
Liver & intrahepatic bile ducts
Other malignancies
Infantile hemangioendothelioma / hemangioma
Author: Deepali Jain, M.D.

Last author update: 1 February 2012
Last staff update: 19 March 2024 (update in progress)
Copyright: 2004-2024, PathologyOutlines.com, Inc.
PubMed search: Infantile hemangioendothelioma OR infantile hemangioma liver
Table of Contents
Definition / general | Clinical features | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Differential diagnosisCite this page: Jain D. Infantile hemangioendothelioma / hemangioma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/livertumorIHE.html. Accessed April 26th, 2024.
Definition / general
- Most common hepatic mesenchymal tumor in childhood (20% of all pediatric hepatic tumors)
Clinical features
- 90% are < 6 months old at diagnosis, slight female predominance
- 10 - 40% have coexisting cutaneous cavernous hemangiomas
- 50% are incidental findings at autopsy
- Symptoms: hepatic mass (48%), high output cardiac failure due to shunting through tumor (15%); also Kasabach-Merritt syndrome (bleeding diathesis due to platelet sequestration and severe thrombocytopenia); may be asymptomatic
- Associations: chromosomal abnormalities, developmental abnormalities, hemangiomas, mesenchymal hamartoma, Wilms tumor (Virchows Arch A Pathol Anat Histopathol 1988;413:463)
Laboratory
- Normal AFP (usually), rarely elevated due to secretion from entrapped or nearby hepatocytes (Hum Pathol 2010;41:763)
Radiology description
- Xray: multiple small nodules
Prognostic factors
- Poor prognostic factors: congestive heart failure, jaundice, multiple nodules, lack of cavernous differentiation
