

Autopsy & forensics
Types of injuries
Blunt force injuries
Authors: Lorenzo Gitto, M.D., Robert Stoppacher, M.D.
Deputy Editor-in-Chief: Patricia Tsang, M.D., M.B.A.


Last author update: 26 April 2021
Last staff update: 26 April 2021
Copyright: 2012-2025, PathologyOutlines.com, Inc.
PubMed search: Blunt force [TI] injuries forensic

Table of Contents
Definition / general | Essential features | Wound biomechanics | Abrasions | Contusions | Lacerations | Fractures | Special topics in blunt force injuries | Case reports | Clinical images | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Gitto L, Stoppacher R. Blunt force injuries. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/forensicsbluntforce.html. Accessed January 21st, 2025.
Definition / general
- Blunt object: an object that has a wide, dull or convex surface with rounded edges or corners; does not possess any pointed or sharp edges
- Blunt force injuries: produced by blunt objects due to different possible mechanisms
- Moving blunt object impacting against a resting body
- Moving body impacting against a resting blunt object
- Moving body and a moving blunt object collide
- Body is trapped between 2 surfaces
Essential features
- Many different objects can produce blunt force injuries
- Different objects may create similar injuries, so caution is needed when attributing a specific injury to a particular weapon or object
- Specific determination of the age of blunt force injuries is currently not reliable
- Distinguishing between antemortem and postmortem blunt force injuries is mandatory
- Resuscitation injuries can produce blunt force injuries and must be differentiated at the postmortem examination
Wound biomechanics
- Kinetic energy:
- Energy possessed by an object due to its motion
- Function of the object's mass (M) and its velocity (V)
- KE = 1/2 MV2
- Impact dynamics:
- Impact refers to the physical force that develops during blunt trauma
- Elastic impact: after the impact, an object bounces, preserving its kinetic energy
- Plastic impact: kinetic energy is entirely or partially transferred to the body, leading to wound development; the vast majority of blunt force injuries have a plastic impact dynamic
- Inertia:
- Property of a body to resist changes in velocity
- If velocity changes suddenly (e.g. acceleration / deceleration), there will be a more severe effect on the affected body
- Impacting surface features: blunt force injury's appearance depends on the composition, size and shape of the impacting object or surface (Postepy Dermatol Alergol 2013;30:302)
- Tissue properties:
- Elasticity and plasticity play an essential role in determining the wound features
- Allow for deformation in response to an applied force
- After deformation, elastic tissue can drive passive recoil and return to its initial state after the force's termination
- When the force exceeds the tissue resistance, then a wound occurs
- Size of the involved area:
- Large body areas will disperse more energy, lessening the injury to the tissue
- Focal or curved areas concentrate the energy from the impact on a limited area, resulting in more severe damage
