

Kidney nontumor / medical renal
Vascular disease
Vasculitis
Pauci-immune complex crescentic glomerulonephritis / ANCA associated vasculitis
Author: Ana Belén Larqué, M.D., Ph.D.
Editorial Board Member: Nicole K. Andeen, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 11 January 2021
Last staff update: 11 January 2021
Copyright: 2019-2024, PathologyOutlines.com, Inc.
PubMed Search: ANCA related glomerulonephritis

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Immunohistochemistry & special stains | Immunofluorescence description | Immunofluorescence images | Electron microscopy description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Larqué A. Pauci-immune complex crescentic glomerulonephritis / ANCA associated vasculitis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneyANCArelatedgngen.html. Accessed November 26th, 2024.
Definition / general
- Pauci-immune necrotizing crescentic glomerulonephritis related to or caused by antineutrophil cytoplasmic antibody (ANCA)
Essential features
- Pauci-immune necrotizing crescentic glomerulonephritis (renal biopsy: gold standard)
- Rapidly progressive glomerulonephritis with hematuria and proteinuria
- Small vessel necrotizing vasculitis associated with ANCAs that can be renal limited or with systemic vasculitis: granulomatous with polyangiitis, microscopic polyangiitis, eosinophlic granulomatous with polyangiitis or renal limited vasculitis (J Am Soc Nephrol 2010;21:1628)
Terminology
- Pauci-immune glomerulonephritis
- Pauci-immune crescentic glomerulonephritis
- ANCA associated vasculitis
ICD coding
- ICD10: NO1.7 - rapidly progressive nephritic syndrome with diffuse crescentic glomerulonephritis
Epidemiology
- By far the most common cause of rapidly progressive glomerulonephritis in adults (Kidney Int 2003;63:1164)
- 80% of pauci-immune crescentic glomerulonephritis is associated with ANCA (Kidney Int 2003;63:1164)
- Crescentic glomerulonephritis occurs in 75 - 80% of patients with granulomatosis with polyangiitis, 80 - 100% of microscopic polyangiitis and 25 - 40% of eosinophilic granulomatosis with polyangiitis (Semin Arthritis Rheum 2005;35:95, Clin Rheumatol 2017;36:1949)
- Age: > 60 years (53%); 21 - 60 years (39%); < 20 years (8%) (Kidney Int 2003;63:1164)
- No gender predilection
- Geographic variation of antimyeloperoxidase and proteinase 3 (PR3) ANCA (Mod Rheumatol 2010;20:54)
Sites
- Kidney glomeruli
Pathophysiology
- ANCA is a primary pathogenic factor, mainly by augmenting leukocyte endothelial interactions (Mod Rheumatol 2010;20:54)
- In vitro evidence:
- ANCA IgG can activate cytokine primed neutrophils by interacting with myeloperoxidase (MPO) or PR3 at the surface of the cells
- Endothelial injury by ANCA activated neutrophils and disruption of glomerular capillary walls
- Alternative complement pathway activation by ANCA activated neutrophils (Nat Rev Rheumatol 2014;10:463)
Etiology
- Trigger for ANCA production generally unknown
- Presumed immune dysregulation (Th17 / Treg) (Eur J Immunol 2017;47:724)
- Microbial factors and molecular mimicry (J Immunol Res 2015;2015:858027, Nat Med 2008;14:1088)
- Can be precipitated by drugs: propylthiouracil, hydralazine, minocycline, levamisole adulterated cocaine (Curr Opin Rheumatol 2014;26:42, Curr Opin Rheumatol 2013;25:50)
- Suggested risk factors
- Distinct HLA class II associations for MPO and PR3 ANCA (Am J Kidney Dis 2013;62:1176)
- Leptin receptor gene (LEPR) polymorphism (Rheumatology (Oxford) 2010;49:907)
- CTLA4 and PTPN22 (single nucleotide polymorphisms) (BMC Med Genet 2009;10:121)
- Epigenetic control of MPO and PR3 expression, both neutrophil cytoplasmic enzymes (J Clin Invest 2010;120:3209, Presse Med 2015;44:e223)
Clinical features
- Rapid deterioration of renal function
- Oliguria, hematuria and proteinuria (usually nonnephrotic range)
- Flu-like syndrome common at onset (fever, arthralgia, myalgia)
- Signs of extrarenal vasculitis in ~ 75% (Mod Rheumatol 2010;20:54, Semin Arthritis Rheum 2005;35:95)
- Microscopic polyangiitis: renal involvement (90%), lung usually affected, also skin, ear, nose, throat, musculoskeletal, nervous system, gastrointestinal
- Granulomatosis with polyangiitis: kidney, upper airway and lung involvement in 90% of cases
- Eosinophilic granulomatosis with polyangiitis: four phases - allergic, eosinophilic, vasculitic, postvasculitic (Colvin: Diagnostic Pathology - Kidney Diseases, 2nd Edition, 2015)
Diagnosis
- Rapidly progressive glomerulonephritis clinically
- Pauci-immune crescentic glomerulonephritis pathologically
- Positivity for ANCA (Clin Rheumatol 2017;36:1949)
- Extrarenal clinical manifestations in systemic vasculitis
Laboratory
- Positive ANCA test by indirect immunofluorescence plus enzyme linked immunosorbent assays in serum
