
Liver & intrahepatic bile ducts
Systemic conditions
Cardiac (congestive) hepatopathy and Fontan associated liver disease
Editorial Board Members: Monika Vyas, M.D., Wei Chen, M.D., Ph.D.


Last author update: 5 June 2023
Last staff update: 5 June 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Cardiac (congestive) hepatopathy and Fontan associated liver disease
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Carreon CK, Putra J. Cardiac (congestive) hepatopathy and Fontan associated liver disease. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/liverCHF.html. Accessed April 24th, 2024.
Definition / general
- Manifestations of chronic, passive congestion of the liver in the setting of heart failure or other heart defects (Clin Liver Dis (Hoboken) 2016;8:68)
Essential features
- Congestive hepatopathy can result from various cardiac diseases
- Similar hepatic manifestations following Fontan palliation in congenital heart defects is recognized as Fontan associated liver disease (Int J Mol Sci 2020;21:9420, Semin Thorac Cardiovasc Surg 2022;34:653, Pediatr Radiol 2021;51:2598)
Terminology
- Hepatic venous outflow obstruction
- Chronic passive congestion of the liver
- Congestive hepatopathy
- Cardiac hepatopathy
- Cardiac sclerosis
- Cardiac cirrhosis
ICD coding
Epidemiology
- Any cause of right sided heart failure can lead to congestive hepatopathy
- Widespread use of heart transplantation and major advances in medical and surgical management have significantly altered the profile of patients with congestive hepatopathy (Int J Mol Sci 2020;21:9420)
- Cases due to noncongenital heart failure are declining
- Cases following Fontan surgery (Fontan associated liver disease) are on the rise
Sites
- Liver
Pathophysiology
- Hepatic manifestations result from passive venous congestion / impaired hepatic venous drainage, secondary to chronic right sided heart failure (Int J Mol Sci 2020;21:9420)
- Fontan associated liver disease (FALD) (Int J Mol Sci 2020;21:9420):
- Functional structural alterations in the liver following Fontan creation (total cavopulmonary connection achieved by implanting a surgical shunt to divert blood from the inferior and superior vena cava to the pulmonary arteries) passively carry blood to the functionally single ventricular chamber
- Bypass leads to chronic hepatic venous congestion, secondary to high pressure nonpulsatile flow in the inferior vena cava
- Lack of subpulmonary ventricle also leads to diminished cardiac preload for the systemic ventricle, resulting in chronically low cardiac output
- FALD's natural history is poorly understood; at present, there are no methods to identify or predict patients that will eventually develop clinically significant advanced liver disease
Etiology
- Right sided heart failure or right ventricular failure (RVF), whether primary or secondary
- In the adult population, RVF is usually a result of left ventricular failure (Interact Cardiovasc Thorac Surg 2018;27:921)
- Primary RVF (Card Fail Rev 2019;5:140):
- Chronic conditions leading to pressure overload
- Congenital heart defects (pulmonic stenosis, those with right ventricular outflow obstruction or RV exposed to systemic pressure)
- Chronic conditions leading to volume overload (Card Fail Rev 2019;5:140):
- Valvular insufficiency involving tricuspid or pulmonic valves
- Congenital heart disease with left to right shunt (atrial septal defect, anomalous pulmonary venous return)
- Fontan associated liver disease (Int J Mol Sci 2020;21:9420):
- Recognized consequence of Fontan palliation in patients born with univentricular physiology, congenital heart disease
- Intrinsic RV myocardial disease / injury (Interact Cardiovasc Thorac Surg 2018;27:921):
- Ischemia or infarct
- Infiltrative disease (e.g., sarcoidosis, tumor, amyloidosis)
- Arrhythmogenic right ventricular dysplasia
- Cardiomyopathy
- Microvascular disease
- Impaired RV filling (Interact Cardiovasc Thorac Surg 2018;27:921):
- Constrictive pericarditis
- Tricuspid stenosis
- Systemic vasodilatory shock
- Cardiac tamponade
- Superior vena cava syndrome
- Hypovolemia
Clinical features
- Usually asymptomatic and in such a scenario, passive liver congestion may be incidentally discovered through abnormalities in routine laboratory evaluations (Clin Liver Dis (Hoboken) 2016;8:68)
- When symptomatic, patients may experience
- Dull right upper quadrant pain
- Jaundice
- Clinical stigmata of portal hypertension are generally absent until cirrhosis ensues (Clin Liver Dis 2002;6:947)
- Progressive dyspnea
- Hepatomegaly
- Gastroesophageal varices
- Ascites
- Hepatojugular reflux
- Peripheral edema
Diagnosis
- Diagnosis is often made by abnormal laboratory workup (see Laboratory findings)
