

Lung
Noninfectious granulomatous inflammation
Sarcoidosis
Authors: Brittany Cody, D.O., Aliya N. Husain, M.D.


Last staff update: 4 January 2024 (update in progress)
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed search: Lung sarcoidosis

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Negative stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Cody B, Husain AN. Sarcoidosis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lungnontumorsarcoidosis.html. Accessed April 19th, 2024.
Definition / general
- Systemic disease characterized by granulomatous inflammation, typically nonnecrotizing, with 90% of overall cases showing involvement of the lungs and hilar lymph nodes
- Subset of cases may involve the lung with sparing of lymph nodes
Essential features
- Granulomatous involvement of one or more tissues that is not attributable to other etiologies (including infectious)
- Clinical correlation is necessary even in the presence of classic histology
Terminology
- Previously called Besnier-Boeck-Schaumann disease (use not recommended)
- Löfgren syndrome: form of sarcoidosis presenting with hilar adenopathy, erythema nodosum, arthritis and fever
- Reference: StatPearls: Lofgren Syndrome [Accessed 9 March 2023]
ICD coding
Epidemiology
- Age of onset / diagnosis has shifted in recent years, with most cases now diagnosed at an older median age; most cases first occur in the fifth and sixth decades of life
- Women are affected at twice the rate of men; Black patients have the highest incidence of disease, followed by White patients
- Reference: Ann Am Thorac Soc 2016;13:1244
Sites
- Lungs, lymph node, cardiovascular, liver, skin, eye (see below under Clinical features)
Pathophysiology
- Believed to result from stimulation of CD4+ T cells by an unknown antigen
- Downstream effects of cytokines and chemokines stimulate macrophages and lead to granuloma formation
- Increased IFNγ and TNFα present in affected tissues
- Increased CD4+ T cells are seen in bronchoalveolar lavages (BAL) performed on sarcoidosis patients compared to controls
- Reference: Chest 2018;153:1432
Etiology
- Incompletely understood at this time
- Sarcoidosis occurs more frequently in those with chronic inhalational exposures of silica and metal particulates
- Reference: JAMA 2022;327:856
Clinical features
- Presentation: cough, dyspnea and other pulmonary symptoms are common; nonpulmonary presentations often include skin or eye lesions
- Acute presentations may display fever, arthralgia and painful skin lesions
- May be discovered incidentally following chest radiographs which often show hilar adenopathy and reticular opacities
- Lungs
- Reticular opacities on chest radiograph may be evident
- High resolution CT may show multiple subcentimeter nodules with a perilymphatic distribution
- Most cases will be associated with hilar lymphadenopathy
- Pulmonary involvement in the absence of lymphadenopathy portends a worse prognosis
