
Lung
Other tumors
Metastases
Author: Roseann I. Wu, M.D., M.P.H.
Last author update: 1 February 2018
Last staff update: 14 September 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Metastatic lung tumor [title]

Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology images | Positive stains | Negative stains | Differential diagnosis | Board review style question #1 | Board review style answer #1Cite this page: Wu R. Metastases. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lungtumormetastases.html. Accessed December 21st, 2024.
Definition / general
- Lung is a common site of metastases; usually multiple, bilateral, sharply outlined, rapidly growing, more pleomorphic and necrotic than lung primaries
- May appear as multiple discrete nodules in periphery of lung or as lymphangitic carcinomatosis (peribronchial and perivascular patterns via lymphatics)
- Rarely appear as intralymphatic microscopic foci that cause pulmonary hypertension
- Metastases can also be from other lung primaries (Am J Surg Pathol 2009;33:1752)
Essential features
- Lung is a common site of metastatic disease and may be the first or only site of metastatic involvement
- Lung metastases are generally multiple, well circumscribed and tend to grow rapidly
- A history of malignancy is helpful in determining the primary site but a panel of immunohistochemical stains can help support the diagnosis
ICD coding
Epidemiology
- In autopsy studies, 20 - 50% of patients with malignancy had lung metastasis (Cancer 1981;47:2595)
Sites
- Generally peripheral lung but can also be endobronchial
Pathophysiology
- Five year overall survival for all lung metastases is 36% (J Thorac Cardiovasc Surg 1997;113:37)
Etiology
- Mostly hematogenous or lymphogenous spread from primary site
Clinical features
- Usually asymptomatic or may present with nonspecific cough, chest pain, hemoptysis, spontaneous pneumothorax (J Surg Oncol 2014;109:42)