- Chronology of the impact:
- Slow, gradual forces cause a progressive compression and the energy can be slowly absorbed, resulting in minor damage
- Rapid or sudden forces result in a rapid transfer of energy to the body, frequently exceeding tissue resistance and producing more severe injuries
- Energy transfer: injuries can develop in body areas far from the point of impact due to the transfer of energy within the body (e.g. ring fracture of the skull in a subject who falls from a height and hits the ground with the sacrum)
Abrasions
- Skin injury consisting of the traumatic removal or detachment of the epidermis due to friction (shearing) or pressure (crushing) mechanisms
- Tangential abrasions: a lateral rubbing mechanism that scrapes off the superficial layers of the skin; epidermal shreds (skin tags) can be present and may suggest the impact's direction, although this phenomenon does not always occur
- Linear abrasions: caused by a sliding movement of a narrow object on the skin, which results in superficial epidermis denudation; typical examples are fingernail abrasions that can be observed in manual or ligature strangulations (Am J Forensic Med Pathol 1981;2:45, J Clin Forensic Med 2003;10:255)
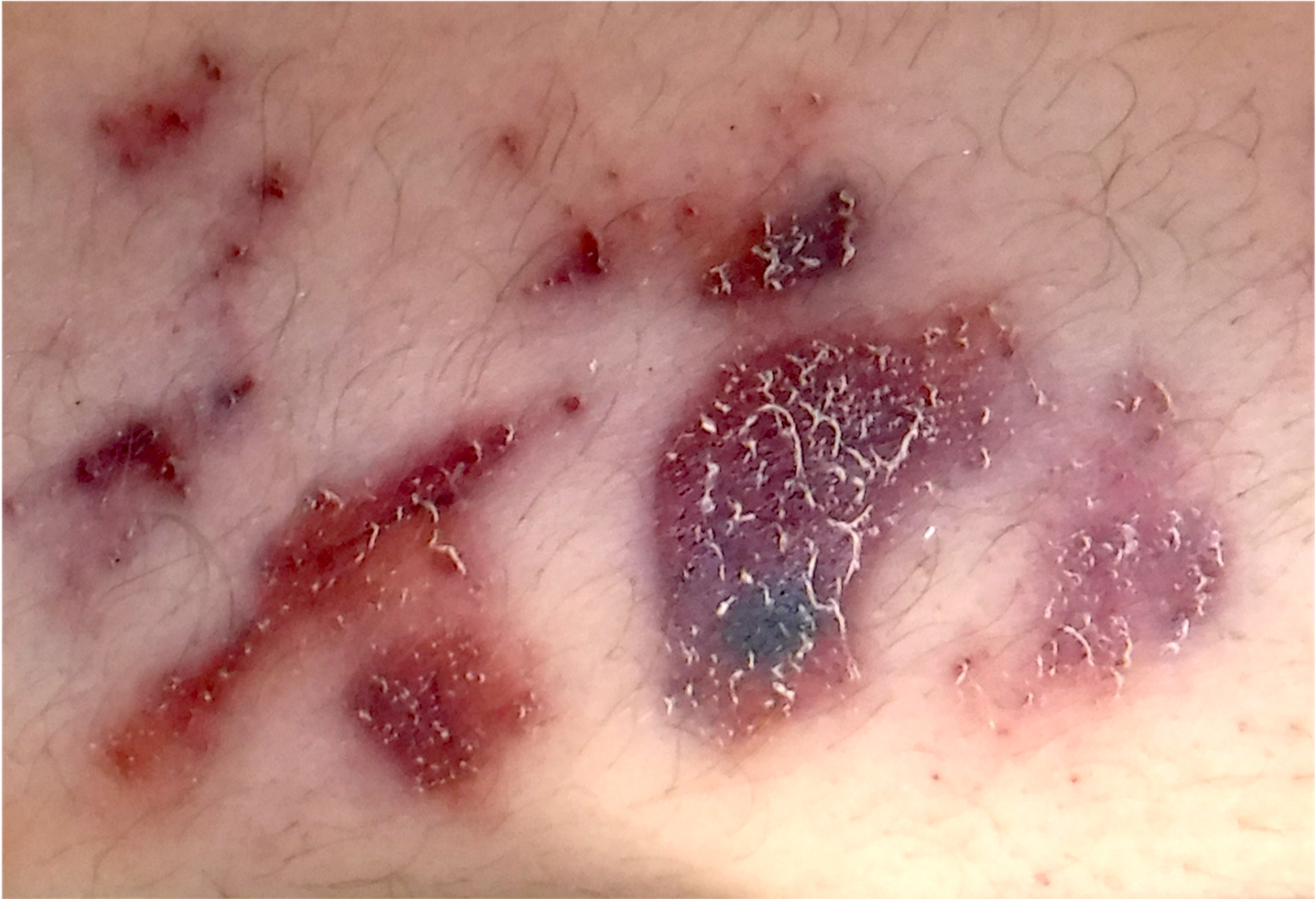
- Brush abrasions: caused by the body's frictional movements against a wide, rough surface or object, leading to scraping of the epidermis; usually wider at the starting point and narrower at the end (e.g. "road rash" in traffic accidents) (J Clin Forensic Med 2003;10:255)
- Compression abrasions: direct pressure from a blunt object together with slight rubbing movements produce skin and epidermal crushing
- Patterned abrasions: these injuries show a distinct pattern that may reflect the shape of the impacting blunt object; frequently observed in tortures (Forensic Sci Int 2018;284:85)
- Typically occur when the force is applied at or near perpendicular to the skin surface and can be classified as:
- Impact abrasions: occur when a force is applied suddenly or rapidly and perpendicular to the skin, pushing and crushing it on a body surface
- Pressure abrasions: occur when there is a slow, prolonged compression of the skin by a blunt object, which results in a dried, parchment-like abrasion (e.g. hanging mark)
- Typically occur when the force is applied at or near perpendicular to the skin surface and can be classified as:
- Nonpatterned abrasions: abrasions that don't resemble the producing object
- Patterned abrasions: these injuries show a distinct pattern that may reflect the shape of the impacting blunt object; frequently observed in tortures (Forensic Sci Int 2018;284:85)
- Differential diagnosis in abrasions:
- Antemortem abrasions (with survival interval):
- Usually dark red or red, covered with a dark scab and showing signs of healing
- Inflammatory cell infiltration, evidence of hemorrhage or granulation tissue are histologic signs of vitality (Clin Dermatol 2007;25:39)
- Postmortem abrasions:
- Several mechanisms can produce abrasions in the postmortem period (autopsy procedures, insect activity, body dragging on a rough surface, etc.)
