
Liver & intrahepatic bile ducts
Other malignancies
Epithelioid hemangioendothelioma
Authors: Tom Liang, M.D., Shefali Chopra, M.D.
Editorial Board Member: Catherine E. Hagen, M.D.
Deputy Editor-in-Chief: Raul S. Gonzalez, M.D.


Last author update: 5 November 2020
Last staff update: 19 September 2023
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Epithelioid hemangioendothelioma liver


Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Frozen section description | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Electron microscopy images | Molecular / cytogenetics description | Molecular / cytogenetics images | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Liang T, Chopra S. Epithelioid hemangioendothelioma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/livertumorEHE.html. Accessed March 30th, 2025.
Definition / general
- Epithelioid hemangioendothelioma (EHE) is a malignant vascular tumor composed of epithelioid cells within a distinctive myxohyaline stroma
Essential features
- Rare malignant vascular neoplasm composed of epithelioid endothelial cells in a background of myxohyaline stroma
- Often presents as multifocal disease in the liver; may be confused for metastatic disease
- Most cases characterized by presence of WWTR1-CAMTA1 gene fusion, subset of cases characterized by YAP1-TFE3 fusion
ICD coding
- ICD-O: 9133/3 - epithelioid hemangioendothelioma, malignant
- ICD-11: 2B5Y & XH9GF8 - other specified malignant mesenchymal neoplasms; epithelioid hemangioendothelioma, NOS
Epidemiology
- Mostly affects middle aged adults (30 - 50 years); rare in children
- Incidence slightly F > M (Cancer 1999;85:562)
Sites
- Soft tissue, visceral organs (liver and lung), bone
- Often presents as multifocal disease in liver
- Some patients present with both liver and lung or spleen involvement
Etiology
- Sporadic
Clinical features
- Often discovered incidentally in the liver
- Most cases asymptomatic
- May present with abdominal discomfort, weight loss
- Rare cases may present with hemoperitoneum and may cause noncirrhotic portal hypertension
- Multifocal involvement of both left and right hepatic lobes seen in up to 87% of patients (Transplantation 2017;101:555)
- Extrahepatic disease seen in 37% of patients (Transplantation 2017;101:555)
Diagnosis
- Made on biopsy (preferable) or cytology specimen
Radiology description
- Radiological findings variable
- Ultrasound: hypoechoic nodules
- CT: hypodense nodules
- MRI: in 30% of cases, the nodules have targetoid appearance with low signal intensity on T1; high signal intensity on T2 called bright dark sign
- References: Case Rep Gastroenterol 2020;14:56, Case Rep Gastrointest Med 2019;2019:7530845
Radiology images
Images hosted on other servers:

CT, multifocal EHE

CT, peripheral enhancement
Prognostic factors
- Variable clinical course (ranges from stable / indolent disease to progressive with metastasis)
- Distant metastatic rate is 20 - 30%
- Better prognosis than angiosarcoma of the liver
- Histological features do not reliably predict outcome but increased cellularity and necrosis may be poor prognostic factors (Cancer 1999;85:562)
Case reports
- 25 year old man with multifocal EHE treated successfully with liver transplant (Clin Case Rep 2019;8:108)
- 30 year old man with Crohn's disease presenting with multifocal EHE (Case Rep Gastroenterol 2020;14:56)
- 33 and 62 year old men with metastatic hepatic EHE treated with doxorubicin & olaratumab (Ther Clin Risk Manag 2020;16:141)
- 65 year old woman with YAP1-TFE3 rearranged hepatic EHE (Case Rep Gastrointest Med 2019;2019:7530845)
- 74 year old man with solitary hepatic EHE treated with hepatic resection (Case Rep Gastroenterol 2018;12:402)
Treatment
- Solitary disease: resection (curative)
- Multifocal disease: observation, liver transplantation, chemotherapy
- References: Dig Liver Dis 2020;52:1039, Cancer 2006;107:2108
Gross description
- Can range in size from subcentimeter nodules to large, coalescing masses > 10 cm
- Cut surface is white and firm and can have infiltrative pattern with prominent myxohyaline or fibrous stroma
- Background liver appears normal
- References: Case Rep Gastroenterol 2020;14:56, Case Rep Gastroenterol 2018;12:402
Gross images
Images hosted on other servers:

