
Autopsy & forensics
Types of injuries
Gunshot wounds
Authors: Lorenzo Gitto, M.D., Robert Stoppacher, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 11 January 2021
Last staff update: 24 August 2021
Copyright: 2012-2024, PathologyOutlines.com, Inc.
PubMed search: Gunshot wound [TI] forensic pathology
Table of Contents
Definition / general | Essential features | Ballistics | Firearms | Bullets | Wound ballistics | Handgun wounds | Shotgun wounds | Rifle wounds | Gunshot wounds to the head | Medicolegal investigation of gunshot fatalities | Case reports | Clinical images | Microscopic (histologic) images | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Gitto L, Stoppacher R. Gunshot wounds. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/forensicsgunshotwounds.html. Accessed April 18th, 2024.
Definition / general
- Gunshot wounds occur when a bullet hits the body, producing injuries
- One of the most common causes of death and injury
- Severity of injuries depends on multiple factors, including the type of weapon and bullet and the affected body area
- May result in severe tissue and organ damage with sudden incapacitation, profuse bleeding, fractures and death
Essential features
- Determining the range of fire is one of the most critical parts of the forensic pathologist activity; secondary effects of the discharge surrounding the entrance wound (muzzle imprint, soot deposition, stippling or blackening of the skin edges) can help estimate the firing range
- Entrance wounds can be round, oval or irregular (atypical); an abrasion ring is almost always present
- Exit wounds are usually irregular and there is no abrasion ring in the vast majority of cases; there are no secondary effects of the discharge
- Wound mechanism and injury severity are mostly related to the kinetic energy transferred by the bullet to the tissues with the development of 2 cavities within the body: the permanent and temporary cavities
- At autopsy, it is essential to provide proper documentation (by photographs and body diagrams) of the gunshot wound's features
Ballistics
- Science that pertains to firearms and bullets; can further be classified as:
- Internal ballistics: what happens within the firearm from the deflagration to the exit of the bullet from the barrel
- External ballistics: the behavior of the bullet while traveling from the firearm to the final target
- Terminal ballistics: what happens when the bullet hits the final target; if the final target is a biological one, the term wound ballistics is used (Eur J Trauma Emerg Surg 2017;43:579)
Firearms
- Firearms of forensic interest can be generally classified as:
- Handguns (pistols and revolvers)
- Long guns (shotguns and rifles)
- Rifled: the barrel contains spiral lands and grooves into the inside of the barrel that grips the bullet as it exits the firearm, providing spin and stabilization along its path
- Smoothbore: the barrel is not rifled; typically found in shotguns
- Low velocity: usually fires at less than 1,000 ft/sec (Bull Emerg Trauma 2016;4:65)
- High velocity: usually fires at more than 1,000 ft/sec (Bull Emerg Trauma 2016;4:65)
Bullets
- During its travel, the bullet is subject to rotational forces causing:
- Yawing: oscillation of the bullet along its longitudinal axis (Forensic Sci Med Pathol 2009;5:204)
- Tumbling: bullet loses its gyroscopic stability, presenting a continually changing surface to the direction of motion (Forensic Sci Med Pathol 2009;5:204)
- Precession: rotation of the bullet around the center of mass (Forensic Sciences Research 2020;5:1)
- Nutation: circular movement of the tip of the bullet (Forensic Sciences Research 2020;5:1)
Wound ballistics
- When the bullet hits the biological target, it transfers its energy to the body, resulting in injuries
- Kinetic energy: the energy possessed by an object due to its motion; a function of the object's mass (M) and velocity (V): KE = 1/2 MV2
- While the bullet's mass plays an important role in gunshot wounds, the most critical variable is the bullet velocity; doubling the velocity will quadruple the kinetic energy
- Types of gunshot wounds:
- Penetrating wounds: the bullet enters the body but does not exit
- Perforating wounds: the bullet enters and exits the body
- Re-entry wounds: the bullet passes through a body segment, exits and re-enters the body (Int J Legal Med 2009;123:419)
- Graze / tangential wounds: the bullet strikes the skin at a shallow angle, producing a superficial wound (Acad Forensic Pathol 2016;6:291)
Handgun wounds
- Entrance wounds: point where the bullet enters the biological target
- General features:
- Abrasion ring: a reddish brown abrasion on the skin surrounding the gunshot wound of entrance
- Greasy rim or bullet wipe is a dirt collar due to the lubricant carried on the bullet
- Inverted edges: due to the bullet movement inside the body
- Smaller than bullet caliber (usually): due to the elastic recoil of the affected tissues
- Shape
- Round (circular) shape: suggests a perpendicular discharge with respect to the skin
- Oval shape: suggests an acute angle of fire with respect to the skin
- Atypical or irregular shape: indicates loss of stability of the bullet before hitting the target or hard contact gunshot wounds to the skin overlying bone (i.e. skull) (Am J Forensic Med Pathol 2012;33:250)