- Usually orange-yellow or brown with a parchment appearance (J Forensic Leg Med 2014;26:10, Am J Forensic Med Pathol 2009;30:84)
- Antemortem abrasions (with survival interval):
- Dating of abrasion: despite recent research describing possible morphological features to establish an abrasion's age, it is extremely difficult to reach reliable conclusions based on the morphology of the injury (Am J Forensic Med Pathol 2017;38:167)
Contusions
- A contusion results from crushing or tearing of the dermis and subcutaneous tissues without breaking of the skin; the applied force causes blood vessel rupture, leading to variable bleeding in the subcutaneous space
- Locations: contusions can develop on the body surface as well as on internal organs
- Terms:
- Contusion: lesion that can happen anywhere in the body
- Bruise: lesion visible on the skin surface
- Ecchymosis: lesion resulting from nontraumatic bleeding, such as medical therapy (e.g. intravenous injection) or senile ecchymoses
- Petechia: small, pinpoint hemorrhage due to acute rise in venous pressure (congestion) leading to capillary rupture (e.g. from asphyxia)
- Hematoma: large collection of extravasated blood (e.g. from traffic accident)
- Patterned contusions:
- Linear contusions: when a rectangular shaped object strikes the body
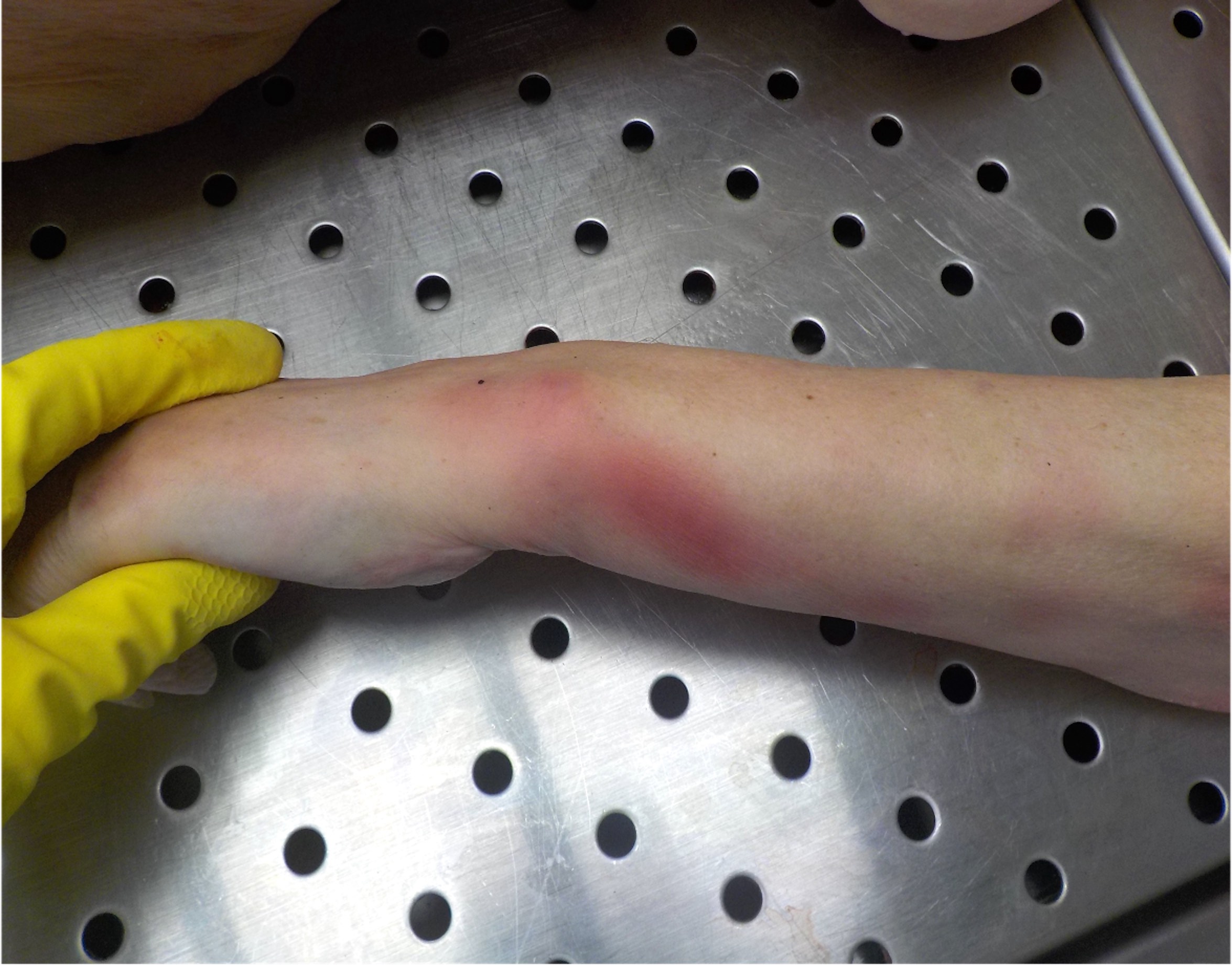
- Tram-like or railway line contusions: when a cylindrical or rod-like object hits the body, the blood accumulates laterally to the point of impact, creating an injury that appears pale in the center, lined by 2 linear, parallel bruises on each side (Forensic Sci Med Pathol 2017;13:508)
- Loop contusions: when a cable or cord-like item strikes the body, frequently seen in child abuse (Paediatr Child Health 2013;18:433)