- Sensitivity of 80% and specificity of 96% for pauci-immune glomerulonephritis
- Negative ANCA in ~ 20% of pauci-immune glomerulonephritis
- Type of ANCA does not permit specific diagnosis
- MPO ANCA most common in pauci-immune glomerulonephritis, microscopic polyangiitis and eosinophilic granulomatosis with polyangiitis (50 - 60%)
- PR3 ANCA most common in granulomatosis with polyangiitis (~ 75%)
- Other (atypical) ANCA specificities described
- React with lactoferrin, elastase and P-cathepsin-G in serum
- Found in variety of conditions with chronic inflammation or infection
- Negative ANCA associated with absence of disease activity
- Normal complement levels in serum
- Peripheral eosinophilia in 10 - 20% of microscopic polyangiitis
- References: Kidney Int 2000;57:846, Clin Rev Allergy Immunol 2013;45:109
Prognostic factors
- ~ 75% achieve remission
- ~ 30% relapse, frequently with PR3 ANCA
- 60 - 75% 5 year patient and kidney survival
- Risk factors for early death
- Higher serum creatinine or dialysis dependence at onset
- Female gender
- Age > 65 years (J Am Soc Nephrol 2006;17:1224, Clin Exp Rheumatol 2004;22:S94, J Am Soc Nephrol 2010;21:1628)
- Pathological prognostic features
- Number of normal glomeruli (strong predictor of renal function)
- Active lesions are associated with renal recovery: active glomerular necrosis and crescents, higher in granulomatosis with polyangiitis
- Chronic lesions are associated with poor renal prognosis: glomerulosclerosis higher in microscopic polyangiitis or MPO ANCA than in granulomatosis with polyangiitis or PR3 ANCA patients (Clin Rheumatol 2017;36:1949, Nephrol Dial Transplant 2005;20:96)
Case reports
- 19 year old woman with PR3 vasculitis presenting with symptomatic renal wedge infarction (BMC Nephrol 2019;20:84)
- 55 year old man with MPO ANCA associated necrotizing glomerulonephritis in rheumatoid arthritis (J Nephropathol 2017;6:58)
- 59 year old man with myeloperoxidase ANCA negative microscopic polyangiitis with pulmonary hemorrhage and IgA nephropathy (Case Rep Dermatol 2011;3:22)
- 66 year old woman with de novo ANCA associated vasculitis after renal transplantation (BMC Nephrol 2018;19:270)
- 67 year old woman with giant cell arteritis and granulomatosis with polyangiitis (Am J Case Rep 2018;19:651)
- 78 year old woman with ANCA associated necrotizing glomerulonephritis overlapping with mesangial proliferative lupus nephritis (Case Rep Rheumatol 2018;2018:3076806)
Treatment
- Cyclophosphamide and prednisolone to induce remission
- Maintenance therapy with less toxic drugs such as mycophenolate mofetil, azathioprine
- Plasmapheresis or plasma exchange in refractory cases
- Rituximab (anti-CD20) for induction or relapses (Nat Rev Rheumatol 2014;10:484)
Microscopic (histologic) description
- Pathological classification (J Am Soc Nephrol 2010;21:1628)
- Focal (> 50% normal glomeruli)
- Crescentic (> 50% cellular or fibrocellular crescents):
- Crescents containing > 10% cellularity included
- Fibrous crescents not counted
- Mixed (heterogeneous glomerular lesions, none predominating as > 50%)
- Sclerotic (> 50% global glomerulosclerosis, defined as > 80% of capillary tuft sclerosed)
- Focal segmental fibrinoid necrosis (glomerular basement membrane is disrupted in areas of necrosis)
- Extracapillary proliferation with the accumulation of macrophages and epithelial cells in Bowman space (age of crescents: cellular, fibrocellular, fibrous)
- Karyorrhectic debris and fibrin thrombi are frequently seen within the affected glomerular capillary lumens
- Active periglomerular inflammation and rupture of Bowman capsule
- Sometimes periglomerular granulomatous inflammation
- Normal glomeruli usually present
- Endocapillary hypercellularity, typical of immune complex mediated glomerulonephritides, is lacking
- Variable inflammation, predominantly composed of lymphocytes, histiocytes, plasma cells and sometimes brisk number of eosinophils
- Granulomas suggest the possibility of underlying granulomatous with polyangiitis or eosinophilic granulomatous with polyangiitis
- Note that an apparent interstitial granuloma adjacent to a disrupted Bowman capsule does not carry the same connotation
- Vasculitis 5 - 35%; involves small arteries, arterioles, capillaries, venules
- Interlobular arteries usually site affected in systemic vasculitis
- Leukocytoclastic vasculitis pattern (neutrophils, fibrinoid necrosis)
- Necrotizing, leukocytoclastic angiitis of the medullary vasa recta (frequently associated with interstitial hemorrhage and the presence of neutrophilic tubulitis and neutrophils within tubular lumens) (Colvin: Diagnostic Pathology: Kidney Diseases, 2nd Edition, 2015, Zhou: Silva's Diagnostic Renal Pathology, 2nd Edition, 2017)
Microscopic (histologic) images
Contributed by Ana Belén Larqué, M.D, Ph.D.