- Lymph nodes
- The vast majority of patients show hilar or mediastinal lymphadenopathy
- Involved lymph nodes may be calcified or sclerotic
- Cardiovascular
- Symptomatic cardiac involvement is rare but autopsy studies have shown that > 50% of cases may show subclinical cardiac involvement
- Liver
- A subset of patients display liver involvement, often accompanied by hepatomegaly
- Cirrhosis is a rare complication
- Skin
- Skin involvement in ~25%
- Findings can include erythema nodosum or presence of numerous skin colored papules, especially on the face / nose
- Eye
- Common manifestations include uveitis and keratoconjunctivitis
- References: JAMA 2022;327:856, Intern Emerg Med 2018;13:325, Ann Am Thorac Soc 2016;13:1244, EClinicalMedicine 2021;37:100966
Diagnosis
- Sarcoidosis is a clinicopathologic diagnosis; may be made in the appropriate clinical setting after exclusion of relevant differential diagnoses
Laboratory
- Multiple inflammatory markers may be altered in patients with sarcoidosis though most abnormalities are nonspecific
- Angiotensin converting enzyme (ACE) is commonly elevated
- Tracking ACE as well as certain acute phase reactants including C reactive protein and serum amyloid A may be useful in tracking disease activity in established disease
- Elevated CD4 / CD8 ratio may be present on bronchoalveolar lavage (BAL)
- Many patients display hypergammaglobulinemia