- Fingertip contusions: a cluster of small round bruises, approximately 1 cm in diameter, develops when the offender grips a victim's body area vigorously
- Most frequently involved body area is the neck
- Sometimes, a single, larger, oval or round bruise on the opposite side of the clustered fingertip contusions may also be present (thumb-like bruise) (Pediatr Emerg Care 2019 Jan 7 [Epub ahead of print])
- Intradermal contusions: when an object with grooves or ridges hits the skin, producing an injury limited to the subepidermal layer (e.g. tire marks, shoe marks) (J Forensic Sci 2007;52:1050, Forensic Sci Int 2020;2:521)
- Suction contusions: confluence of multiple petechiae in a circumscribed area due to a vacuum-like mechanism, which leads to capillary rupture and blood leakage in a circumscribed body area (Oral Implantol (Rome) 2016;8:68)
- Coup / contrecoup contusions: contusions that develop at the point of impact (coup) and on the side opposite the impacted area (contrecoup); typically observed on the brain (Neurocrit Care 2004;1:385)
- Human bites: typical bruise resulting from human bites shows 2 opposing arches separated by a central pale, uninvolved area with possible associated abrasions and lacerations (J Forensic Odontostomatol 2014;32:1)
- Dating of bruises:
- Red blood cells and hemoglobin degradation lead to pigment formation and chromatic changes of the bruise, generally from red / purple to green to yellow-brown
- Chromatic changes have been studied to estimate the age of the bruise
- Consistent gross or histological dating of contusion is not reliable
- With the current knowledge, it is reasonable to state that a yellow colored bruise may have been produced > 18 hours before the examination