- Range of fire: determination by estimating the distance from the muzzle of the weapon to the target; specific findings on the skin (secondary effects of the discharge) surrounding the entrance wound can help determine the range of fire
- Thermal effect: due to the gas and flame produced by the deflagration; flames cause searing of the skin and regional hairs
- Soot deposition: due to the carbon produced by combustion of the gunpowder that exits the barrel and deposits on the skin surrounding the entrance wound; can be wiped out by cleaning the body
- Stippling (or powder tattooing): red to orange or brownish punctate abrasions surrounding the entrance wounds as a result of pieces of gunpowder expelled from the barrel and striking the skin; can't be wiped out by cleaning the body
- Pseudostippling: punctate abrasion due to fragmented bullets or fragments of a damaged intermediate target interposed between the firearm and the target (Am J Forensic Med Pathol 2003;24:243)
- Contact wounds: firearm is in contact with the target at the time of discharge
- Loose contact: circular wound with blackened, seared skin margins
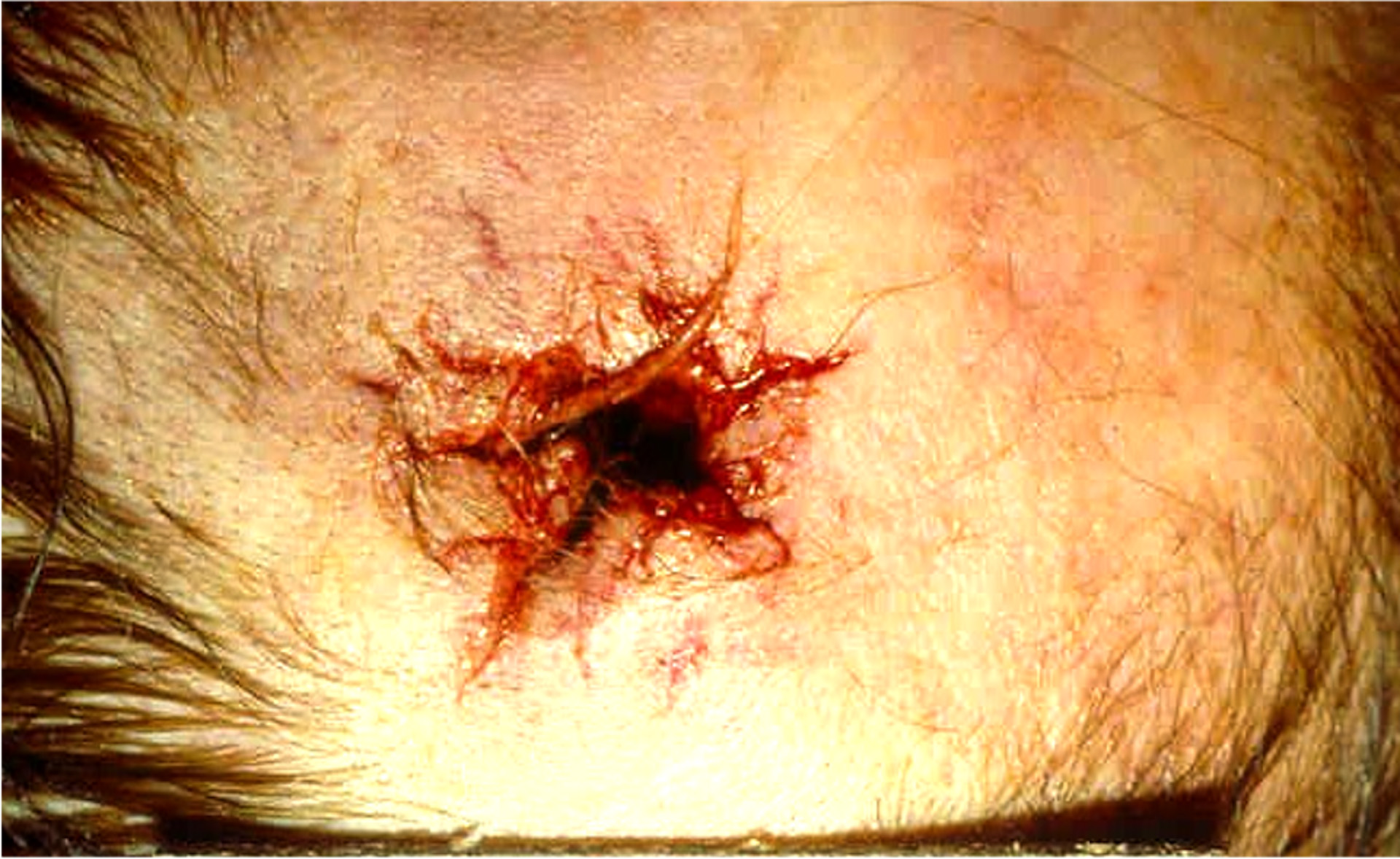
- Hard contact: gas expansion within the subcutaneous tissues may result in a muzzle imprint (abrasion resembling the shape of the muzzle = Werkgartner mark) or in an irregular, stellate appearance with a central defect and radiating lacerations (typically seen in gunshot wounds to the head) (Arch Kriminol 2009;224:145)
- Near contact wounds: firearm is not in contact with the target but is held a very short distance from it (usually < 1 cm)
- Entrance wound may show soot deposition and burn / seared edges; small amount of powder stippling can be present (Forensic Sci Int 2003;138:68)
- Intermediate range: distance between the firearm and the target increases but is still short enough to allow secondary effects of the discharge; distance depends on firearm type (usually from a few centimeters up to several feet)
- Hallmark is the presence of stippling (or powder tattooing) on the skin surrounding the entry wound (Arch Pathol Lab Med 2006;130:1283)
- Greater distance = larger area of stippling but its density will decrease
- Distant range: firearm is at a distance (many feet) from the target so there will be only the gunshot wound of entrance due to the mechanical action of the bullet
- There must be no stippling
- Usually round or oval, depending on the angle of discharge
- If there is an intermediate target between the firearm and the target, close or intermediate gunshot wounds can be confused with distant ones
