Lung
Papillomas and adenomas
Sclerosing pneumocytoma
Last staff update: 17 March 2025 (update in progress)
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Sclerosing pneumocytoma lung



Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Frozen section description | Frozen section images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Cima L, Lin S, Cecchini MJ. Sclerosing pneumocytoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lungtumorsclerosingheman.html. Accessed March 29th, 2025.
Definition / general
- Pulmonary pneumocytoma are indolent tumors with a characteristic dual population of cuboidal surface cells resembling type II pneumocytes and stromal round cells
- Displays varying amounts of hemangiomatous, papillary, sclerotic and solid histologic patterns
Essential features
- First described by Liebow and Hubbell in 1956 as sclerosing hemangioma (Cancer 1956;9:53)
- Renamed pulmonary sclerosing pneumocytoma and categorized into adenoma in WHO 4th edition
- Characteristic bland cytologic features with multiple growth patterns and a dual cell population of surface and round cells that can be highlighted by immunohistochemistry
- Difficult to establish diagnosis on small biopsies, cytology or frozen sections and permanent sections are preferred
Terminology
- Obsolete term (not recommended): pulmonary sclerosing hemangioma
ICD coding
- ICD-O: 8832/0 - sclerosing pneumocytoma
- ICD-11: 2F0Z & XH7436 - benign neoplasms of respiratory and intrathoracic organs, unspecified & sclerosing pneumocytoma
Epidemiology
- Most frequent
- F > M (3.5:1)
- Wide age range, incidence higher in middle age (mean: 46 years) (Am J Surg Pathol 2000;24:906)
- Predilection for Eastern Asian population; rare among individuals of European descent
- Generally in never smokers (World J Surg Oncol 2022;20:140)
Sites
- Typically solitary and peripheral masses, in lower lobes of lung
- Rarely multifocal endobronchial masses or localized in hilum, visceral pleura or mediastinum
Pathophysiology
- Round and surface cells have been demonstrated to be clonal (Mod Pathol 2007;20:1208)
- Alterations in AKT1 are present in most cases (Proc Natl Acad Sci U S A 2016;113:10672)
Etiology
- Tumor is likely derived from primitive respiratory epithelium (Am J Surg Pathol 2000;24:906, J Clin Pathol 2020;73:531)
- Exact underlying mechanism is unknown
Clinical features
- Typically asymptomatic and incidental findings by routine radiological CT / Xray scans
- Patients can present with symptoms based on localization and tumor size
- Nonspecific respiratory symptoms: cough, sputum, hemoptysis and chest pain
- Cases with lymph node metastasis have been reported, however, this does not adversely affect prognosis (Arch Pathol Lab Med 2003;127:321)
Diagnosis
- Histological diagnosis supported by clinical and radiological CT / Xray findings and corresponding ancillary immunohistochemical testing
- Preoperative diagnosis: solitary pulmonary nodule, challenging histological diagnosis on small biopsies, cytology, cell block
- Intraoperative diagnosis: malignancy cannot be ruled out, challenging histological diagnosis on frozen sections
- Reference: World J Surg Oncol 2013;11:85
Radiology description
- Significant size variability, ranging from 1 to 8 cm in diameter, majority are < 3.5 cm
- Xray: solitary, well defined nodular lesion (oval to rounded shadow), may show calcification and crescent radiolucency at the periphery (air crescent sign)
- CT: well defined intraparenchymal nodular mass (often juxtapleural), may show calcification, air crescent sign and inhomogeneous enhancement
- Can occasionally present as lobulated, pure or mixed ground glass nodules or with pleural traction, mimicking malignant tumors
- Reference: Medicine (Baltimore) 2015;94:e498
Radiology images
Images hosted on other servers:

Well defined nodular lesion in peripheral lung
Prognostic factors
- Diagnostic accuracy of sclerosing pneumocytoma is better in nodules > 1.0 cm in diameter
- Less invasive procedure is performed if sclerosing pneumocytoma can be diagnosed intraoperatively on frozen section
- Most sclerosing pneumocytomas behave in a benign fashion with an excellent prognosis
- Cases with recurrence are described (Thorac Cardiovasc Surg 2008;56:120)
- Cases with malignant transformation are described (BMC Cancer 2019;19:1154)
- Cases with lymph node metastasis are described (Am J Surg Pathol 2000;24:906, Jpn J Clin Oncol 1986;16:77, Ann Thorac Surg 2002;73:981, Arch Pathol Lab Med 2003;127:321, Yonsei Med J 2003;44:150, J Thorac Oncol 2016;11:1785, Histopathology 2020;77:718, Gen Thorac Cardiovasc Surg 2021;69:142)
- Cases with distal or pleural metastasis are described (Histopathology 2012;60:1162, Korean J Intern Med 2015;30:928, Surg Today 2011;41:258, Front Med (Lausanne) 2021;8:661032)
- Very rare cases with death are described (Front Med (Lausanne) 2021;8:661032)
Case reports
- 14 year old girl with carcinoid-like tumor characteristics on preoperative imaging (Indian J Thorac Cardiovasc Surg 2021;37:676)
- 23 year old woman with masquerading adenocarcinoma with coexisting BRAF and PTEN mutation (Cancer Treat Res Commun 2021;28:100429)
- 25 year old woman with pulmonary sclerosing pneumocytoma and mediastinal lymph node metastasis misdiagnosed on intraoperative frozen section as adenocarcinoma (Gen Thorac Cardiovasc Surg 2021;69:142)
- 25 year old man with large pulmonary sclerosing pneumocytoma with multiple foci and reported lymph node and extrapulmonary metastases (Front Med (Lausanne) 2021;8:661032)
- 43 year old woman with sclerosing pneumocytoma in highly unusual endobronchial location (Medicine (Baltimore) 2019;98:e15038)
- 64 year old woman with massive necrosis and vascular invasion (Oxf Med Case Reports 2019;2019:omz066)
Treatment
- Mainstay treatment is surgical resection
- Generally, sublobar wedge resection and lymph node dissection (with lymph node metastasis) is curative for peripheral small sized tumors (Korean J Thorac Cardiovasc Surg 2011;44:39)
- Limited resection is favored with preservation of lung function if sufficient resection margin can be achieved (World J Surg Oncol 2022;20:140)
Gross description
- Well circumscribed mass, with varied gray-tan to yellow tumors
- Can also present dark red with hard texture (hemorrhagic)
- May find cystic degeneration and calcification
- Significant size variability, ranging from 1 to 8 cm in diameter, majority are < 3.5 cm
Gross images
Images hosted on other servers:

Well demarcated hemorrhagic peripheral lung lesion
Frozen section description
- Key diagnostic clues intraoperatively
- Gross appearance is consistent with sclerosing pneumocytoma
- Recognition of the dual cell population
- Identification of different architectural patterns: papillary, sclerotic, solid and hemorrhagic
- Clinical history of a nonsmoker younger patient with a well circumscribed peripheral lesion
- Major diagnostic pitfalls: solid predominant pattern, hypercellularity, glandular spaces, desmoplasia-like sclerosis, cellular atypia, coagulative necrosis (Histopathology 2018;72:500)
Frozen section images
Contributed by Matthew J. Cecchini, M.D., Ph.D.