- Absence of yellow color does not mean < 18 hours
- Recommended to describe them just as recent or old (Forensic Sci Med Pathol 2007;3:241)
- Differential diagnosis in contusions:
- Antemortem contusions: contusions are a vital phenomenon; can affect any body area, are usually unilateral and asymmetrical, are commonly associated with tissue swelling, show different colors in the same subject, do not become pale on digital pressure and show a cellular reaction microscopically
- Livor mortis: lividity is usually bilateral and symmetrical, uniform in color, shows pallor on digital pressure (if recent), is preferentially located in the dependent portions of the body with no cellular reaction at the microscopic examination (Am J Forensic Med Pathol 1998;19:46)
- Tardieu spots: small postmortem hemorrhages that develop in areas of intense lividity (also called hypostatic hemorrhages) (Am J Forensic Med Pathol 2009;30:322)
Lacerations
- Laceration occurs when a blunt force causes skin compression, crushing and splitting; lacerations frequently occur on the skin overlying bony prominences but can also affect the internal organs, leaving the skin intact
- Hallmark: presence of tissue bridges in the depth of the wound is the pathognomonic feature for lacerations; also helps to distinguish them from an incised wound (sharp force injury)
- Edges: laceration edges are usually jagged; abrasions, bruising and crushing of the margin are frequently observed
- Types of lacerations:
- Tear lacerations: classic form of laceration occurring when a blunt force impact rips and tears the skin and the subcutaneous tissues
- Split lacerations: compression of the skin between blunt object and bone