- In the absence of reliable evidence of a distant range gunshot wound, it is preferable to classify it as an indeterminate range
- General features:
- Wound channel: path of the bullet within the body; after hitting the target, the bullet releases its energy to the body and creates 2 cavities (J Trauma 1985;25:522)
- Permanent cavity: primary wound channel caused by the tissue damage due to the bullet passage through the body; the final injury that can be observed at autopsy
- Temporary cavity: while the bullet travels through the body, the permanent cavity is stretched, causing progressive pulsations and contractions
- Energy is transferred to the surrounding tissues, causing damage even far from the primary bullet path
- After a variable amount of time, the temporary cavity collapses into the permanent cavity due to the elastic recoil of the biological tissues
- Temporary cavities are not identifiable at autopsy but effects can be observed on tissues and organs surrounding the permanent cavity
- Exit wounds: point where the bullet leaves the body
- Generally, an exit gunshot wound is more irregular in shape than entry wound
- Skin is perforated from the inside out, causing eversion of skin tags and protrusion of tissue from the defect
- Exit wounds do not show soot deposition, muzzle imprint, stippling or blackening of the skin edges
- Can be slit-like lesions that can mimic a stab wound
- Shored exit wound is one in which the skin is in contact with another object when the bullet exits (a belt, a wall, etc.); this causes an irregular area of abrasion on the skin, which can be confused with the abrasion ring of an entrance wound (Am J Forensic Med Pathol 2000;21:220)
Shotgun wounds
- When a shotgun is fired, a compact mass of shot or pellets emerges from the muzzle; dispersion is directly related to the distance increase
- Shotguns are usually smoothbore and fire pellets
- Most common shotgun pellets:
- Birdshots: smallest type of shotgun pellets; small, metal spheres
- Buckshot: larger metal spheres, giving greater weight and force to each pellet
- Some shotguns are rifled and fire slugs
- Slug: single, large projectile with high energy and penetration ability (Rom J Leg Med 2014;22:237)
- Entrance wounds (Am J Forensic Med Pathol 2007;28:99)
- Contact range: up to a few feet, the entrance wound is a single, round defect because the pellets penetrate the target as a single mass; soot deposition can be present, usually in a greater amount than the one produced by handguns
- Near contact: soot deposition, searing, reddish brown rim or skin blistering; wound is still round and regular
