

Kidney tumor
Childhood tumors
Ossifying renal tumor of infancy
Editorial Board Member: Debra L. Zynger, M.D.
Deputy Editor-in-Chief: Maria Tretiakova, M.D., Ph.D.


Last author update: 27 April 2023
Last staff update: 27 April 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Ossifying renal tumor
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: D'Hooghe E, Vujanic GM. Ossifying renal tumor of infancy. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneytumorossifying.html. Accessed April 23rd, 2024.
Definition / general
- Exceptionally rare, benign, renal neoplasm of early life
- Calcified mass in the renal pelvis composed of (partially) calcified osteoid matrix with osteoblast-like cells, mixed with blastema-like cells and sometimes spindle cells
- First described by Chatten et al. in 1980 (Cancer 1980;45:609)
Essential features
- Rare benign renal tumor
- Not linked with other renal tumors of childhood
- The majority in the first year of life
- Characteristic osteoid areas with osteoblast-like cells and areas with blastema-like cells
- Spindle cells can be present or absent
- Treated with surgery only
- No recurrences reported
Terminology
- Ossifying renal tumor of infancy (ORTI)
- No other terms used
ICD coding
- ICD-O: 8967/0 - ossifying renal tumor
- ICD-11: 2F35 & XH3SR2 - benign neoplasm of urinary organs & ossifying renal tumor
Epidemiology
- Very rare tumor; 23 reported in the literature (Pediatr Dev Pathol 2017;20:511)
- Age at presentation: 6 days to 2.5 years
- Median age: 6.5 months; only 3 patients older than 1 year (Pediatr Dev Pathol 2017;20:511)
- M:F = ~7:1 (20 males; 3 females)
Sites
- Kidney (renal pelvis)
- Unifocal
- Never bilateral
Pathophysiology
- Unknown
- Cytogenetic and molecular studies found no evidence that it is linked to Wilms tumor
Etiology
- Not known
Clinical features
- Presents as painless, intermittent, macroscopic hematuria
- Rarely as a mass (incidentally found)
Diagnosis
- On imaging, a calcified mass in the renal pelvis
- Diagnosis is made histologically using the surgical specimen
Laboratory
- No abnormalities
Radiology description
- Can be diagnosed on US, CT or MRI investigations
- Visible as a calcified mass (Pediatr Radiol 2014;44:625)
Prognostic factors
- Benign clinical course
- No recurrences or metastases reported (Pediatr Radiol 2014;44:625)
Case reports
- 8 week and 2 year old boys with gross hematuria (J Pediatr Urol 2007;3:258)
- 6 month old boy underwent laparoscopic treatment for ORTI (Case Rep Urol 2018;2018:1935657)
- 6 month old boy presented with macrohematuria (J Pediatr Surg 2013;48:e37)
Treatment
- Usually total nephrectomy (16 cases)
- Rare cases are treated with partial nephrectomy (4 cases)
- Enucleation also possible in rare cases (3 cases)
- No other treatment necessary
- Reference: Pediatr Dev Pathol 2017;20:511
Gross description
- Exophytic / polypoid mass attached to the renal parenchyma protruding into the renal pelvis
- Rarely greater than 2 to 3 cm in size
- Reference: Pediatr Dev Pathol 2017;20:511
Gross images
Contributed by Ellen D’Hooghe, M.D. and Gordan M. Vujanic, M.D., Ph.D.