- Stretch lacerations: blunt trauma that causes an overstretching of the skin until it ruptures
- Crush lacerations: blunt trauma that causes grinding and compression of the skin and soft tissue, resulting in possible amputation
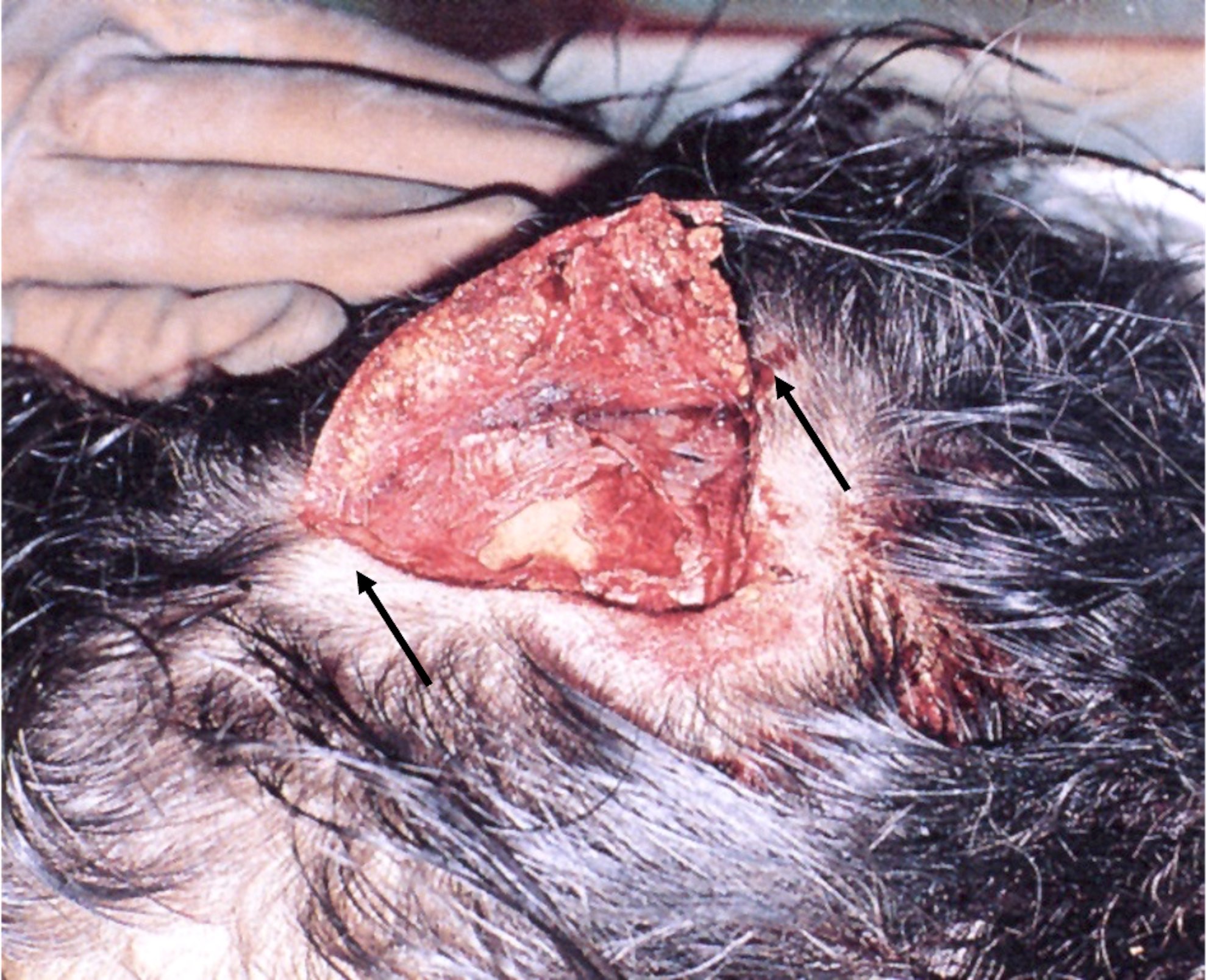
- Degloving injury: blunt mechanism that occurs when the skin and subcutaneous tissues are trapped between 2 hard surfaces and are suddenly pulled at the moment of the impact, resulting in minimal to extensive loss of skin and soft tissues (Rom J Leg Med 2013;21:165)
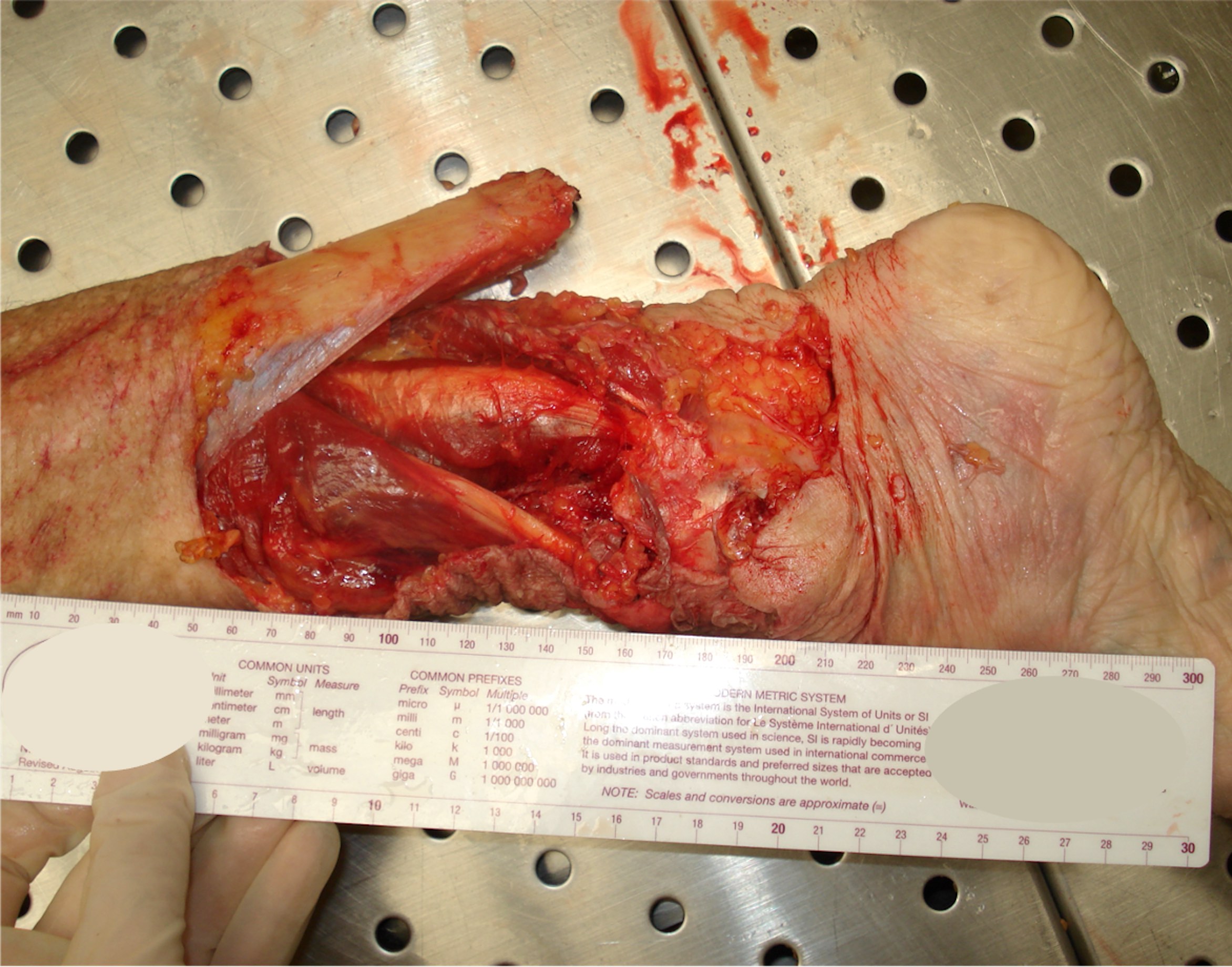
- Avulsions: violent blunt trauma that tears away the tissues from their attachments
- Direction of the impact: sometimes the presence of an abrasion surrounding a laceration may suggest the direction of the impact; abrasion is usually wider at the point of impact
- Undermining: impact is over the bone, resulting in a clean separation of the skin from the underlying bone in the direction of the application of force
- Dating of lacerations: estimation of the age of a laceration is not reliable
- Differential diagnosis:
- Incised wounds: sharp object (such as a knife) produces incised wounds (or cuts) that are typically longer than deeper due to the blade's sharpness and the sharp force related mechanism of injury; incised wounds lack tissue bridges; edges are usually sharply demarcated
Fractures
- Bone lesions that occur when the intensity of the blunt force exceeds the bone resistance
- Types of fractures (Acad Forensic Pathol 2016;6:463):
- Traumatic: typical fractures due to a blunt force trauma
- Pathologic: fractures due to a pathologic condition (e.g. osteoporosis, bone metastasis, etc.)
