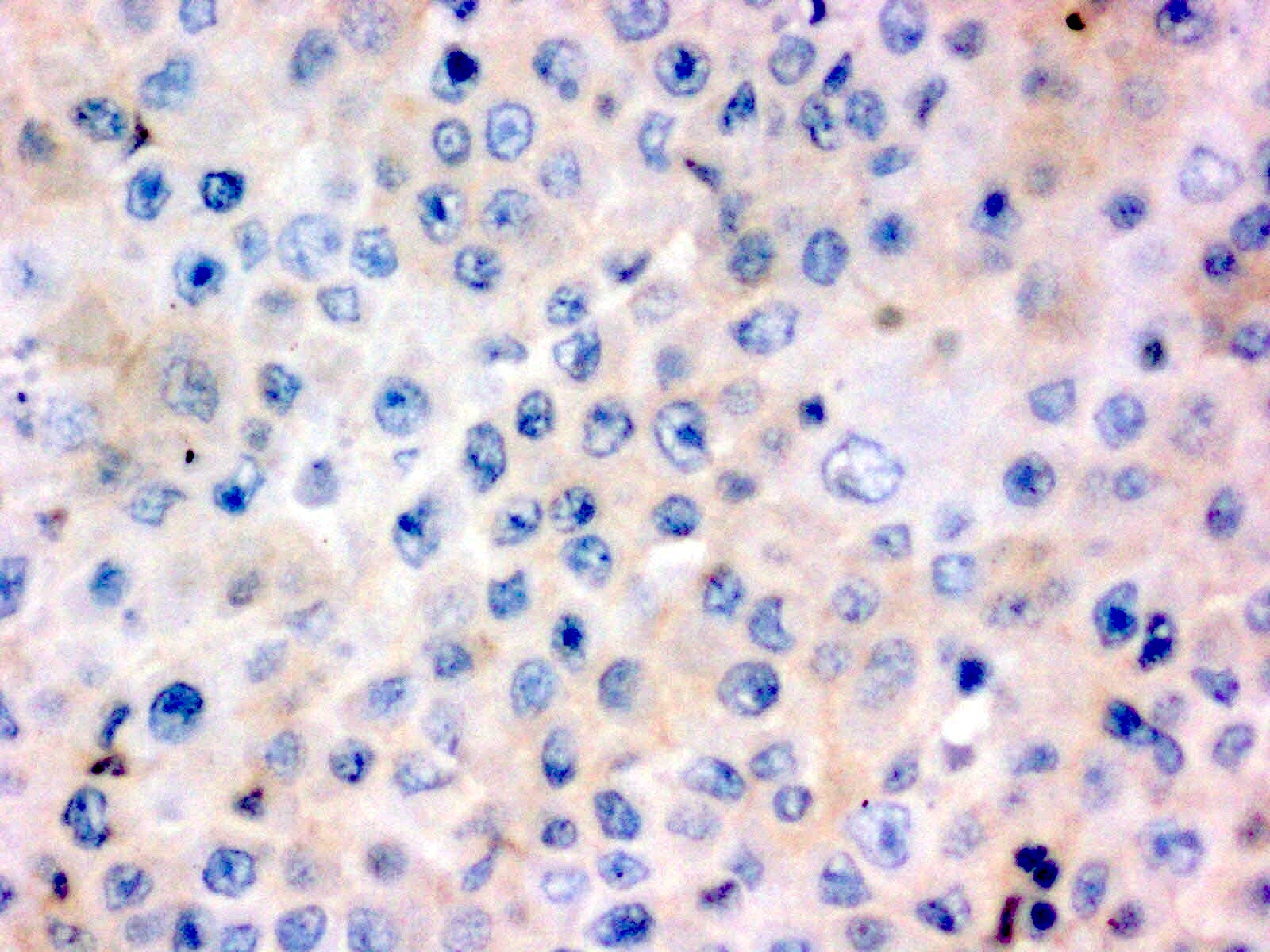
CD30 negativity in tumor cells
CD3 negativity in tumor cells
CD20 negativity in tumor cells
Weak positivity for CD79a
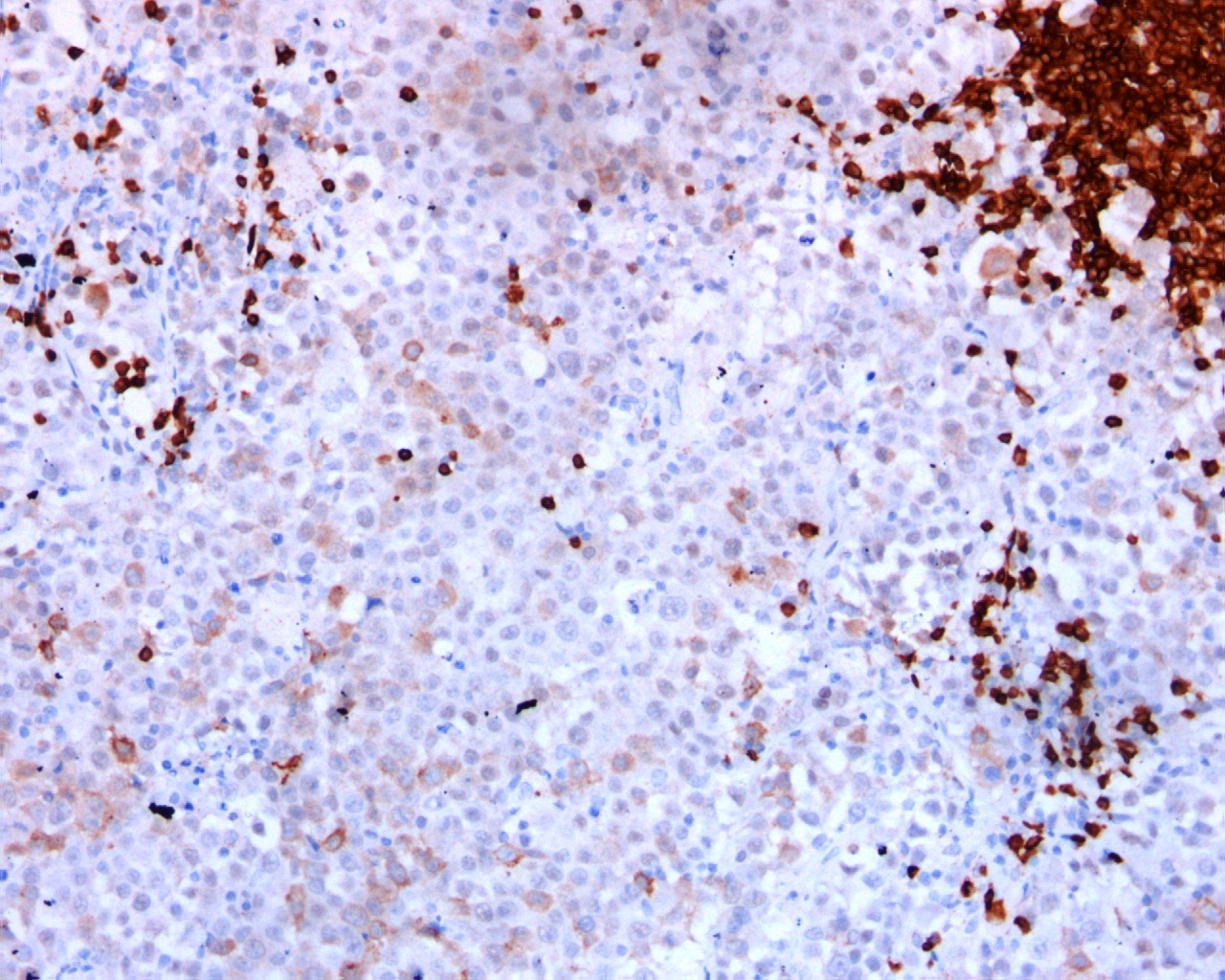
Lymphoma involving bone marrow biopsy
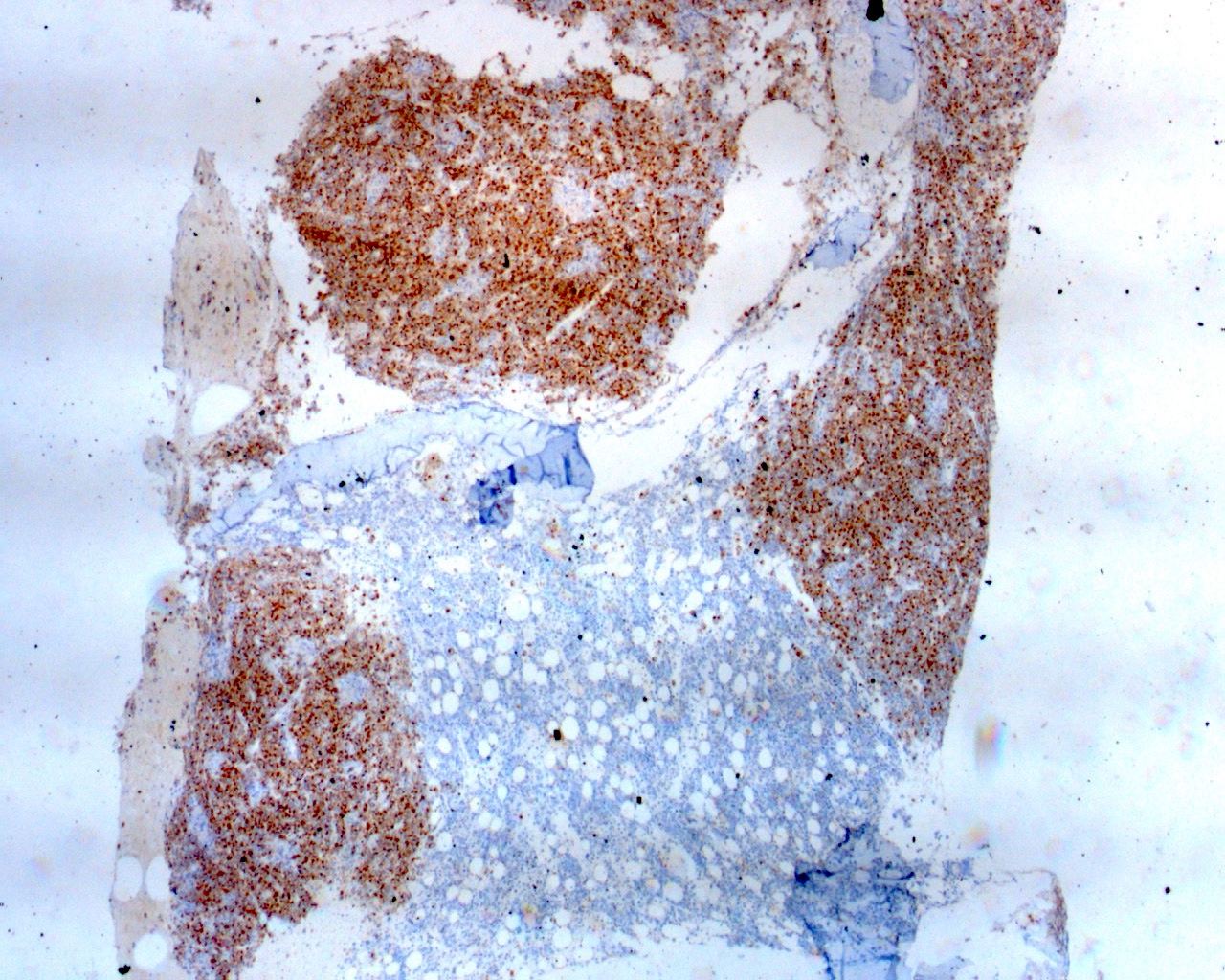
ALK positivity in tumor cells
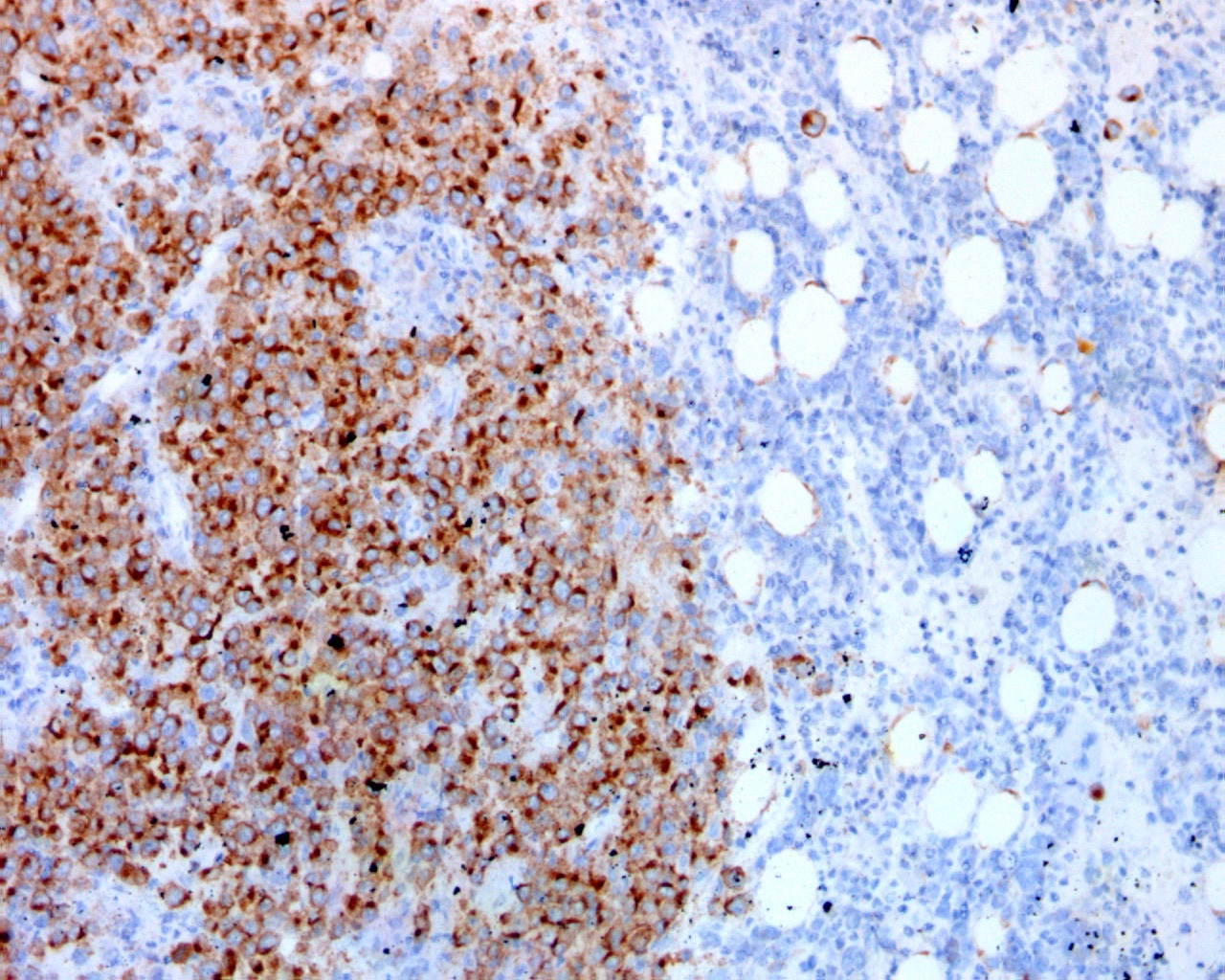
Granular ALK positivity in tumor cells
ALK positive large B cell lymphoma cells
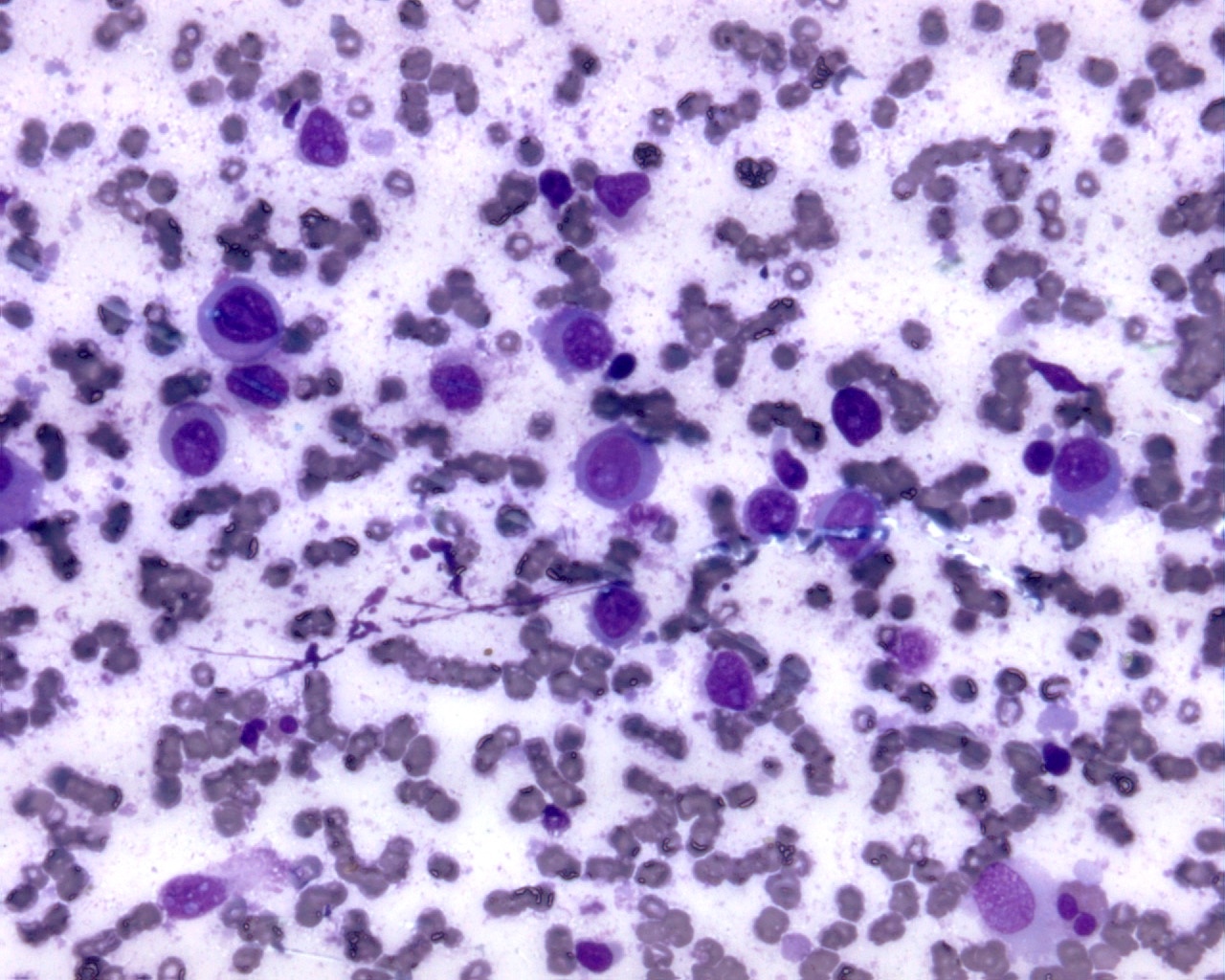
Cytology description
- Only a few case reports are available in the literature and give a brief view of cytological findings
- One case report states, "most of the neoplastic cells had pseudopodial cytoplasmic projections and some of them had eosinophilic pseudopodial cytoplasmic projections that resembled flaming plasma cells" (Int J Clin Exp Pathol 2013;6:2631)