- 70% survival (almost always have benign behavior)
- Deaths (when they occur) are usually within 1 month of diagnosis and due to congestive heart failure or platelet consumption leading to bleeding diathesis or massive hemoperitoneum
Case reports
- Newborn with 5.6 cm hepatic mass (Case of the Week #432)
- 56 year old woman with breast DCIS and liver mass (Arch Pathol Lab Med 2001;125:931)
- With pulmonary metastases (J Pediatr Surg 2006;41:e49)
Treatment
- Spontaneous involution in 5 - 10% at 6 - 8 months; resection if solitary, otherwise steroids, interferon, radiation therapy, embolization or transplantation (World J Surg 2009;33:597)
Gross description
- Solitary or multiple, mean 4 cm (range 0.1 to 15 cm) and circumscribed but not encapsulated
- White red tan, soft and spongy
- Larger nodules may have hemorrhagic, fibrotic or calcified central areas
Microscopic (histologic) description
- Well demarcated or infiltrative (35%)
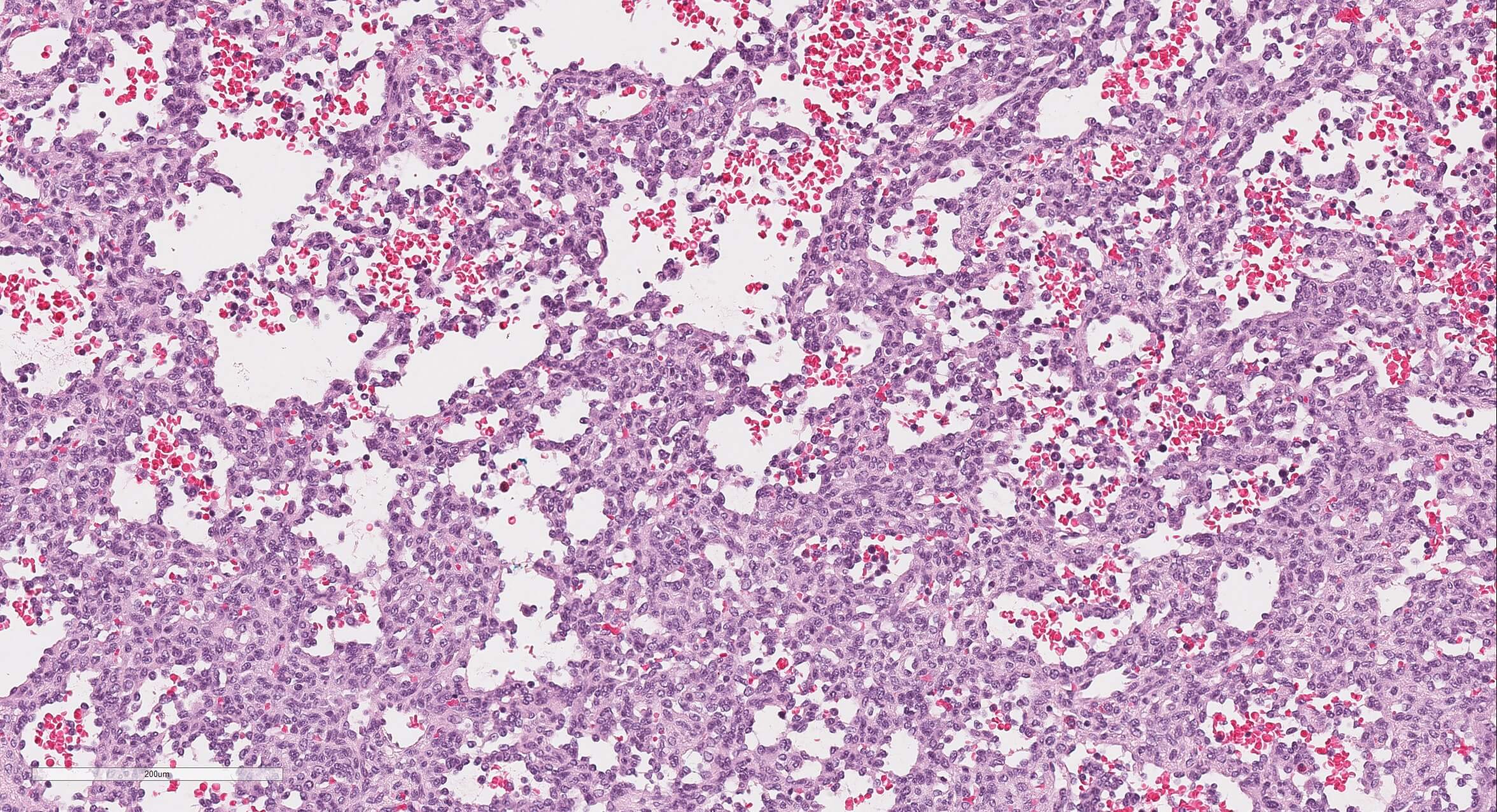
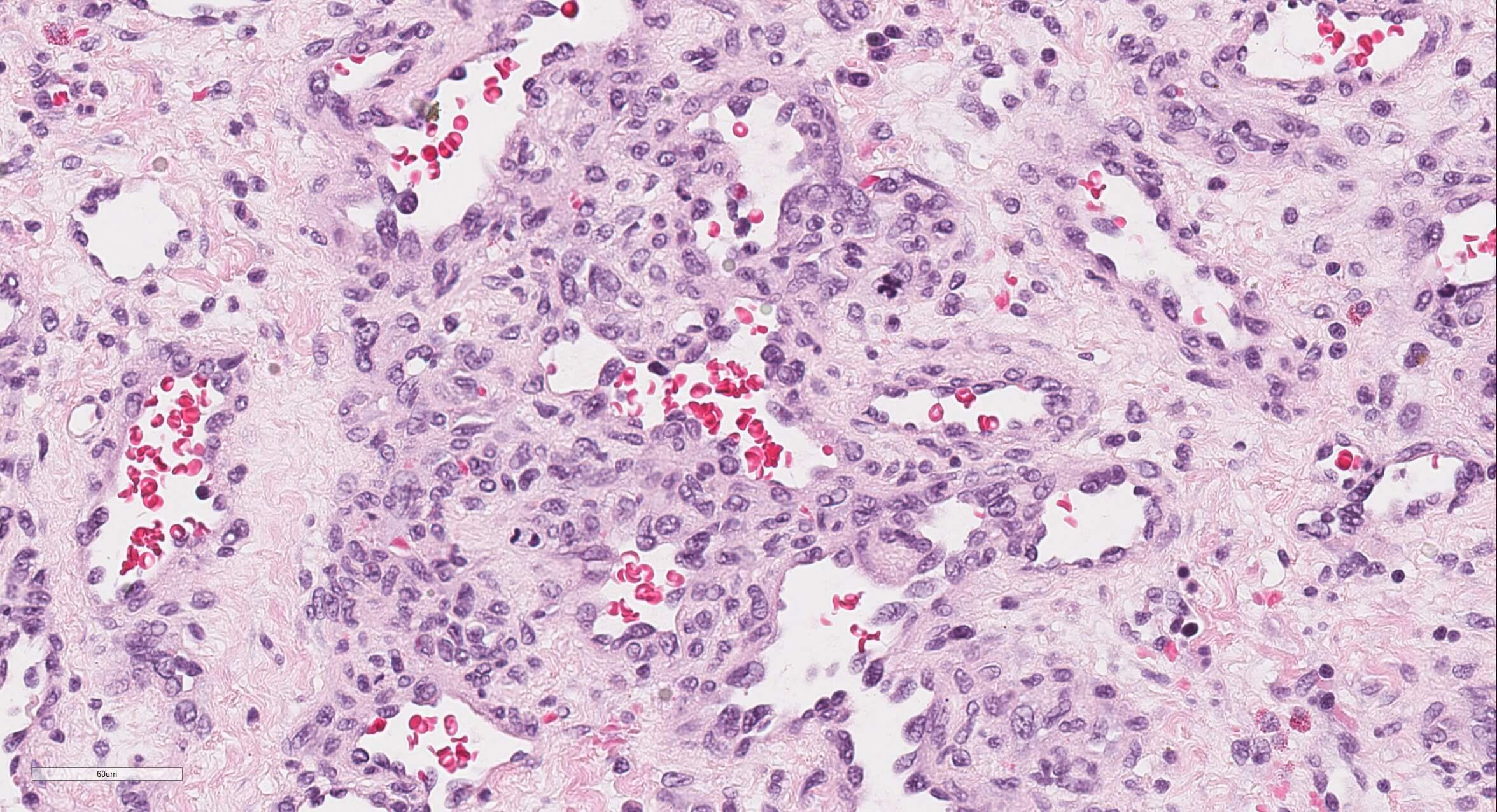