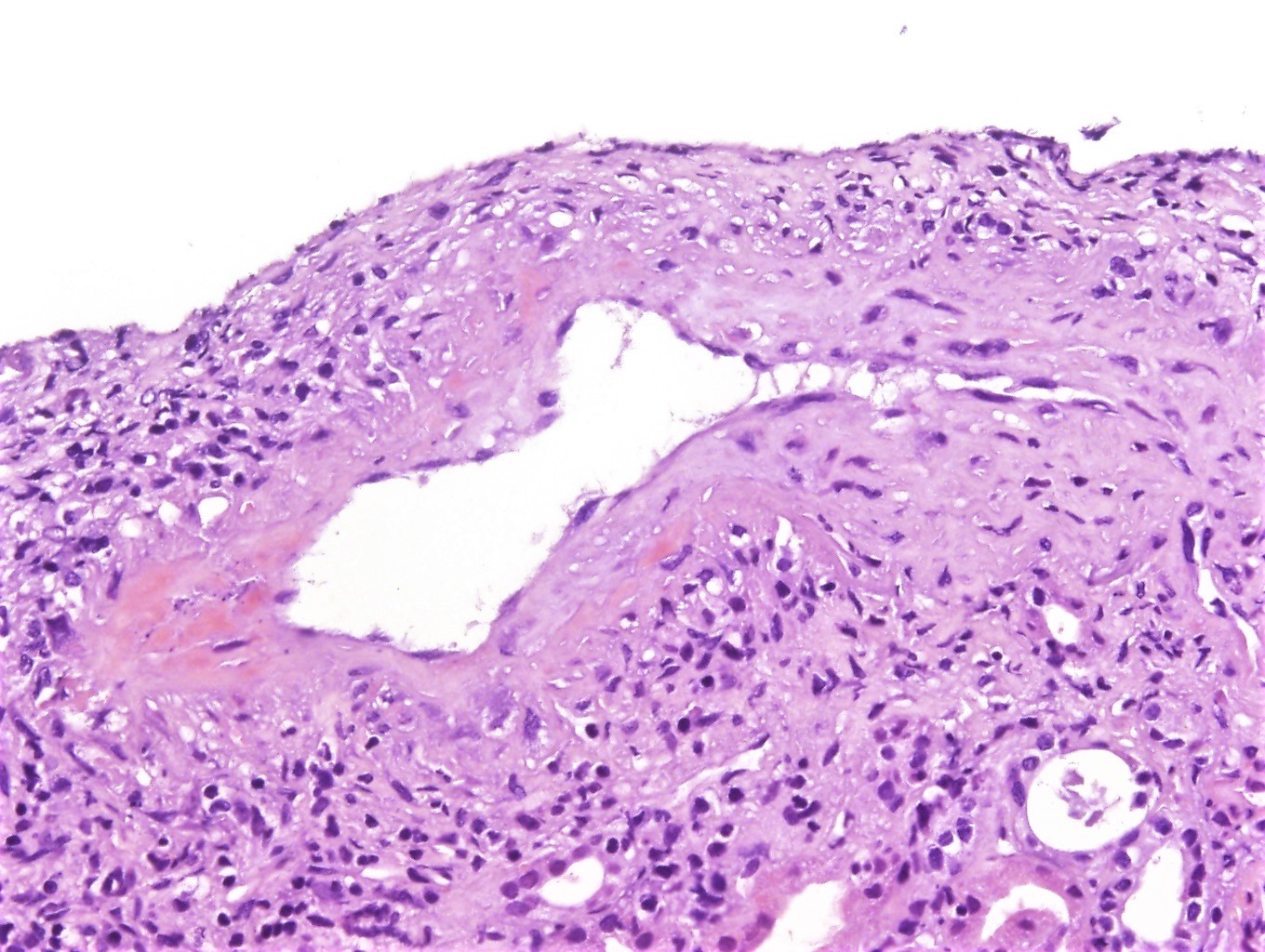
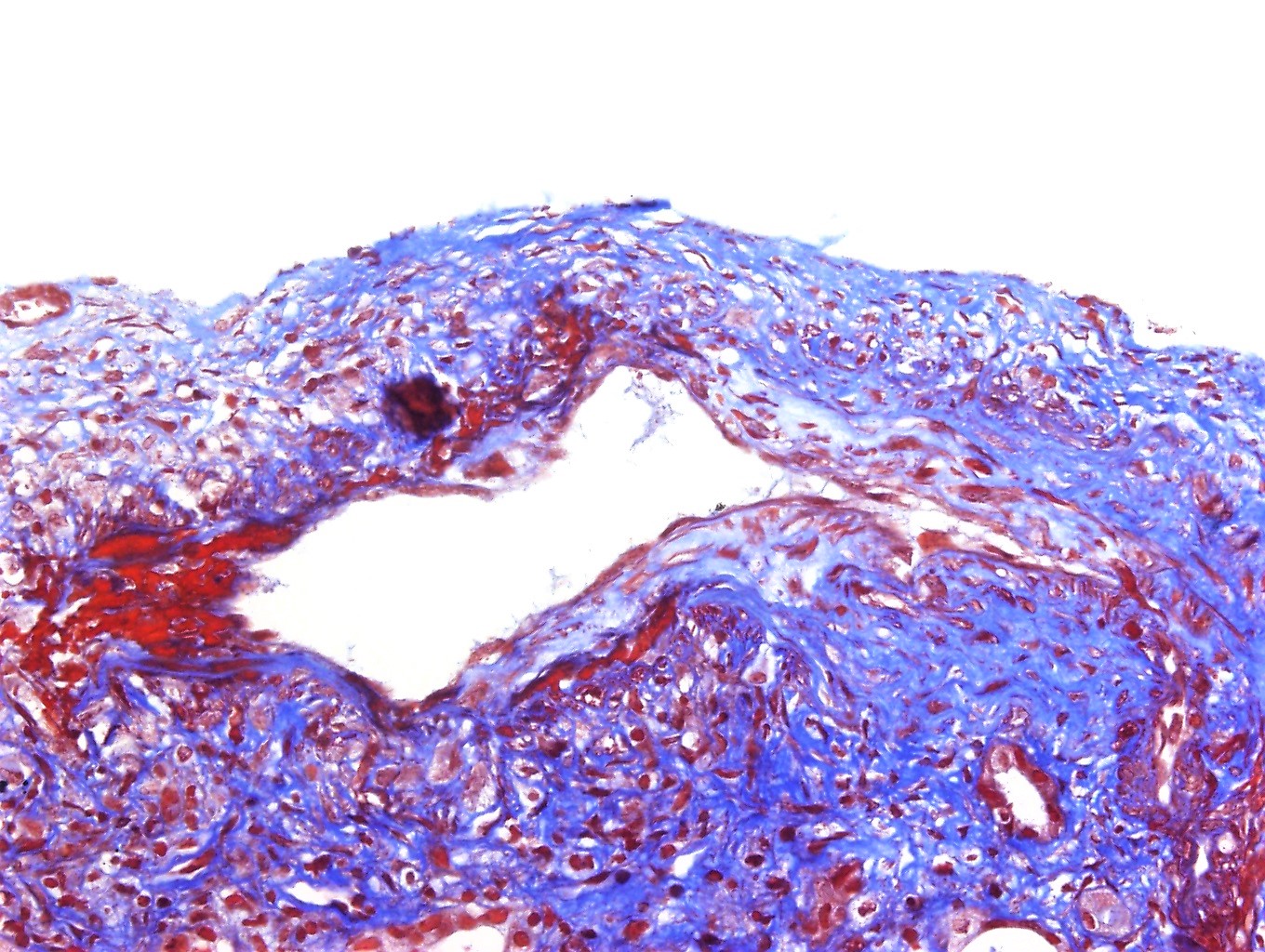
Arterial wall with fibrinoid necrosis
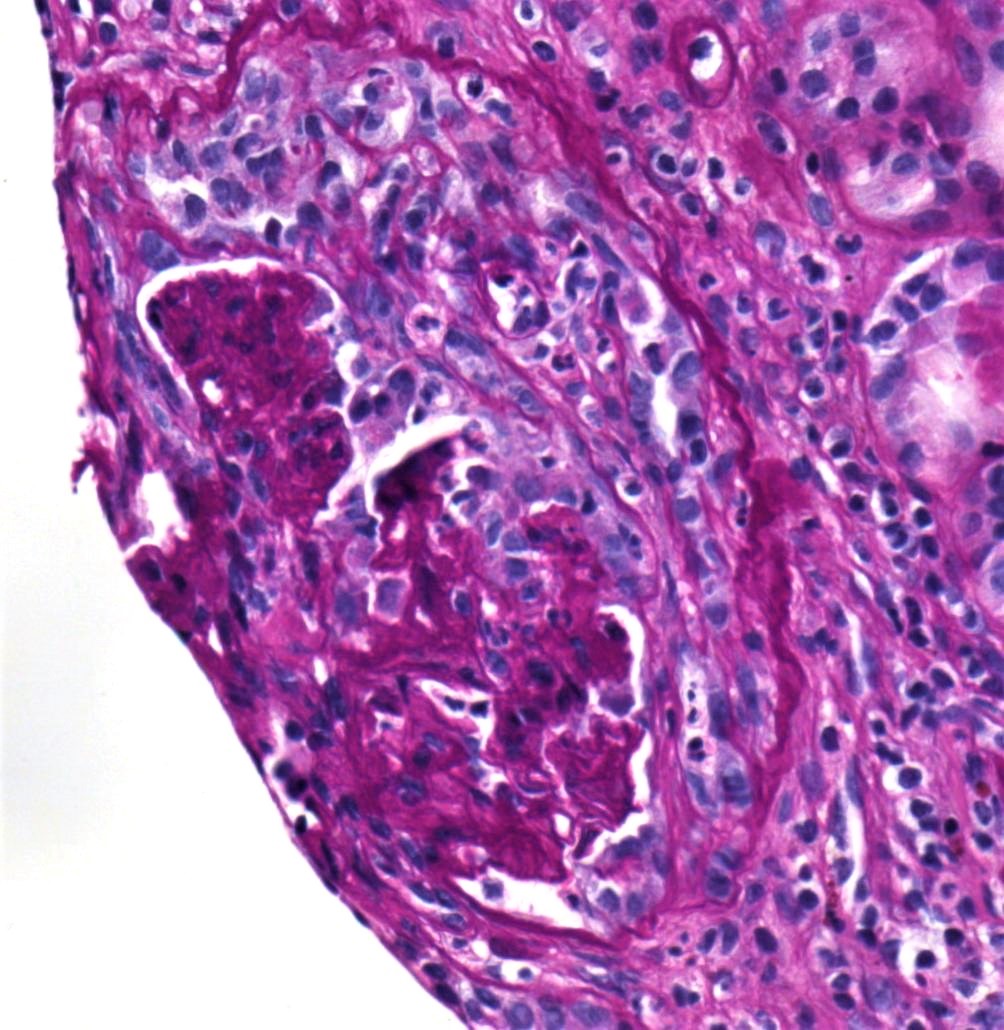
Cellular crescent
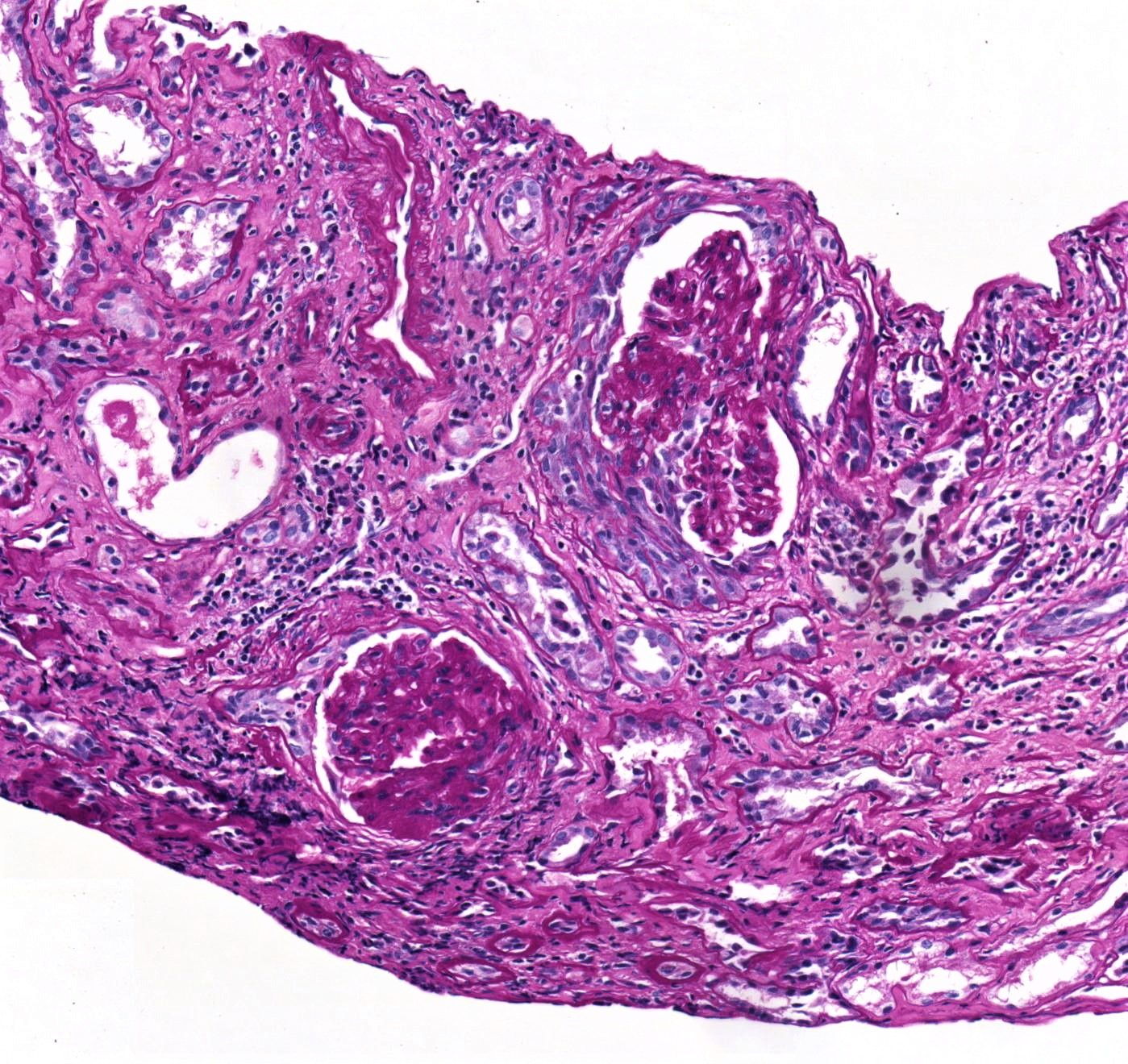
Crescents