- Liver biopsy may be performed if liver tests are persistently abnormal after heart failure treatment or as part of the heart or combined heart / liver transplant workup
Laboratory
- Unconjugated hyperbilirubinemia (total bilirubin < 3 mg/dL [51.31 micromol/L])
- Elevated aminotransferases (< 2 - 3 fold)
- Mild hypoalbuminemia in 30 - 50% of patients (Clin Liver Dis 2002;6:947)
- Prolonged prothrombin time / international normalized ratio (PT / INR)
- Ascitic fluid may show high serum to ascites albumin concentration gradient (JAMA 2016;316:340)
- Gradients ≥ 1.1 g/dL (11 g/L) are specific for ascites due to portal hypertension (the serum albumin concentration minus the ascitic albumin concentration [SAAG]) (JAMA 2016;316:340)
- High ascitic total protein content (typically > 2.5 g/dL [25 g/L]) plus a SAAG ≥ 1.1 g/dL (11 g/L) suggests congestive hepatopathy and differentiates portal hypertension from cirrhosis (typically total protein < 2.5 g/dL [25 g/L] plus a SAAG ≥ 1.1 g/dL [11 g/L])
Radiology description
- Ultrasound (US) may be used to evaluate hemodynamic properties of the liver in patients with congestive hepatopathy (CH)
- Doppler US is the most cost effective and expeditious modality for assessing blood flow direction and velocity in the hepatic vasculature
- Common US findings of CH (Acta Radiol Diagn (Stockh) 1982;23:361, Am J Cardiol 1984;53:579):
- Dilated inferior vena cava
- Dilated hepatic veins
- Degree of dilatation correlates with the severity of heart failure
- CT and MR imaging can show a number of characteristic findings helpful for the diagnosis of CH (Diagn Interv Radiol 2020;26:541)
- Hepatomegaly in acute congestion
- Atrophic nodular liver in patients with chronic congestion and cirrhosis
- As seen on the US, the inferior vena cava and hepatic veins are dilated; in severe cases, venous shunts can be observed between the hepatic veins
- Increased prevalence of hyperenhancing hepatic nodules that appear similar to focal nodular hyperplasia
- Presence of cirrhosis increases the risk for hepatocellular carcinoma in patients with CH; this diagnosis must be taken into consideration
- Reference: Radiographics 2016;36:1024
Prognostic factors
- Clinical outcome generally depends on the severity of underlying cardiac disease; progression to cirrhosis does not necessarily correlate with worse prognosis and reversibility may be achieved by optimization of cardiac function (Clin Liver Dis (Hoboken) 2016;8:68)
Case reports
- 7 year old girl with Fontan associated liver disease and hepatic adenomatosis (Pediatr Cardiol 2010;31:861)
- 36 year old woman with focal nodular hyperplasia in the setting of Fontan associated liver disease (Korean J Intern Med 2022;37:480)
- 40 year old man with Fontan associated liver disease and ruptured hepatocellular carcinoma (SAGE Open Med Case Rep 2020;8:2050313X20922030)
Treatment
- Management of the underlying heart condition with optimization of cardiac output
- Treatment options include diuresis, left ventricular assist device (LVAD) implantation and liver transplantation (Clin Liver Dis (Hoboken) 2016;8:68)
Gross description
- Sinusoidal congestion resulting in a classic nutmeg appearance
- Advanced fibrosis may lead to a firm and nodular cut surface
- Reference: Clin Liver Dis (Hoboken) 2016;8:68
Gross images
Contributed by Juan Putra, M.D.

Nutmeg liver
Microscopic (histologic) description
- Sinusoidal dilatation and congestion
- Centrilobular hepatocyte atrophy or dropout
- Centrilobular and perisinusoidal fibrosis (heterogeneous distribution but generally starts in zone 3 hepatocytes)
- Portal fibrosis in up to 75% of cases
- Minimal portal inflammation and ductular reaction
- Nodular regenerative hyperplasia (Rev Esp Cardiol (Engl Ed) 2018;71:192)
- Hepatocellular carcinoma may arise in the setting of cirrhosis (J Thorac Cardiovasc Surg 2005;129:1348, JHEP Rep 2021;3:100249)
- Focal nodular hyperplasia and hepatic adenoma may also occur (JACC Case Rep 2019;1:175, J Thorac Cardiovasc Surg 2005;129:1348, Pediatr Cardiol 2010;31:861)
- Pseudoground glass and eosinophilic cytoplasmic inclusions (Torbenson: Biopsy Interpretation of the Liver, 4th Edition, 2021, Mod Pathol 2000;13:679)
- Congestive hepatic fibrosis score shows a good correlation with the right atrial pressure (Mod Pathol 2014;27:1552):
- Score 0: no fibrosis
- Score 1: central zone fibrosis
- Score 2A: central zone and mild portal fibrosis, with accentuation at central zone
- Score 2B: at least moderate portal fibrosis and central zone fibrosis, with accentuation at portal zone
- Score 3: bridging fibrosis
- Score 4: cirrhosis
Microscopic (histologic) images
Contributed by Juan Putra, M.D., Monika Vyas, M.D. and Wei Chen, M.D., Ph.D.