Variable architecture
Cell populations
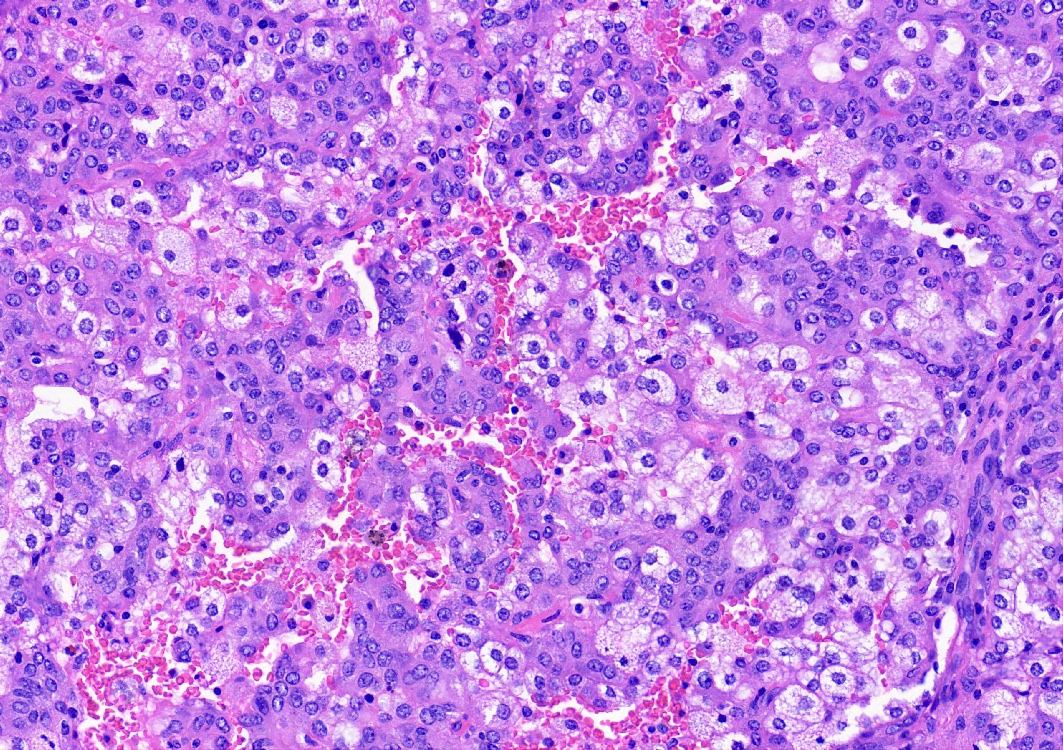
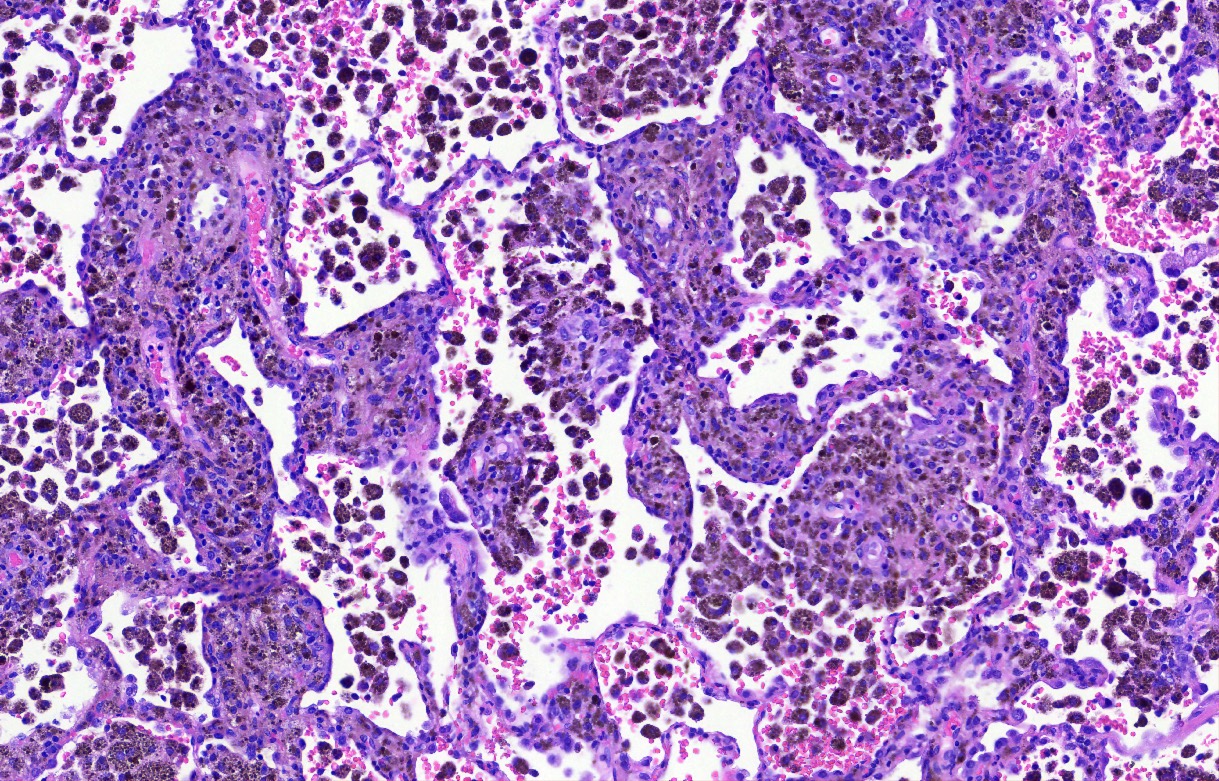
Microscopic (histologic) description
- Key feature is the presence of 2 cell types: cuboidal surface cells and round stromal cells
- Cuboidal surface cells resemble type II pneumocytes
- Round stromal cells have well defined border, with bland monotonous cells and fine chromatin
- 4 histologic growth patterns have been described
- Papillary: surface cells overlying hypercellular fibrovascular cores of round cells
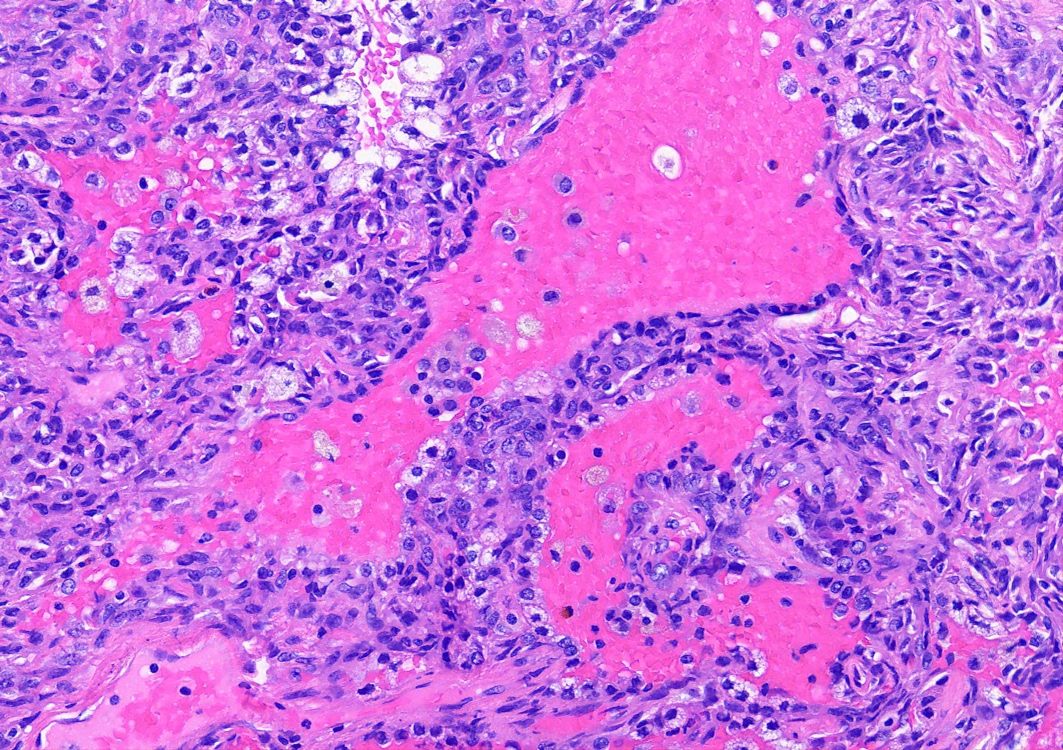