Multifocal EHE

Unifocal EHE
Frozen section description
- Epithelioid, stellate and spindle cells with fine chromatin with occasional intracytoplasmic vacuoles in myxohyaline stroma
Microscopic (histologic) description
- EHE with WWTR1-CAMTA1 gene fusion
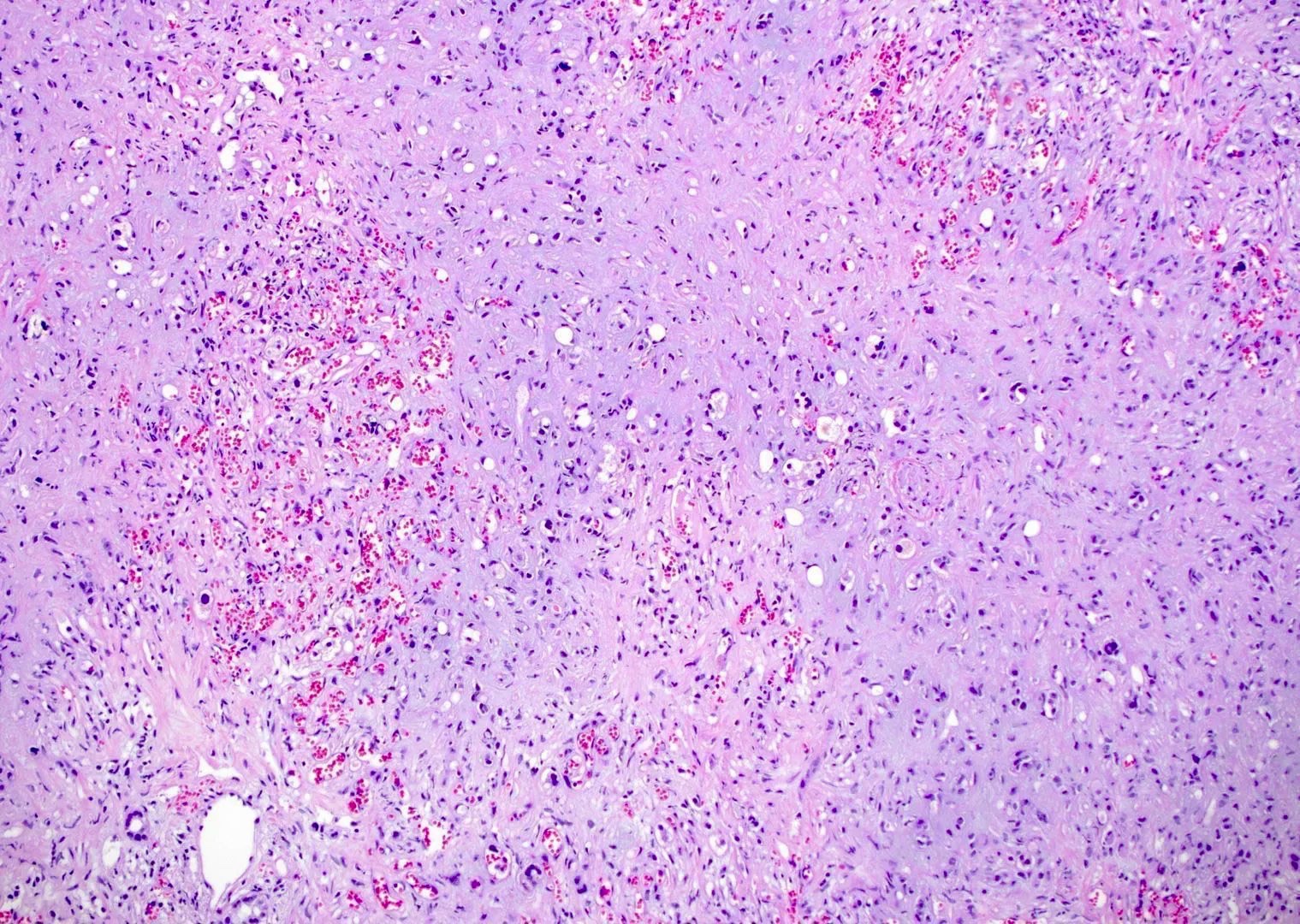
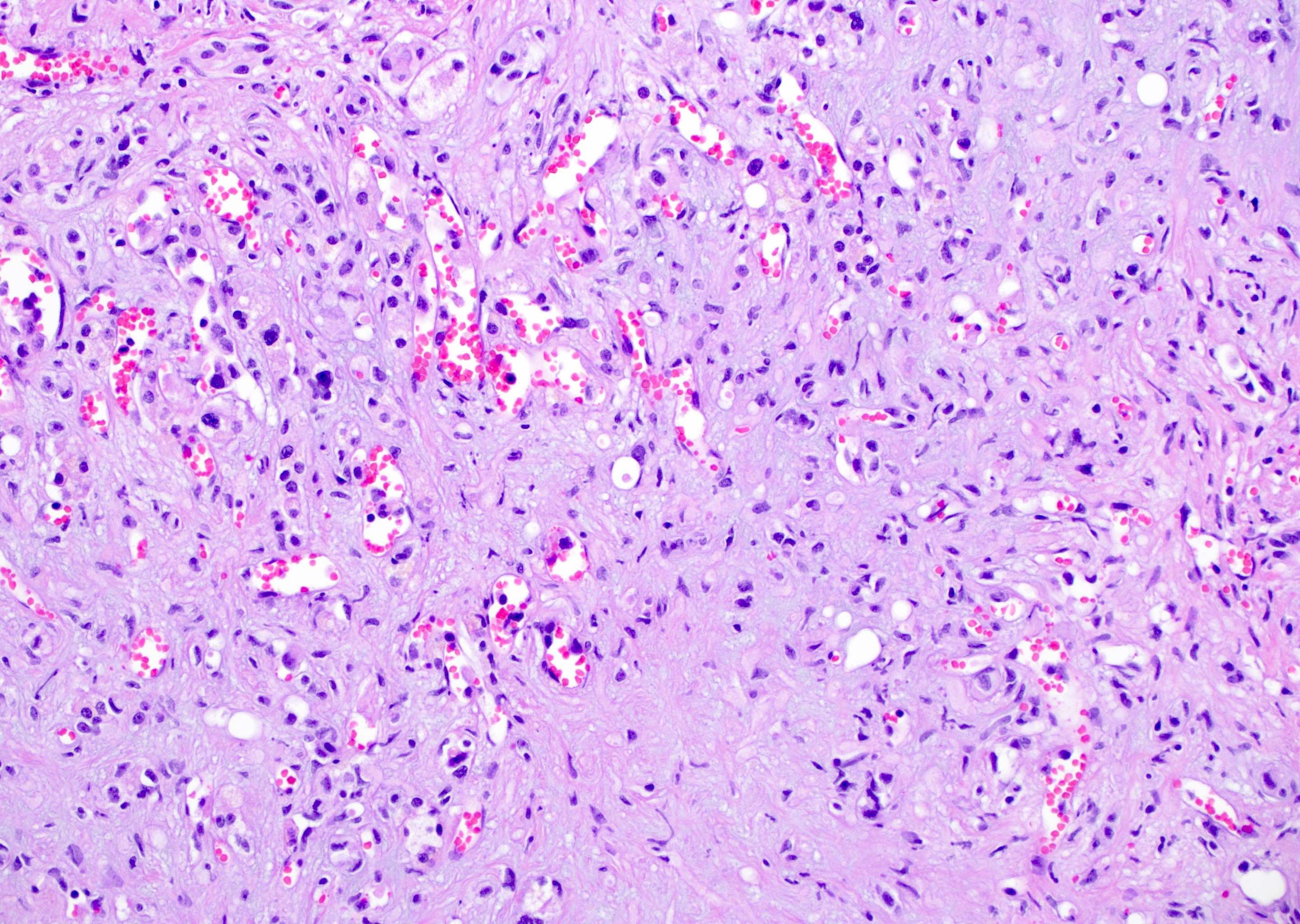
- Cords, nests, solid sheets and single cells with infiltrative growth pattern in myxohyaline / fibrous stroma with increased cellularity at tumor edge