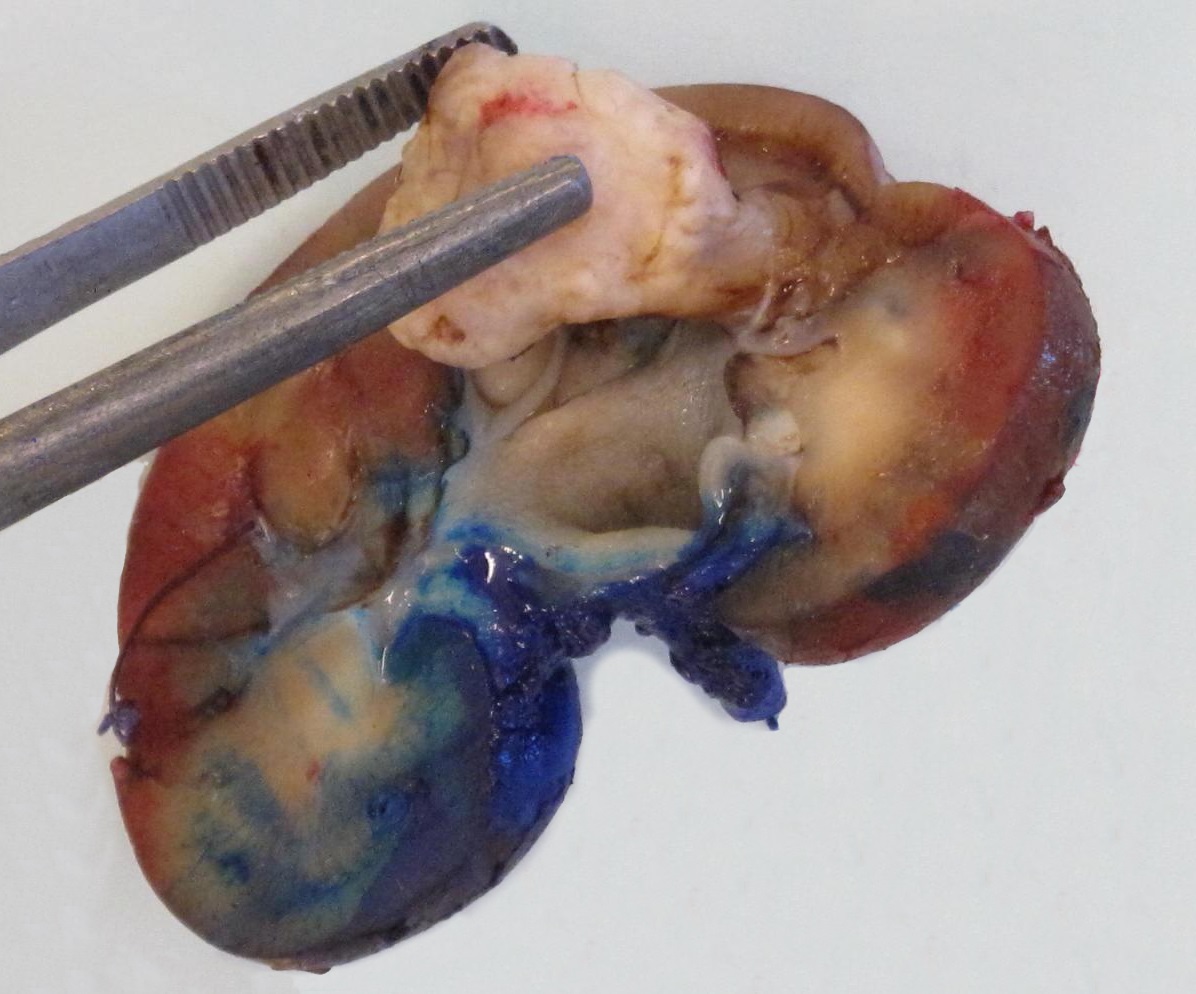
Polypoid / pedunculated calcified mass
Microscopic (histologic) description
- Consists of 2 to 3 components
- Ossifying component with large osteoblast-like cells
- Blastema-like small, undifferentiated cells
- Spindle cells (not always found)
- Mitoses can be seen in the blastema-like component
- Reference: Pediatr Dev Pathol 2017;20:511
Microscopic (histologic) images
Contributed by Ellen D’Hooghe, M.D. and Gordan M. Vujanic, M.D., Ph.D.