- Short distance: at a range of 3 - 4 feet, the pellets begin to spread out before reaching the body, producing one large entry wound that shows serrated or crenated edges (scalloping or rathole appearance)
- Intermediate to distant range: as the range increases, the central defect becomes smaller and is surrounded by several satellite pellet holes, which increase with the increasing distance; when the shotgun is far enough from the target, there will be no central defect but just pellet holes
- Wound channel
- Shape of the pellets does not allow for their stabilization, resulting in lower penetration ability
- In distant shotgun wounds, most of the damage is due to the permanent cavity, while there is a negligible secondary cavity effect
- In contact shotgun wounds, the secondary cavity effect is significant (i.e. intraoral shotgun wound)
- Exit wounds
- Shotguns firing pellets rarely produce exit wounds and mostly when fired at contact or short distance
- Slugs frequently produce exit wounds, since they are comparable to high velocity missiles with high penetration ability
Rifle wounds
- Generally used in the military field
- High velocity missiles: the secondary cavity effect accounts for the vast majority of the damage (J Trauma Acute Care Surg 2019;87:690)
- In contact wounds of the head with centerfire rifles, there is massive tissue destruction of the skin, skull and brain with a heterogenous pattern of entrance and exit wounds (Leg Med (Tokyo) 2016;23:10)
- Full metal jacketed bullets produce less tissue damage and tend to travel through the body undeformed
- Semijacketed ammunition creates the classic lead snowstorm appearance on Xray due to the peeling back of the jacket as it travels through the body, releasing numerous, small lead fragments
Gunshot wounds to the head
- In perforating gunshot wounds to the head, entrance and exit wounds show a typical feature called beveling, distinguishing between entrance and exit
- Beveling is a sort of cone shaped bone erosion in the direction of the bullet path through the cranial vault
- Entrance wounds can be round / oval or stellate in shape and show an internal beveling (bone erosion in the inner part of the bony table) (J Forensic Sci 1991;36:1592)
- Exit wounds are usually irregular and show an external beveling (bone erosion on the outer part of the bony table)
- Fragments of bone travel in the direction of the bullet path through the cranial vault
- In the skull, gunshot wounds often produce numerous fractures due to rapidly increasing pressure as the bullet travels through the skull