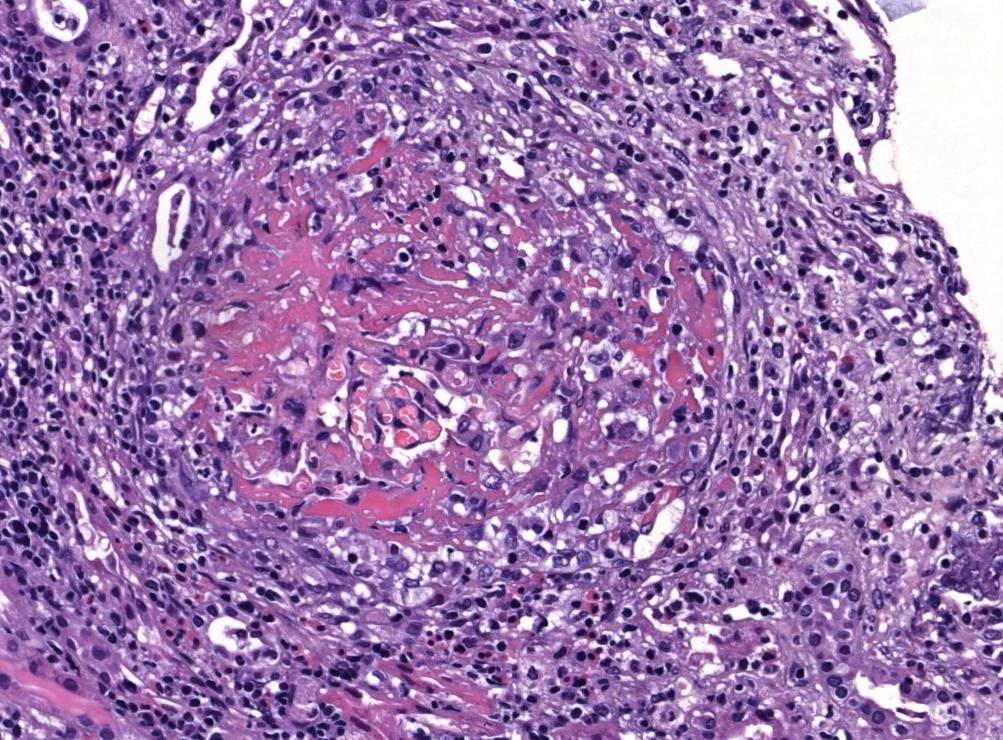
Segmental fibrinoid necrosis of glomerular tufts
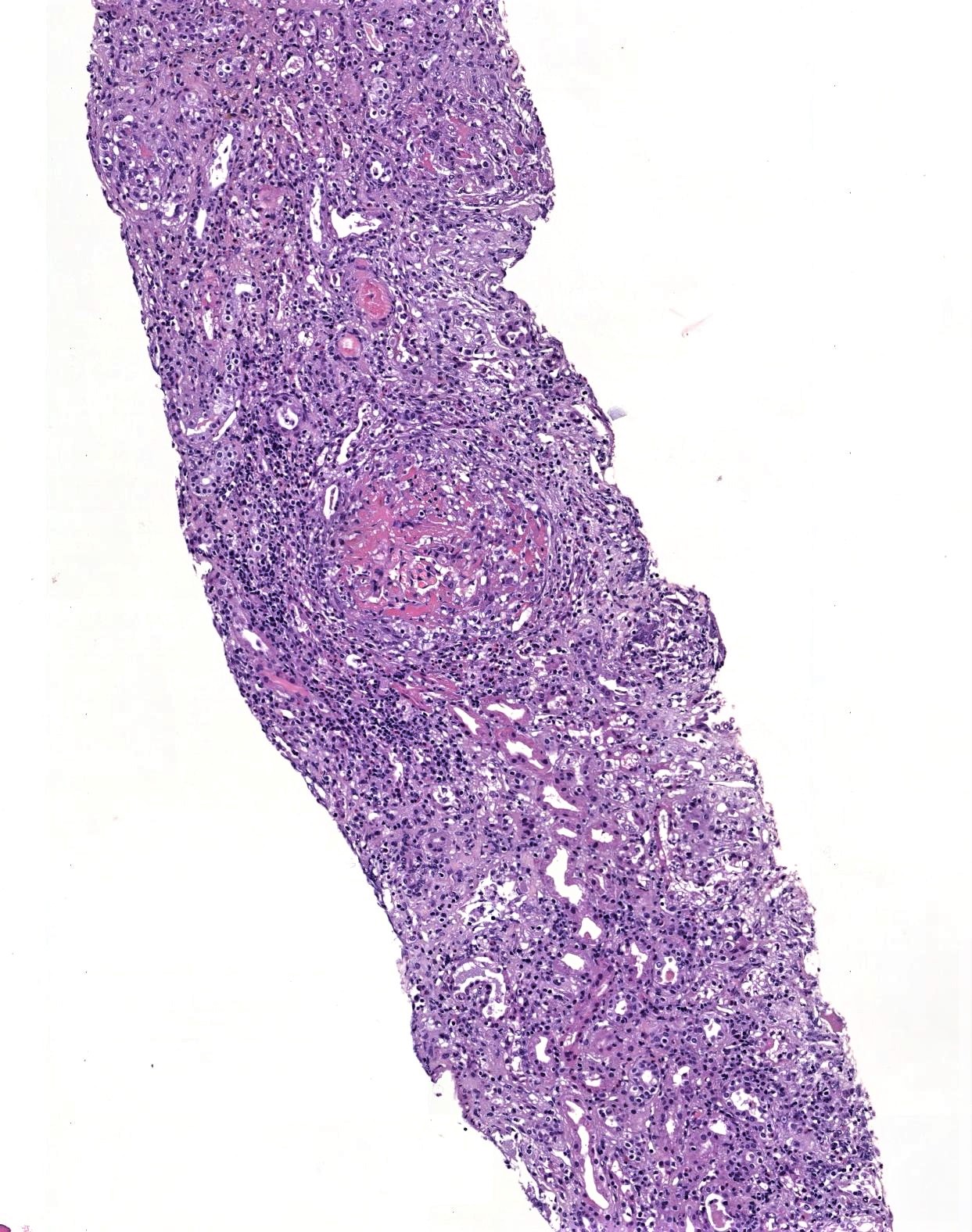
Interstitial inflammation
Immunohistochemistry & special stains
- Immunohistochemistry not used for diagnosis
- PAS, Jones silver and trichrome are used to evaluate morphology but are not specific for the type of glomerular disease
Immunofluorescence description
- Pauci-immune glomerular pattern (weak ≤ 1+) granular staining for IgG, IgM, IgA, C3 and C1q
- There is no evidence of glomerular immunodeposits
- Active crescents and fibrinoid necrosis stain for fibrin
- Reference: Am J Pathol 1989;135:921
Immunofluorescence images
Contributed by Ana Belén Larqué, M.D, Ph.D.