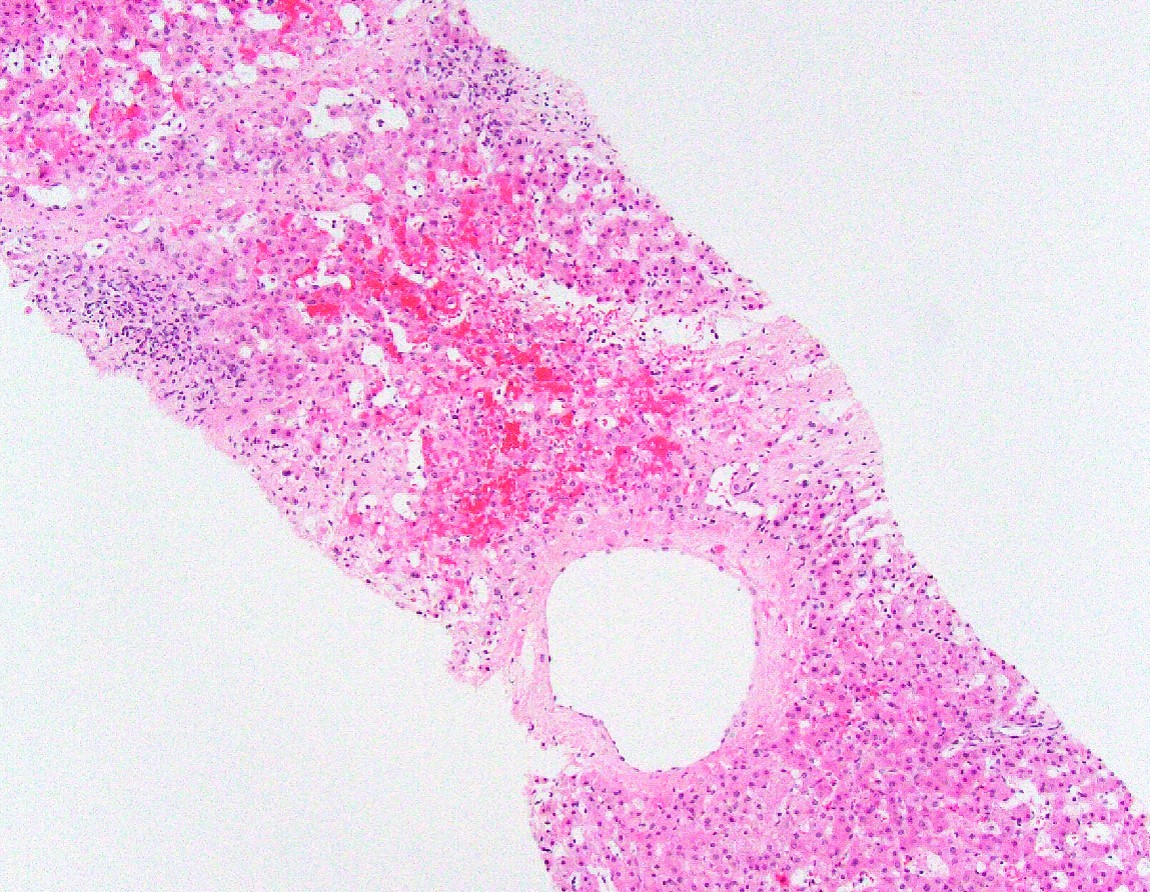
Sinusoidal dilatation and congestion
Centrilobular hepatocyte atrophy
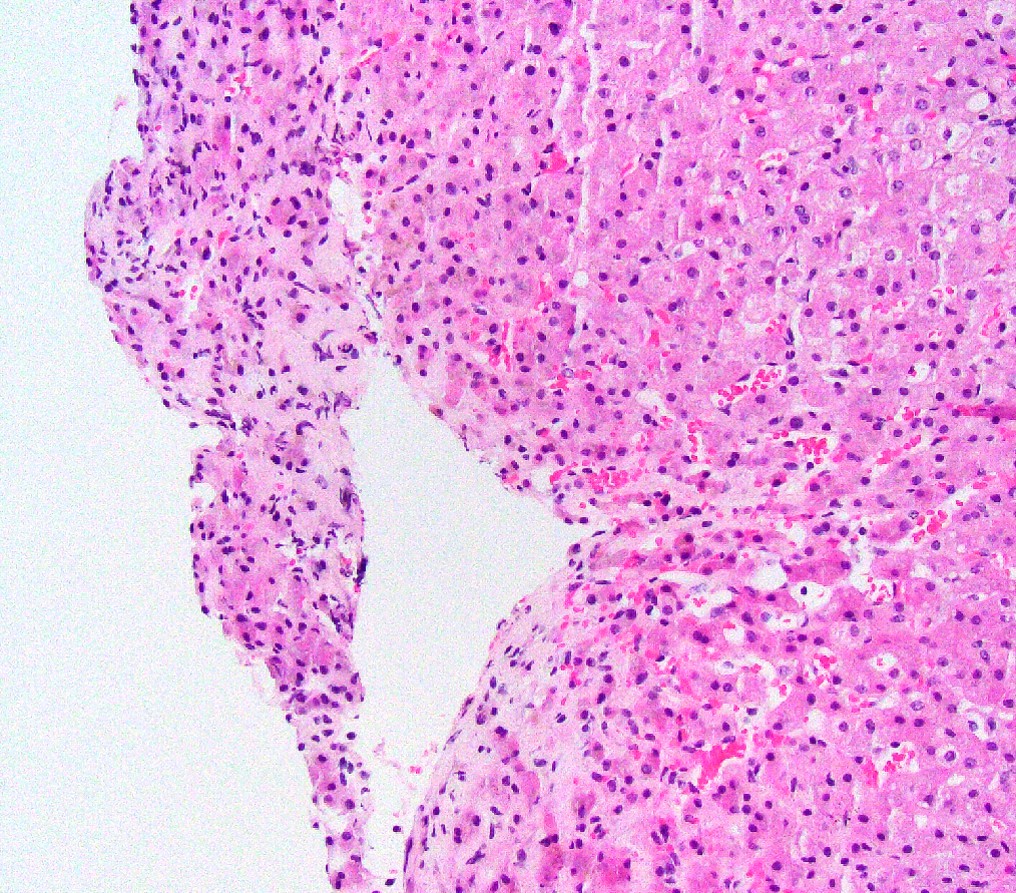
Hepatocyte dropout and atrophy
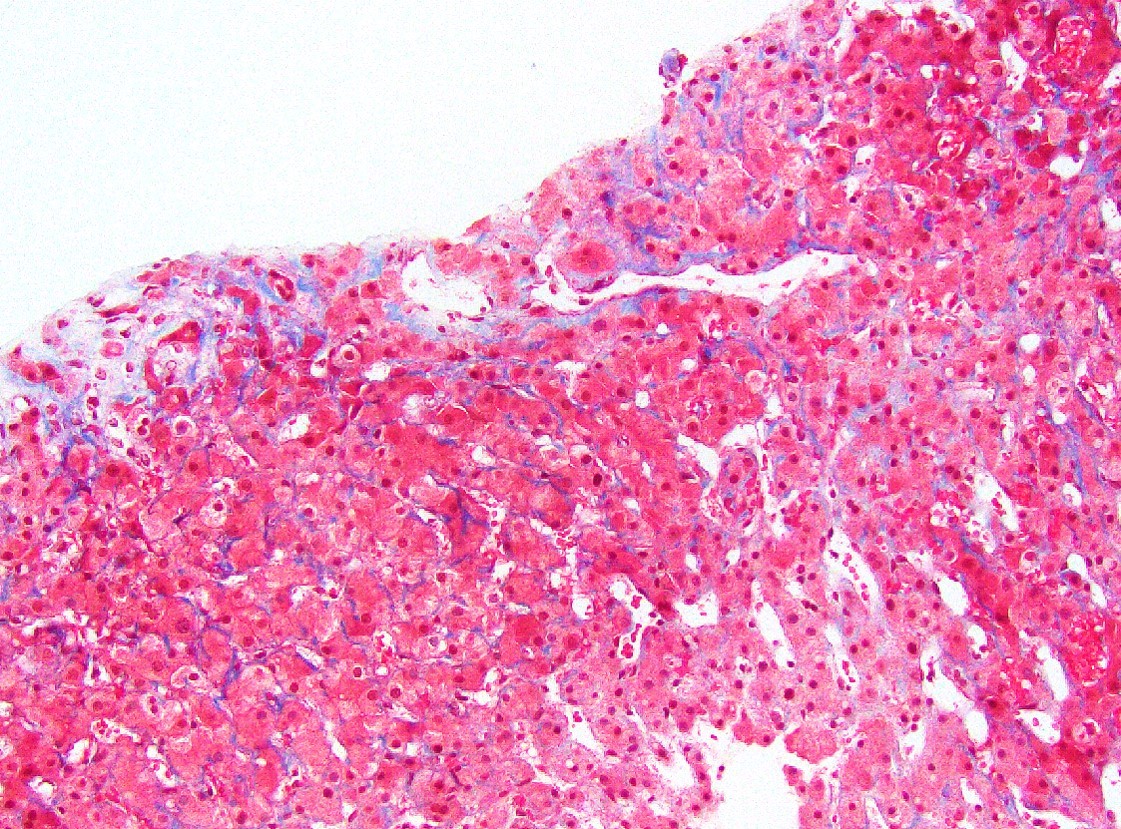
Perisinusoidal fibrosis
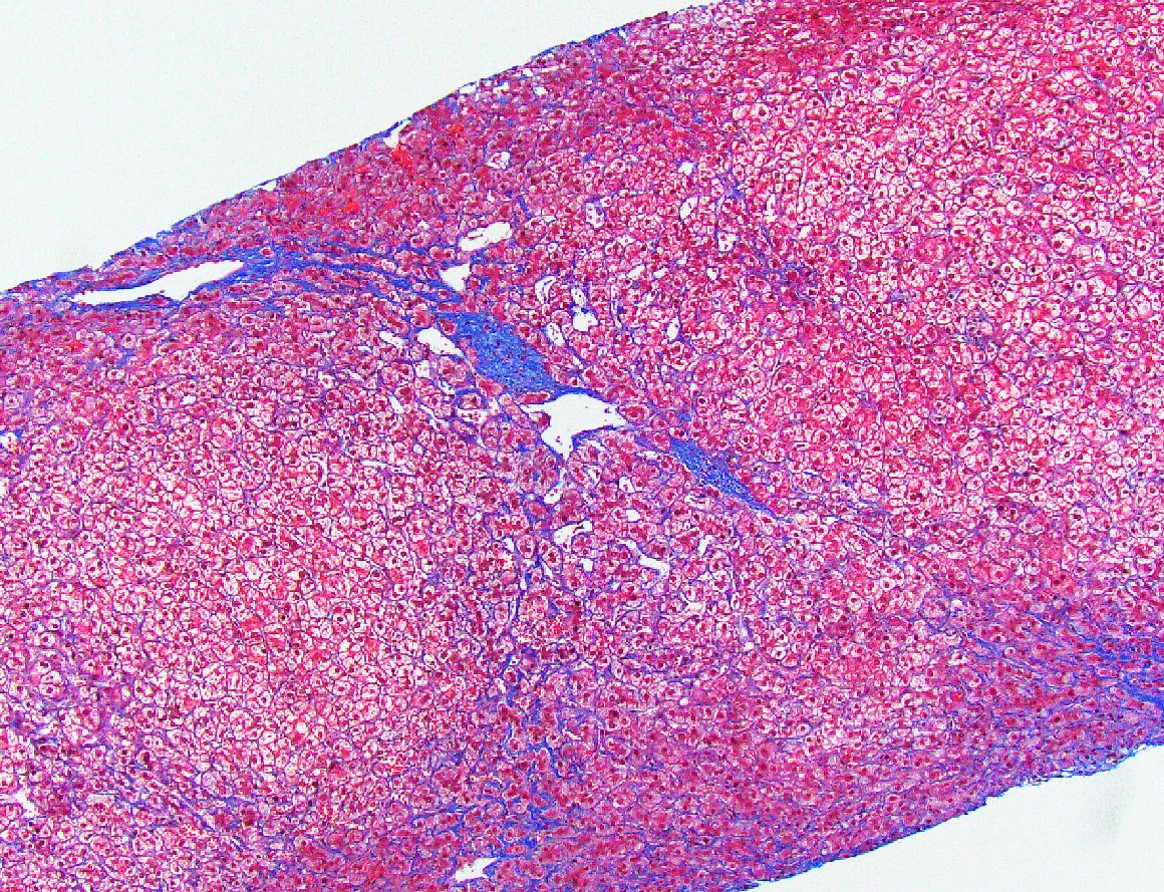
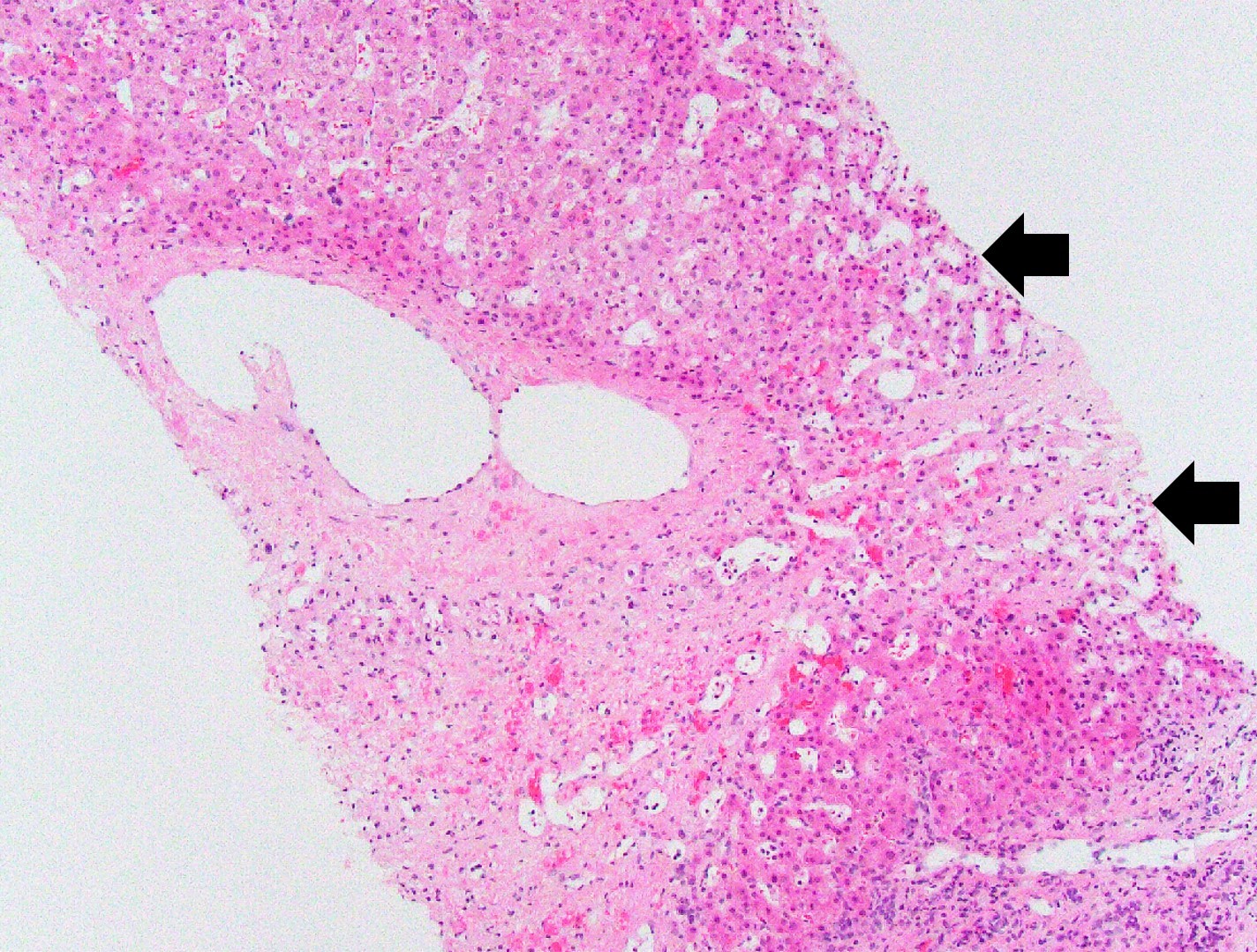
Perivenular fibrosis
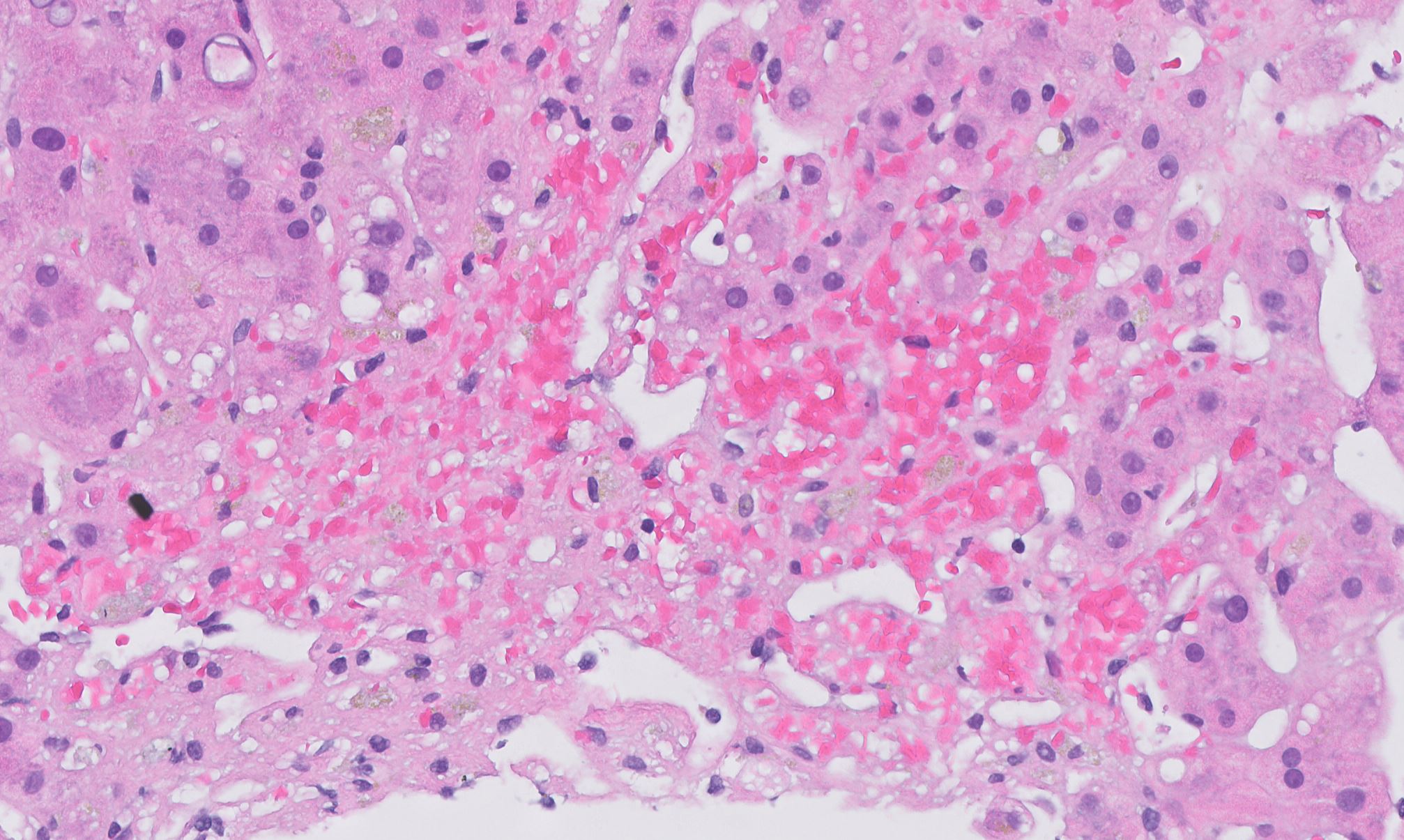
Space of Disse congestion