- Invasion of sinusoids, portal and hepatic veins
- No vascular channel formation
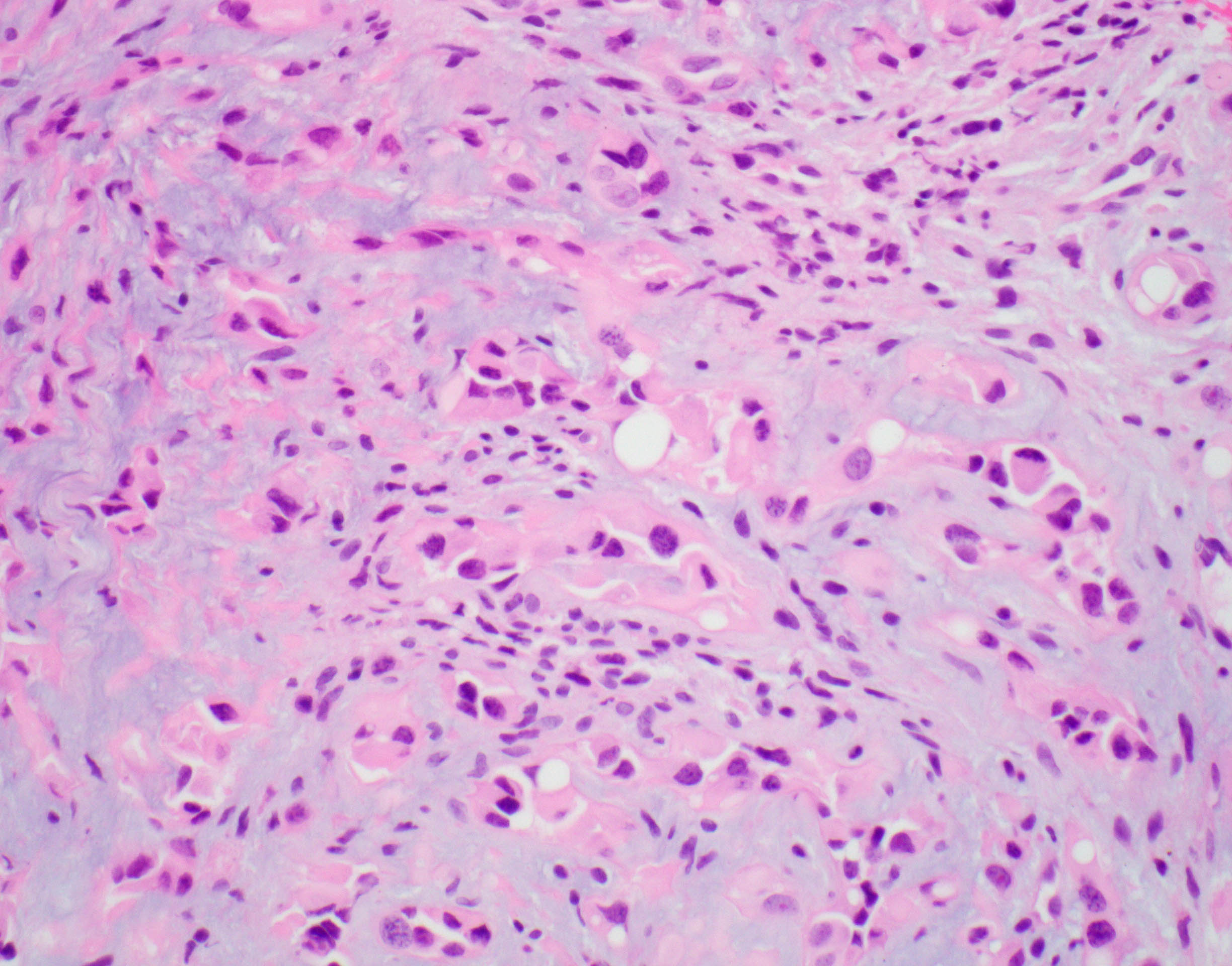
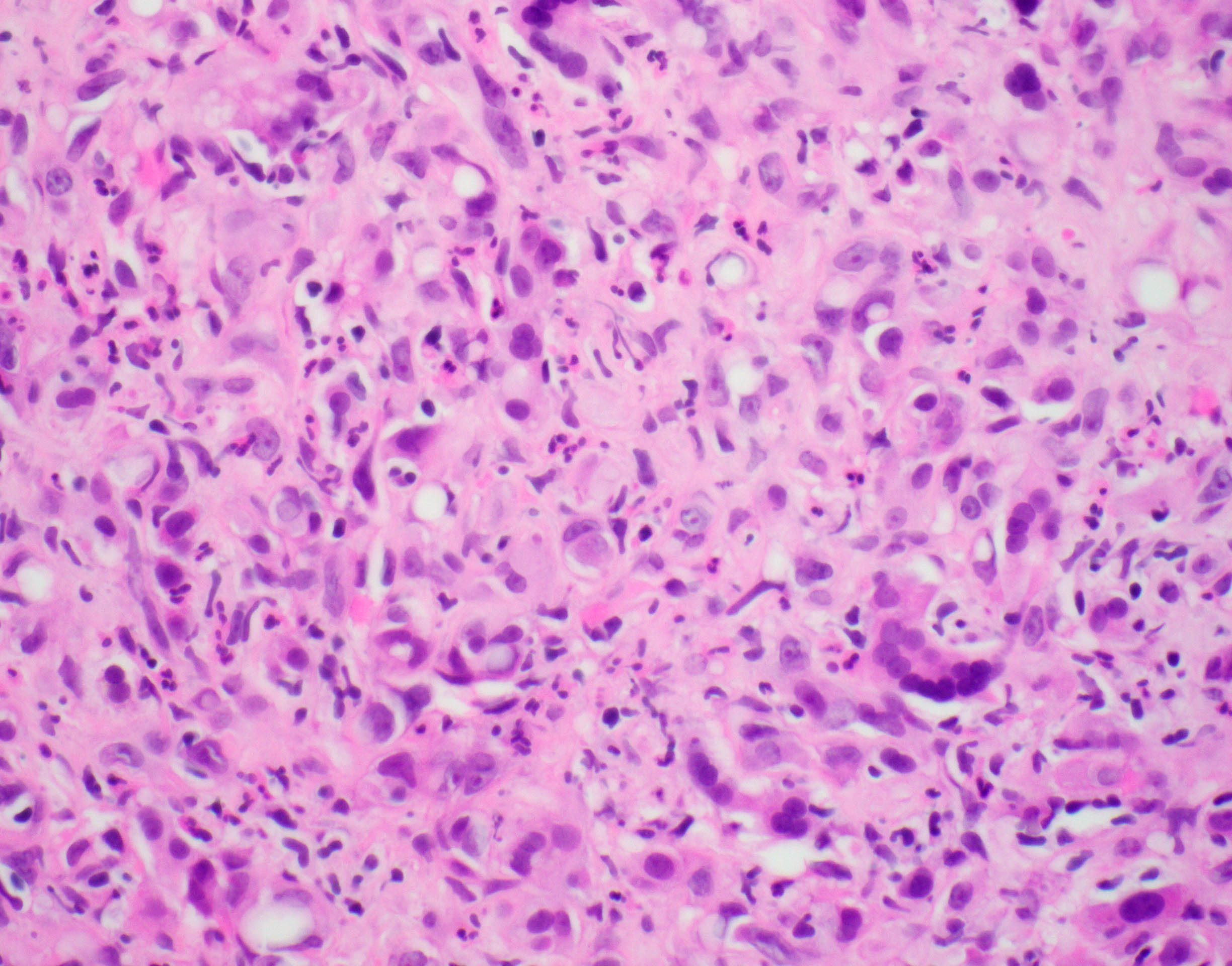
- Cells can be epithelioid, stellate, spindle with fine chromatin
- Eosinophilic cytoplasm with occasional intracytoplasmic vacuoles ("blister cells")
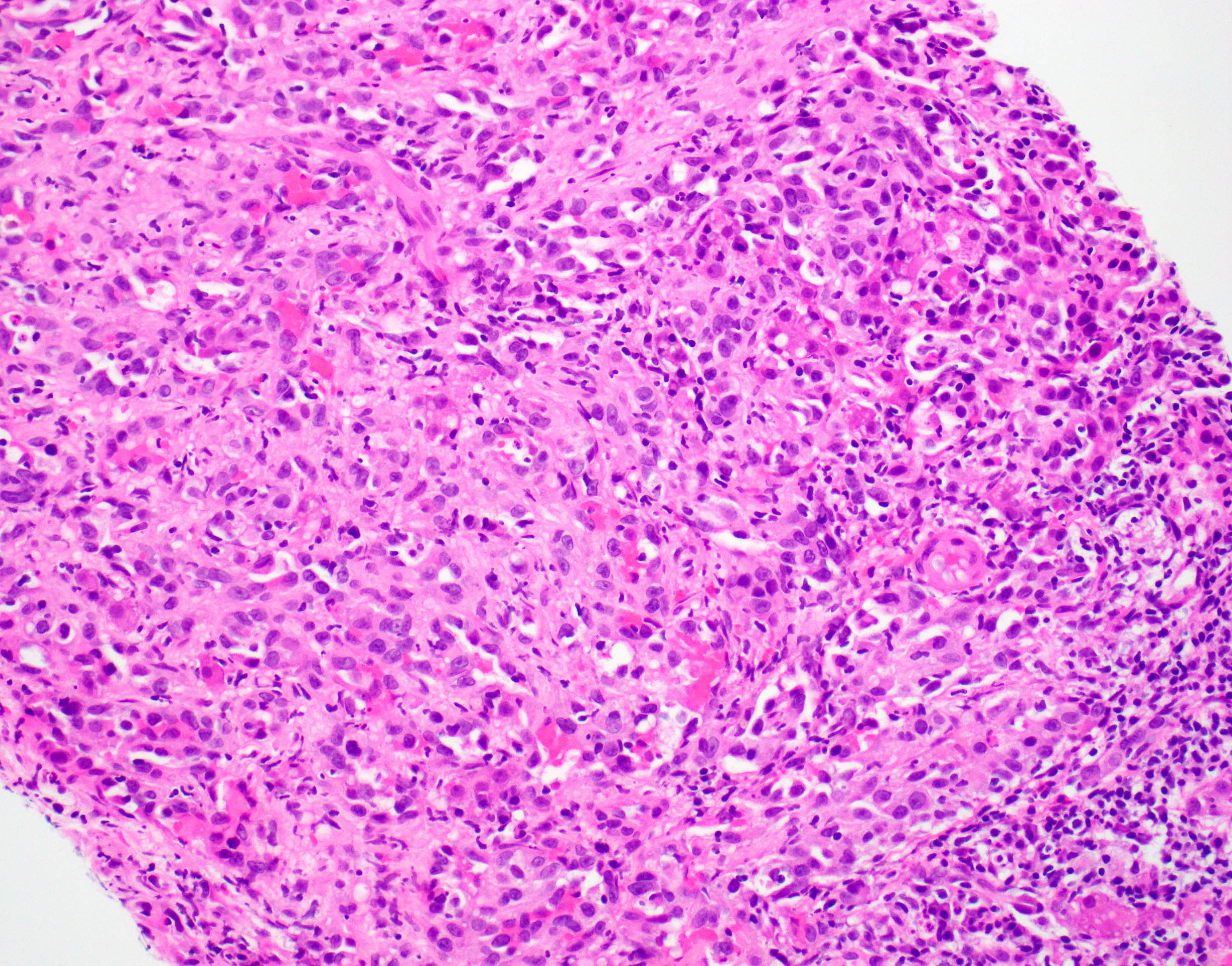
- < 10% can have atypical histological features like nuclear pleomorphism, increased mitotic activity, solid sheet pattern and necrosis