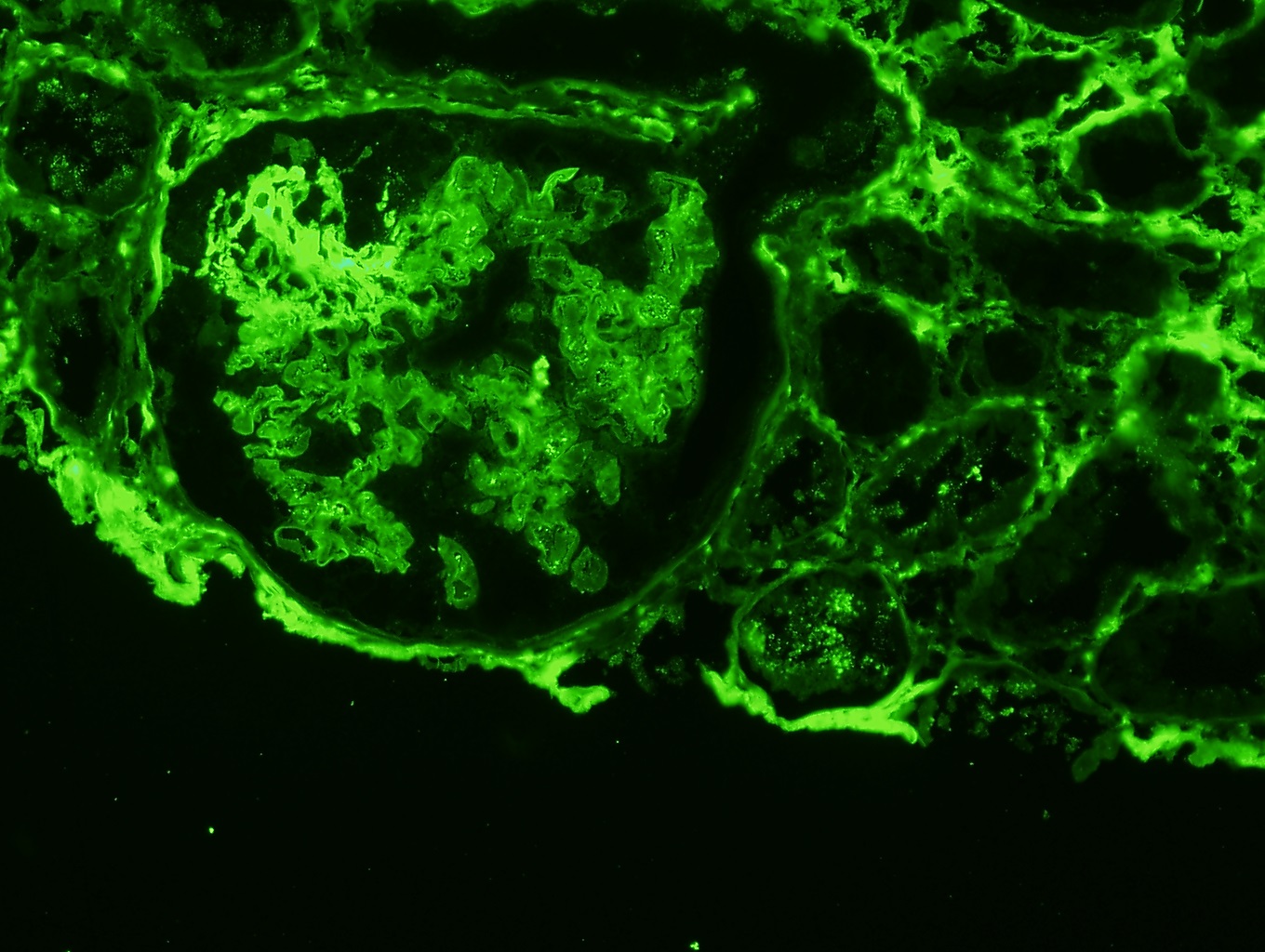
Segmental staining for fibrinogen
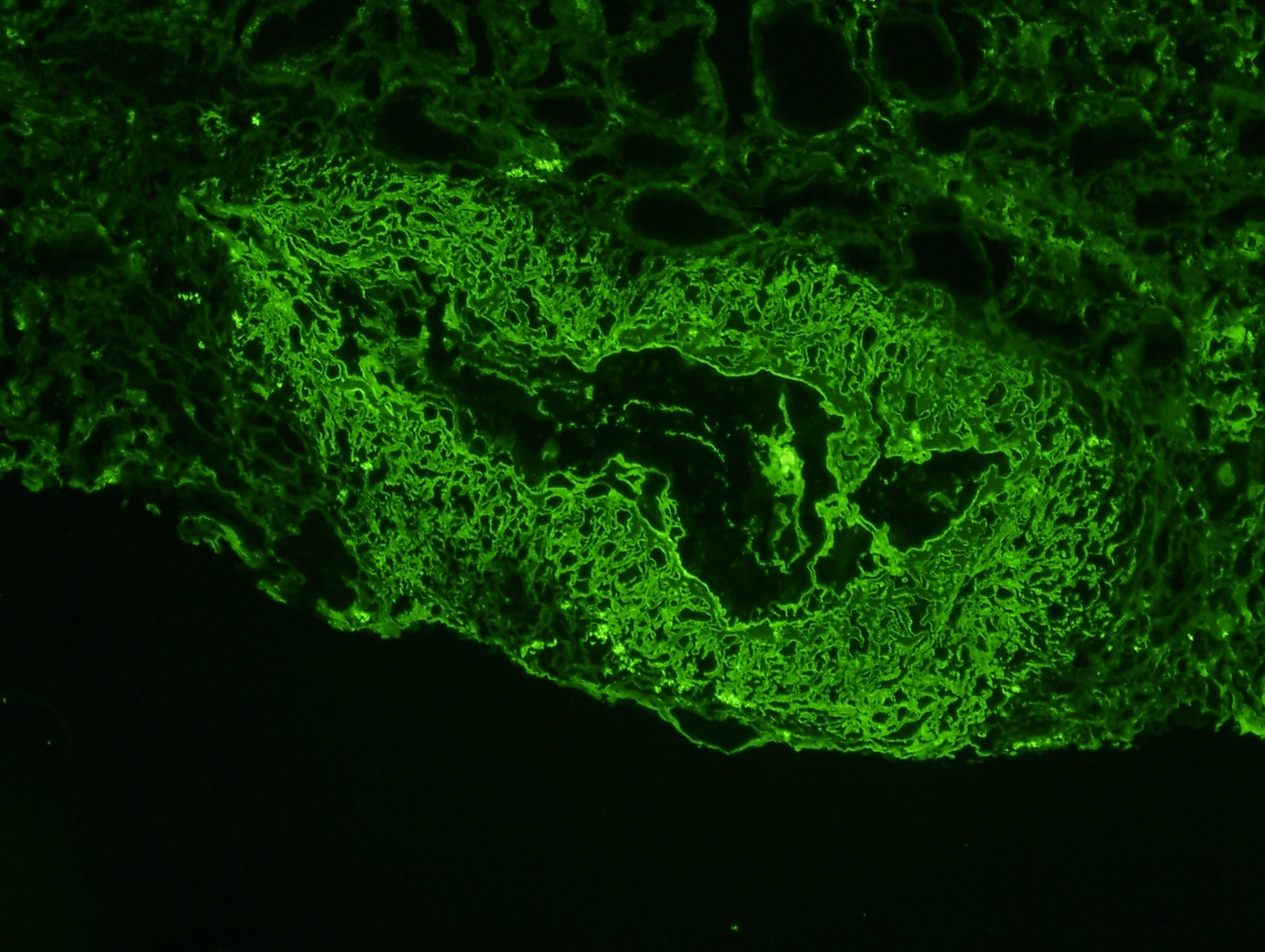
Arterial wall staining for fibrinogen
Electron microscopy description
- Electron microscopy generally contributes little, mainly recapitulating the changes seen on light microscopy
- Subendothelial edema, microthrombosis and degranulation of neutrophils are present but immune deposits are absent (J Am Soc Nephrol 2010;21:1628)
Sample pathology report
- Left kidney, biopsy:
- Focal necrotizing and crescentic ANCA glomerulonephritis
- Adequacy: adequate (cortex 80%, medulla 20%)
- Microscopic description: 13 glomeruli, 5 of these exhibited crescents (one with fibrinoid necrosis), including 2 cellular crescents and 3 fibrocellular crescents. Fibrosis occupying 30% of the interstitium with minimal lymphoplasmacytic infiltrate. There was no evidence of extraglomerular arteritis.
- Immunofluorescence microscopy: Number of glomeruli: 3. There were no deposits of IgA, IgM, IgG, C3, C1q or fibrin.
- Focal necrotizing and crescentic ANCA glomerulonephritis
Differential diagnosis
- ANCA negative crescentic glomerulonephritis:
- Serologic testing for ANCA negative
- Antiglomerular basement membrane disease (anti-GBM):
- Bright, linear staining of glomerular basement membranes for IgG
- Vasculitis absent
- Immune complex mediated crescentic glomerulonephritis:
- 2+ or greater of Ig and complement
- Some due to specific diseases such as lupus, cryoglobulinemia, IgA nephropathy, membranoproliferative glomerulonephritis