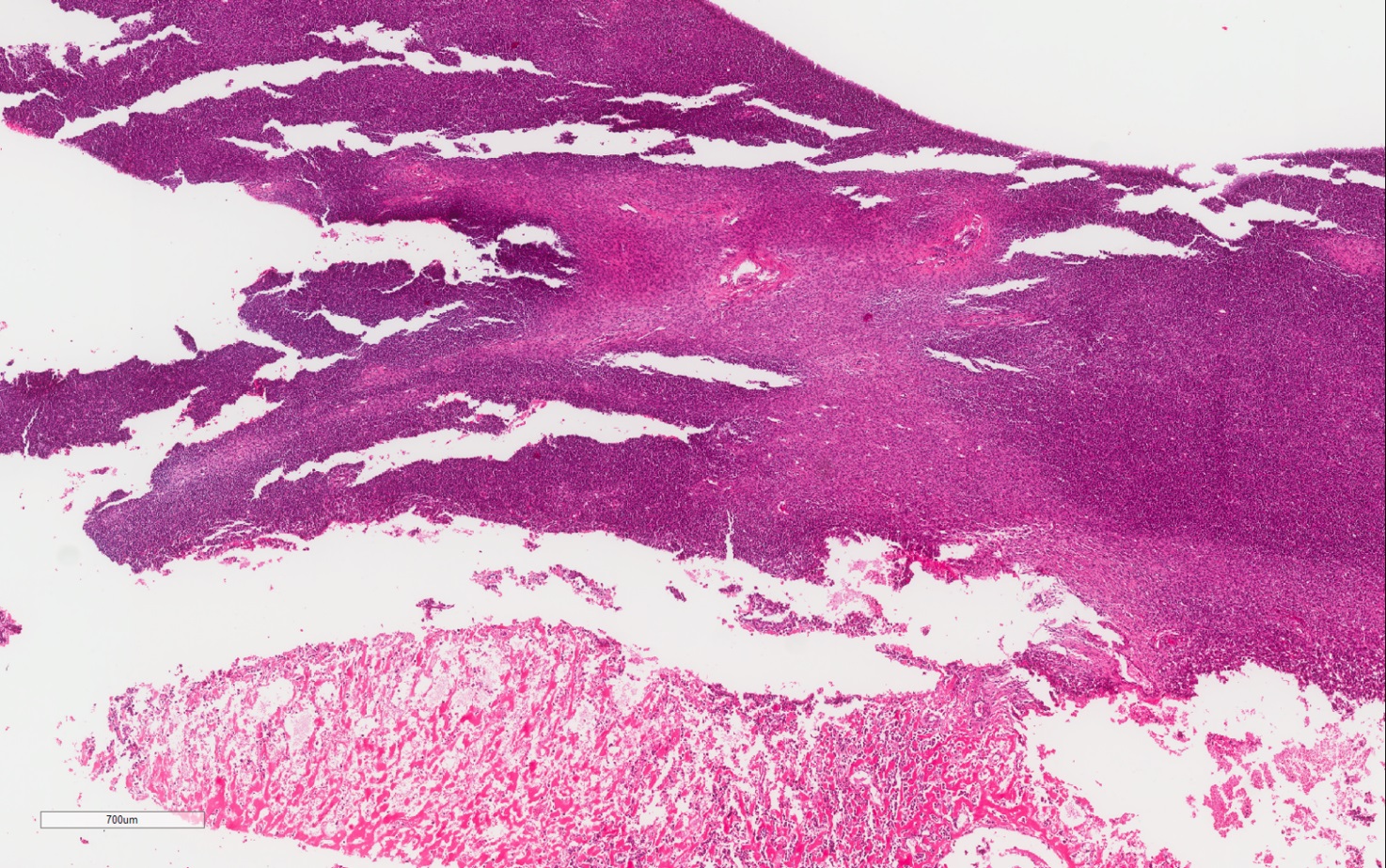
Osteoid and cellular components
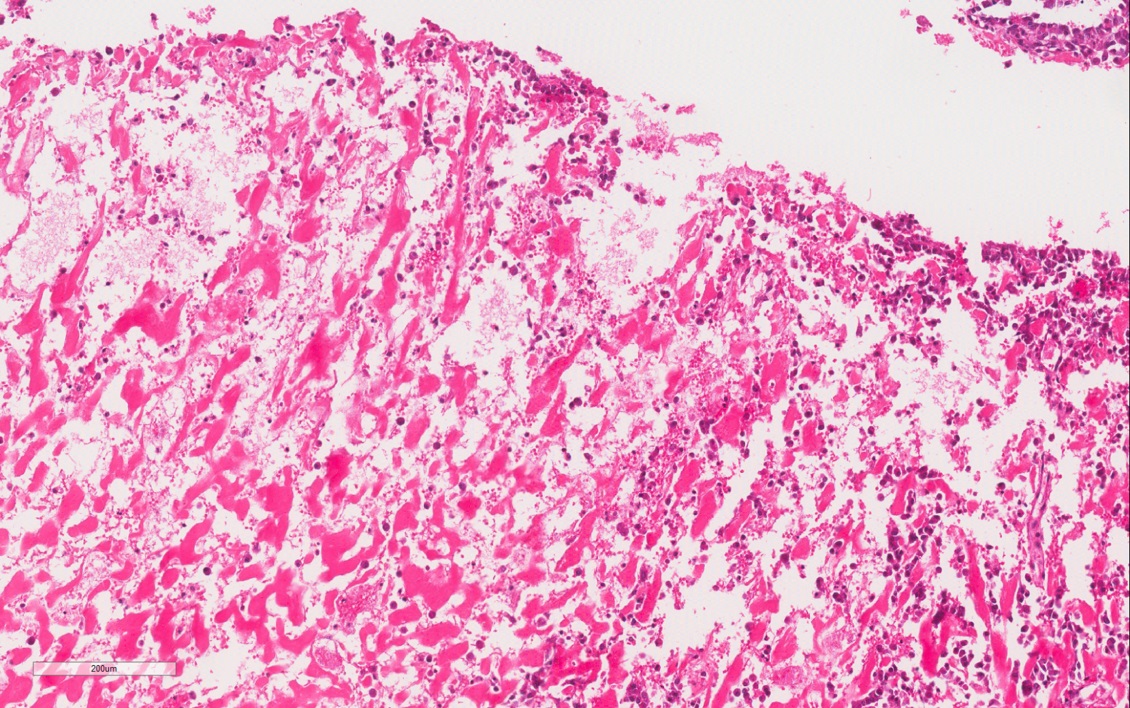
Osteoid component
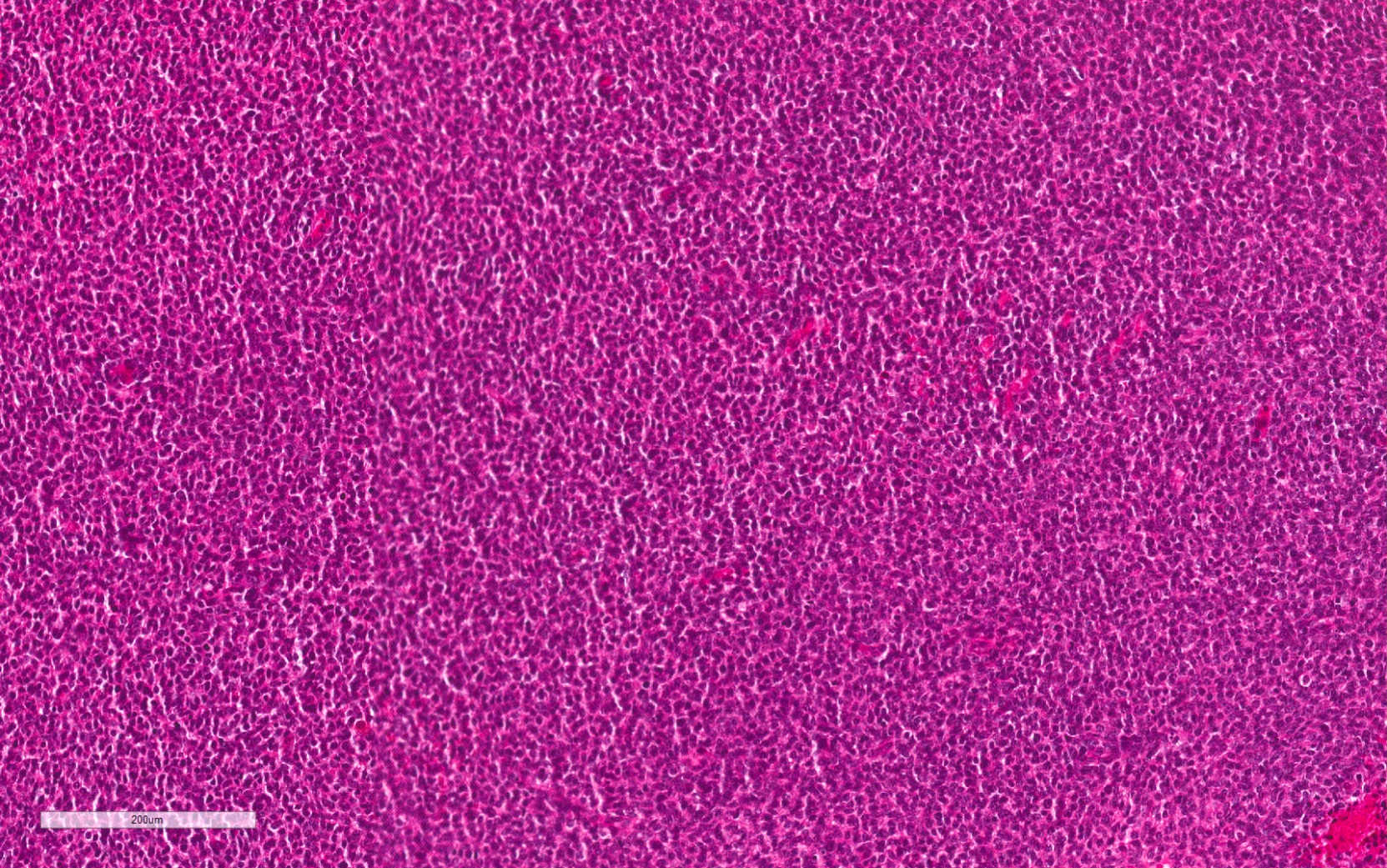
Cellular component
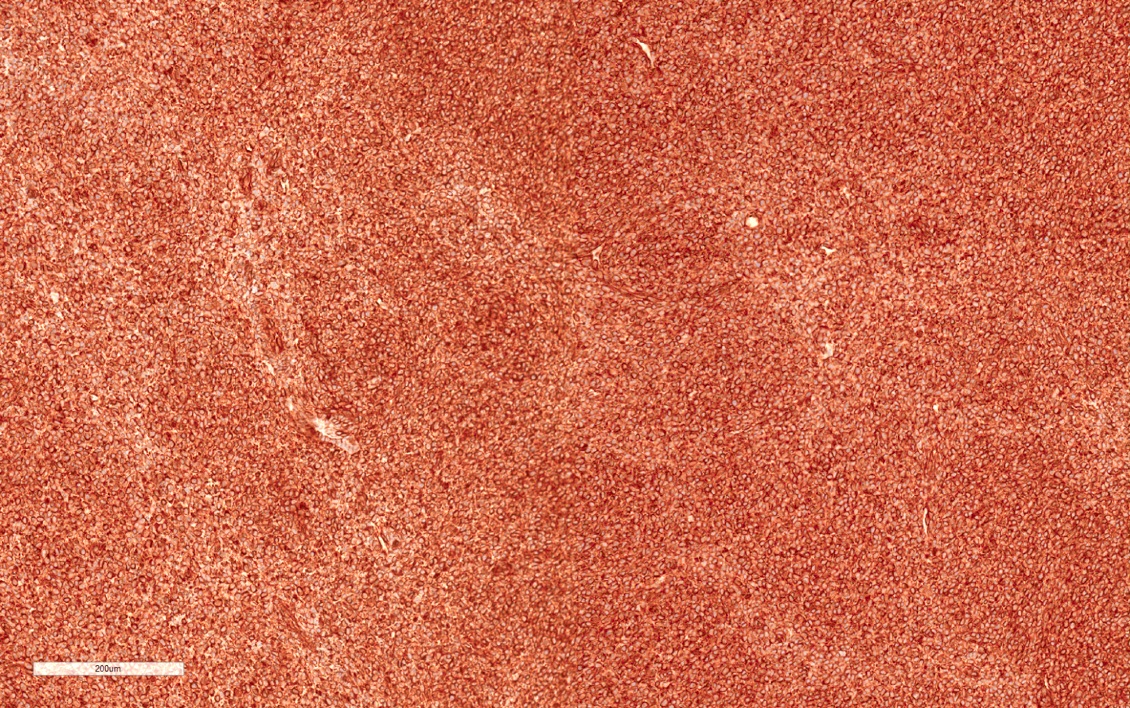
Vimentin+
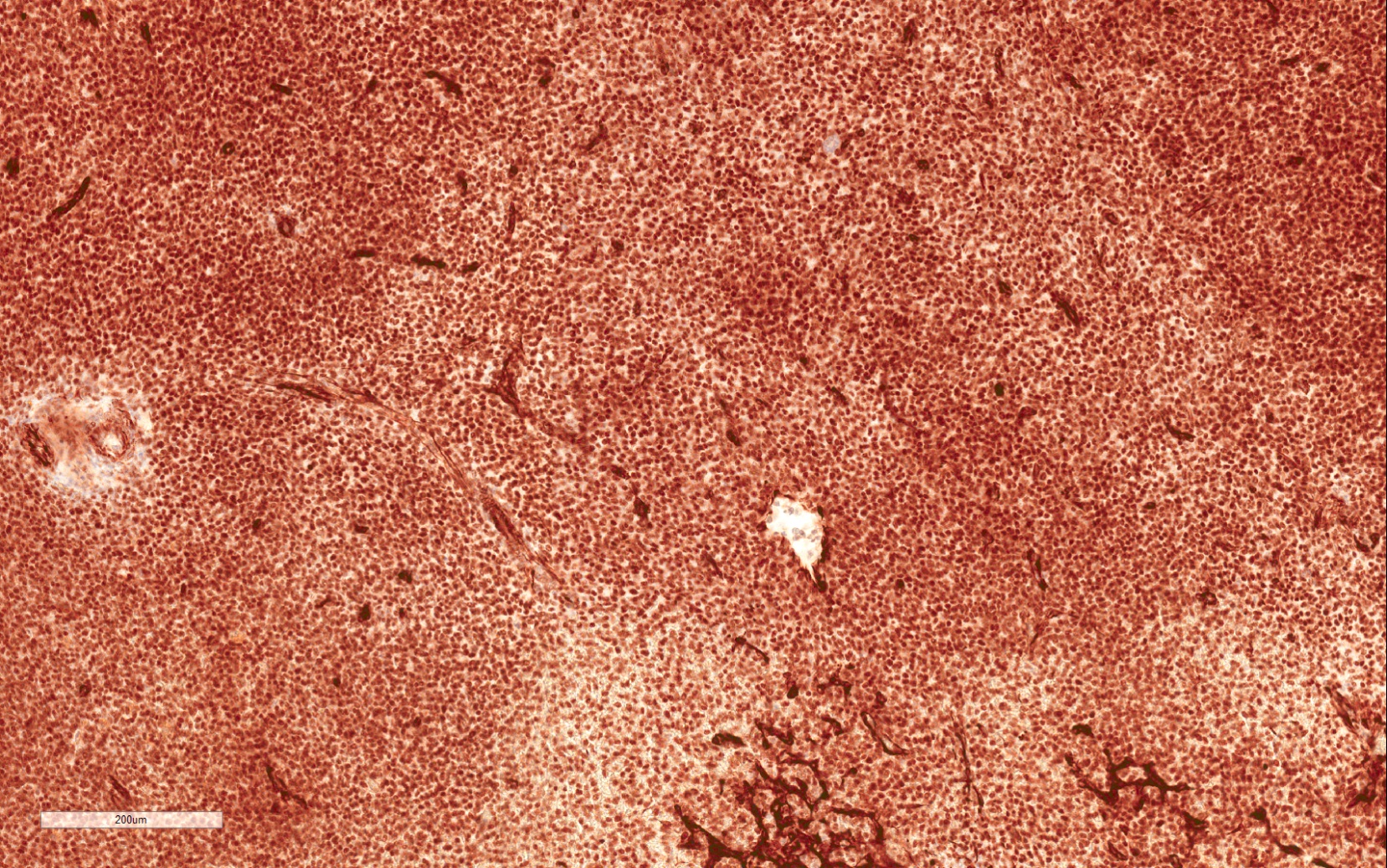
WT1+
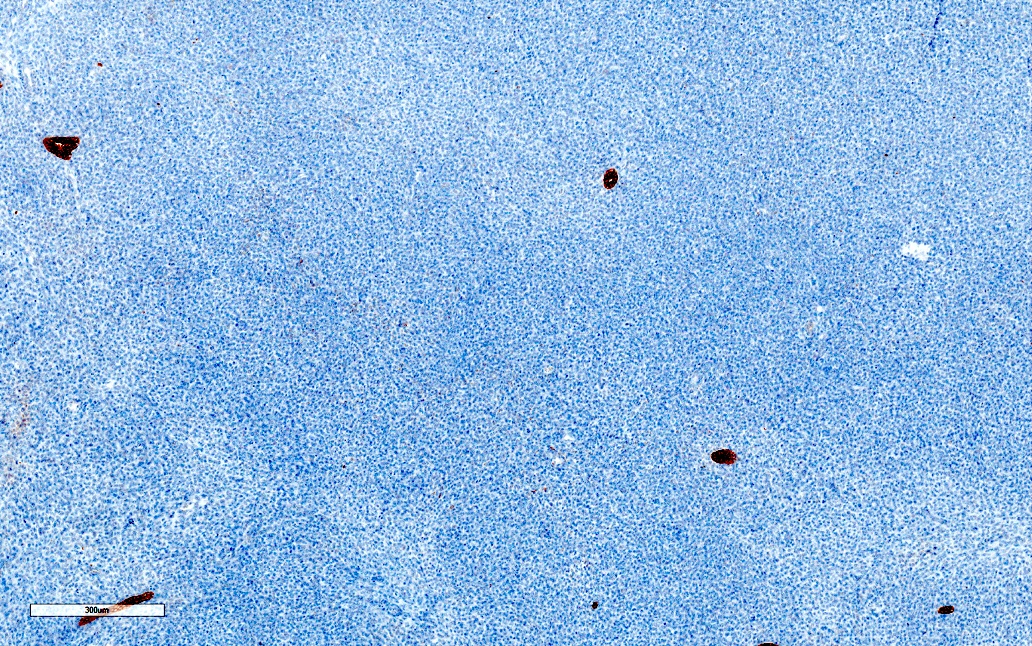
AE1 / AE3-
Positive stains
- Immunohistochemistry is only reported in a limited number of cases
- EMA (osteoblast-like cells 8/9; blastema-like cells 0/9)
- Vimentin (osteoblast-like cells 8/9; blastema-like cells 4/9)
- S100 (osteoblast-like cells 1/1; blastema-like cells 0/1)