- EHE with YAP1-TFE3 gene fusion (rare in liver)
- Well formed vascular channels and areas of solid growth
- Epithelioid cells with bright eosinophilic cytoplasm
- Lacks the characteristic stromal component seen in classic EHE
- References: Cancer 1982;50:970, Am J Surg Pathol 1997;21:363
Microscopic (histologic) images
Contributed by Shefali Chopra, M.D. and @JMGardnerMD on Twitter
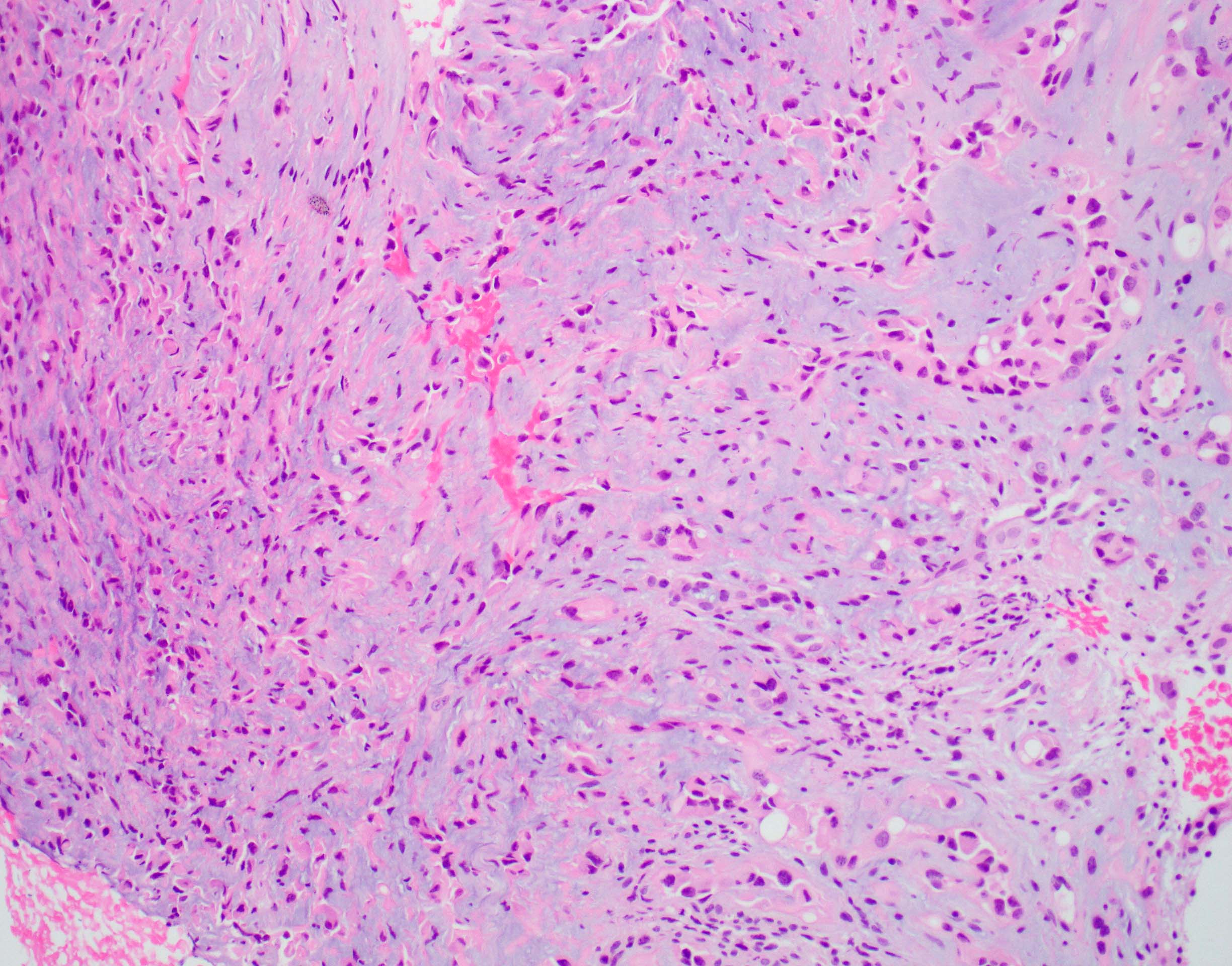
Myxohyaline stroma