- Direct: fractures that occur at the point of impact
- Indirect: fractures that occur away from the point of impact due to energy transfer
- Open (compound): direct communication between the fracture and the external environment
- Closed: the fracture lies underneath intact skin
- Complete: the bone is separated into 2 or multiple parts
- Incomplete: the bone cracks but does not separate
- Biomechanisms of fracture:
- Long bones:
- Compression: leads to an internal shortening of the bone
- Traction: when a tension force pulls the bone apart
- Shear: when a force acts parallel to the bone, resulting in a fracture parallel to the force's direction
- Torsion (spiral): when the bone is twisted; typically observed in child abuse (tibial fractures)
- Bending: when the bone is compressed on one side on its axis, creating tension on the opposite side
- Skull: following a blunt force injury to the head, the area of impact temporarily bends inward while there is a compensatory distortion of surrounding areas; when the intensity of the impact exceeds the skull resistance, fractures develop
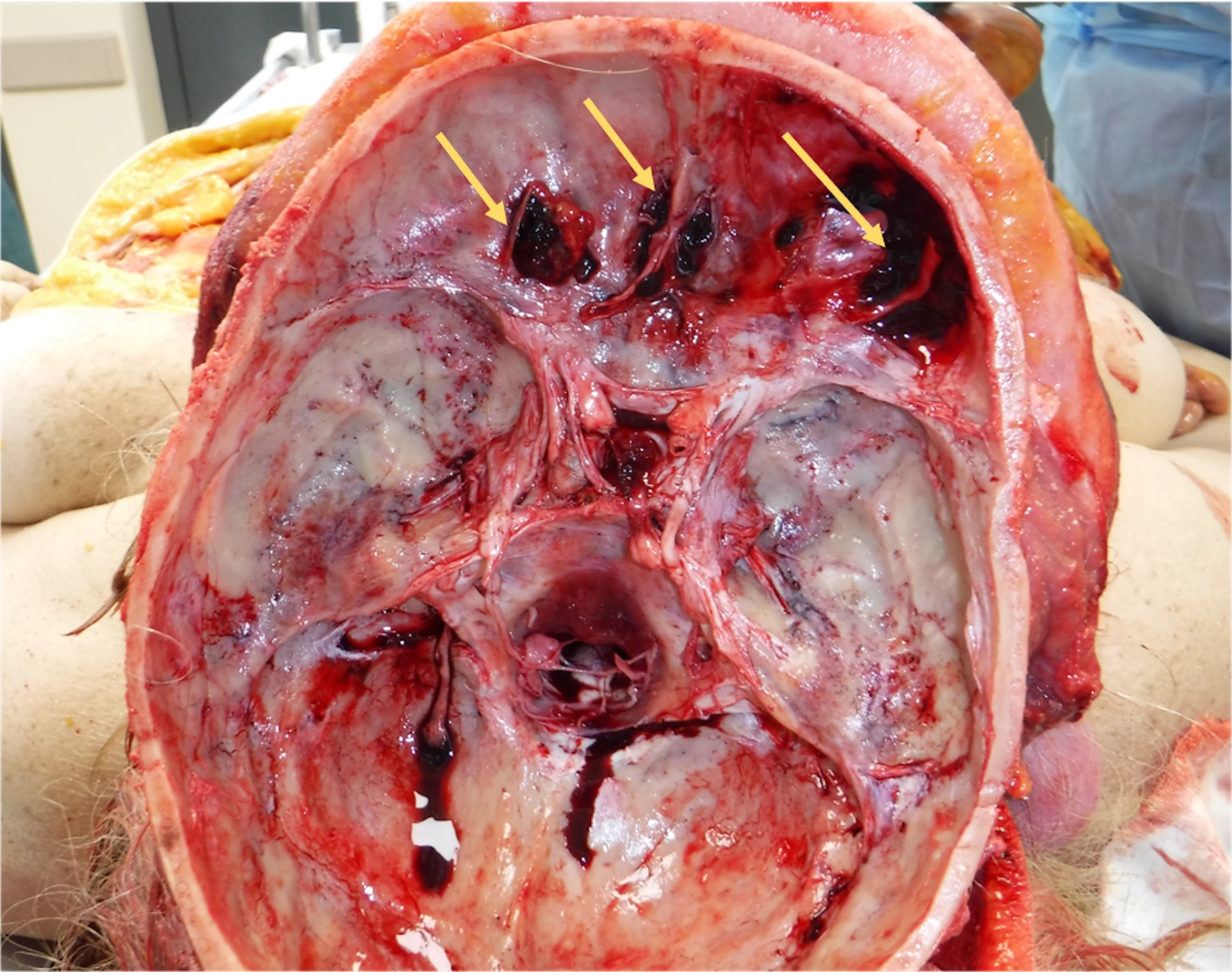
- Linear: usually resulting from the impact of the head against a large surface; can develop on the cranial vault or on the bases and can be single or multiple, sometimes intersecting
- Depressed: break of the bone, which is pushed inward at the point of impact, producing a permanent focal depression of the skull; usually results from a blunt object with a limited surface striking the head (e.g. hammer) (Med Sci Law 2015;55:44)
- Ring: fracture encircling the foramen magnum resulting from the transmission of energy over the bone from the impact point to a distant site
- Diastatic: fracture involves and separates the cranial sutures (common in children)
- Combined: combination of the mechanisms described above
- Long bones:
Special topics in blunt force injuries
- Basilar skull fractures: delayed bruises may follow cranial base fractures but they should not be considered definitive evidence of a specific cranial base fracture
- Anterior cranial fossa fracture: conjunctival, palpebral or periorbital bruises (raccoon eyes) with or without liquorrhea or bleeding from the nose (J Neurosci Rural Pract 2018;9:370)
- Middle cranial fossa fracture: bruising visible behind and below the ear at the mastoid process (Battle sign) or bleeding from the ear (StatPearls: Battle Sign [Accessed 8 February 2021])
- Posterior cranial fossa fracture: Battle sign or pharyngeal bruises / hematomas
- Commotio cordis: cardiac concussion in which a blunt impact to the precordium leads to a cardiac rhythm disorder in the absence of structural heart damage (Leg Med (Tokyo) 2019;38:73, Med Sci Law 2017;57:146)