- Pure type 1 change: 80%, orderly proliferation of small, capillary-like vascular spaces, relatively bloodless, may be dilated (particularly centrally) and slightly irregular; lined by bland or plump endothelial cells that may occlude the lumen; vascular channels separated by variable connective tissue; may have interspersed small bile ducts; extramedullary hematopoiesis in 60%, often in vascular lumina; often trapped hepatocytes at periphery; large lesions show thrombosis, fibrosis, myxoid change and calcification; no / rare mitotic figures and no malignant spindle cell component
- Type 2 change: equivalent to angiosarcoma (with aggressive behavior) with irregular branching vascular structures lined by pleomorphic, hyperchromatic endothelial cells, frequent mitotic activity
Microscopic (histologic) images
Case #432
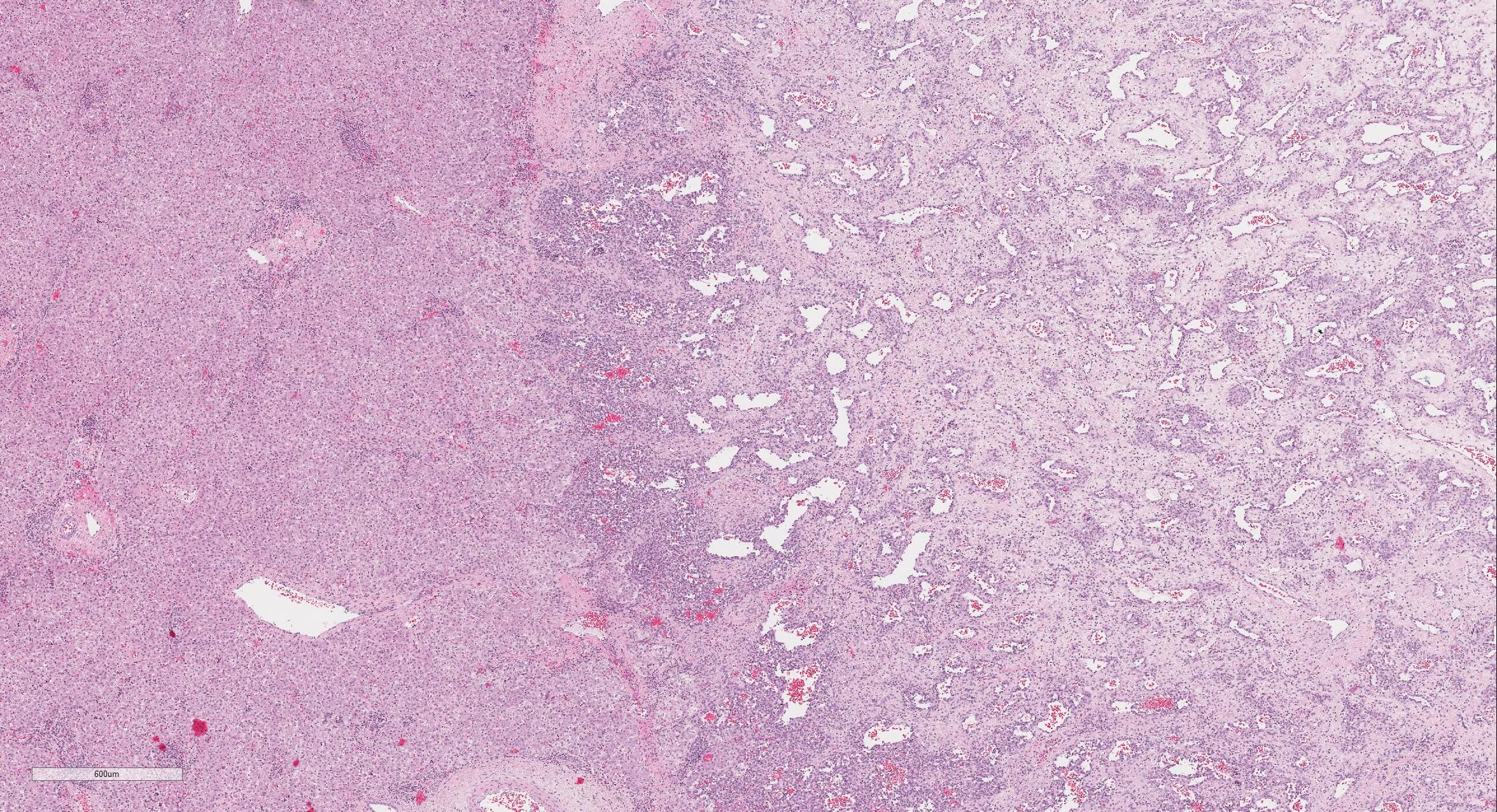
4x
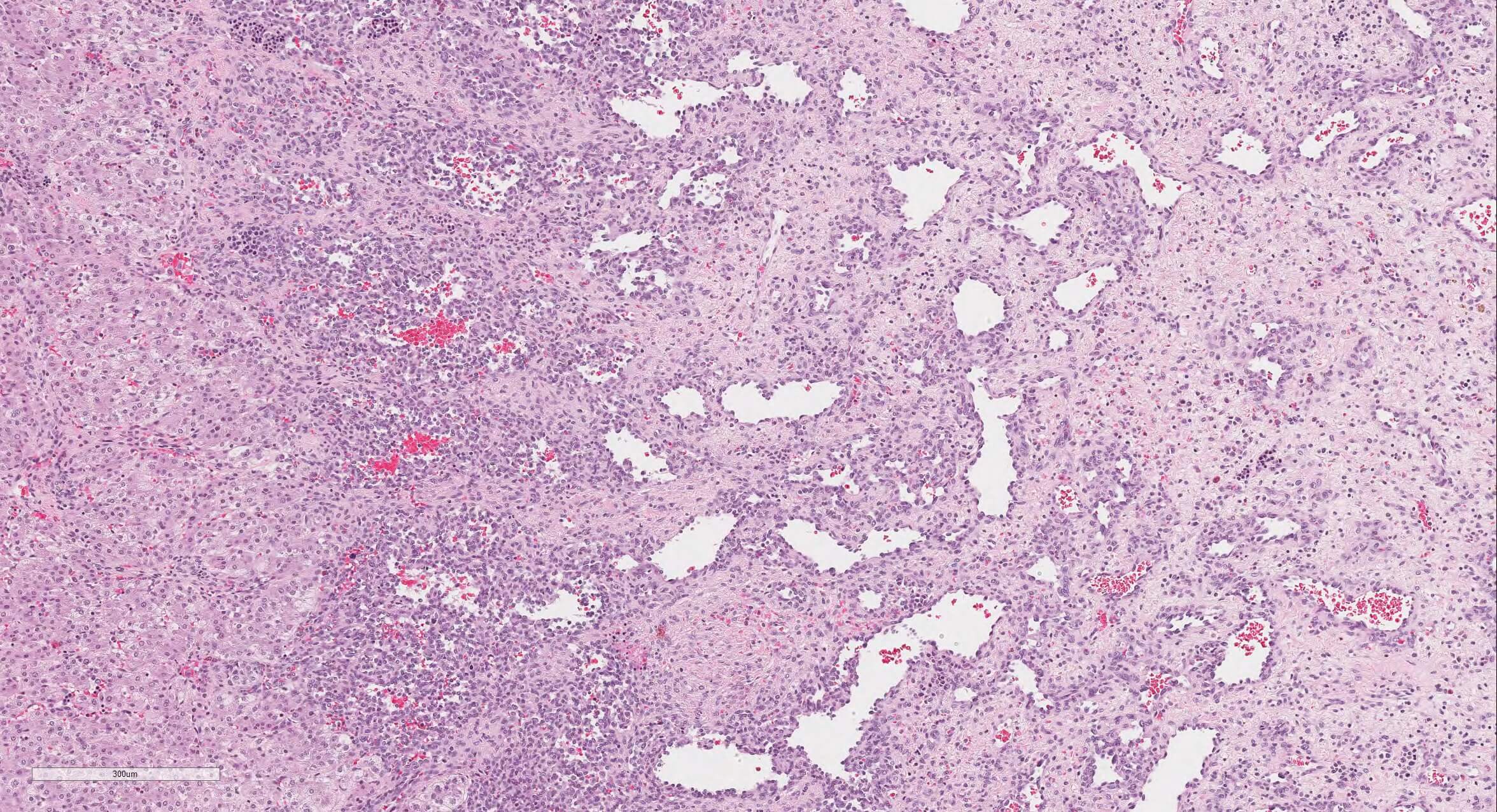
10x
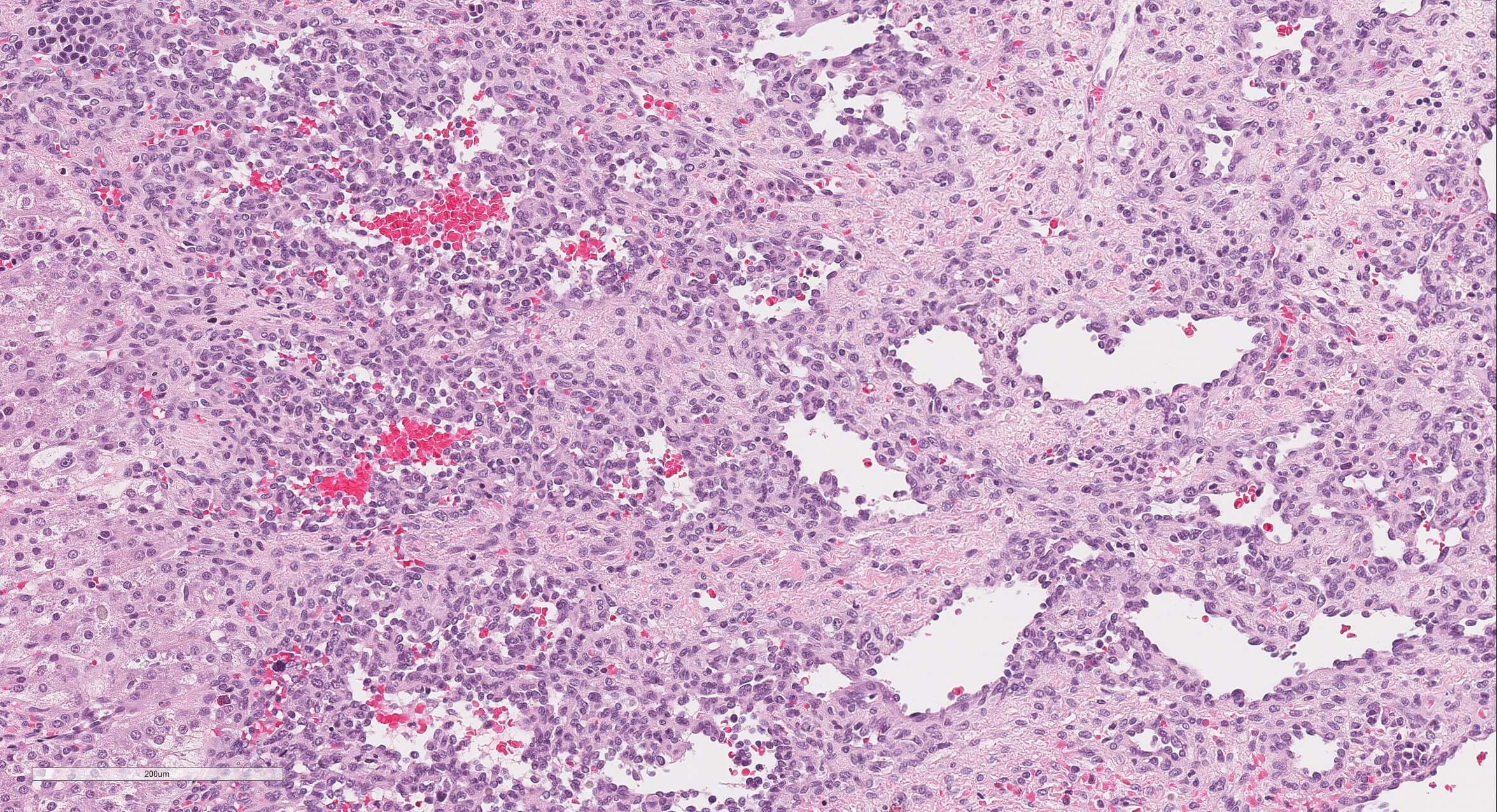
20x
20x
40x
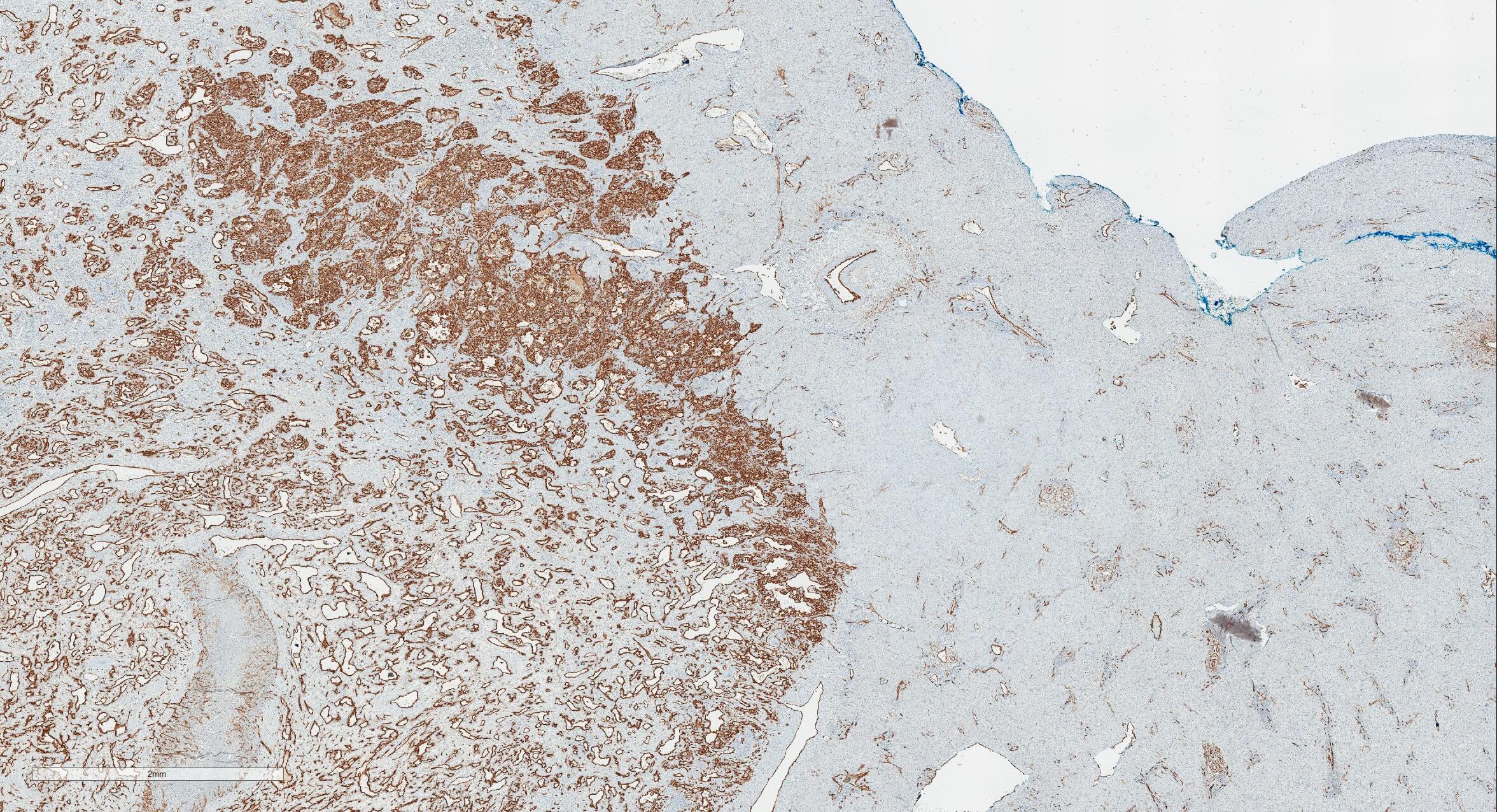
CD34 2x
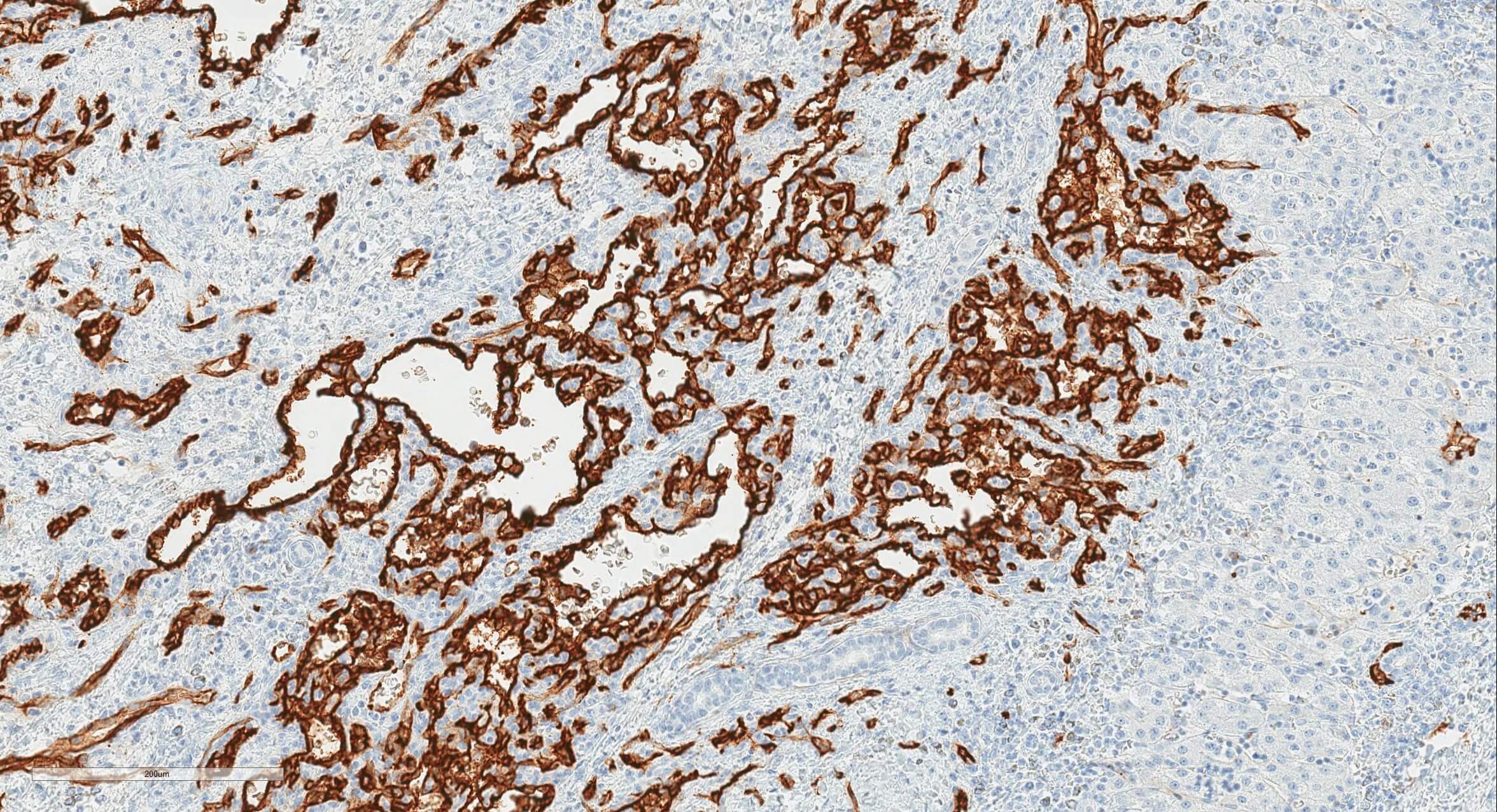
CD34 20x
Positive stains
Differential diagnosis
- Angiosarcoma:
- Adequate sampling is important; has solid sarcomatous areas, vascular and sinusoidal permeation, marked pleomorphism
- May have history of exposure to toxins
- Cavernous hemangioma:
- Less common in children
- Lacks peripheral small vascular proliferation
- Epithelioid hemangioendothelioma:
- Intracellular vascular lumina containing RBCs
- Hepatic vascular malformation with capillary proliferation:
- Typically single large mass, malformed, irregular large vessels and GLUT1-
- Mesenchymal hamartoma:
- Primitive mesenchymal stroma, not a vascular tumor