Diagnosis
- Typically detected by imaging, specifically CT scans
- Confirmation by cytologic or histologic sampling
Radiology description
- CT scans are preferred modality
- Single or multiple, peripheral, well circumscribed nodule(s)
- Limited detection of subcentimeter disease
Radiology images
Contributed by Fulvio Lonardo, M.D.
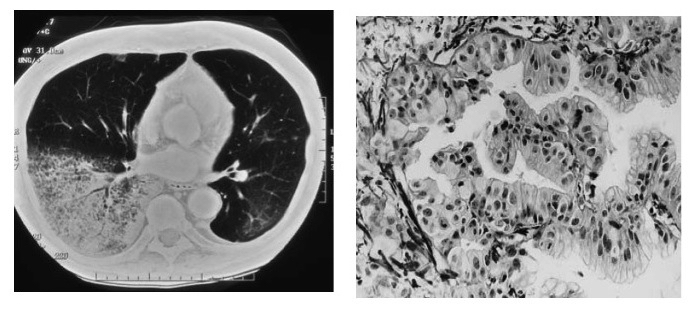
Pancreas: adenocarcinoma
Images hosted on other servers:

Malignant melanoma
shows pulmonary
nodules

Multiple round nodules and masses in both lungs

Cannonball lung metastases in patient with colon cancer

Multiple lung metastases
Prognostic factors
- Clinical variables associated with prolonged survival after lung metastasectomy in colorectal cancer patients
- Prolonged disease free interval between primary tumor and metastasis, normal prethoracotomy carcinoembryonic antigen, absence of thoracic node involvement and single pulmonary lesion (Ann Surg Oncol 2013;20:572)