- Gunshot wounds to other flat bones can produce similar effects
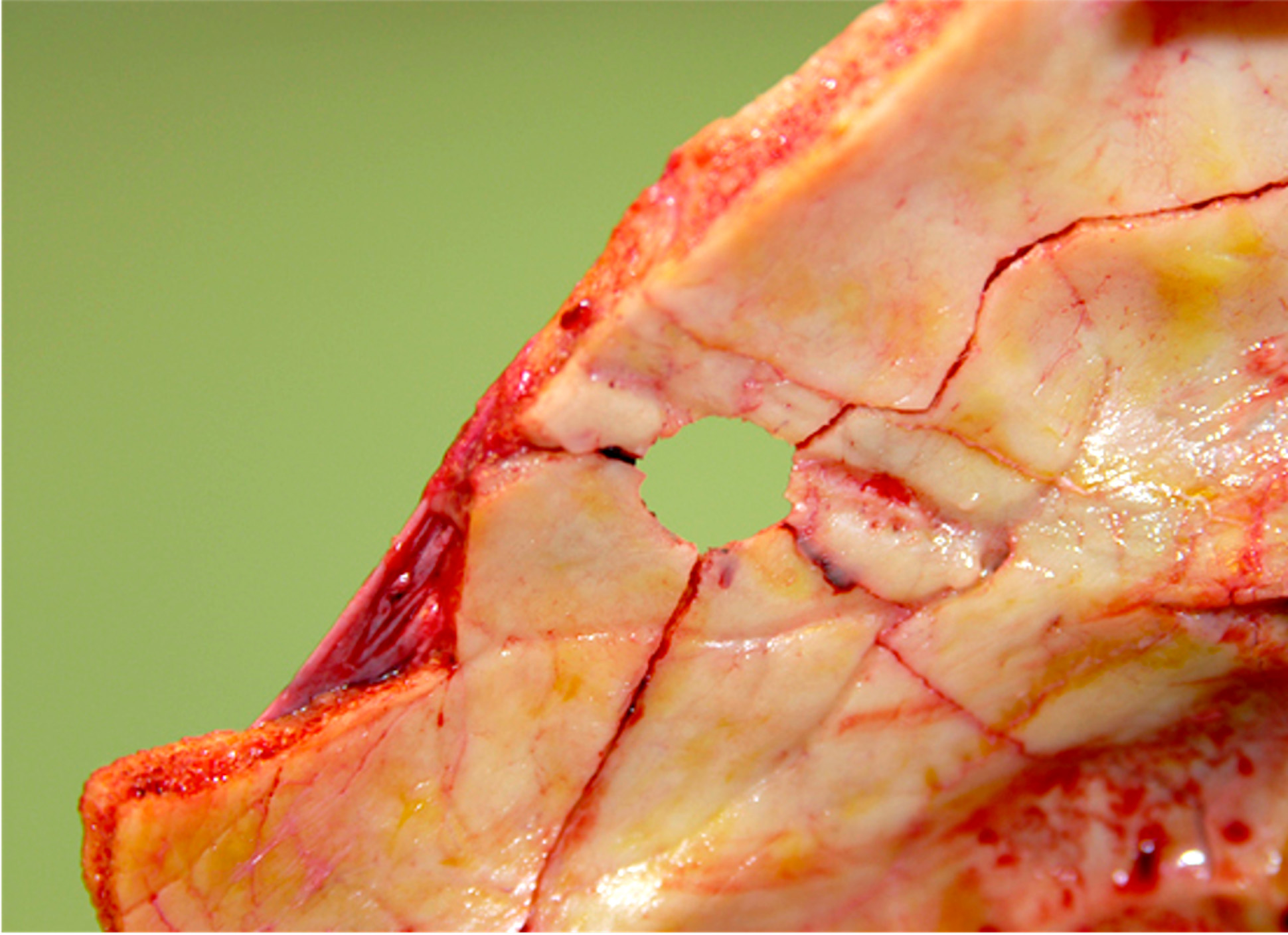
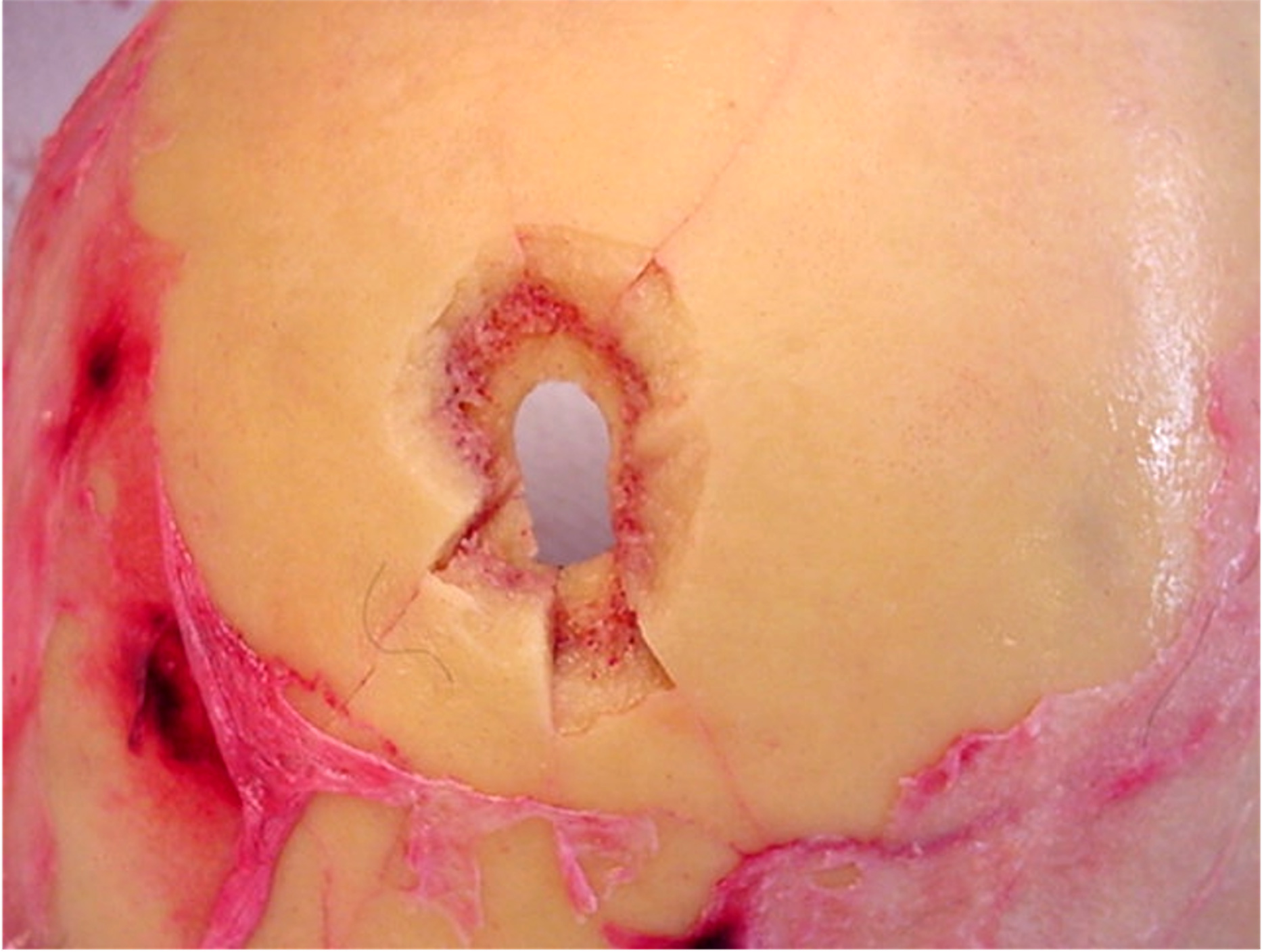
- Keyhole lesion: a single bone defect that shows both entrance and exit wound morphologies due to a bullet that strikes the skull at a shallow angle (Australian Journal of Forensic Sciences 2014;46:258)
- Distinguishing between entrance and exit wounds and determining the direction of fire can be challenging
- Even if the bullet does not penetrate into the cranial cavity, its energy is still transferred to the bone and central nervous system, resulting in fractures and severe damage
Medicolegal investigation of gunshot fatalities
- Scene investigation
- Before examining the body, observe, take photographs and document the environment
- Avoid any unnecessary procedures that can alter the scene or the body
- Search for a suicide note, medications and the weapon on the scene (Am J Forensic Med Pathol 1999;20:1)
- Analyze the blood spatter: passive stains, transfer stains or impact stains can give clues about the dynamic of the event (Data Brief 2018;22:269)
- Postmortem imaging
- Usually performed before the autopsy to detect and locate potential bullets or their fragments
- At least an Xray study should be performed in every gunshot wound death, since bullets or fragments need to be collected at the time of autopsy
- Postmortem computer tomography (virtopsy) gives more accurate information about the location of the bullet / fragments, providing a 3D view of the body; also allows for software manipulation of the CT scans (taking measurement, adding virtual probes, 3D reconstruction or other tools) (Leg Med (Tokyo) 2014;16:357)
- External examination and autopsy
- It is essential to provide a proper documentation (by photographs and body diagrams) and description of the following (Arch Pathol Lab Med 2006;130:1283):
- Body conditions before any alteration
- Clothes
- Entrance wound, wound channel and exit wound features
- Direction of fire: give 3 directions according to the main body axis (left / right, front / back and top / bottom)
- Any possible bullet or bullet fragments that are recovered within the body: the location must be reported and the bullet should not be recovered using metal forceps or other metal tools to avoid creating artificial marks on its surface
- Extremities: a small, linear abrasion / bruise can be present on the interdigital groove between the thumb and index finger (Felc mark), which can be due to the pinching of the skin between the sliding barrel and the handgrip; may suggest that the subject fired the shot