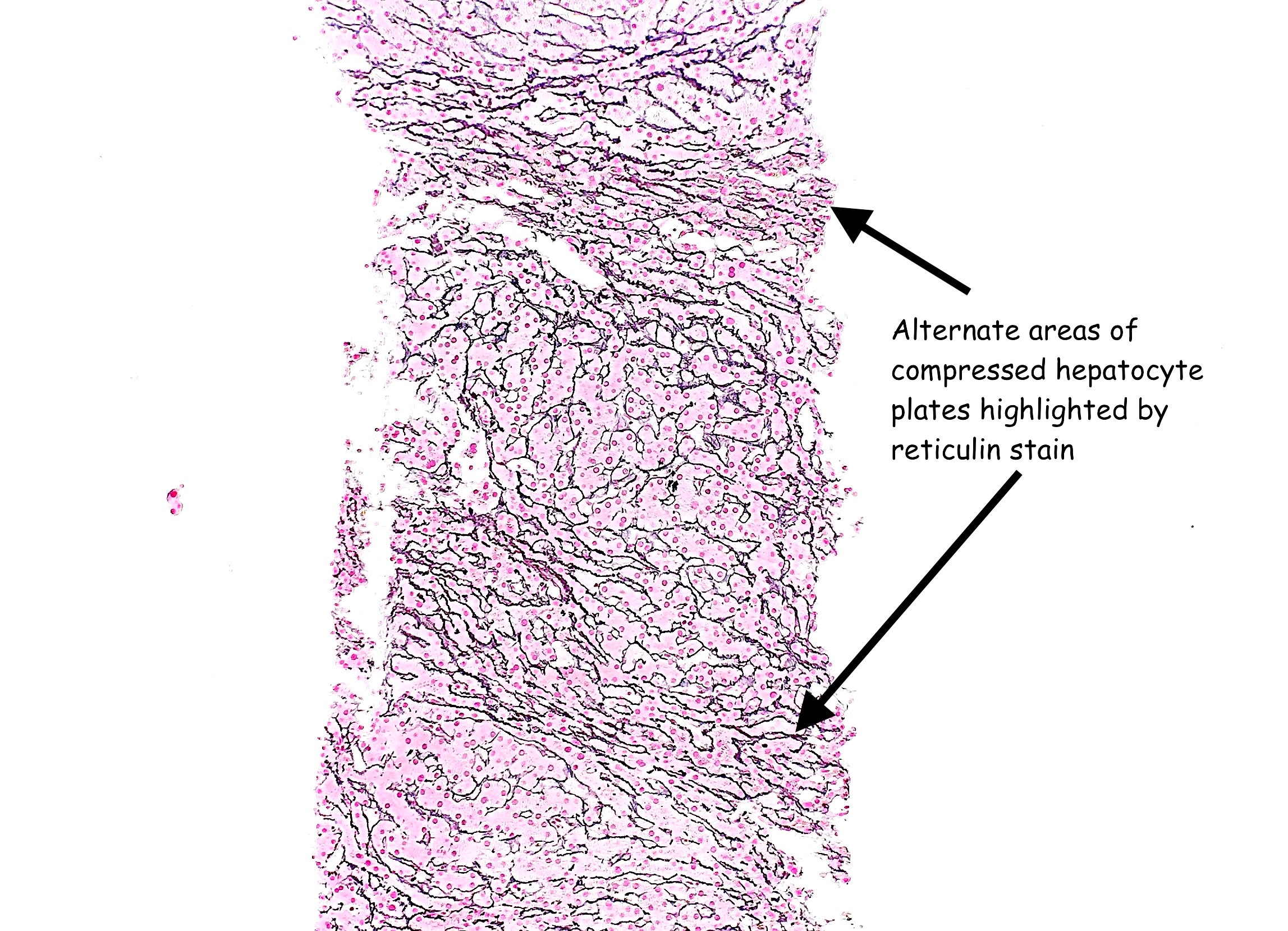
Zones of compressed and normal hepatic cell plates
Positive stains
- Special stains for fibrosis evaluation: Masson trichrome or Sirius red
- Special stain for nodular regenerative hyperplasia and fibrosis evaluation: reticulin
Sample pathology report
- Liver, biopsy:
- Liver with patchy sinusoidal dilatation and congestion, in keeping with Fontan associated liver disease (congestive hepatopathy)