- Complete resection and longer disease free interval > 6 months associated with better survival (Surg Oncol 2012;21:237)
Case reports
- 48 year old man with lymphangitic spread of hepatocellular carcinoma (Arch Pathol Lab Med 2003;127:e11)
- 50 year old man with ameloblastoma of jaw metastatic to lung (Case of the Week #318)
- 51 year old man with metastatic melanoma showing ground glass opacities (Am J Respir Crit Care Med 2015;191:954)
- 59 year old man with cavitary lung metastasis from urothelial carcinoma, diagnosed by FNA (Can Respir J 2011;18:e46)
- 65 year old woman with parotid gland acinic cell carcinoma metastatic to lung (Arch Pathol Lab Med 2007;131:970)
- 83 year old man with epithelioid tumor of lungs (Arch Pathol Lab Med 2005;129:e7)
Treatment
- Chemotherapy, immunotherapy, other systemic therapy
- Criteria for pulmonary metastasectomy: primary site of disease controlled, complete resection of lung metastasis feasible, patient able to tolerate procedure, no better alternative treatments (J Surg Oncol 2014;109:42)
- Stereotactic body radiation therapy (SBRT) and radiofrequency ablation (RFA) may be considered for small, solitary, peripheral tumors
Gross description
-
Patterns associated with specific primaries
- Central cavitation: colonic adenocarcinoma, leiomyosarcoma, squamous cell carcinoma of upper aerodigestive tract
- Intrabronchial masses: breast, colon, kidney
- Lymphangitic carcinomatosis: breast, choriocarcinoma, pancreas, prostate, stomach
- Nodular metastases: breast, GI, kidney, melanoma, sarcoma
- Tumor emboli: breast, choriocarcinoma, liver, stomach
Gross images
Contributed by Roseann Wu, M.D., M.P.H.
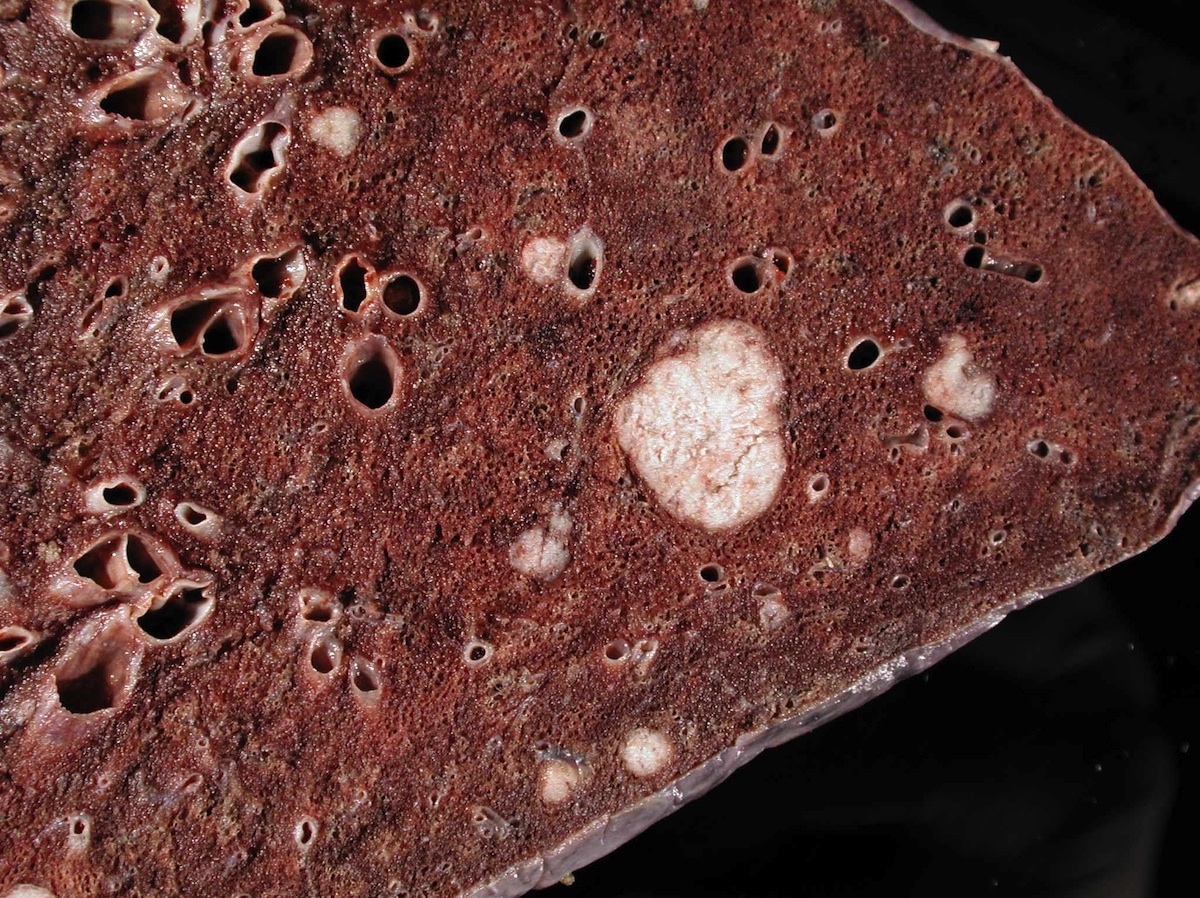
Lung with metastatic tumor
Images hosted on other servers:


Multiple tumor nodules
Microscopic (histologic) description