- ANCA superimposed on other diseases:
- Membranous glomerulonephritis, IgA nephropathy, lupus nephritis may have crescents and necrosis due to superimposed ANCA glomerulonephritis
- Drug induced pauci-immune crescentic glomerulonephritis (CEN Case Rep 2016;5:188)
- Thrombotic microangiopathies:
- Subendothelial widening along the glomerular capillaries with endothelial cell swelling and loss of fenestration by ultrastructural examination
Board review style question #1

- What is the most likely diagnosis on this biopsy?
- Focal segmental glomerulosclerosis
- Minimal changes disease
- Myeloma cast nephropathy
- Pauci-immune necrotizing and crescentic glomerulonephritis, ANCA associated
Board review style answer #1
D. Pauci-immune necrotizing and crescentic glomerulonephritis, ANCA associated
Comment Here
Reference: Pauci-immune complex crescentic glomerulonephritis / ANCA associated vasculitis
Comment Here
Reference: Pauci-immune complex crescentic glomerulonephritis / ANCA associated vasculitis
Board review style question #2
- Which of the following signs and symptoms are common in ANCA related glomerulonephritis?
- Edema
- Lipiduria
- Nephrotic range proteinuria
- Rapidly progressive renal failure
Board review style answer #2
D. Rapidly progressive renal failure
Comment Here
Reference: Pauci-immune complex crescentic glomerulonephritis / ANCA associated vasculitis
Comment Here
Reference: Pauci-immune complex crescentic glomerulonephritis / ANCA associated vasculitis