- Heterogeneous degree of fibrosis with portal, perivenular and perisinusoidal fibrosis with focal portal to central bridging fibrosis (congestive hepatic fibrosis score 2A-3 of 4)
- No significant portal inflammation, lobular activity, steatosis or cholestasis
Differential diagnosis
- Budd-Chiari syndrome:
- Centrilobular hepatocyte necrosis is more common
- Sinusoidal obstruction syndrome:
- Marked centrilobular hemorrhagic necrosis in the early phase and occlusion of the central veins by fibrous tissue in later stages of the disease
- Ischemia:
- Centrilobular coagulative hepatocyte necrosis is more common
Additional references
Board review style question #1
Which of the following histologic features is typical of congestive hepatopathy?
- Bile duct injury
- Feathery degeneration of hepatocytes
- Microvesicular steatosis
- Obliterated portal veins
- Perisinusoidal fibrosis
Board review style answer #1
E. Perisinusoidal fibrosis
Comment Here
Reference: Cardiac (congestive) hepatopathy and Fontan associated liver disease
Comment Here
Reference: Cardiac (congestive) hepatopathy and Fontan associated liver disease
Board review style question #2
Which is the most likely condition associated with the H&E findings shown above?
- Caroli syndrome
- Celiac disease
- Constrictive pericarditis
- Cystic fibrosis
- Portal vein thrombosis
Board review style answer #2
C. Constrictive pericarditis
Comment Here
Reference: Cardiac (congestive) hepatopathy and Fontan associated liver disease
Comment Here
Reference: Cardiac (congestive) hepatopathy and Fontan associated liver disease