- It is essential to provide a proper documentation (by photographs and body diagrams) and description of the following (Arch Pathol Lab Med 2006;130:1283):
- Microscopic examination
- Rarely needed (Am J Forensic Med Pathol 2012;33:231)
- Used to distinguish between the entrance and exit gunshot wounds in unclear cases
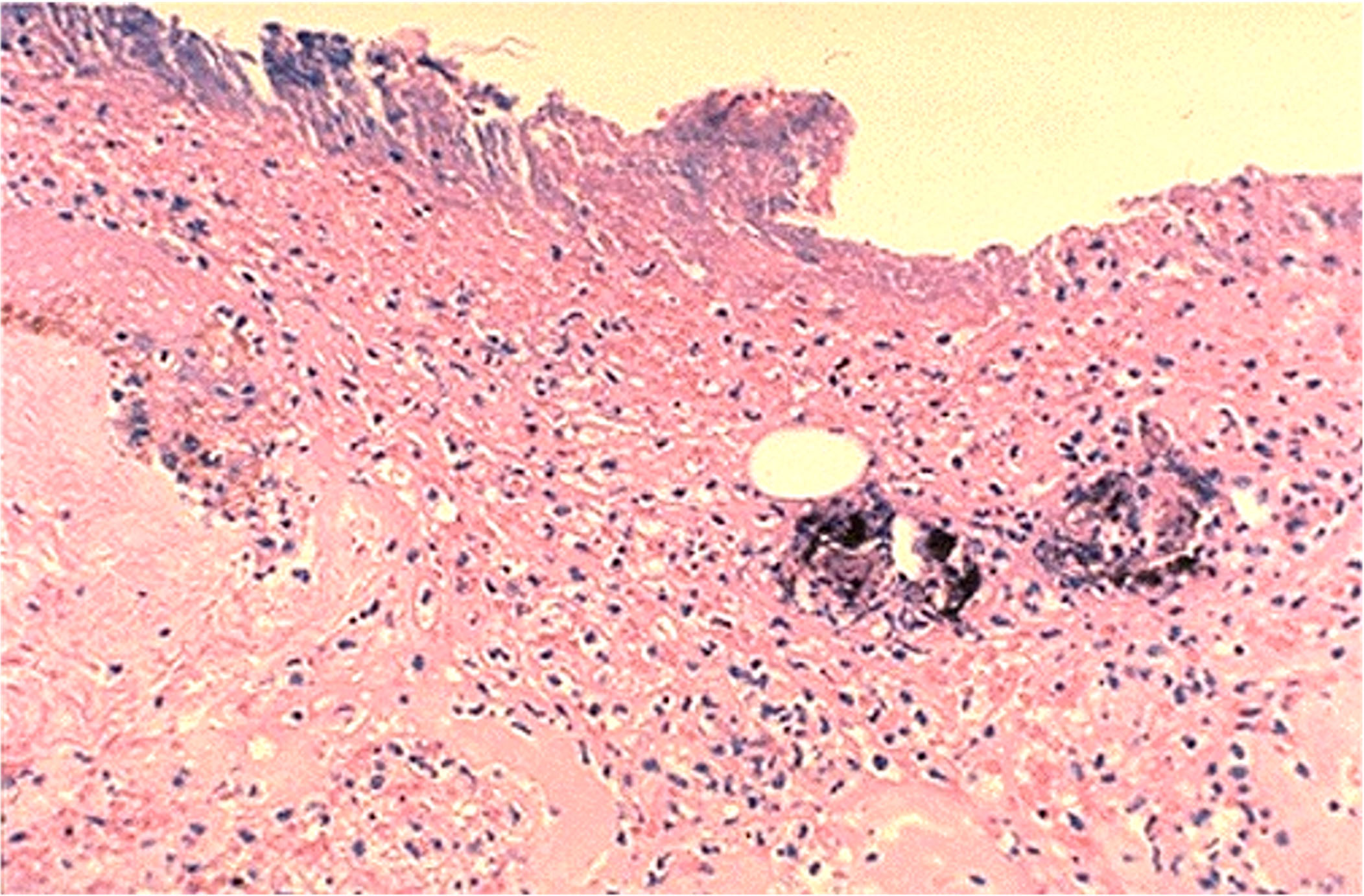
- Entrance wound: cell compression, nuclear streaming, epidermis and dermal thermal injury with coagulative necrosis of keratinocytes, dermoepidermal disjunction, hemorrhage (a sign of vitality); gunshot residues can be observed as a black granular material progressively decreasing from the entrance to the exit wound (Am J Dermatopathol 2016;38:566)
- Exit wound: fragments of bone, adipose tissue and muscle can be found, oriented toward the exit (J Forensic Leg Med 2014;25:49)
- Manner of death determination
- Suicide note, history of mental illness and weapon on the scene support suicide; however, an offender can place the weapon in the victim's hand or close to the body to simulate suicide (J Clin Diagn Res 2017;11:HD01)
- Multiple gunshot wounds generally support homicide; however, the subject may retain a certain amount of ability to act after multiple gunshot wounds (even when the head is involved) if targets of immediate incapacitation are spared (J Forensic Sci 2015;60:1373)
- Accidental fatal gunshot wounds are rare
Case reports
- 14 year old boy with tandem bullet wounds (Acad Forensic Pathol 2016;6:130)
- 28 year old man with atypical exit shotgun wound (Forensic Sci Int 2017;275:e1)
- 63 year old man suffers homicide by intraoral gunshot wound (Forensic Sci Med Pathol 2011;7:209)
- 2 cases of tandem bullets (Am J Forensic Med Pathol 2019;40:262)
- Suicide by 8 gunshot wounds to the head (J Forensic Sci 2015;60:1373)
- Bullet embolism (J Forensic Leg Med 2016;42:33)
Clinical images
Contributed by Lorenzo Gitto, M.D. and Robert Stoppacher, M.D.


Hard contact entrance gunshot wound

Loose contact entrance gunshot wound

Near contact entrance gunshot wound

Intermediate range gunshot wound

Distant (or indeterminate) range gunshot wound

Atypical entrance

Exit gunshot wound
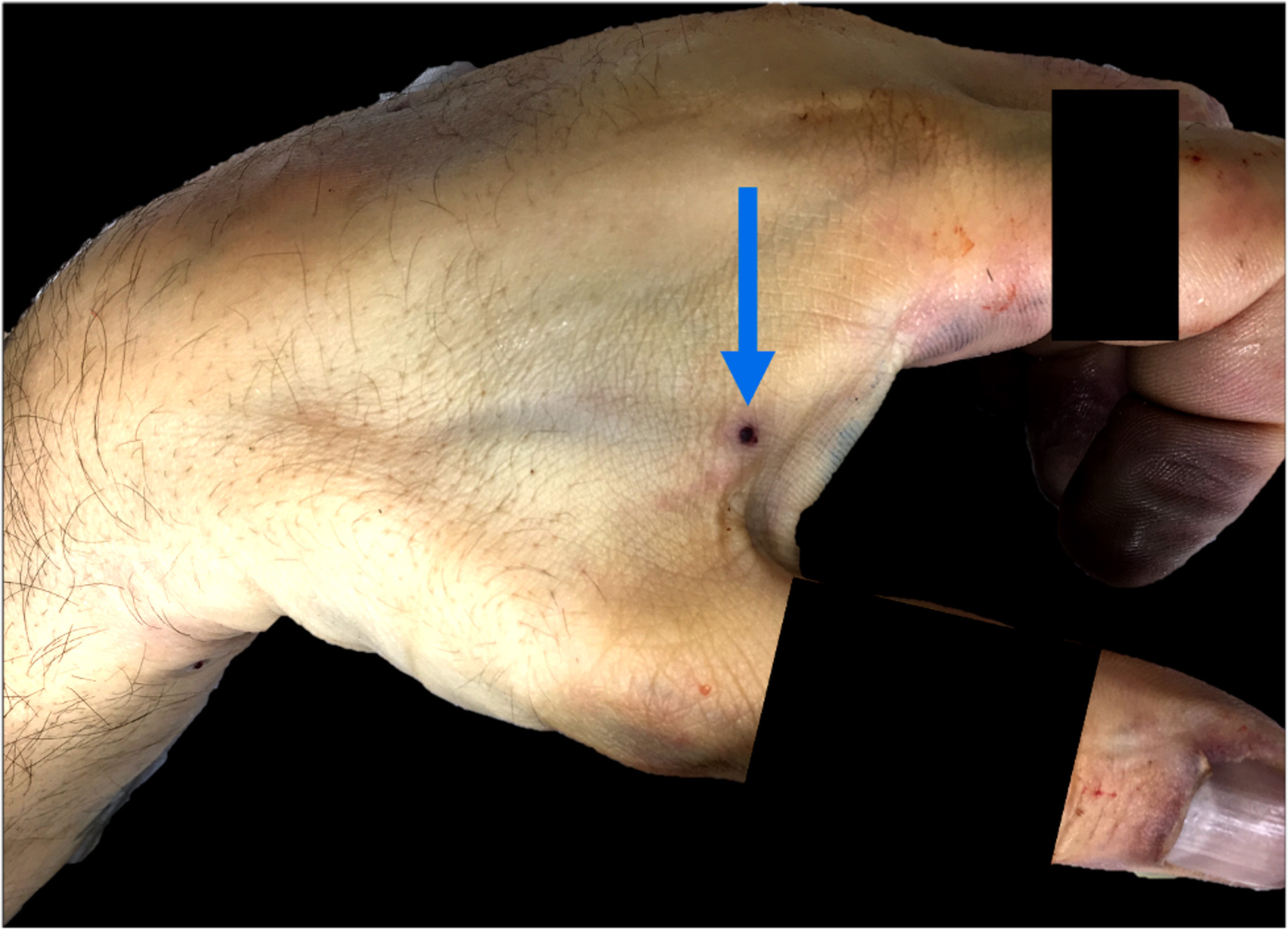
Felc mark

Graze wound

Contact shotgun entrance wound

Exit shotgun wounds
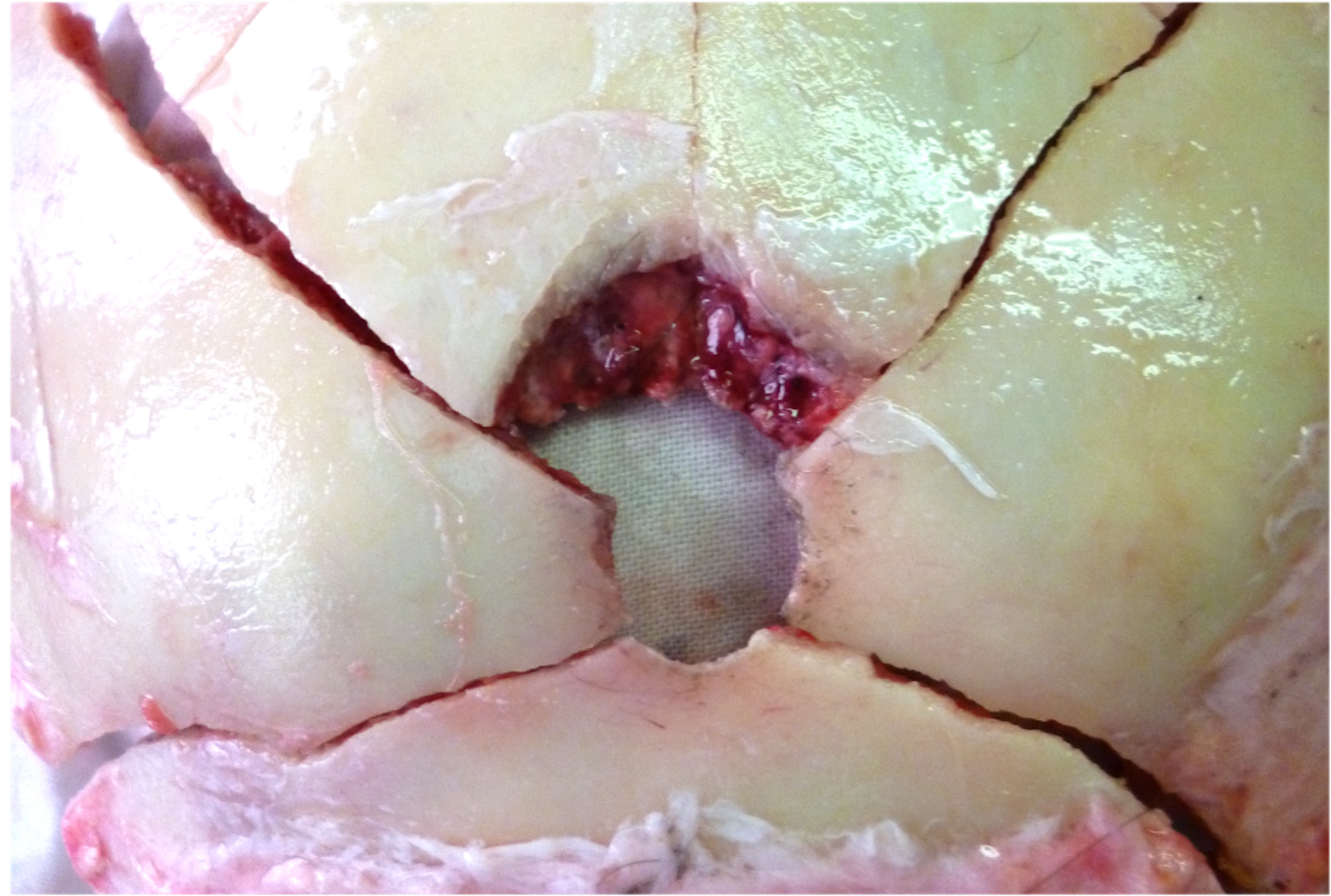
Keyhole lesion of the skull
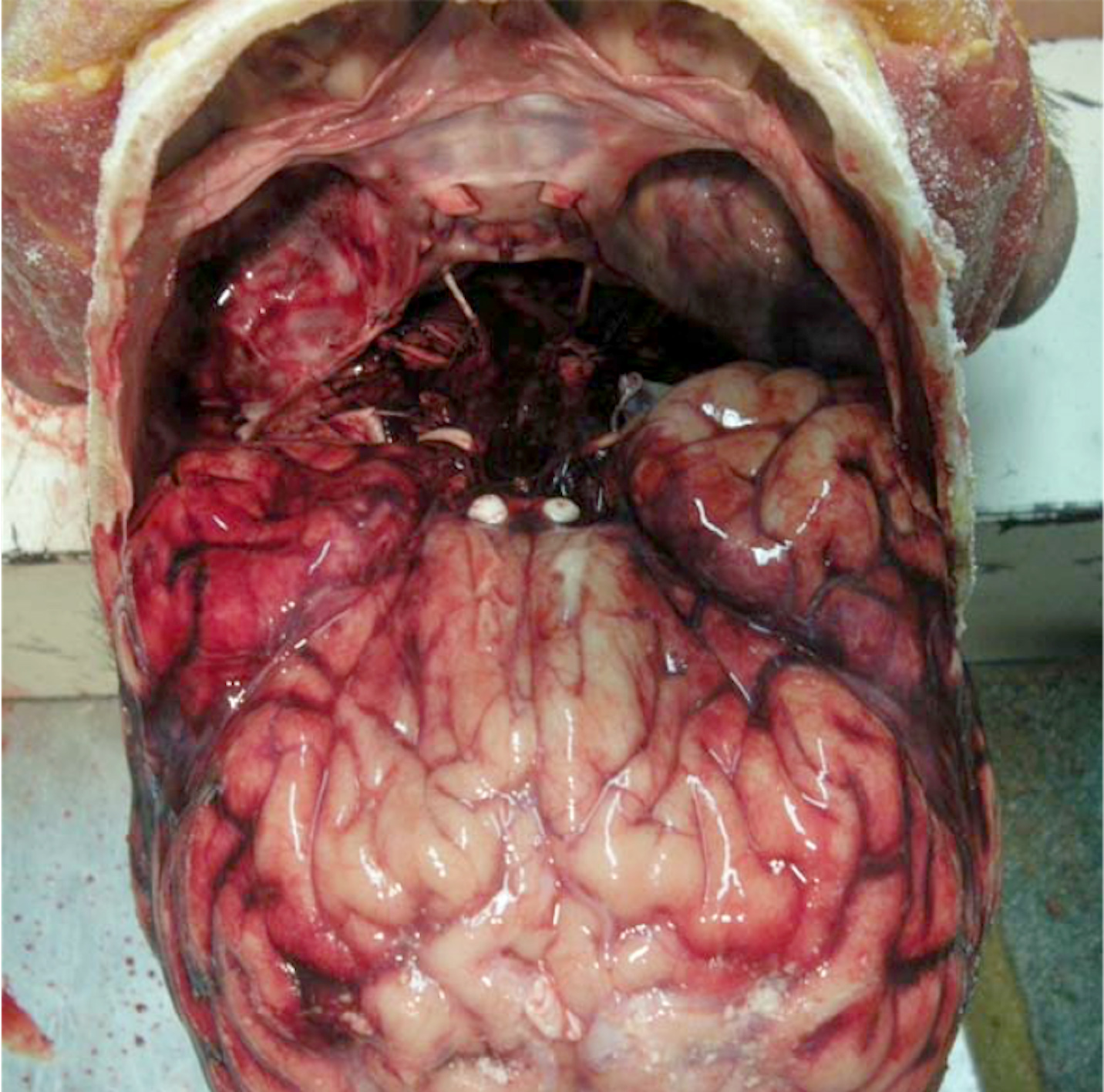
Gunshot wound to the head

Rifle wound to the thigh

Rifle wound to the face

Rifle wound to the face
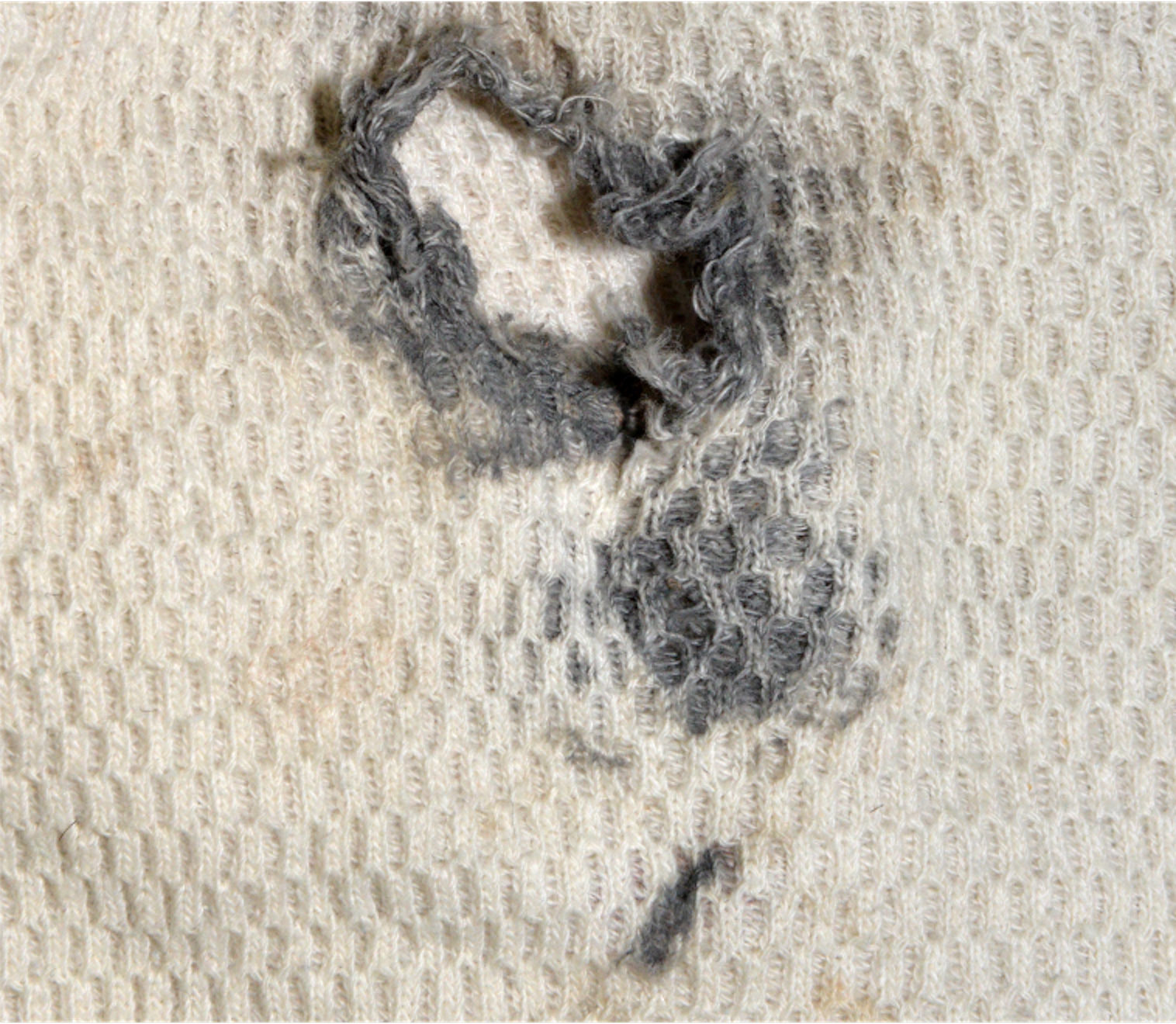
Clothes examination
Microscopic (histologic) images
Contributed by Lorenzo Gitto, M.D. and Robert Stoppacher, M.D.