- ~10% of patients have hypercalcemia
- Hepatic involvement can cause abnormal liver function tests
- References: JAMA 2022;327:856, Eur Respir J 1997;10:2716
Radiology description
- High resolution CT findings include perihilar opacities, micronodules with perilymphatic and bronchocentric distribution and variable fibrosis
- Chest radiographs demonstrate bilateral hilar adenopathy in the majority of cases
- Reference: Semin Respir Crit Care Med 2020;41:758
Radiology images
Images hosted on other servers:

Some HRCT patterns
Prognostic factors
- 5 year mortality is ~7%
- Most deaths (> 60%) are attributable to chronic pulmonary disease
- Isolated pulmonary involvement is associated with worse outcomes
- Clinical and radiographic findings are used to stage the disease (stages 0 - IV) (Radiopaedia: Thoracic sarcoidosis (staging) [Accessed 2 June 2023])
- Lower stages are associated with increased rates of resolution
- Higher stages are associated with increased mortality
- Reference: JAMA 2022;327:856
Case reports
- 27 year old man with cystic bronchiectasis related to sarcoidosis (BMJ Case Rep 2020;13:e237863)
- 39 year old man with sarcoidosis presenting as unilateral hilar adenopathy (Respir Med Case Rep 2020;31:101256)
- 58 year old woman with sarcoidosis and autoimmune pulmonary alveolar proteinosis (Clin Case Rep 2019;7:731)
- 60 year old woman presented with pulmonary infarct secondary to vascular involvement of sarcoidosis (Pathol Int 2021;71:480)