Increased cellularity at tumor edge
Cells in small nests and cords
Intracytoplasmic vacuoles
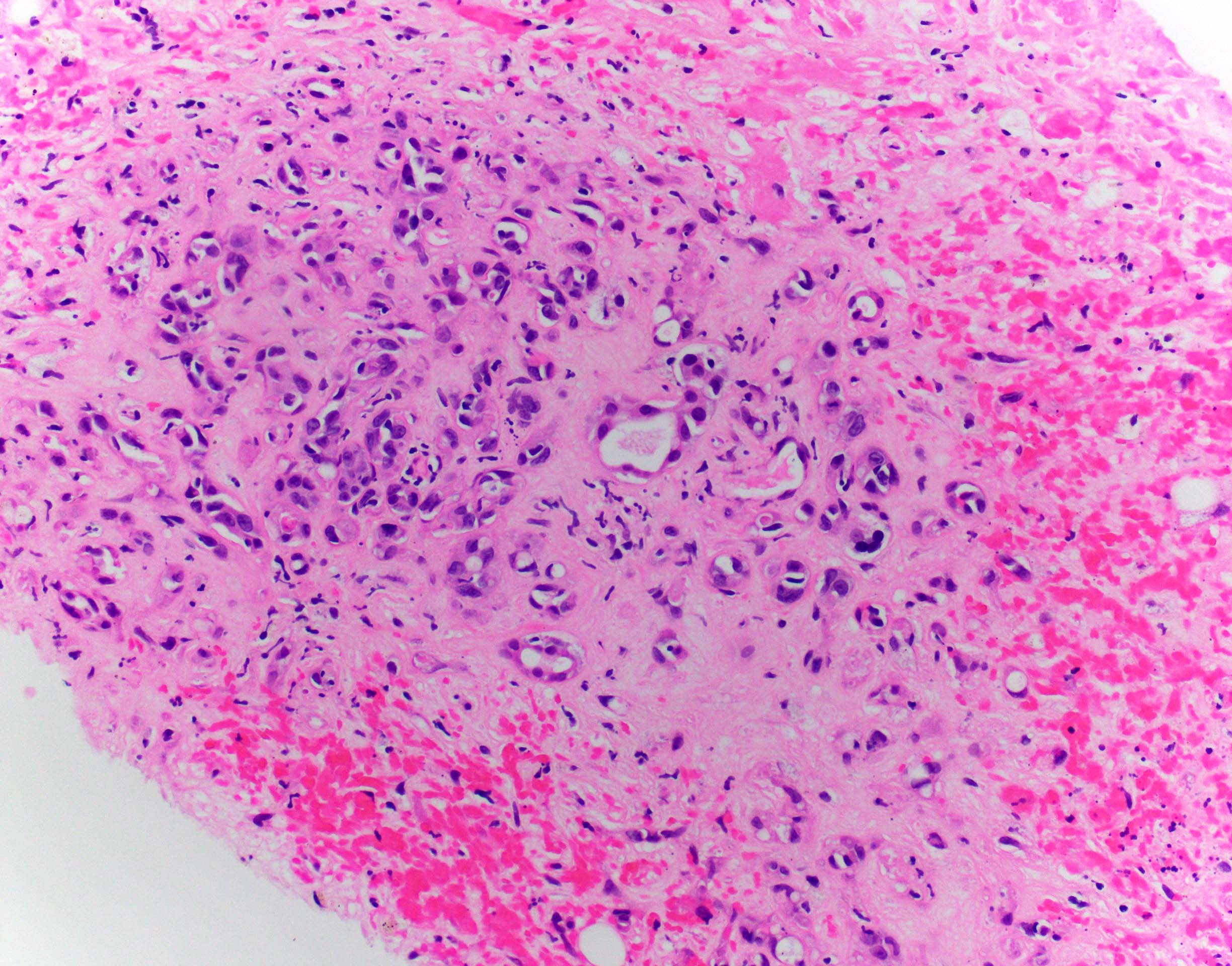
Poorly vasoformative cells
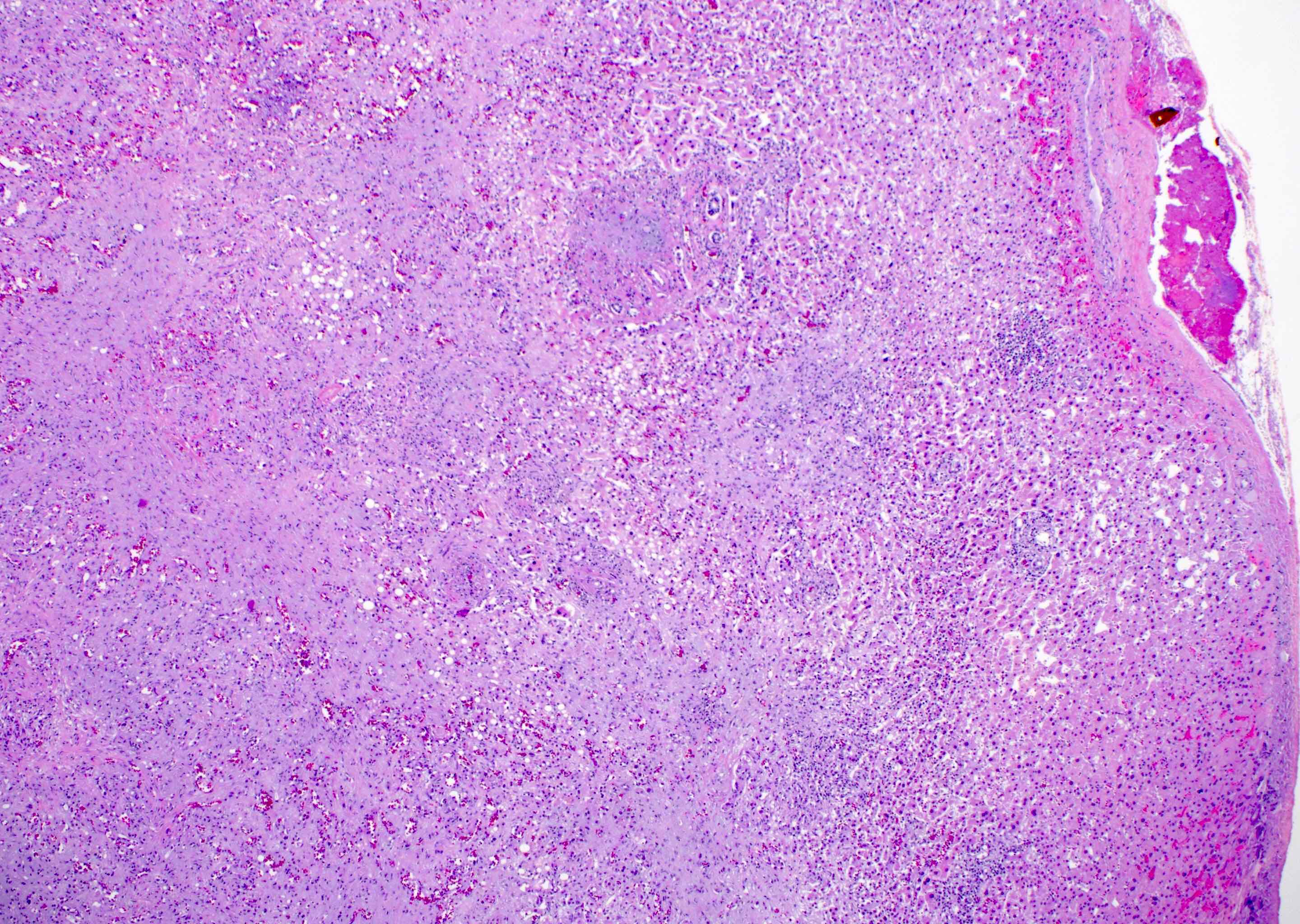