- Cytokeratin (osteoblast-like cells 2/4; blastema-like cells 0/4)
- WT1 (osteoblast-like cells 1/2; blastema-like cells 1/2)
- Desmin (osteoblast-like cells 1/3; blastema-like cells 0/3)
- Reference: Pediatr Dev Pathol 2017;20:511
Negative stains
Molecular / cytogenetics description
- Chromosome 4 trisomy: unknown significance (Pathol Res Pract 2016;212:1004)
Sample pathology report
- Kidney, total nephrectomy:
- Ossifying renal tumor of infancy (see comment)
- Comment: The tumor consists of a well defined mass with calcification and osteoid with osteoblast-like cells, blending with dense, blastema-like areas. The tumor does not infiltrate the renal sinus or perirenal fat. Tumor cells show strong and diffuse vimentin and EMA positivity in the osteoid component. This is a benign tumor, which requires no further treatment.
Differential diagnosis
- Wilms tumor (WT) with prominent heterologous osteoid differentiation:
- Other Wilms tumor components normally present
- WT1 does not differentiate
- Mesoblastic nephroma:
- Does not contain blastema-like cells
- Cartilage but not osteoid may be present
- Renal teratoma:
- Other tissues are present
Additional references
Board review style question #1
A 6 month old boy presents with a painless macroscopic hematuria that was noticed by his parents. Imaging studies show a right sided calcified mass in the renal pelvis. Total right nephrectomy is performed. Both histology (microscopic image shown above) and imaging fit with the very rare entity, ossifying renal tumor of infancy. Which is the most characteristic pathologic finding for this tumor?
- Infiltrative intrarenal growth
- Numerous mitoses
- Osteoid with osteoblast-like and blastema-like cells
- Unique immunohistochemical profile
Board review style answer #1
C. Osteoid with osteoblast-like and blastema-like cells. The combination of those components with or without a spindle cell component is characteristic for ossifying renal tumor of infancy.
Comment Here
Reference: Ossifying renal tumor of infancy
Comment Here
Reference: Ossifying renal tumor of infancy
Board review style question #2
Which of the following describes the biological behavior of ossifying renal tumor of infancy?
- Benign
- High grade malignant
- Low grade malignant
- Uncertain / undetermined malignant potential
Board review style answer #2