- Sclerotic: composed of hyalinized collagen, hemosiderin deposition in macrophages, cholesterol clefts and dystrophic calcification
- Solid: sheets of round cells with tubular / incomplete adenoid structures surrounded by surface cells
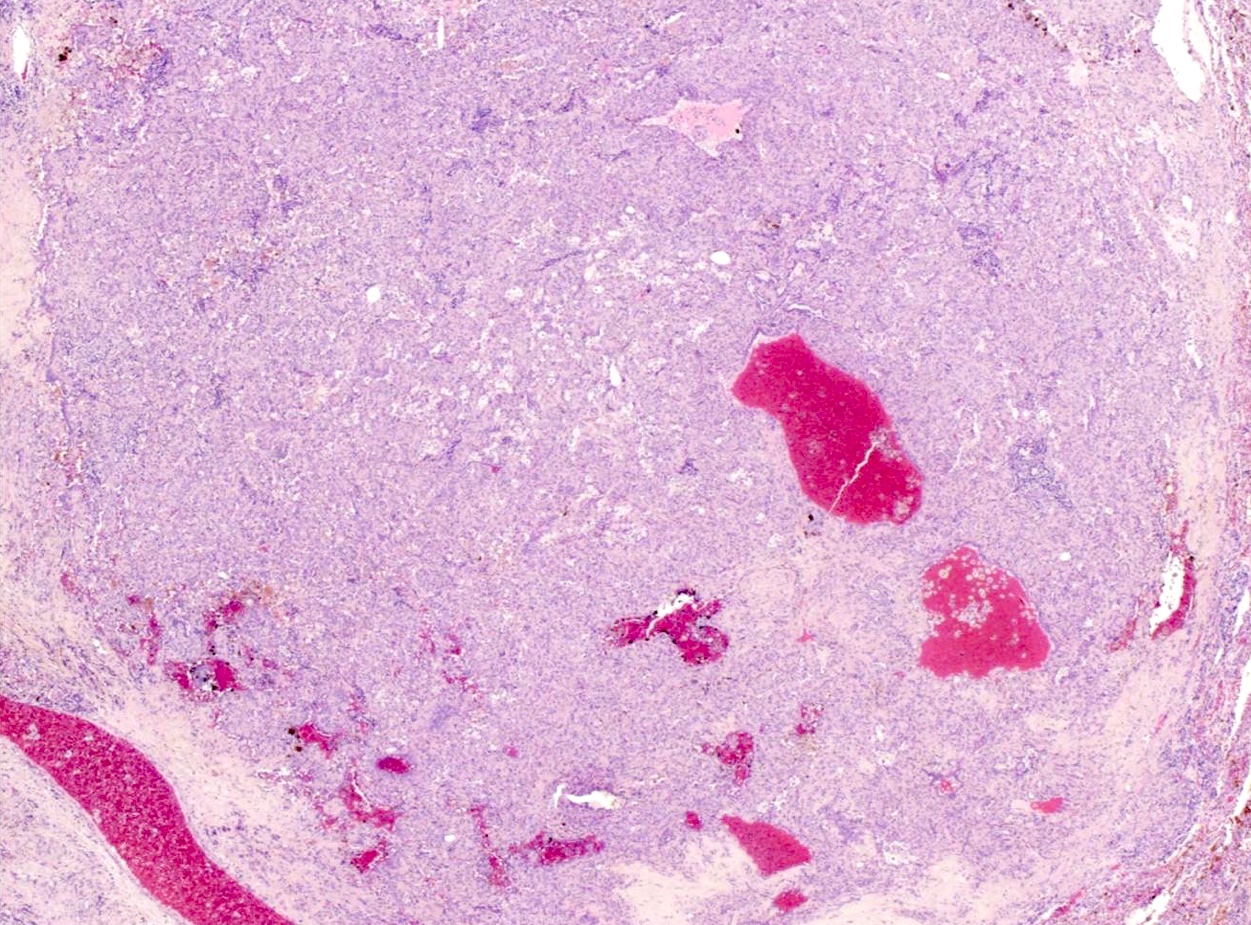
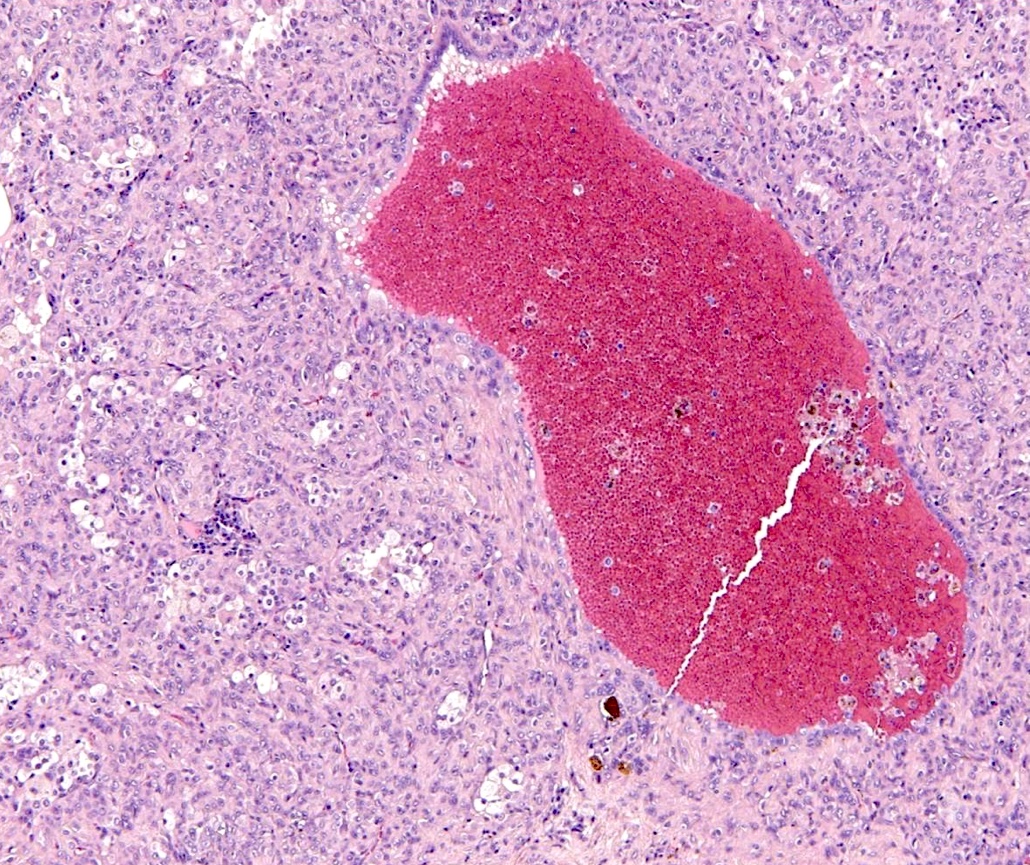
- Hemorrhagic: blood filled spaces lined by cuboidal epithelial cells
- Most tumors contain at least 3 of the 4 growth patterns in various proportions (Histopathology 2018;72:500)
Microscopic (histologic) images
Contributed by Matthew J. Cecchini, M.D., Ph.D. and Pooja Navale, M.D.