Epithelioid hemangioendothelioma
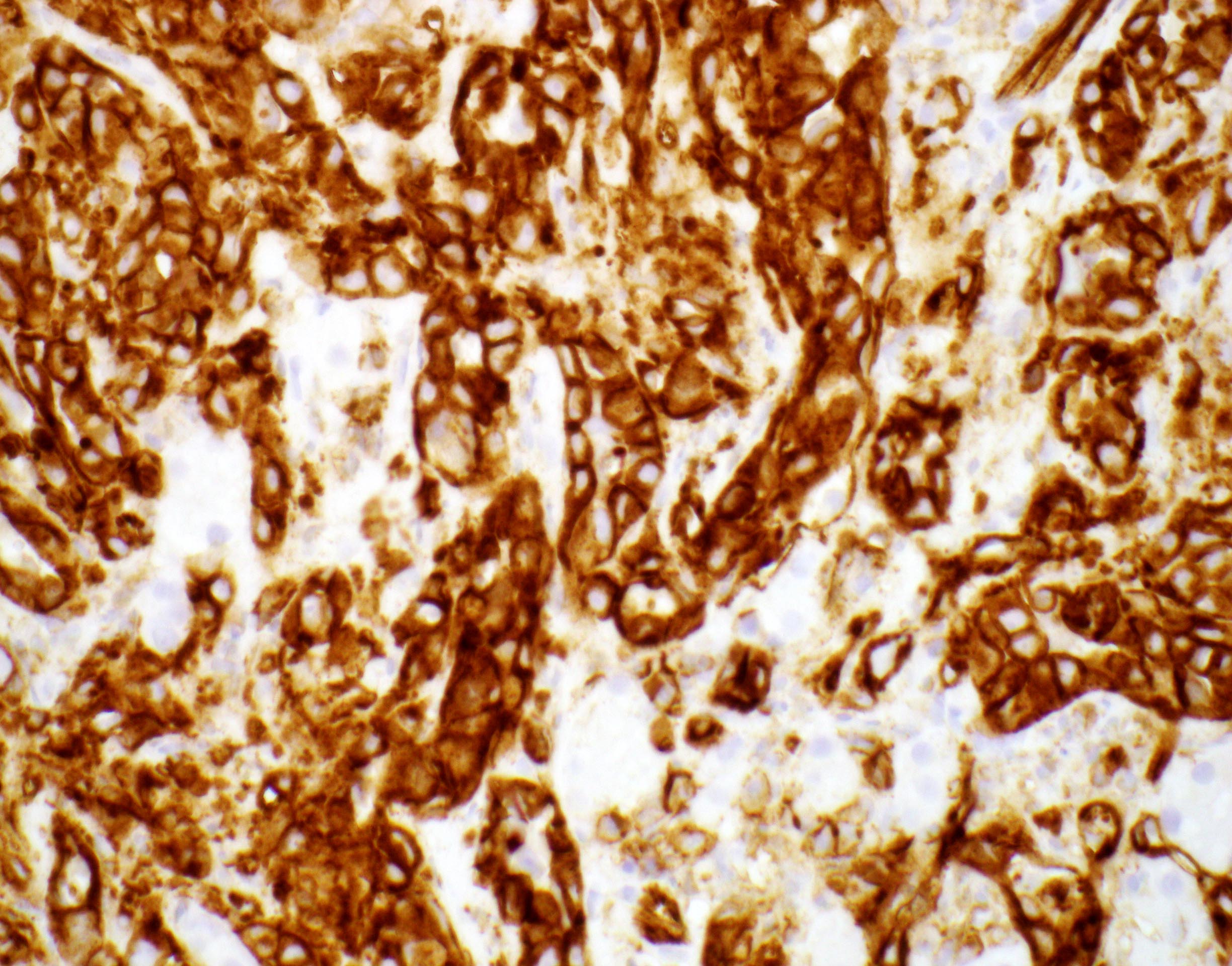
CD31
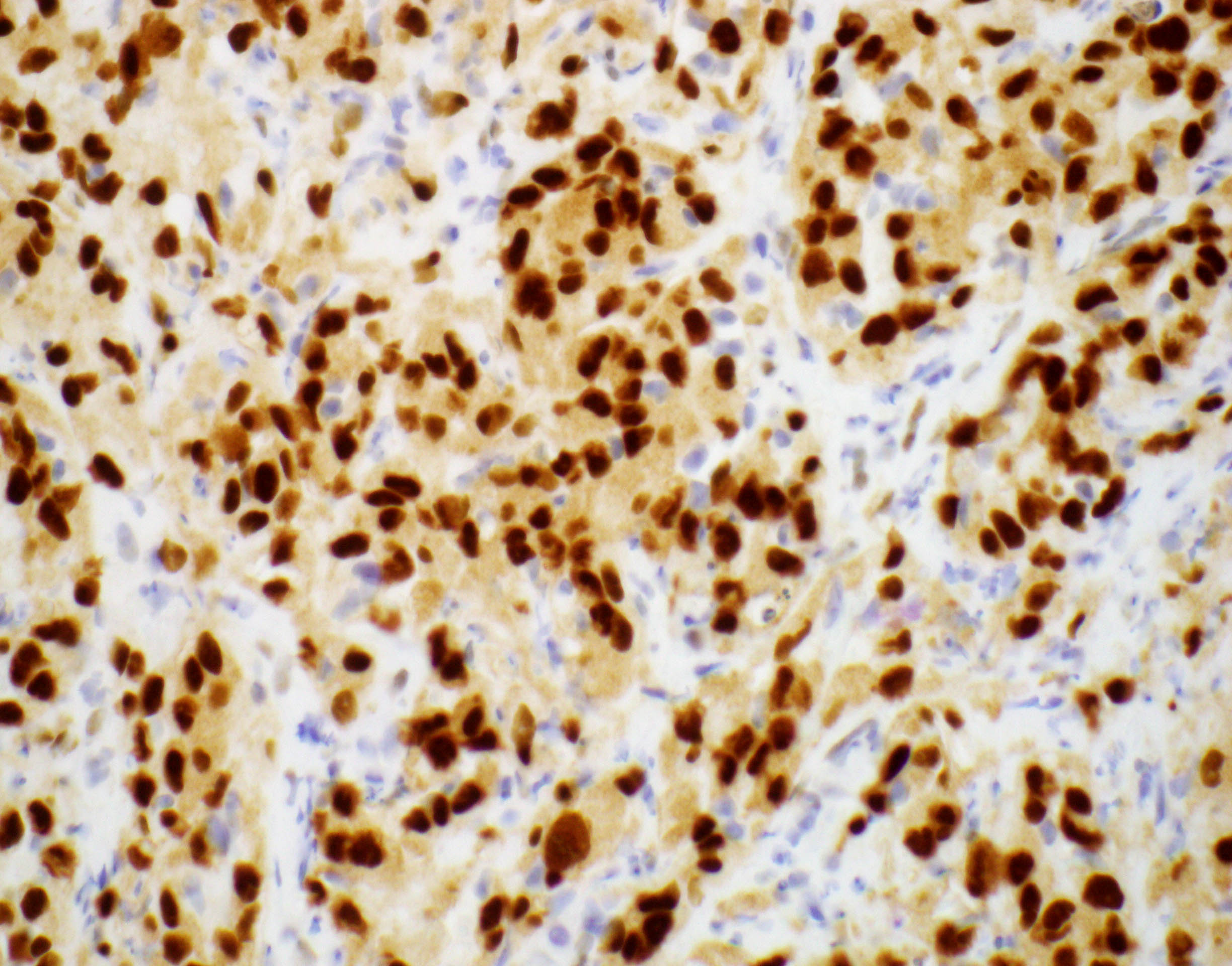
ERG
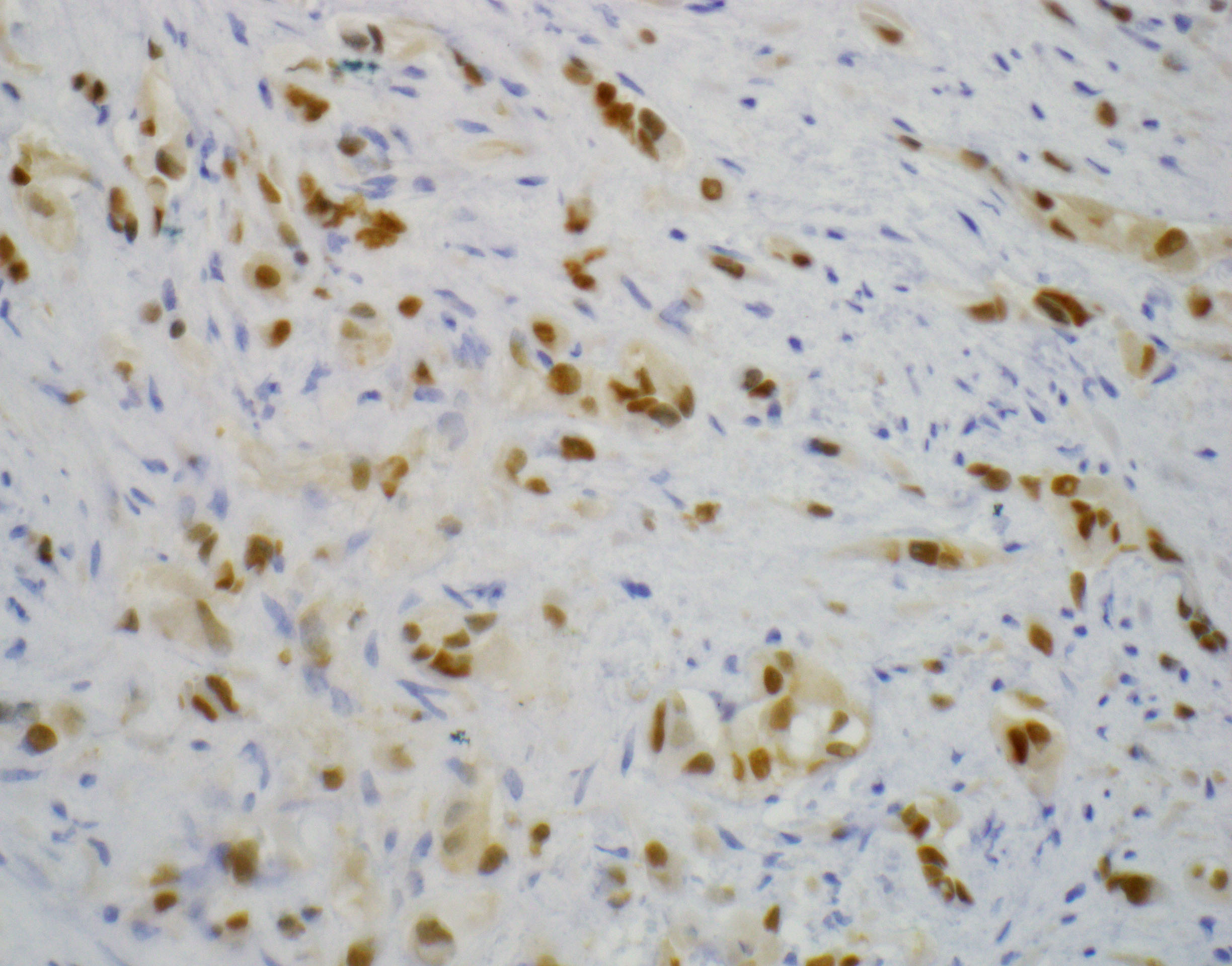
CAMTA1
Virtual slides
Images hosted on other servers:

Liver, epithelioid
hemangioendothelioma
Cytology description
- Round to polygonal plasmacytoid cells with minimal pleomorphism and few mitoses
- Frequent nuclear grooves and psuedoinclusions
- Dense cytoplasm with occasional intracytoplasmic lumina
- Hyaline stroma
- Reference: Am J Clin Pathol 2011;136:739
Cytology images
Images hosted on other servers:



FNA smears (Pap & cell block)
Positive stains
- Vascular markers: CD31, CD34 and ERG
- Keratins: especially CK8 and CK18
- WWTR1-CAMTA1 gene fusion tumors: positive for CAMTA1 (Am J Surg Pathol 2016;40:94)
- YAP1-TFE3 fusion tumors: nuclear expression of TFE3
- AE1 / AE3, CK7: usually negative, though a few cases can be positive (Ann Diagn Pathol 2020;49:151589
Negative stains
- EMA
- Desmin
- HepPar1
- Reference: Am J Surg Pathol 1997;21:363
Electron microscopy description
- Weibel-Palade bodies, prominent intracytoplasmic vacuoles, endothelial cells with elaborate intercellular contacts and desmosomes (Cancer 1982;50:970)
Electron microscopy images
Images hosted on other servers:

Endothelial cells, solid nests

Luminal differentiation

Desmosomes

Weibel-Palade bodies

Intracytoplasmic vacuoles
Molecular / cytogenetics description
- Multifocal hepatic disease is monoclonal
- t(1;3)(p36.3;q25) WWTR1-CAMTA1 gene fusion is characteristic, found in up to 90% of cases
- Fusion of WWTR1 to CAMTA1 results in dysregulation of the Hippo pathway, driving oncogenic transformation
- YAP1-TFE3 fusion found in small subset of tumors
- Similar to WWTR1, YAP1 is a downstream transcriptional regulator of the Hippo pathway
- References: Sci Transl Med 2011;3:98ra82, Genes Chromosomes Cancer 2011;50:644, Genes Chromosomes Cancer 2013;52:775
Molecular / cytogenetics images
Images hosted on other servers:

Identification of WWTR1-CAMTA1 fusion by FISH

YAP1-TFE3 fusion

Protein domains of YAP1, TFE3
Videos
Laparoscopic segment 6 liver resection for hepatic EHE
Overview of vascular tumors of the skin (by Dr. Jerad Gardner)
Sample pathology report
- Liver, core biopsy:
- Epithelioid hemangioendothelioma (see comment)
- Comment: FISH testing for CAMTA1 / WWTR1 fusion is positive. IHC for CAMTA1 shows nuclear positivity.
Differential diagnosis
- Angiosarcoma:
- Angiosarcomas have greater atypia and more mitoses and tend to be hemorrhagic with destructive growth pattern
- No nuclear staining for CAMTA1
- Adenocarcinoma (including cholangiocarcinoma):
- Sclerotic hepatocellular carcinoma:
- Abundant fibrous stroma separating nests or trabeculae of tumor cells
- Positive for arginase1, CK7 and glypican 3
- Negative for vascular markers
- Epithelioid hemangioma:
- Most commonly cutaneous and soft tissue lesions in head and neck, followed by distal extremities and trunk; visceral organs rare with lung being the only reported organ
- Histology shows proliferation of well formed small blood vessels lined by plump and epithelioid endothelial cells with mild cytological atypia; no myxohyaline stroma seen as in epithelioid hemangioendothelioma
- Marked lymphoplasmacytic infiltrates, prominent lymphoid follicles and abundant eosinophils are present, a feature not seen in epithelioid hemangioendothelioma
- Tumor cells express endothelial markers CD31, ERG and CD34 and can be EMA and keratin positive
- FOSB can be positive
- Immunostain for CAMTA1 negative
- Anastomosing hemangioma:
- Anastomosing sinusoidal capillary sized vessels with scattered hobnail endothelial cells
- Mild cytologic atypia and no multilayering of cells seen
- Mitoses are absent or rare (Am J Surg Pathol 2013;37:1761)
- No myxohyaline stroma seen
- Frequent GNAQ and GNA14 activating hotspot mutation seen, similar to those described in hepatic small vessel neoplasm (Am J Surg Pathol 2018;42:1201)
- Immunostain for CAMTA1 negative
Additional references
Board review style question #1
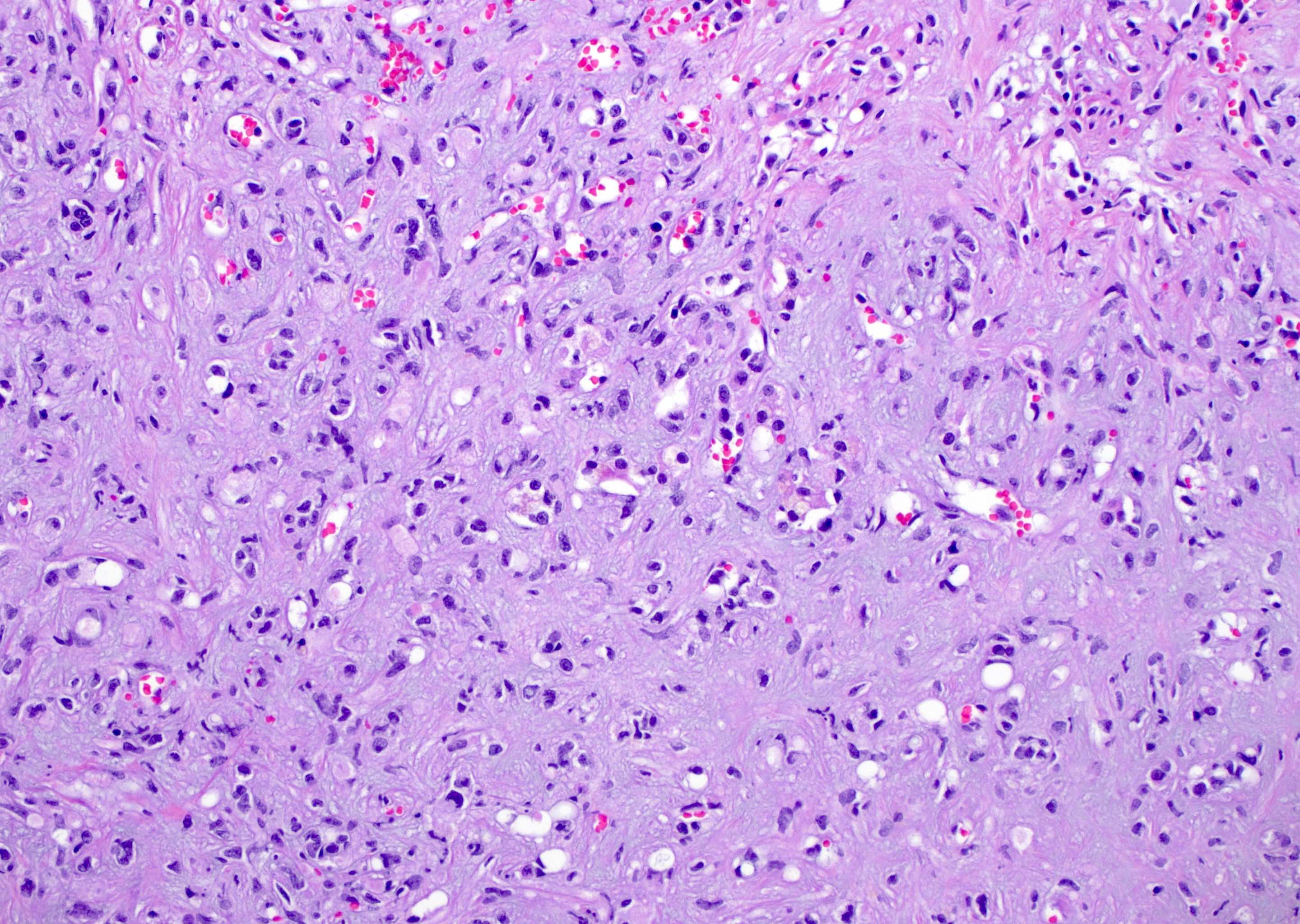
A liver biopsy of a 45 year old woman with multiple liver lesions is shown. Regarding this entity, which of the following is true?
- AE1 / AE3, CK7 and CDX2 are usually positive
- Arginase1, glypican 3 and albumin ISH are usually positive
- CD31, ERG and CAMTA1 are usually positive
- GNAQ mutations are common
Board review style answer #1
C. CD31, ERG and CAMTA1 are usually positive. This photo shows a tumor with poorly vasoformative epithelioid and spindle shaped cells growing in small nests and cords. Other scattered single cells are seen in a background of myxohyaline stroma. These histologic findings as well as multifocal presentation are consistent with an epithelioid hemangioendothelioma. EHE is a low grade malignant vascular neoplasm that commonly occurs in younger patients (30 - 50 year old), has a slight female predominance and may arise in multiple areas in the body (soft tissue and visceral organs, liver, lung). Epithelioid hemangioendothelioma is usually defined by a WWTR1-CAMTA1 fusion (~ 90% of cases), with a subset defined by a YAP1-TFE3 fusion. Epithelioid hemangioendothelioma is negative for arginase1, glypican 3, albumin ISH, CK7 and CDX2. They are usually negative for AE1 / AE3. GNAQ mutations are seen in a vast majority of cases of anastomosing hemangioma but not EHE.
Comment Here
Reference: Epithelioid hemangioendothelioma
Comment Here
Reference: Epithelioid hemangioendothelioma
Board review style question #2
The presence of a WWTR1-CAMTA1 fusion transcript, resulting in t(1;3) translocation can be used as a molecular test to confirm diagnosis of which vascular tumor?
- Epithelioid angiosarcoma
- Epithelioid hemangioma
- Epithelioid hemangioendothelioma
- Pseudomyogenic hemangioendothelioma
Board review style answer #2
C. Epithelioid hemangioendothelioma. Epithelioid hemangioendothelioma are low grade malignant vascular neoplasms and may arise in multiple areas in the body (soft tissue and visceral organs, liver, lung). They usually have a WWTR1-CAMTA1 fusion (~ 90% of cases). The WWTR1-CAMTA1 translocation is present in EHE across all anatomical sites and fusion of WWTR1 to CAMTA1 results in dysregulation of the Hippo pathway, driving oncogenic transformation. A separate translocation YAP1-TFE3 has been identified in a subset of tumors and YAP1, similarly to WWTR1, is a downstream transcriptional regulator of Hippo pathway. Epithelioid hemangiomas are characterized by recurrent fusion genes involving FOS or FOSB in as many as half the cases. Psuedomyogenic hemangioendothelioma is caused by a balanced translocation t(7;19)(q22;q13) resulting of fusion of SERPINE1 to FOSB and ACTB-FOSB. No recurrent gene fusions have been described in angiosarcoma, though MYC amplification can be seen, primarily in the setting of irradiation or lymphedema associated angiosarcoma.
Comment Here
Reference: Epithelioid hemangioendothelioma
Comment Here
Reference: Epithelioid hemangioendothelioma