- Dependent on site of origin (colorectal cancer, bone and soft tissue sarcoma, renal cell carcinoma, melanoma, head and neck tumors, germ cell tumors and many others)
- Evidence for breast metastasis over lung primary: comedonecrosis, solid nests, trabecular architecture, cribriform growth pattern (Am J Clin Pathol 2009;131:122)
Microscopic (histologic) images
Contributed by Roseann Wu, M.D., M.P.H., Debra Zynger, M.D., Case #318 and Fulvio Lonardo, M.D.
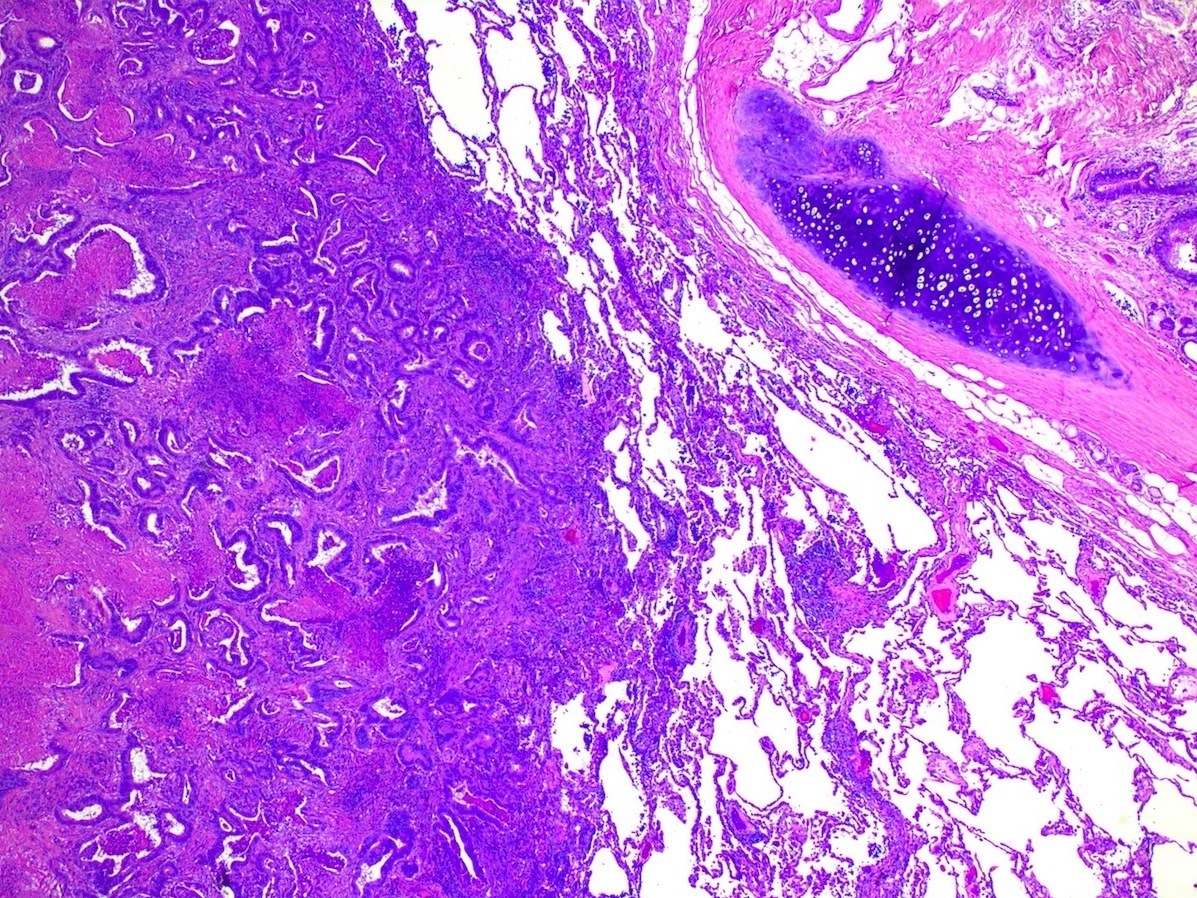
Metastatic colon CA to lung 25x
Clear cell renal
cell carcinoma
metastatic to lung
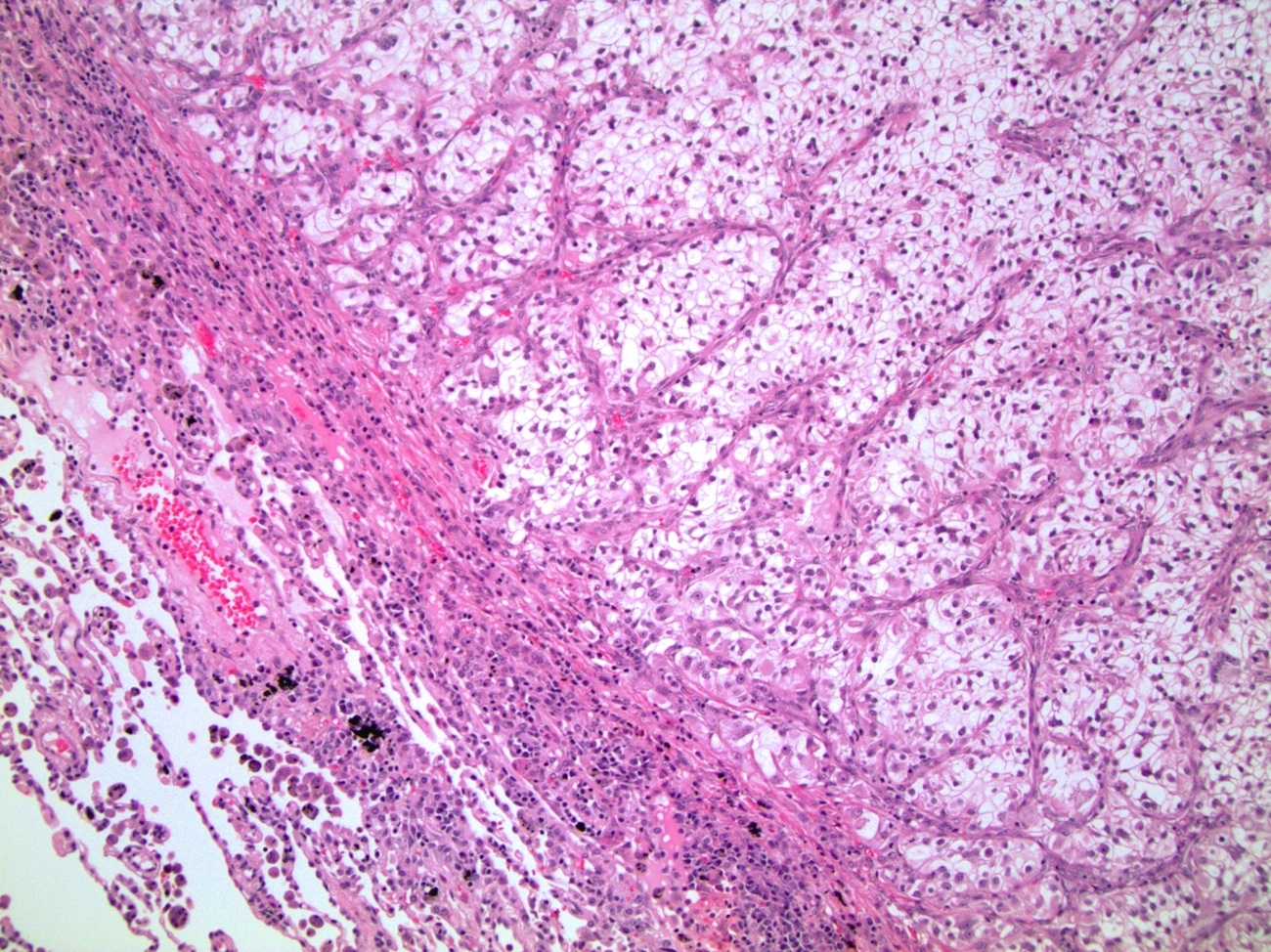
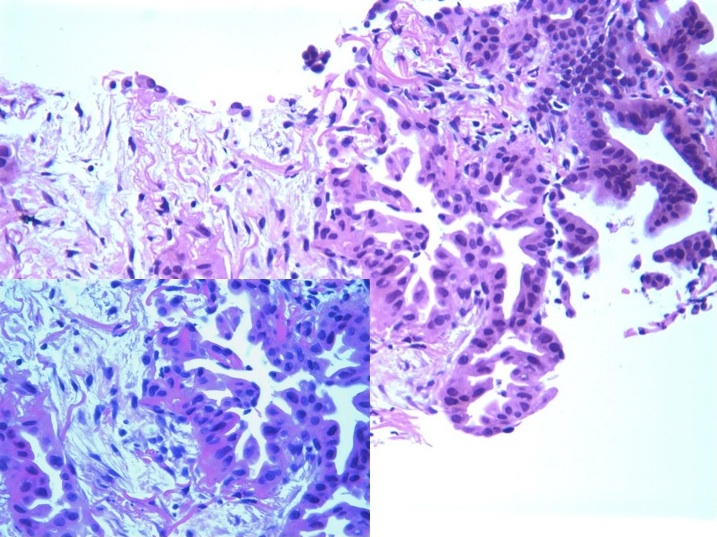
Prostatic
adenocarcinoma
metastatic to lung
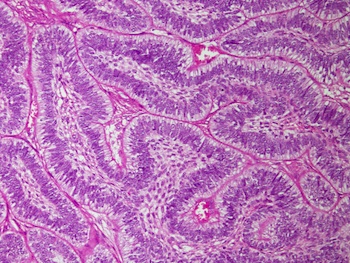
Testicular germ
cell tumor (teratoma)
metastatic to lung
Jaw: ameloblastoma
metastatic to lung
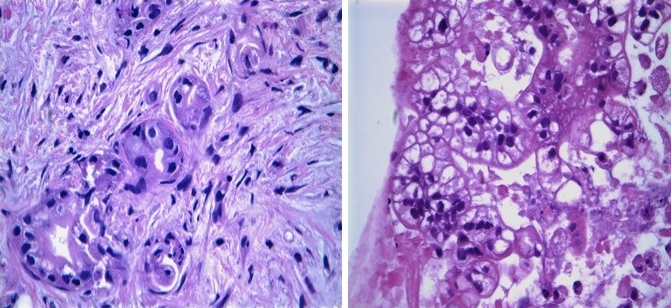
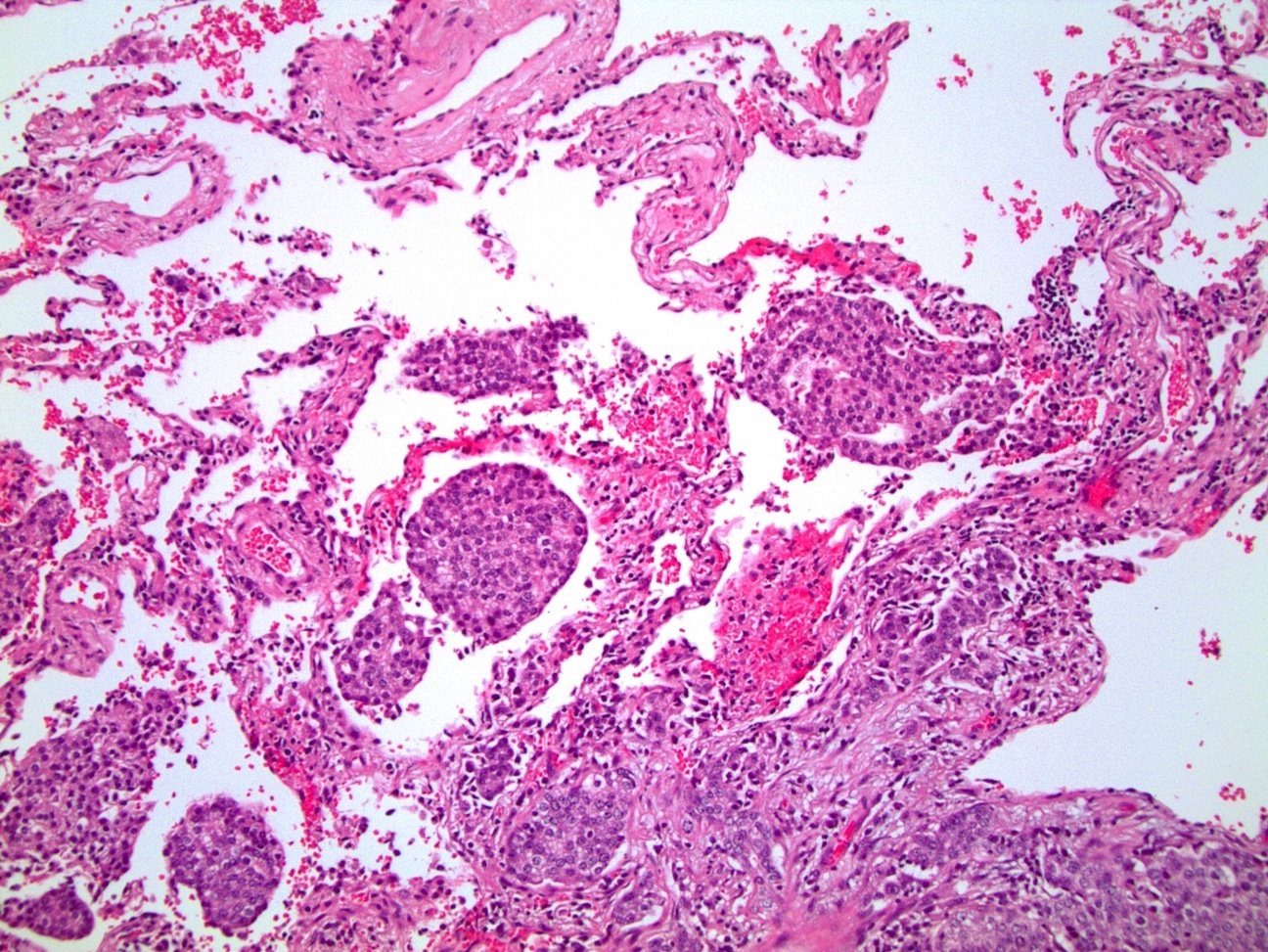
Pancreas: adenocarcinoma
Cytology images
Contributed by Roseann Wu, M.D., M.P.H.