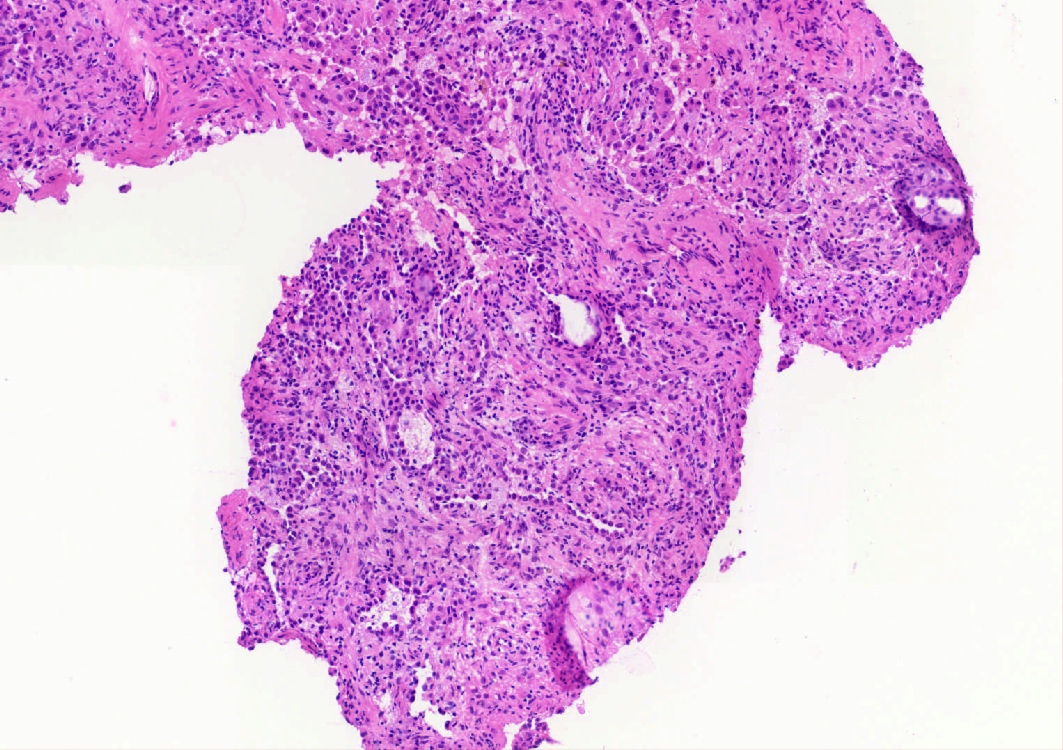
Core needle biopsy with various growth patterns
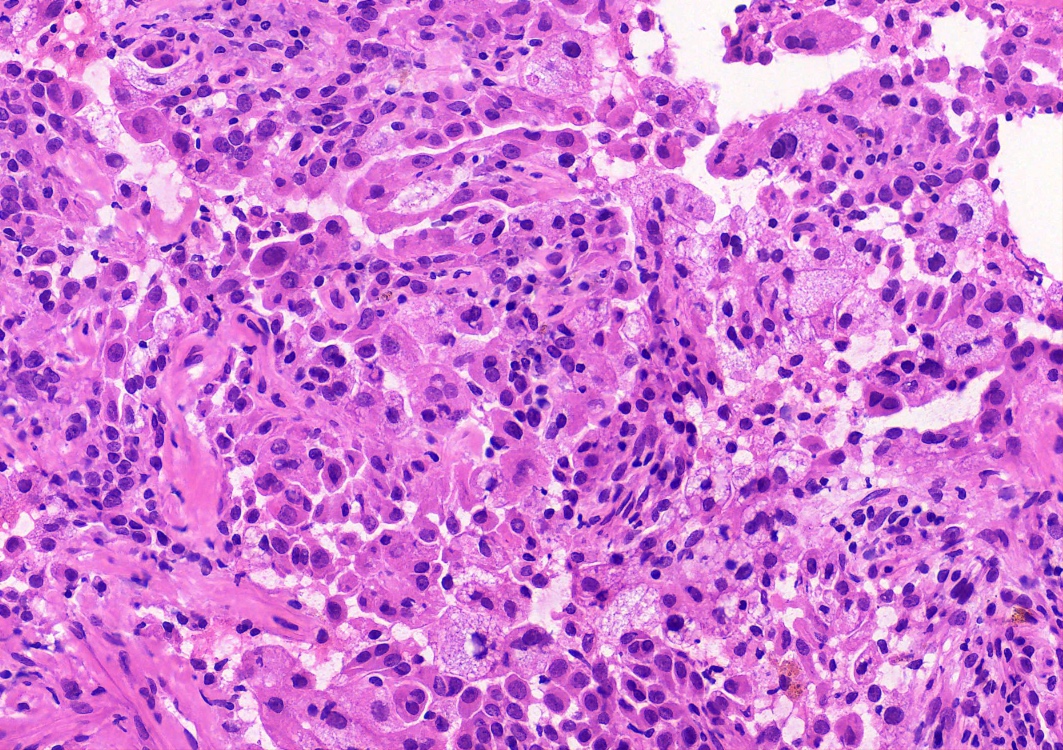
Core needle biopsy with 2 cell population
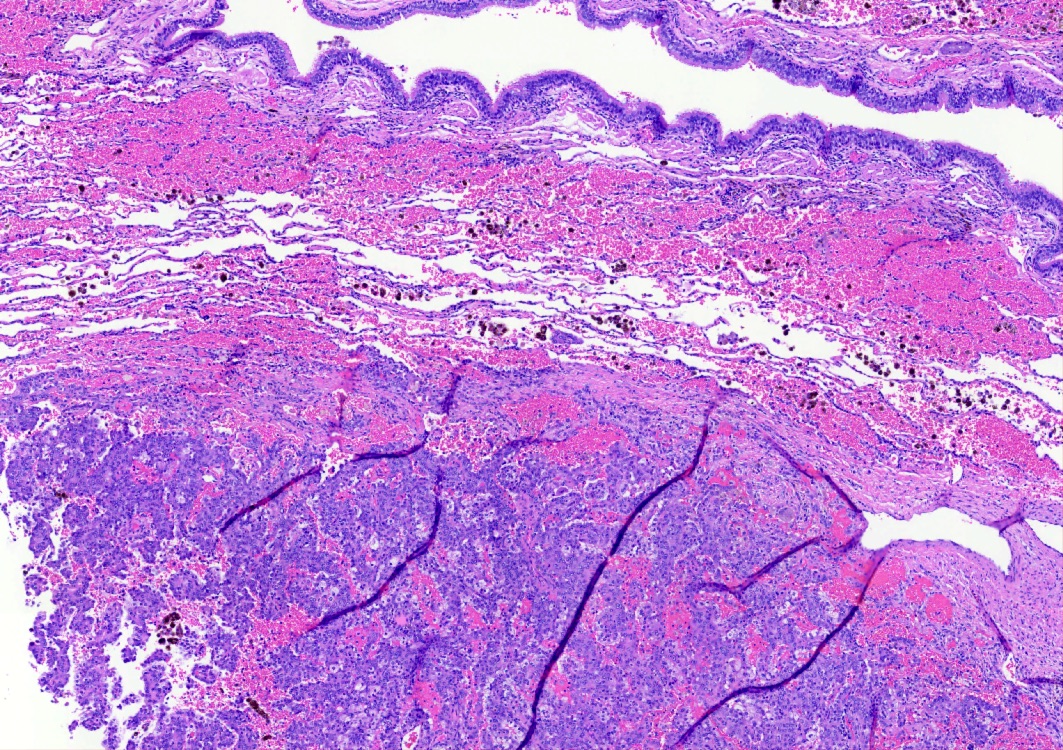
Well demarcated lesion
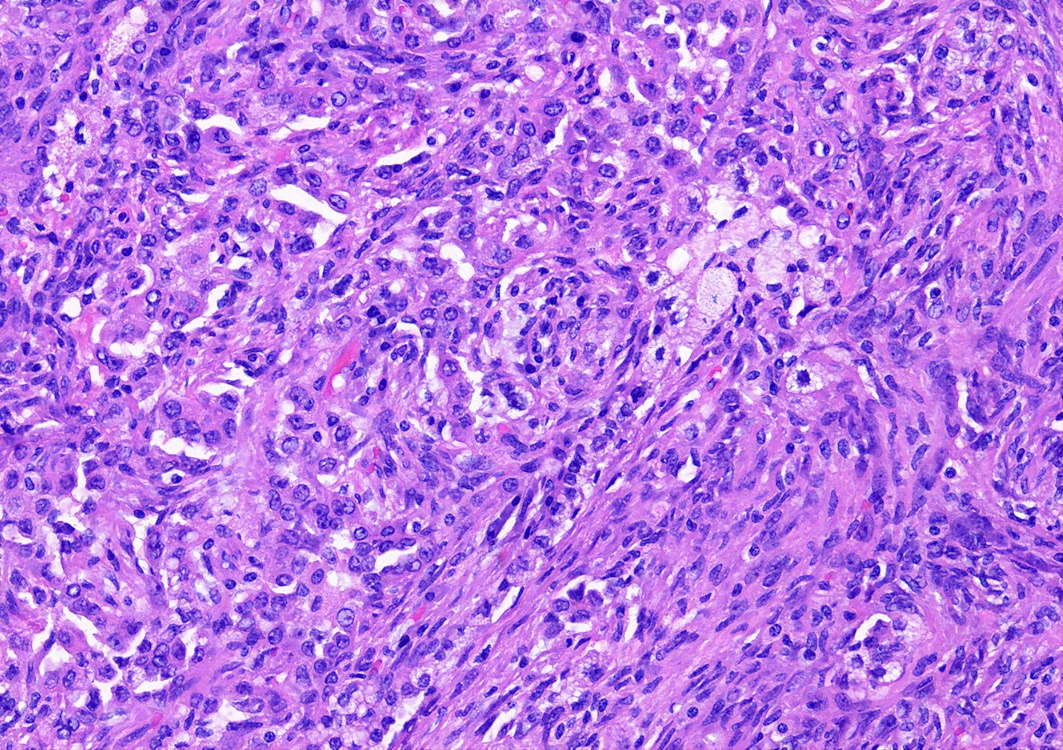
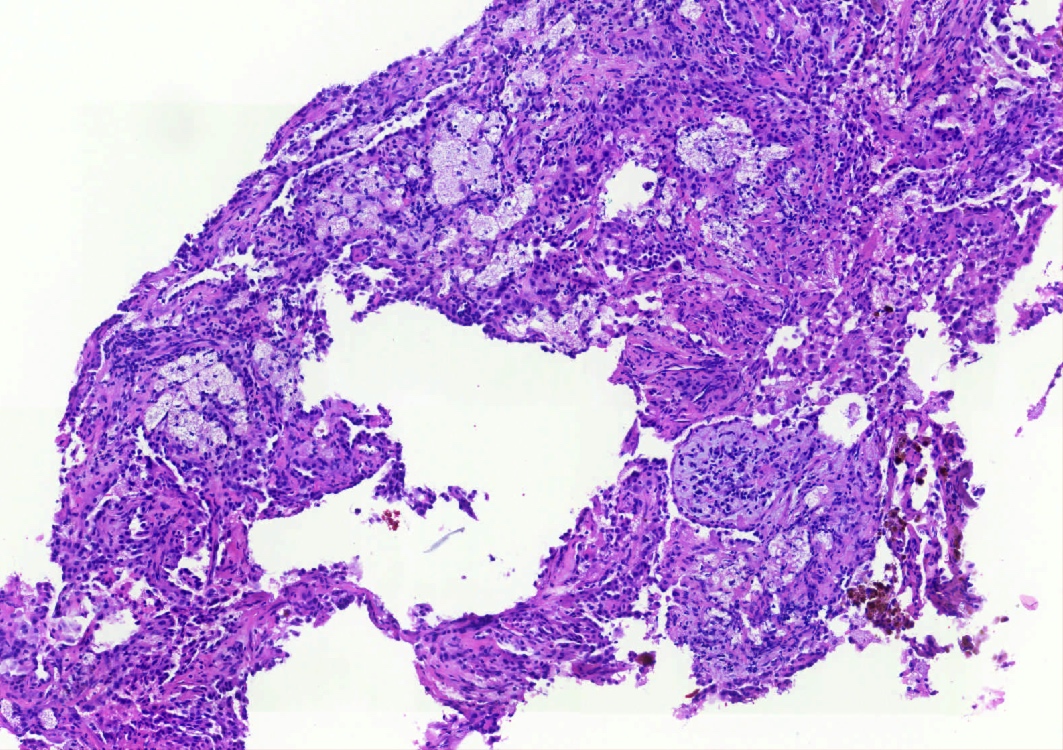
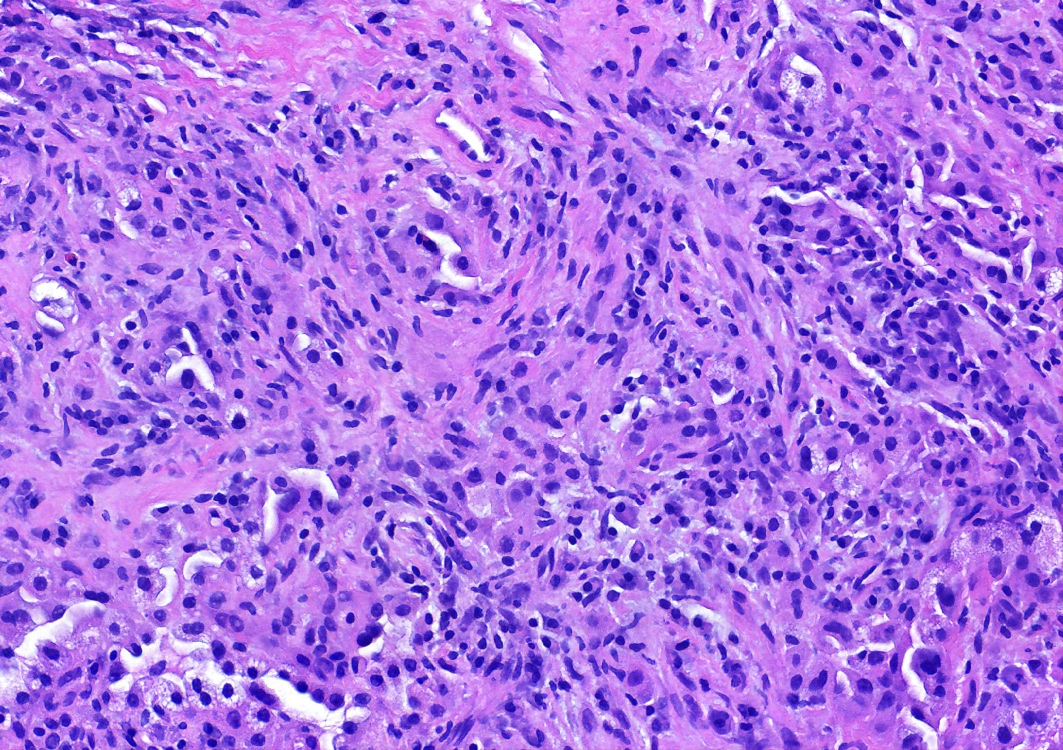
Solid growth architecture
Papillary architecture
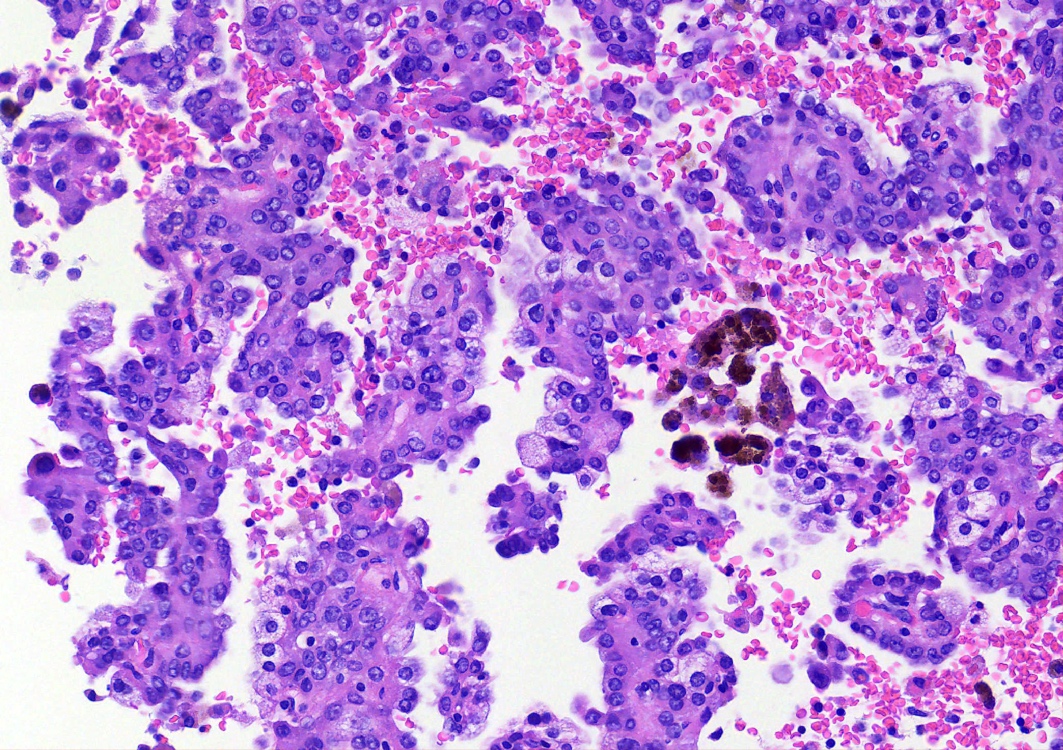
Hemorrhagic areas
Prominent foamy macrophages
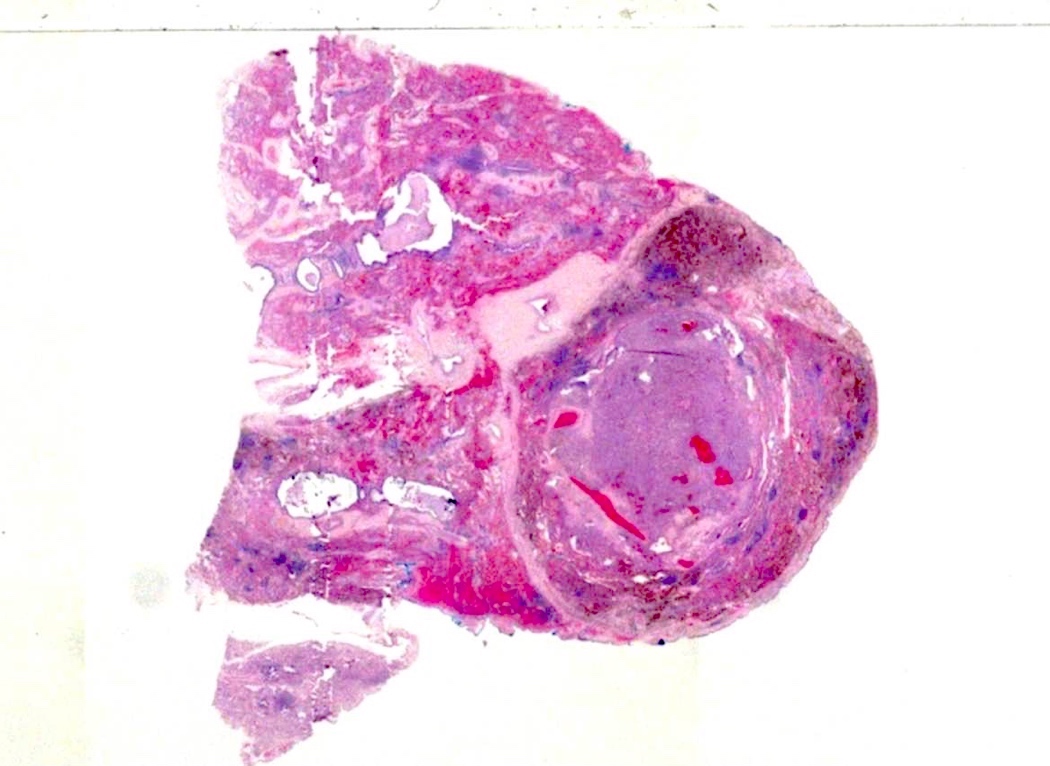
Whole mount view
Solid tumor
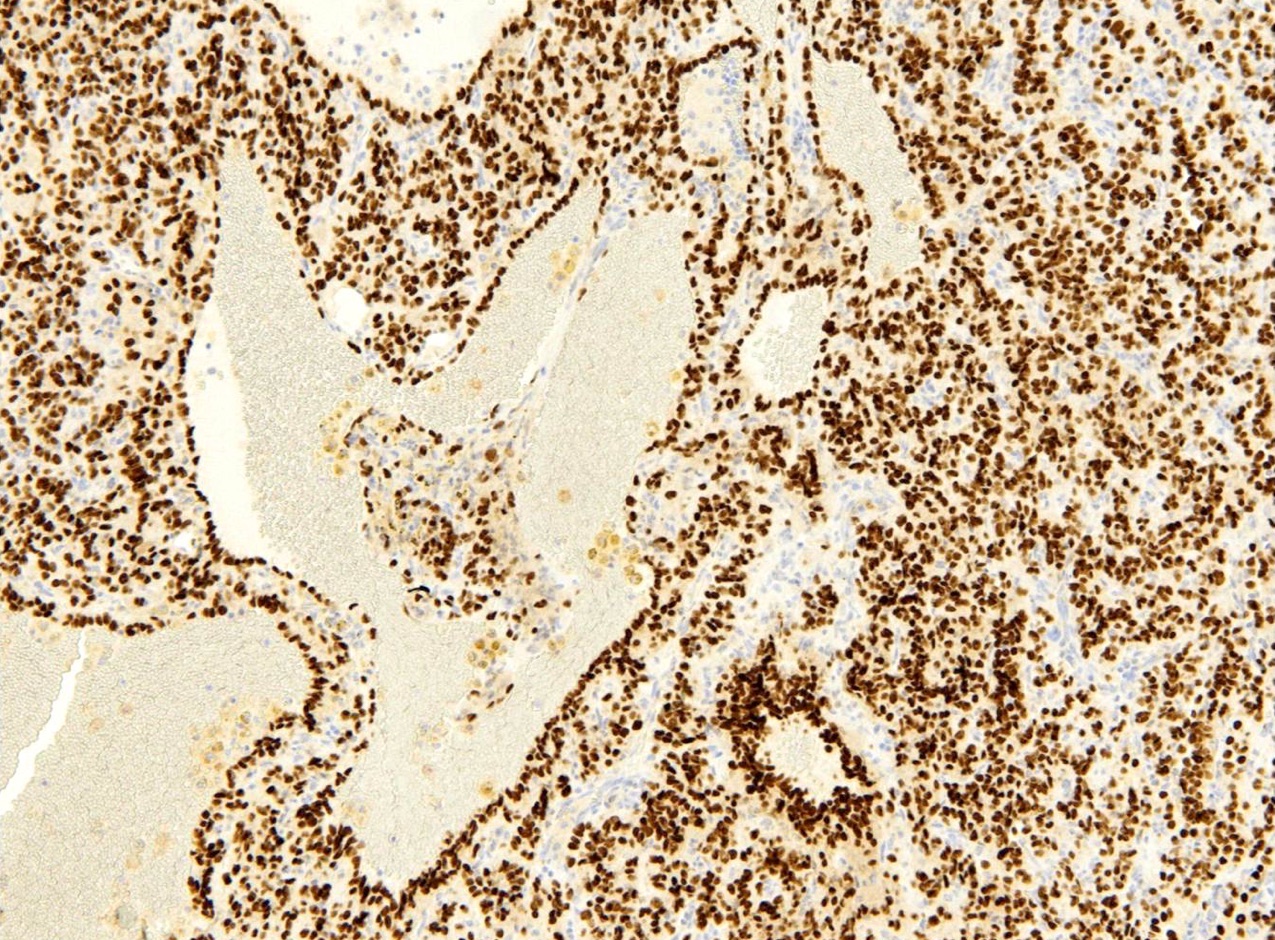
Surface cells and round cells
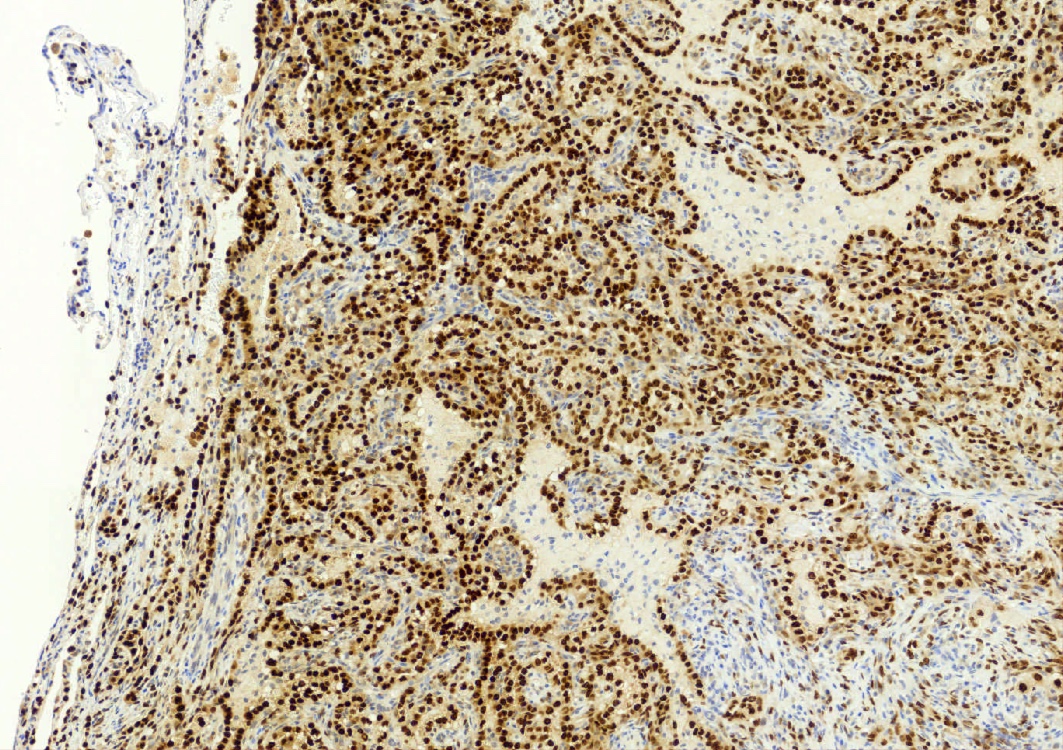
TTF1 highlights both cell populations
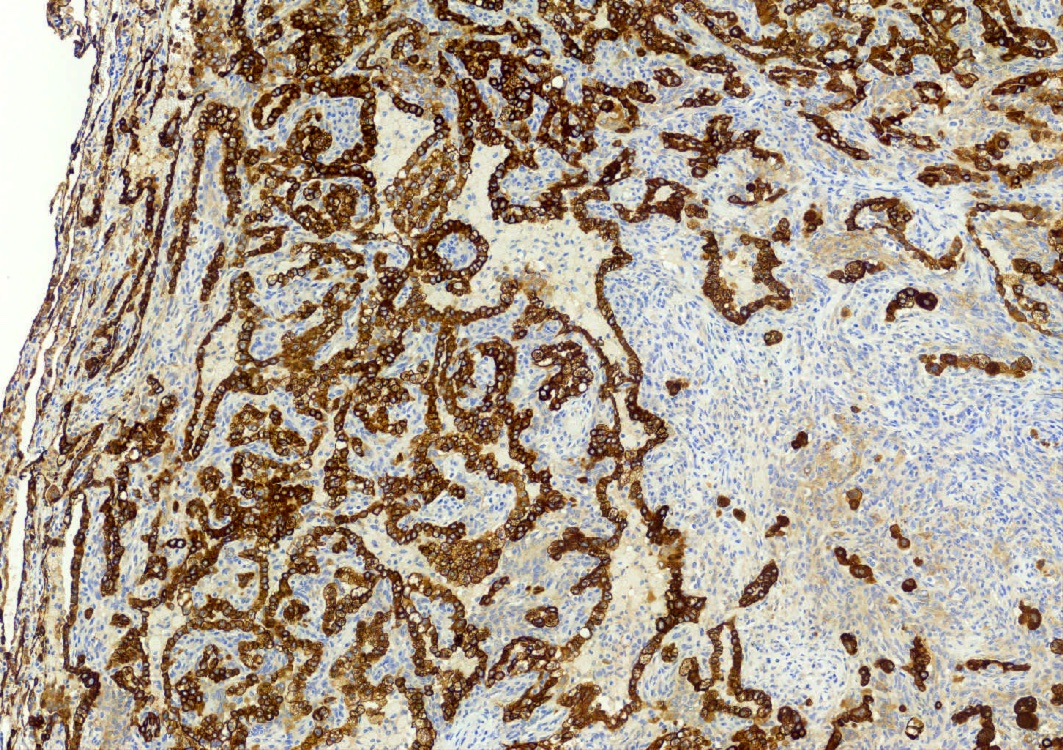
Pancytokeratin highlights the surface cells
TTF1
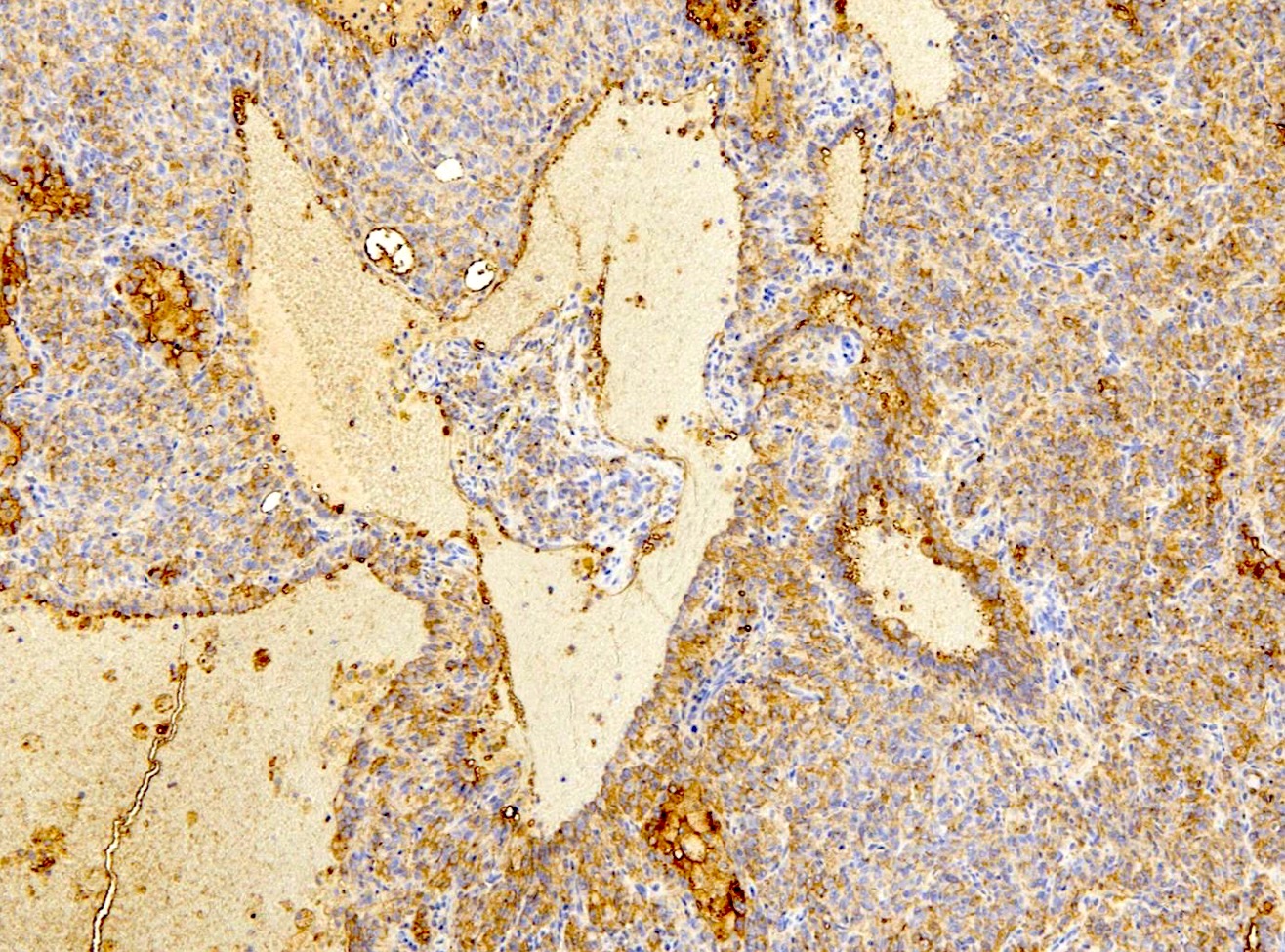
