

Heart & vascular pathology
Endocarditis
Noninfective endocarditis
Author: R. Amita, M.D.

Last author update: 1 April 2014
Last staff update: 31 December 2020
Copyright: 2014-2024, PathologyOutlines.com, Inc.
PubMed Search: Noninfective endocarditis [title]
Table of Contents
Definition / general | Terminology | Diagrams / tables | Epidemiology | Sites | Pathophysiology | Risk Factors | Clinical features | Diagnosis | Laboratory | Radiology description | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Differential diagnosis | Additional referencesCite this page: Amita R. Noninfective endocarditis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/heartnontumornoninfecendo.html. Accessed April 25th, 2024.
Definition / general
- First described by Zeigler in 1888, who called it "thromboendocarditis"
- In 1936, Gross and Friedberg coined the term "nonbacterial thrombotic endocarditis" (NBTE)
- Defined as vegetations on the valve surface, rich in fibrin and platelet aggregates but devoid of inflammation or infective organisms
Terminology
- Also called marantic endocarditis
Diagrams / tables
Images hosted on other servers:

Differences between NBTE and infective endocarditis
Epidemiology
- NBTE is uncommon but underestimated as symptoms are often attributed to other diseases
Sites
- Cardiac valves and endocardial surface
Pathophysiology
- Thrombotic endocarditis develops due to endothelial damage and subsequent exposure of the subendothelial connective tissue to circulating platelets
- The factors involved in pathogenesis can be divided into initiating NBTE and subsequent development of vegetation
- Factors implicated in initiation are: (a) immune complexes, (b) hypoxia, (c) hypercoagulability and (d) carcinomatosis
- Immune complexes: Libman-Sacks endocarditis is the prototype
- Hypoxia: studied by Nakanishi et al. in a rodent model (Virchows Arch 1998;433:375)
- Hypercoagubility: Trousseau first noted the association between thrombosis and malignancy
- Histological evidence of disseminated intravascular coagulopathy (DIC) has been found in 50% patients with NBTE
- Carcinomatosis: mucin producing adenocarcinoma from the gut, lung and ovary and acute promyelocytic leukemia are commonly associated with NBTE
Risk Factors
- Advanced stage malignancy: solid organ or hematological
- Chronic diseases: tuberculosis, uremia, AIDS
- Connective tissue disorders with hypercoaguable state: SLE patients with APLA positive
- Trauma from indwelling pulmonary catheter or central venous catheter, snake bite, late effect of radiation therapy
Clinical features
- There are no pathognomonic signs and symptoms that allow for the confident diagnosis of NBTE
- Patients can present with:
- Cardiac failure
- Secondary to valvular dysfunction (most commonly mitral regurgitation), leading to dyspnea, orthopnea, paroxysmal nocturnal dyspnea, peripheral edema, lethargy
- Cerebrovascular embolism
- Focal weakness or numbness, visual loss, dysphasia, dysarthria, dysphagia, memory loss
- Systemic thromboembolism
- Pain, coldness and numbness of the peripheries, or acute abdominal syndromes with pain and vomiting
- Secondary infective endocarditis
- Fever, weight loss, night sweats, lethargy, chest pain
- Cardiac failure
Diagnosis
- Requires a high degree of clinical suspicion in a patient treated for infective endocarditis (IE) and not clinically improving
- Mckay and Wahler proposed a triad for diagnosis of NBTE:
- Presence of a disease process known to be associated with NBTE
- Presence of heart murmur and
- Evidence of multiple systemic emboli
- Main differential diagnosis is Infective endocarditis - distinction is important
Laboratory
- Exclude DIC: full blood count, prothrombin time, partial thromboplastin time, fibrinogen, thrombin time, D dimers and cross linked fibrin degradation products
- These may be normal, but in the presence of risk factors, an abnormal result should alert the physician to a diagnosis of NBTE
- Multiple blood cultures to rule out any infective cause
- Immunological assays for antiphospholipid syndrome (APS)
- Polymerase chain reaction (PCR) for rapid and reliable detection of culture negative endocarditis by fastidious organisms
Radiology description
- Transoesophageal echo (TEE) has a higher sensitivity (90%) than transthoracic echo (TTE), especially for vegetations of < 5 mm
- Cardiac MRI using TrueFISP gradient echo sequence allows the morphology of small heart structures such as valves to be examined in detail (J Comput Assist Tomogr 1996;20:613)
- Diffusion weighted MRI (DWI) can differentiate cardioembolic stroke caused by infective endocarditis from that of NBTE due to the lack of a cellular component in NBTE emboli
Prognostic factors
- Dependent on underlying disease activity and associated renal and myocardial dysfunction
Case reports
- Young woman (J Heart Valve Dis 2009;18:159)
- 43 year old woman with Libman-Sacks endocarditis in systemic lupus erythematosus (J Gen Intern Med 2008;23:883)
- 55 year old woman (J R Soc Med 2005;98:24)
- Extensive nonbacterial thrombotic endocarditis isolated to the tricuspid valve in primary antiphospholipid syndrome (J Am Soc Echocardiogr 2010;23:107)
- Nonbacterial thrombotic endocarditis in three members of a family (N Engl J Med 1997;336:1677)
Treatment
- Treatment is difficult - correction of the underlying cause is of paramount importance
- In patients with potentially curable cancer, coagulopathy should be corrected and, if there is no contraindication, these patients should be anticoagulated with heparin
- There are no guidelines for surgical intervention in patients with NBTE - decision is based upon individual case
Clinical images
Images hosted on other servers:
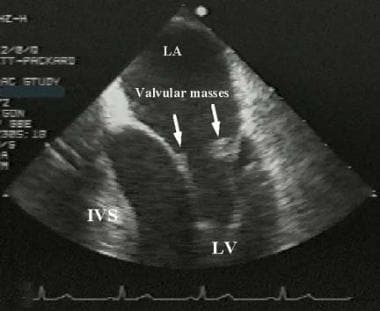
Mitral valve with masses

Mitral valve with mass

Enlarging mitral valve mass
Gross description
- NBTE vegetations are typically small, friable, white or tan masses, < 1 cm in diameter, broad based and irregular, usually along lines of valve closure on leaflets which may be normal or previously damaged
- Vary from tiny lesions to large and exuberant masses
- Based on morphology, Allen and Sirota proposed a macroscopic classification of NBTE:
- Type 1:
- Small, < 3 mm univerrucal, firmly attached to the valve
- Type 2:
- Large, > 3mm univerrucal, adherent to the valve
- Type 3:
- Small, 1 - 3mm multiverrucal, friable
- Type 1:
Gross images
Images hosted on other servers:

Typical finding

Typical appearances

Large NBTE vegetations
Microscopic (histologic) description
- NBTE consists of degenerating platelets interwoven with strands of fibrin and forming a bland, featureless eosinophilic mass except for a few trapped leucocytes
- Three stages have been described in the evolution of NBTE vegetations: (eMedicine: Libman-Sacks Endocarditis Workup [Accessed 28 February 2018])
- Active verrucae: Consist of clumps of fibrin on and within the valvular leaflet tissue which is focally necrotic, with plasma cells and lymphocytes
- Combined active and healed lesions: Contain vascularized, fibrous tissue adjacent to fibrinous and necrotic areas
- Healed lesions: Consist of dense, vascularized, fibrous tissue
Microscopic (histologic) images
Images hosted on other servers:

Uniform eosinophilic appearance
Differential diagnosis