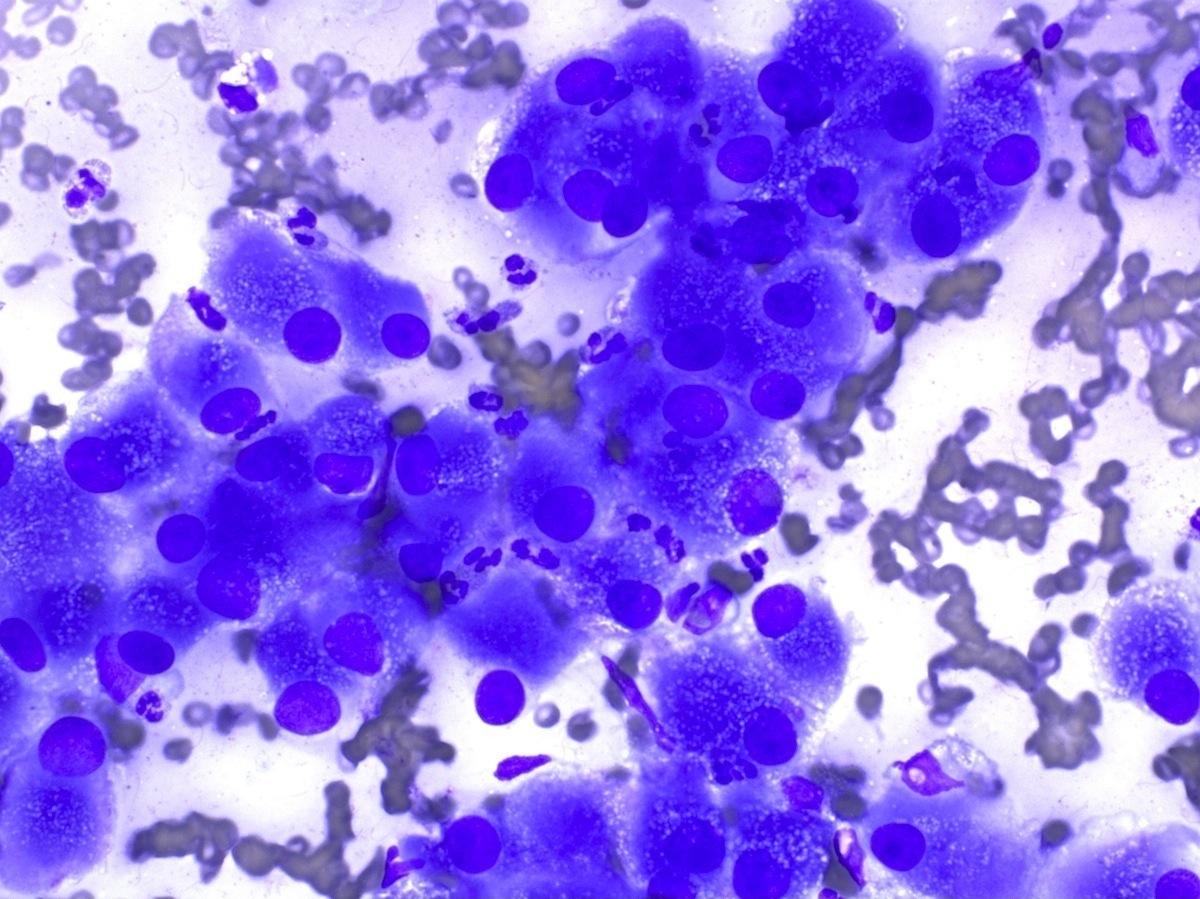
Metastatic renal cell carcinoma to lung
Images hosted on other servers:

Bladder, urothelial carcinoma
Positive stains
- CDX2 suggests colorectal carcinoma (Am J Surg Pathol 2003;27:141)
- Pankeratin to prove epithelial origin, CK7 / CK20 to help differentiate
- Lineage specific markers variable depending on site of origin, see Table 2 for suggested stains (Arch Pathol Lab Med 2016;140:508)
Differential diagnosis
- Primary lung carcinoma: acini, lepidic growth, nuclear pseudoinclusions, central scar (Am J Clin Pathol 2009;131:122)
- Inflammatory nodule or benign neoplasm
Board review style question #1
- For which malignancy is pulmonary metastasectomy most commonly performed and reported?
- Colorectal cancer
- Germ cell tumors
- Melanoma
- Osteosarcoma
- Renal cell carcinoma
Board review style answer #1