Treatment
- Oral corticosteroids are primary therapy
- Refractory cases may be treated with immunosuppressive agents
- Reference: JAMA 2022;327:856
Gross description
- In most cases, the cut surface will demonstrate the presence of multiple small white to tan nodules along the bronchovascular bundle and in the pleura
- Some cases may show larger, confluent nodularity
Gross images
Contributed by @AKhannaMBBS on Twitter


Sarcoidosis
Images hosted on other servers:

Hilar lymphadenopathy in sarcoidosis
Frozen section description
- Well circumscribed granulomas, often containing multinucleated giant cells
Microscopic (histologic) description
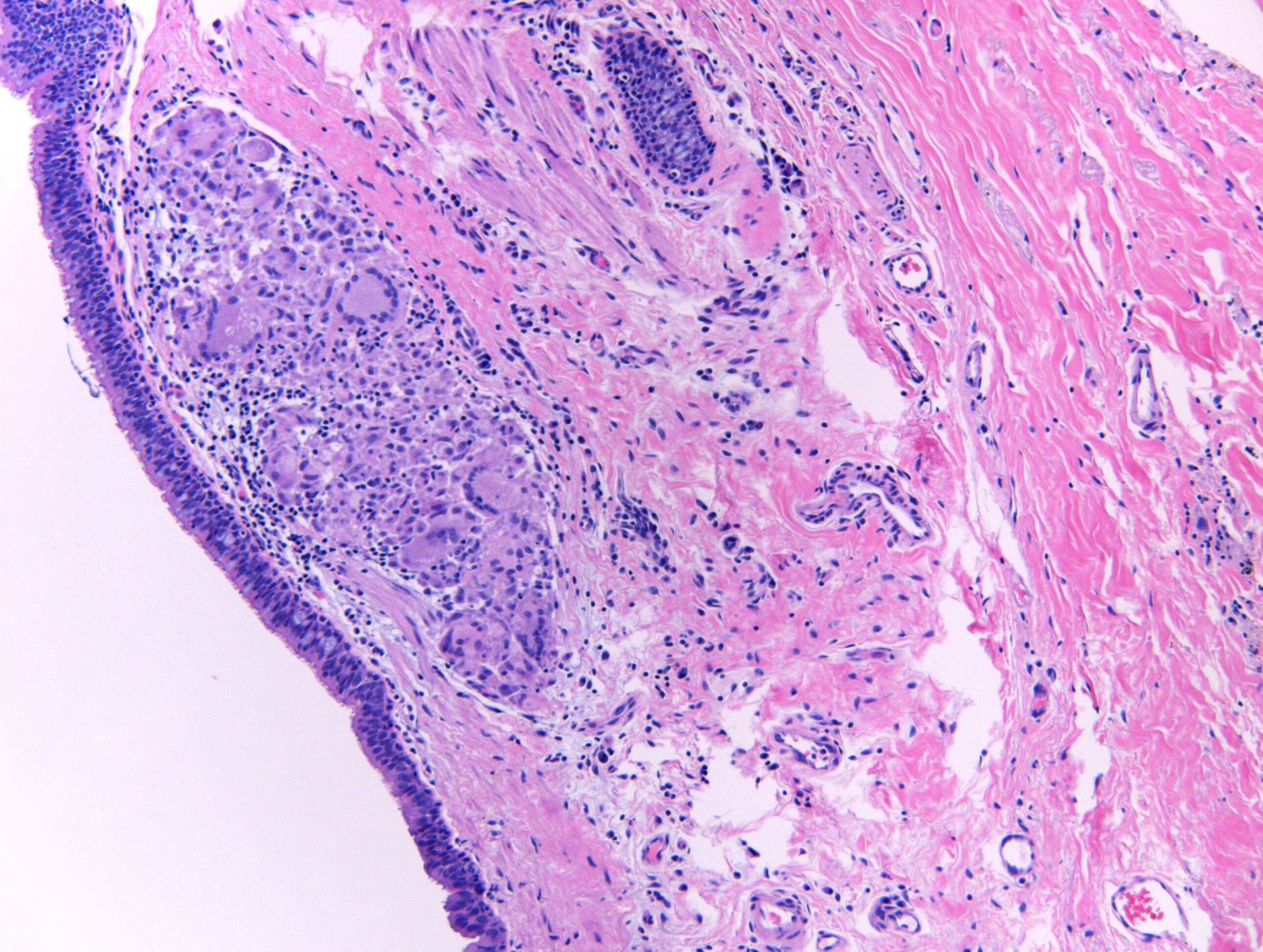
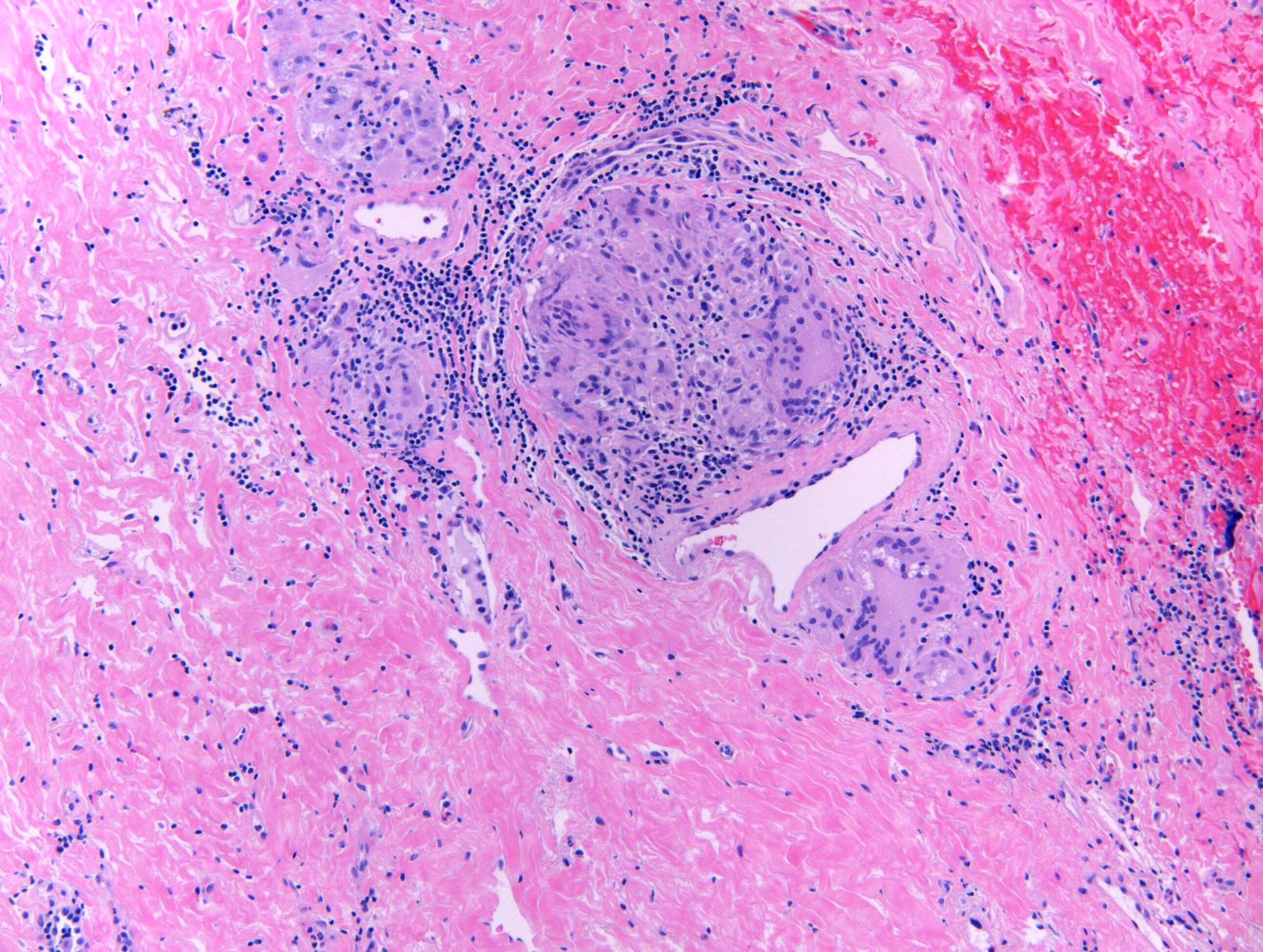
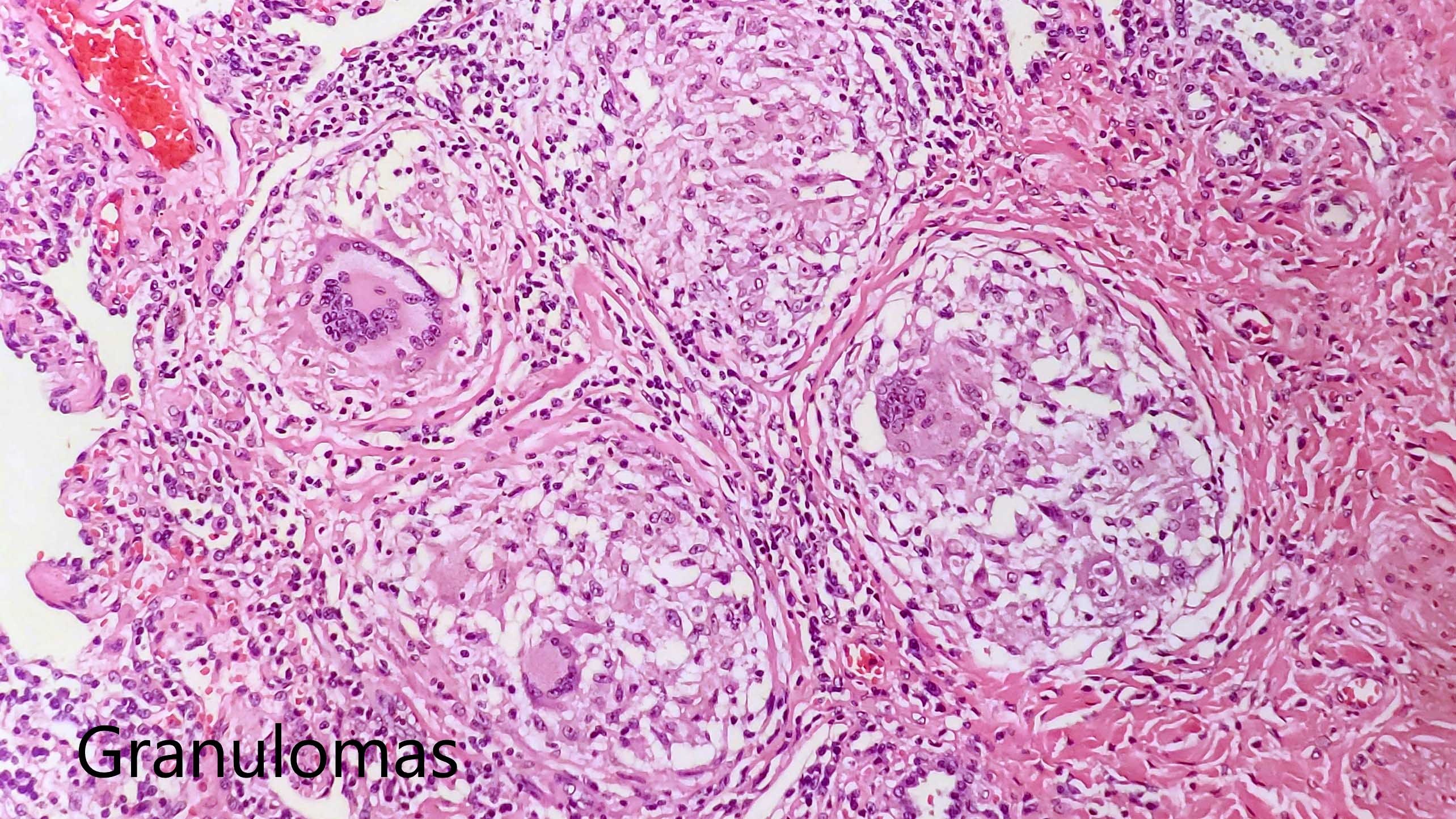
- Well circumscribed granulomas that may coalesce to form large nodules
- Typically nonnecrotizing
- Multinucleated giant cells are common and may contain cytoplasmic inclusions (e.g., asteroid bodies or Schaumann bodies)
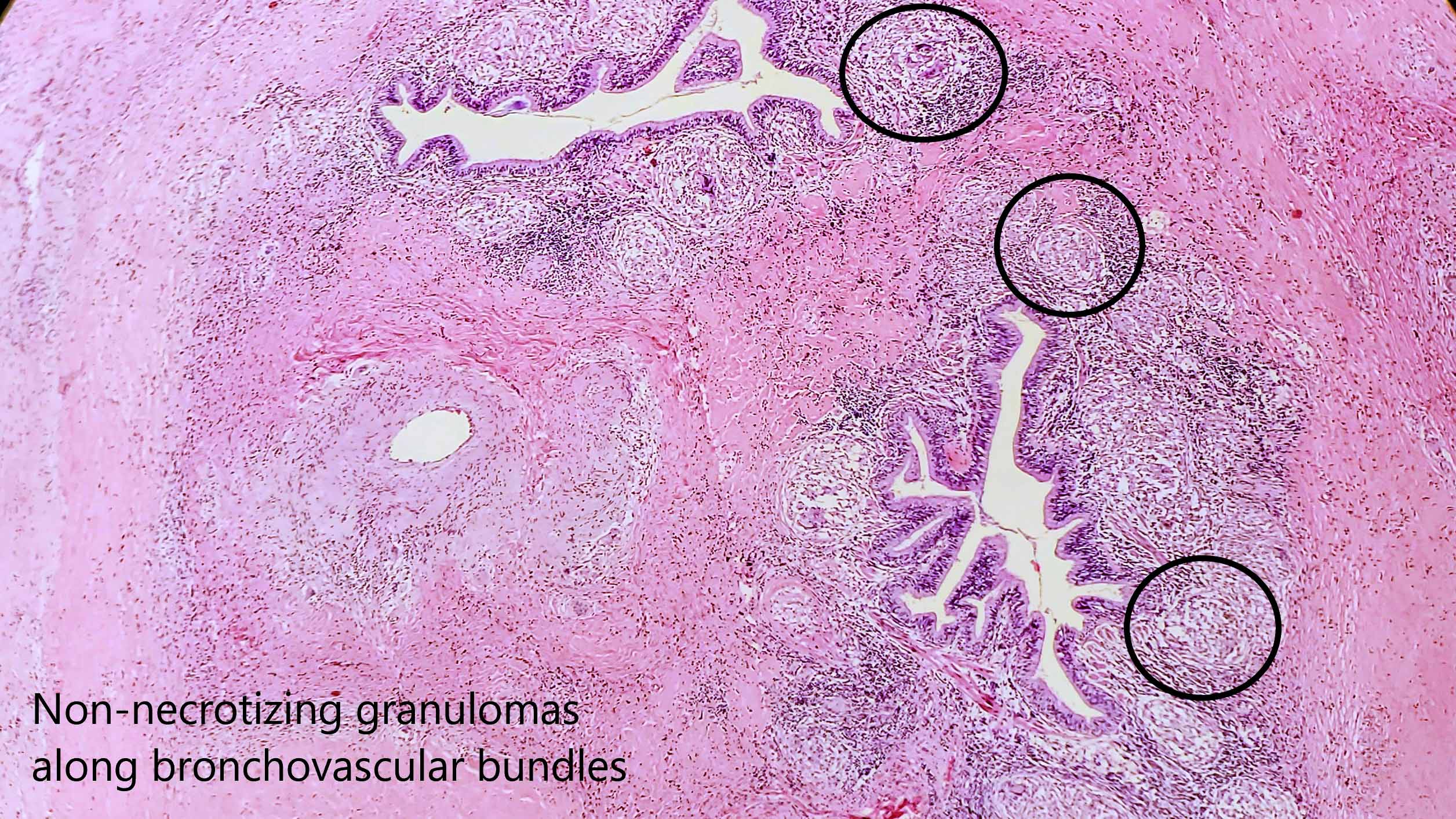
- Distribution is submucosal and perilymphatic (along bronchovascular structures, intralobular septa and occasionally, the pleura)
- Involvement of lung parenchymal or larger vessels may be seen
- Lymphoplasmacytic infiltrate is variably present surrounding the sarcoid granulomas
- Variable degrees of associated fibrosis are often present and can be extensive, especially in longstanding disease