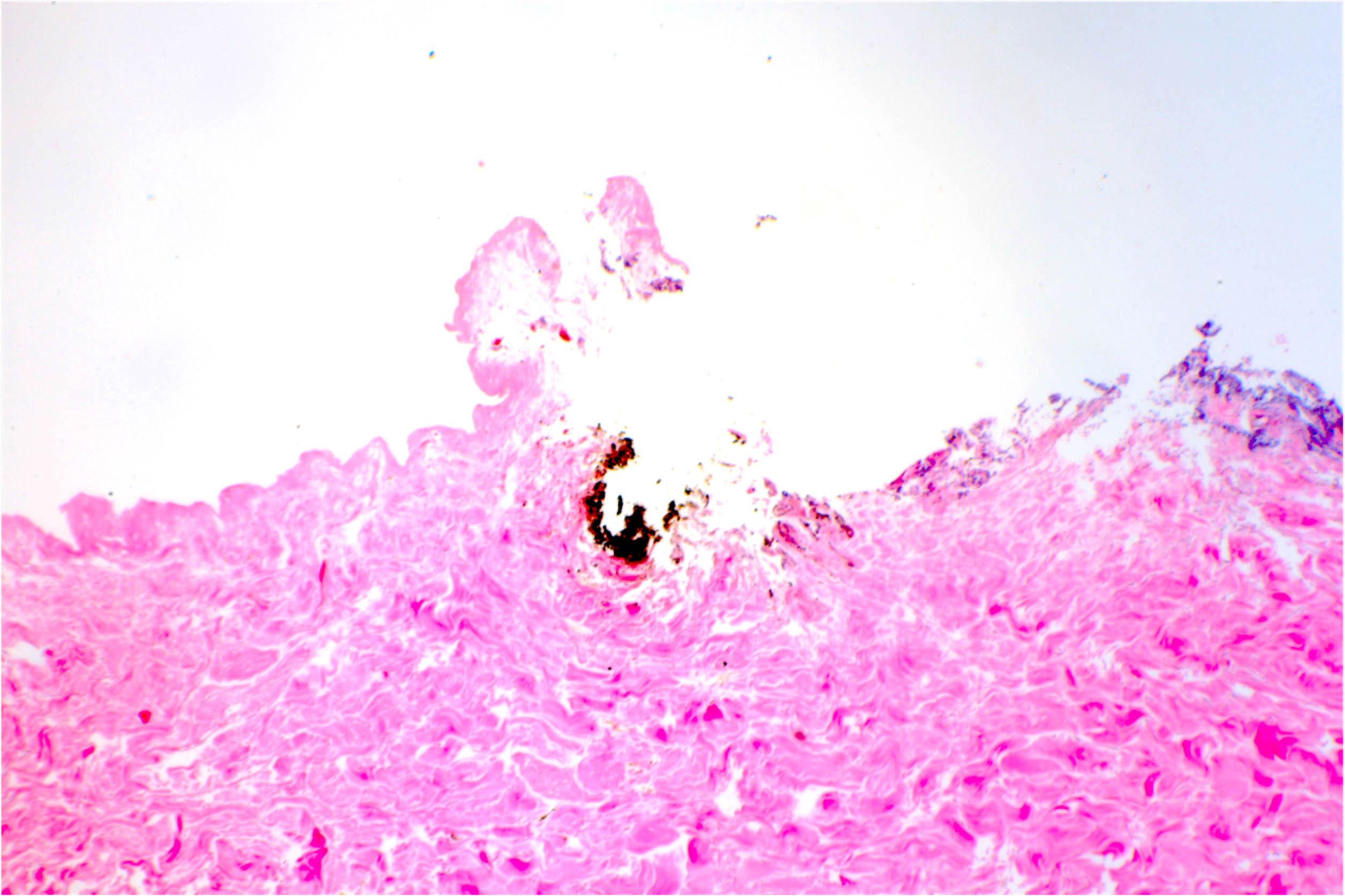
Gunshot entrance wound
Contact gunshot entrance wound
Additional references
- DiMaio: Gunshot Wounds - Practical Aspects of Firearms, Ballistics, and Forensic Techniques, 3rd Edition, 2015, Knight: Knight's Forensic Pathology, 4th Edition, 2015, Brooks: Ryan's Ballistic Trauma - A Practical Guide, 3rd Edition, 2011, Dolinak: Forensic Pathology - Principles and Practice, 1st Edition, 2005, Spitz: Spitz and Fisher's Medicolegal Investigation of Death, 4th Edition, 2005
Board review style question #1
The severity of a gunshot wound is mostly due to which of the following?
- Caliber of the bullet
- Kinetic energy of the bullet
- Location of the injury
- Shape of the bullet
- Weight of the bullet
Board review style answer #1
B. Kinetic energy of the bullet
The weight and the velocity of the bullet are the most critical variable in determining the amount of kinetic energy. Doubling the mass doubles the energy, while doubling the velocity quadruples it. However, the wound's ultimate extent and severity are determined by the kinetic energy released to the body at the moment of the impact. The higher the kinetic energy transferred to the tissues, the greater the temporary cavity size is and the most severe is the resulting injury. The wound's morphology and size (especially on the bone) may give information about the bullet caliber and shape but caution is recommended in any attempt to determine precise bullet caliber from the wound examination alone. Gunshot wounds can show different features based on the affected body area but their severity is still mainly due to the amount of energy transmitted to the body.
Comment Here
Reference: Gunshot wounds
The weight and the velocity of the bullet are the most critical variable in determining the amount of kinetic energy. Doubling the mass doubles the energy, while doubling the velocity quadruples it. However, the wound's ultimate extent and severity are determined by the kinetic energy released to the body at the moment of the impact. The higher the kinetic energy transferred to the tissues, the greater the temporary cavity size is and the most severe is the resulting injury. The wound's morphology and size (especially on the bone) may give information about the bullet caliber and shape but caution is recommended in any attempt to determine precise bullet caliber from the wound examination alone. Gunshot wounds can show different features based on the affected body area but their severity is still mainly due to the amount of energy transmitted to the body.
Comment Here
Reference: Gunshot wounds
Board review style question #2

The finding above is observed at the autopsy of a 34 year old Caucasian man. Which of the following is correct regarding this gunshot wound?
- Its morphological features are indicative of an exit gunshot wound
- It results from a bullet fired from a long distance at an acute angle of fire with respect to the skin
- There was an intermediate target between the muzzle of the firearm and the body
- This wound typically occurs in hard contact gunshots to the head
- Weapon was not in contact with the target but was held a very short distance from it
Board review style answer #2
D. This wound typically occurs in hard contact gunshots to the head
Hard contact gunshot wounds to specific body areas may result in a peculiar patterned injury, called muzzle imprint, surrounding the central defect. When the weapon is pressed firmly and fired against a body area covered only by a thin layer of skin and subcutaneous tissue overlying the bone (such as the head), the gases produced by the detonation enter the body together with the bullet. The gases accumulate between the skin and the bone, causing a sudden expansion of the subcutaneous tissues. The skin is forced to balloon outward and push against the weapon muzzle, producing a typical abrasion / bruise that resembles the muzzle's shape. When the expansion exceeds skin elasticity and resistance, it will tear, resulting in an entrance gunshot wound with a stellate or irregular appearance.
Comment Here
Reference: Gunshot wounds
Hard contact gunshot wounds to specific body areas may result in a peculiar patterned injury, called muzzle imprint, surrounding the central defect. When the weapon is pressed firmly and fired against a body area covered only by a thin layer of skin and subcutaneous tissue overlying the bone (such as the head), the gases produced by the detonation enter the body together with the bullet. The gases accumulate between the skin and the bone, causing a sudden expansion of the subcutaneous tissues. The skin is forced to balloon outward and push against the weapon muzzle, producing a typical abrasion / bruise that resembles the muzzle's shape. When the expansion exceeds skin elasticity and resistance, it will tear, resulting in an entrance gunshot wound with a stellate or irregular appearance.
Comment Here
Reference: Gunshot wounds