- A second case report states, "aspiration cytology revealed many clusters of cohesive, large and solitary cells that showed abundant cytoplasm and large round to oval nuclei with prominent nucleoli" (Diagn Cytopathol 2014;42:69)
Positive stains
- ALK positivity is important for diagnosis and characteristically demonstrates a restricted granular cytoplasmic staining pattern, highly indicative of the expression of CLTC-ALK fusion protein or ALK-SEC31A translocation
- Other patterns (diffuse cytoplasmic, nuclear or nucleolar) of ALK staining correspond to translocation of ALK with NPM1 [t(2;5)(p23;q35)], SQSTM1, RANBP2 or EML4, which are associated with a poorer prognosis (Int J Hematol 2016;103:399)
- EMA (73%), CD138 (96%), PRDM1 (BLIMP1), MUM1 / IRF4 (100%), CD45 (96%), IgA (67%), BOB1 (100%), OCT2 (81%), PAX5 (28%) and CD79a (30%)
- Tumor may be positive for CD4 (67%), CD57, CD43 and perforin
- 83% of cases showed kappa or lambda light chain restriction by immunohistochemistry or in situ hybridization (Am J Surg Pathol 2017;41:25)
Negative stains
Molecular / cytogenetics description
- Clonal rearrangement of IG genes
- ALK is overexpressed due to fusion proteins generated by translocations
- Most common translocation is t(2;17)(p23;q23), responsible for CLTC (clathrin)-ALK fusion protein
- Few cases are associated with t(2;5) (Blood 2003;102:2642)