EMA
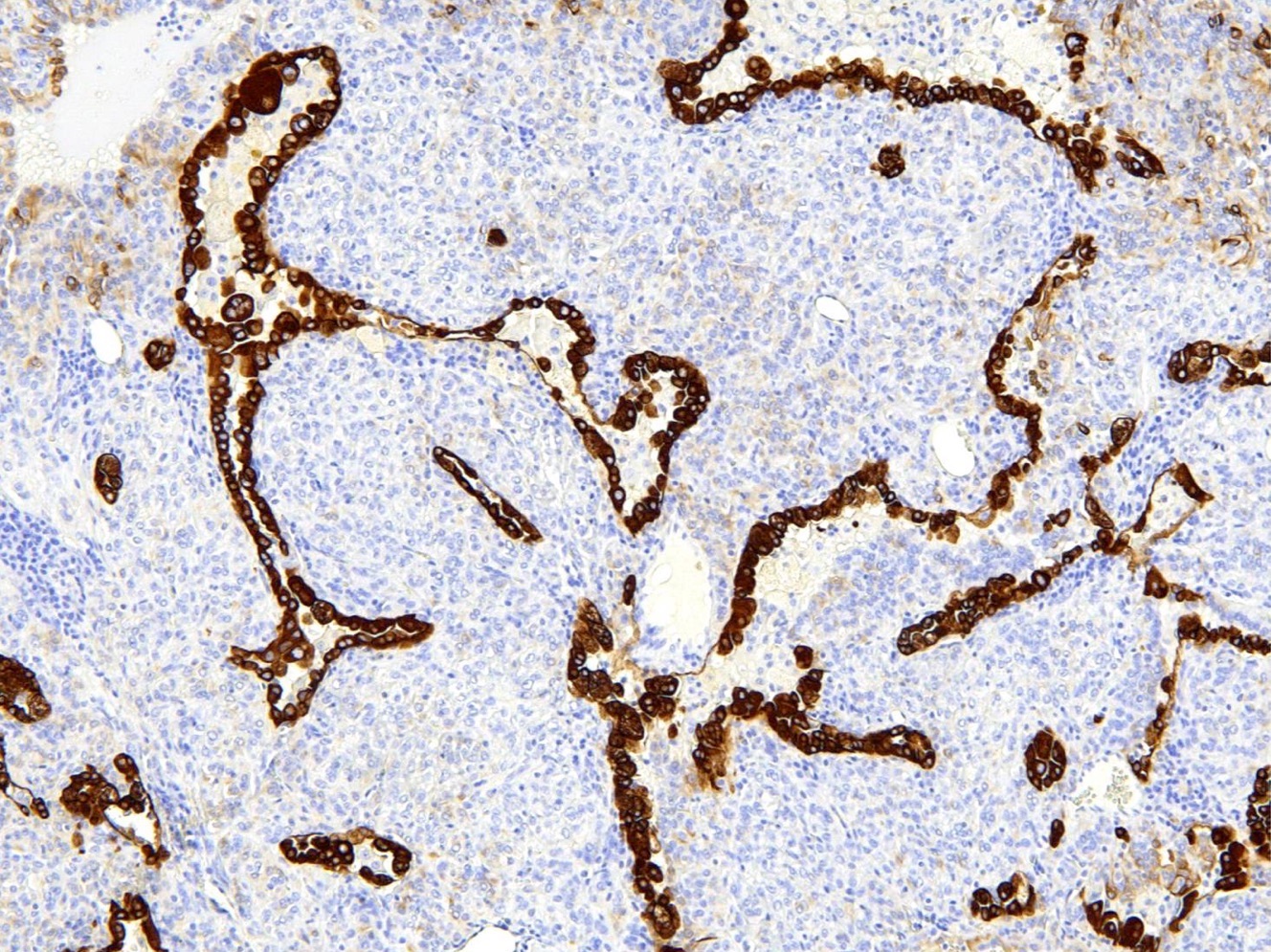
CAM 5.2
Cytology description
- Cytomorphological findings of sclerosing pneumocytoma overlap with lung adenocarcinoma (Cancer Cytopathol 2020;128:414)
- Most common cytological features (Diagn Cytopathol 2014;42:242)
- Moderately to highly cellular
- Papillary structures and large sheets
- Small to medium sized cells with moderate / abundant cytoplasm
- Bland round to oval nuclei with inconspicuous nucleoli
- Hemorrhagic background (fresh blood, siderophages, free hemosiderin pigment)
Positive stains
- EMA and TTF1: both surface and round cells stain strongly positive
- Pancytokeratin (AE1 / AE3), CAM5.2, CK7, Napsin A: stain surface cells diffusely but weakly or negative for round cells
- Reference: Am J Surg Pathol 2000;24:906
Negative stains
- Neuroendocrine markers: chromogranin A, synaptophysin