- Asteroid bodies and Schauman bodies are characteristic but not pathognomonic
- Asteroid body: stellate cytoplasmic inclusion with peripheral clearing
- Schaumann (conchoidal) body: cytoplasmic inclusion composed of concentric calcifications
- References: JAMA 2022;327:856, Am J Respir Crit Care Med 2020;201:e26
Microscopic (histologic) images
Contributed by Aliya N. Husain, M.D. and @AKhannaMBBS on Twitter
Multinulceated giant cells and fibrosis
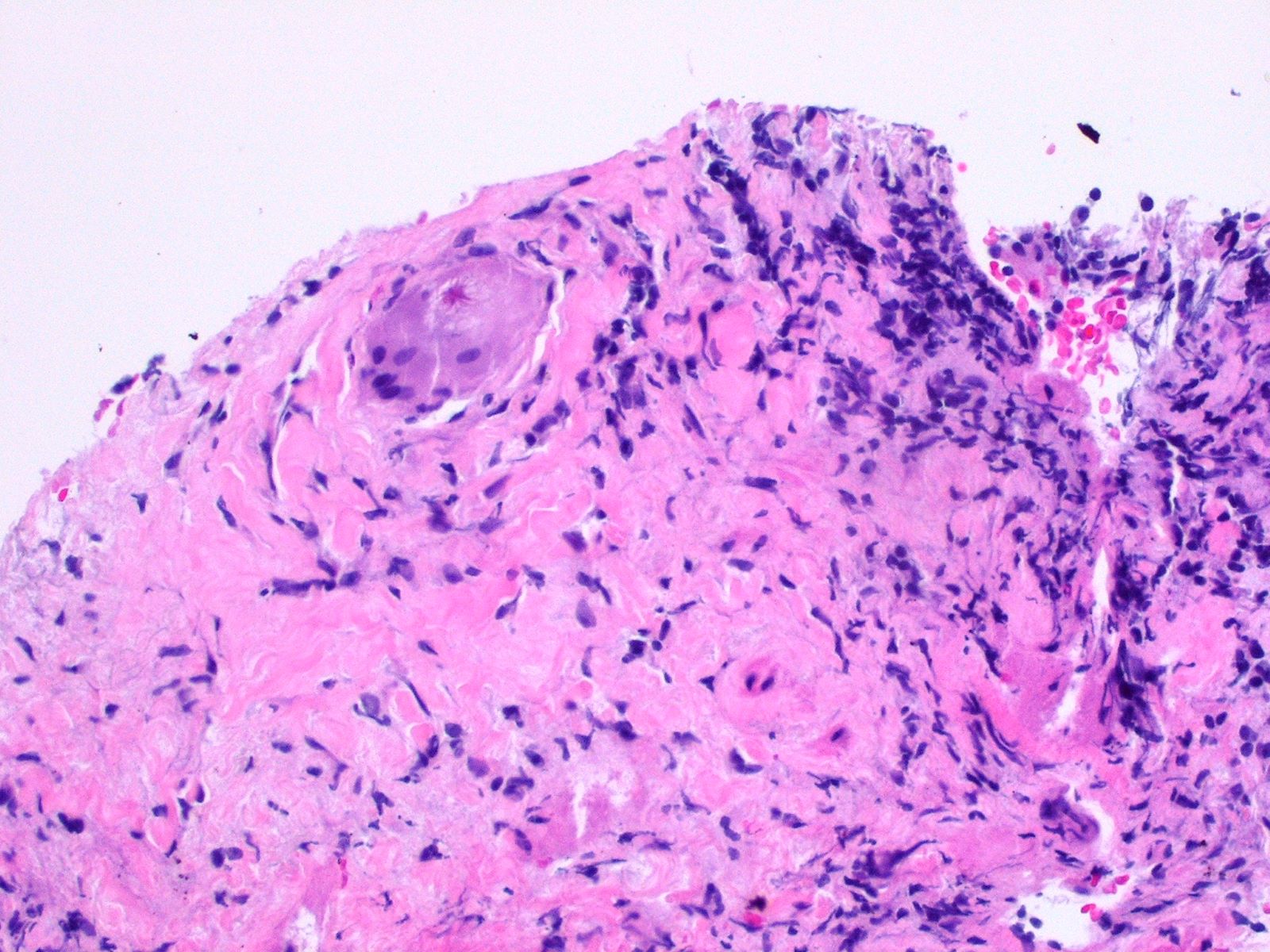
Granuloma with asteroid body
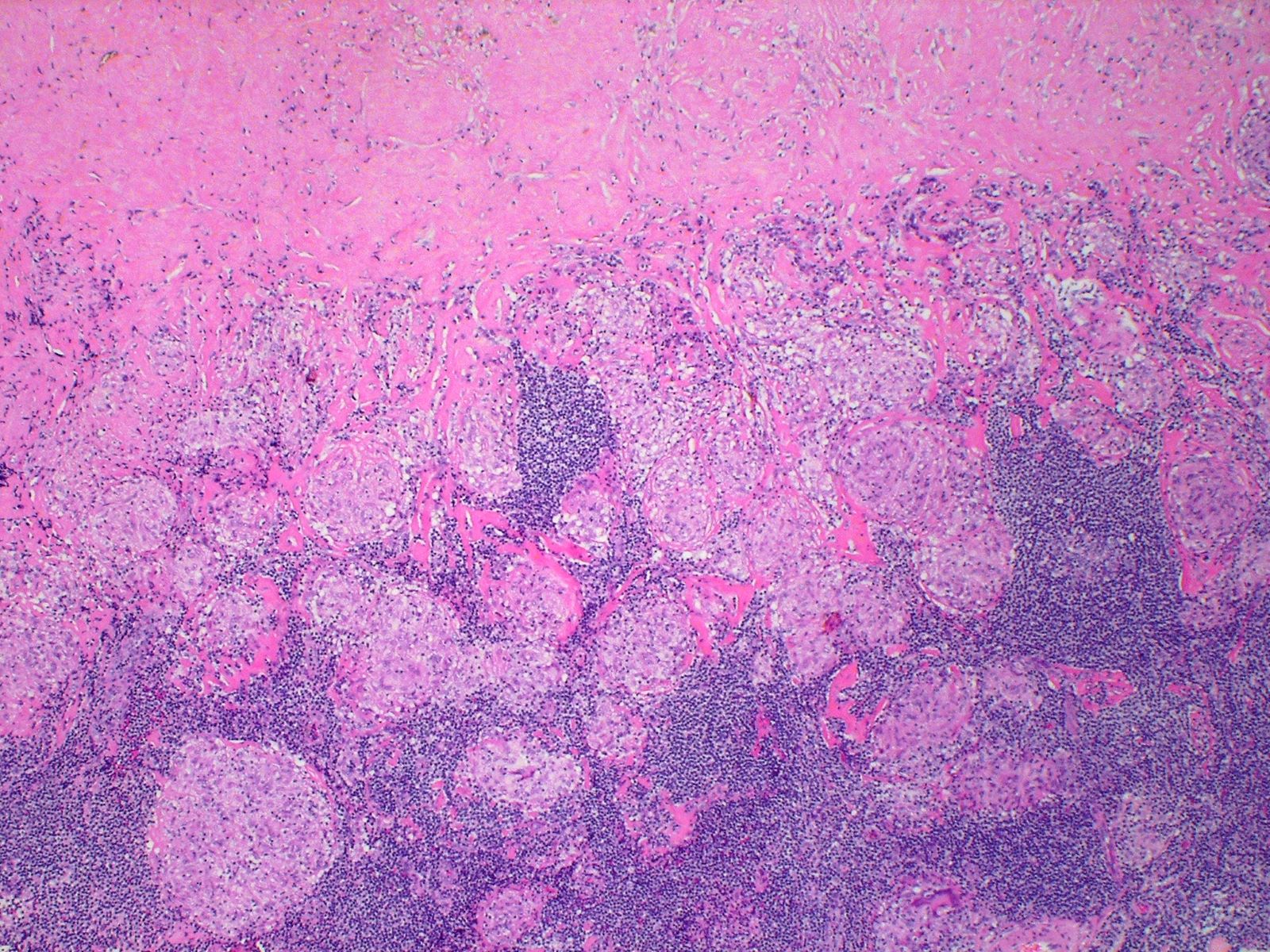
Mediastinal node with granulomas and fibrosis
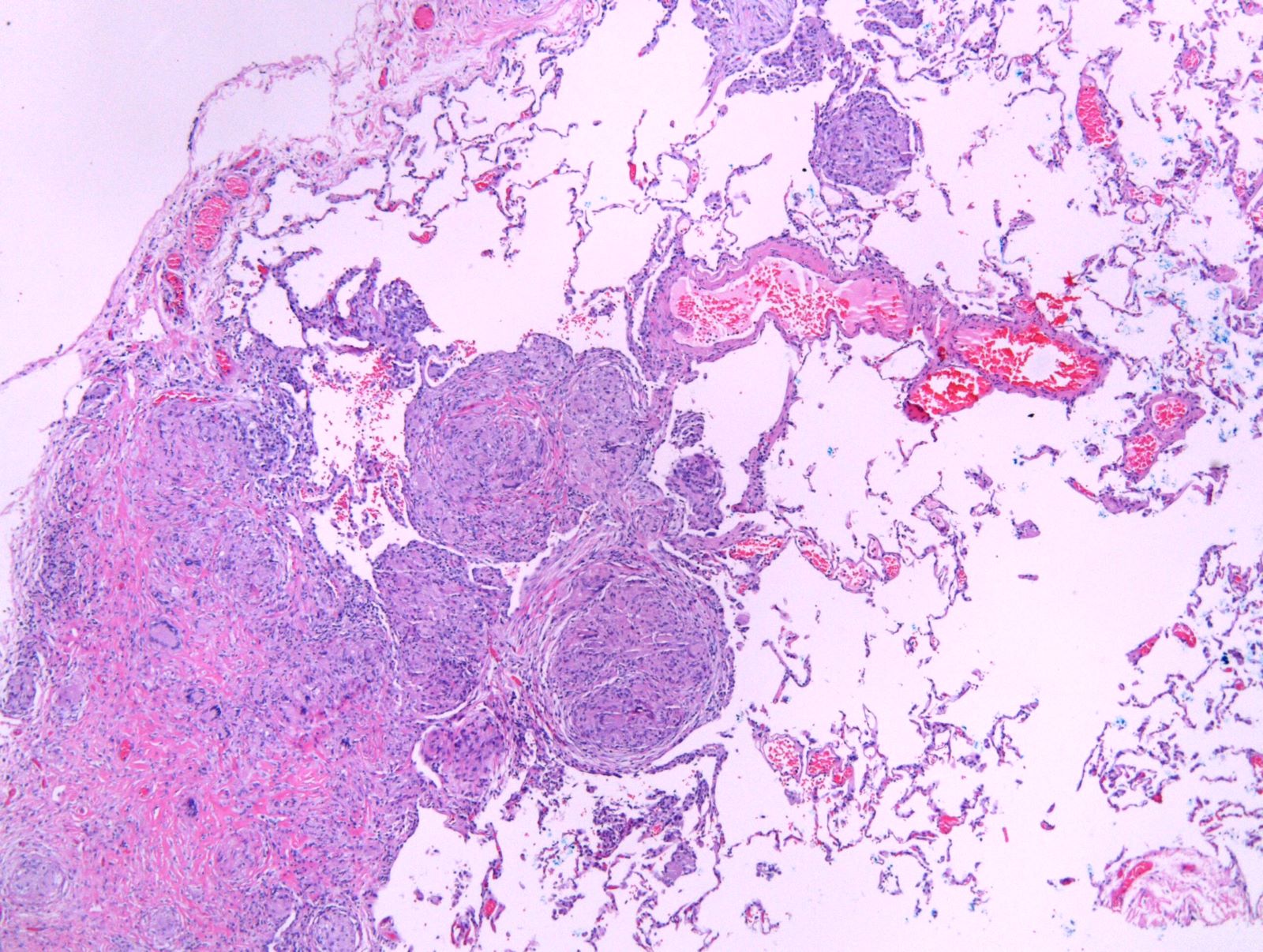
Granulomas of bronchovascular bundle and pleura
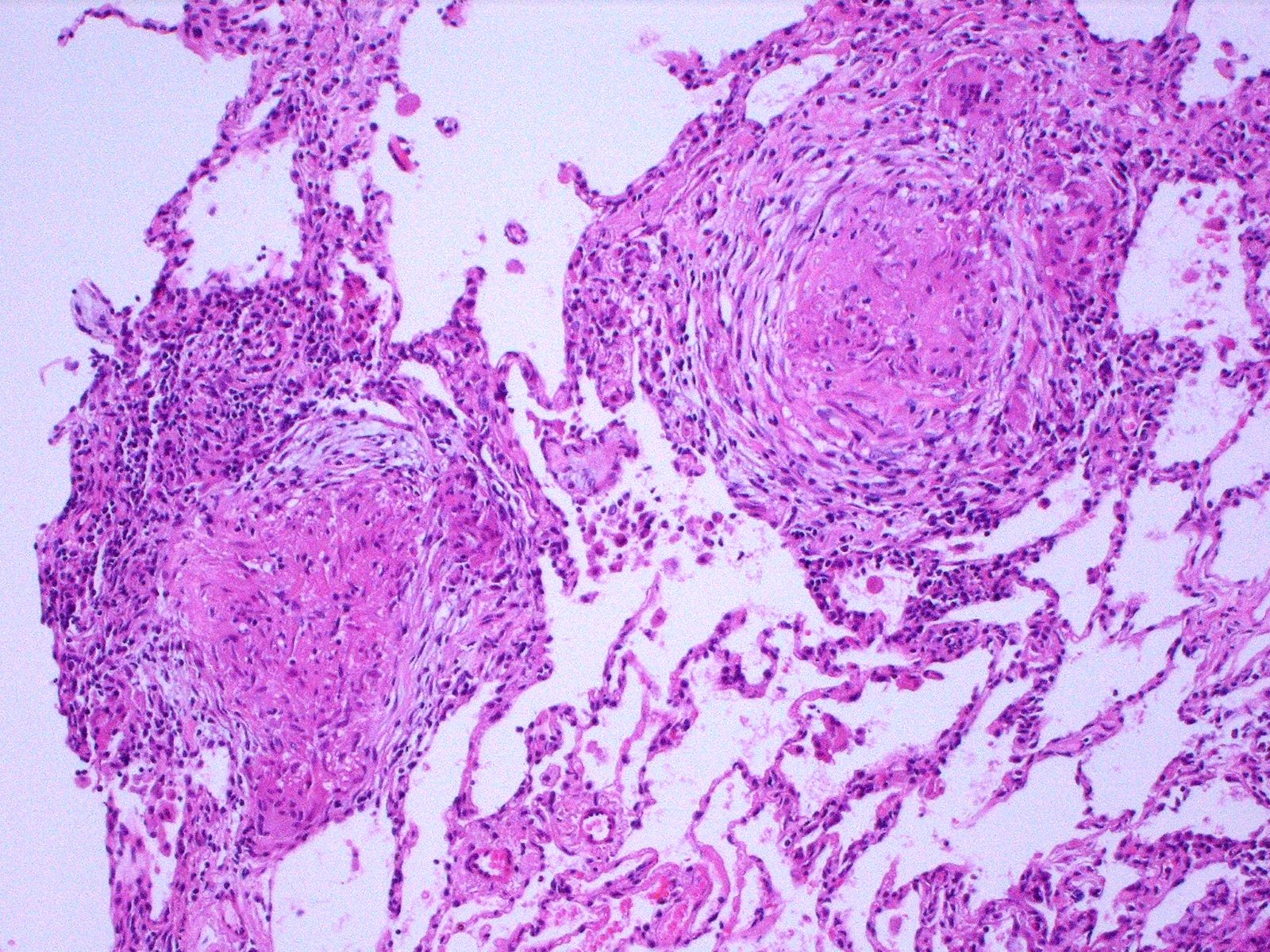
Granulomas with fibrosis
Sarcoidosis
Cytology description
- Epithelioid histiocytes with curved, often boomerang shaped nuclei; characteristically present in a syncytium
- Fibrotic granulomas may be hypocellular
Sample pathology report
- Lung, left upper lobe, wedge biopsy:
- Numerous well formed granulomas, consistent with sarcoidosis (see comment)
- Comment: The specimen shows numerous well formed granulomas, which demonstrate a predominantly bronchovascular and submucosal distribution and show associated fibrosis. Several associated multinucleated giant cells are present. The patient's clinical history and radiographic findings (hilar adenopathy and perilymphatic nodularity) are noted.
Differential diagnosis
- Berylliosis:
- Diagnosis requires clinical history of exposure
- Infectious causes (fungi, atypical mycobacteria):
- Foreign body granulomas:
- Polarization can aid in identifying foreign bodies; however, polarizing material may occasionally be present in giant cells of sarcoidosis
Additional references
Board review style question #1
A 55 year old woman with clinically suspected sarcoidosis undergoes biopsy of mediastinal lymph nodes and wedge biopsy of involved lungs. Which of the following findings are most consistent with sarcoidosis?
- Lungs with poorly formed granulomas along the bronchovascular structures and lymph nodes with granulomatous lesions containing refractile material
- Lungs with poorly formed interstitial granulomas and lymph nodes with granulomatous lesions containing refractile material
- Lungs with well formed granulomas along bronchovascular structures and pleura and lymph nodes with well formed granulomas
- Lungs with well formed interstitial granulomas with refractile material and lymph nodes with reactive changes
Board review style answer #1
C. Lungs with well formed granulomas along bronchovascular structures and pleura and lymph nodes with well formed granulomas. Answers A, B and D are incorrect because sarcoid associated granulomas tend to be well formed and typically do not contain foreign material including refractile particles.
Comment Here
Reference: Sarcoidosis
Comment Here
Reference: Sarcoidosis
Board review style question #2
The image above shows a mediastinal lymph node biopsy in a patient whose CT findings include mediastinal and hilar opacities as well as micronodularity of perilymphatic and bronchocentric distribution. What is the most likely diagnosis and which stains should be performed on the biopsy prior to signout?
- Diagnosis: infectious process; stains: Gram stain, AFB
- Diagnosis: infectious process; stains: trichrome, Gram stain
- Diagnosis: sarcoidosis; stains: AFB, GMS
- Diagnosis: silicosis; stains: AFB, GMS
Board review style answer #2
C. Diagnosis: sarcoidosis; stains: AFB, GMS. This section demonstrates a lymph node with multiple well formed, nonnecrotizing granulomas as well as fibrosis. These findings are characteristic of sarcoidosis. Answer D is incorrect because no fine particulate is seen, which makes silicosis less likely. Answers A and B are incorrect because the differential for granulomatous inflammation also includes infectious processes including fungal and atypical mycobacterial infections and GMS and AFB should be performed on all pulmonary / mediastinal lymph node specimens with granulomas. Negative special stains do not rule out this possibility; if clinical suspicion is high and special stains and cultures are negative, RNA sequencing may be considered to more definitively rule out infectious etiology. Remember that sarcoidosis is a diagnosis of exclusion.
Comment Here
Reference: Sarcoidosis
Comment Here
Reference: Sarcoidosis