- ALK may have other fusion partners (given above)
Sample pathology report
- Right cervical lymph node, excisional biopsy:
- ALK positive large B cell lymphoma (see comment)
- Comment: Tumor cells are positive for ALK (cytoplasmic granular staining) and MUM1 with high MIB1 proliferation index. Tumor cells are negative for CD3, CD20, CD30, CD45, EBV-LMP1 and LANA. Few cells show weak positivity for CD79a.
- Microscopic description: Section studied shows completely effaced lymph node architecture with diffuse infiltration by a tumor arranged in sheets and composed of monomorphic large immunoblast-like cells containing a round to oval nucleus, vesicular chromatin, large central nucleolus and abundant cytoplasm. Few cells show plasmablast-like morphology. An intrasinusoidal pattern is seen focally.
Differential diagnosis
- ALK positive anaplastic large cell lymphoma:
- Plasmablastic lymphoma:
- Tumor is EBV positive (EBER) and ALK and HHV8 (LANA) negative
- Primary effusion lymphoma:
- Tumor is positive for HHV8 (LANA) and EBV (EBER) and negative for ALK
- HHV8 positive diffuse large B cell lymphoma:
- Tumor is positive for HHV8 (LANA) and EBV (EBER) and negative for ALK and MUM1 / IRF4
- Intravascular large B cell lymphoma:
- Extraosseous plasma cell neoplasm in case of extranodal ALK positive large B cell lymphoma:
- This entity will be ALK negative
- Metastatic carcinoma:
- May be considered because of the sinusoidal distribution, EMA positivity and cytokeratin positivity in rare cases of ALK positive large B cell lymphoma
Additional references
Board review style question #1
Which of the following combinations of IHC markers is diagnostic of ALK positive large B cell lymphoma that comprises monomorphic large lymphoid cells?
- ALK positive, MUM1 positive and CD30 positive
- ALK positive, MUM1 positive and CD30 negative
- ALK positive, MUM1 negative and CD30 positive
- ALK positive, MUM1 negative and CD30 negative
Board review style answer #1
Board review style question #2
What is the most common pattern of ALK IHC positivity in ALK positive large B cell lymphoma?
- Granular cytoplasmic positivity
- Nuclear positivity
- Nuclear and cytoplasmic positivity
- Membranous positivity
Board review style answer #2