Molecular / cytogenetics description
- AKT1 mutations are the molecular hallmark of pulmonary sclerosing pneumocytoma (Mod Pathol 2020;33:391)
Videos
Sclerosing pneumocytoma in small biopsy
Sclerosing pneumocytoma in resection
Sample pathology report
- Right lung, lower lobe, wedge resection:
- Sclerosing pneumocytoma (see microscopic description)
- 1.5 cm in greatest dimension
- Tumor present 1.0 cm from nearest (parenchymal) margin
- 2 lymph nodes, negative for malignancy
- Sclerosing pneumocytoma (see microscopic description)
Differential diagnosis
- Adenocarcinoma (papillary):
- Malignant tumor with 1 (epithelial) cell population
- Neuroendocrine tumor (carcinoid tumor):
- Tumor with 1 cell population with expression of neuroendocrine markers by immunohistochemistry
Board review style question #1
What is the immunophenotype of the round cells in a sclerosing pneumocytoma?
- TTF1 negative, pancytokeratin negative
- TTF1 negative, pancytokeratin positive
- TTF1 positive, pancytokeratin negative
- TTF1 positive, pancytokeratin positive
Board review style answer #1
C. TTF1 positive, pancytokeratin negative. The round cells have a unique immunophenotype of TTF1 positive and cytokeratin negative, which is proposed to correspond to a primitive respiratory epithelium-like immunophenotype. Answer A is incorrect because the round cells have TTF1 expression.
Answer B is incorrect because the round cells are keratin negative and TTF1 positive. Answer D is incorrect because the round cells are keratin negative.
Comment Here
Reference: Sclerosing pneumocytoma
Comment Here
Reference: Sclerosing pneumocytoma
Board review style question #2
The pigment seen adjacent to a sclerosing pneumocytoma likely relates to which of the following?
- Alveolar hemorrhage (hemosiderin deposition)
- Cannabis use
- Cigarette smoking
- Melanin pigment
Board review style answer #2
A. Alveolar hemorrhage (hemosiderin deposition). These tumors are often associated with hemorrhage and the pigment typically relates to hemosiderin. This can be a clue to the diagnosis. Answer B is incorrect because cannabis pigment has a more coarse brown appearance than hemosiderin.
Answer C is incorrect because the smoking related pigment has a fine yellow-brown appearance with black specks.
Answer D is incorrect because melanin has a fine dusty appearance compared to hemosiderin. Melanin is not typically associated with sclerosing pneumocytoma.
Comment Here
Reference: Sclerosing pneumocytoma
Comment Here
Reference: Sclerosing pneumocytoma