- Acceleration / deceleration injuries:
- Typically observed in motor vehicle collisions
- Rapid deceleration results in differential movements among adjacent structures, resulting in the tearing of visceral organs, ligaments and vascular pedicles
- Internal organs are also crushed between the anterior abdominal wall and the spine or posterior chest, leading to severe parenchymal lacerations
- Blast injuries (Philos Trans R Soc Lond B Biol Sci 2011;366:144):
- Typically observed in explosions
- Following the detonation, a shock wave (blast or pressure wave) propagates radially from the original point, acting as a blunt force when interacting with the body
- Lungs, middle ear (barotrauma), gastrointestinal tract and bones are the most affected body areas
- Chop lacerations:
- Injuries that show both blunt and sharp force trauma features
- Produced by a heavy blunt object with a sharp edge (e.g. cleaver)
- Typically show abraded and bruised edges with a clean separation of the margins and no tissue bridges
- Resuscitation injuries: cardiopulmonary resuscitation (CPR) or other procedures may result in physical injuries that can be hard to interpret during autopsy (J Forensic Leg Med 2015;33:39)
- Commonly observed injuries are:
- Bruises and abrasions on the scalp and face (e.g. use of a mask for resuscitation, intubation attempts, pinching of the nose during mouth to mouth resuscitations, etc.)
- Bruise and abrasions on the precordial region or the central chest area due to external compressions during cardiopulmonary resuscitation
- Rib and sternum fractures and soft tissue hemorrhages are commonly associated
- Laceration of the heart, lungs, pleura and pericardial sac may result from rib fractures
- Electrical burns from defibrillation, in the form of a rectangular, parchment-like, yellow-orange abrasion on the anterior chest
- Retinal hemorrhages have been rarely described in children following cardiopulmonary resuscitation (J Forensic Sci 2017;62:107)
- Commonly observed injuries are:
Case reports
- 4 month old boy with a patterned abrasion of uncertain etiology (Forensic Sci Med Pathol 2009;5:324)
- 49 year old woman with diaphragm laceration due to cardiopulmonary resuscitation (J Forensic Sci 2016;61:1135)
- 90 year old man with an atypical patterned bruise on the forearm (Forensic Sci Med Pathol 2014;10:637)
- 92 year old man with a simple depressed skull fracture (Med Sci Law 2015;55:44)
- Severe degloving injury of the foot (Rom J Leg Med 2013;21:165)
- 3 cases of commotio cordis (Int J Legal Med 2005;119:88)
Clinical images
Contributed by Lorenzo Gitto, M.D., Robert Stoppacher, M.D., Serenella Serinelli M.D., Ponni Arunkumar, M.D. and Luigi Bonaccorso, M.D.

Abrasion
Bruise

Laceration
Fracture
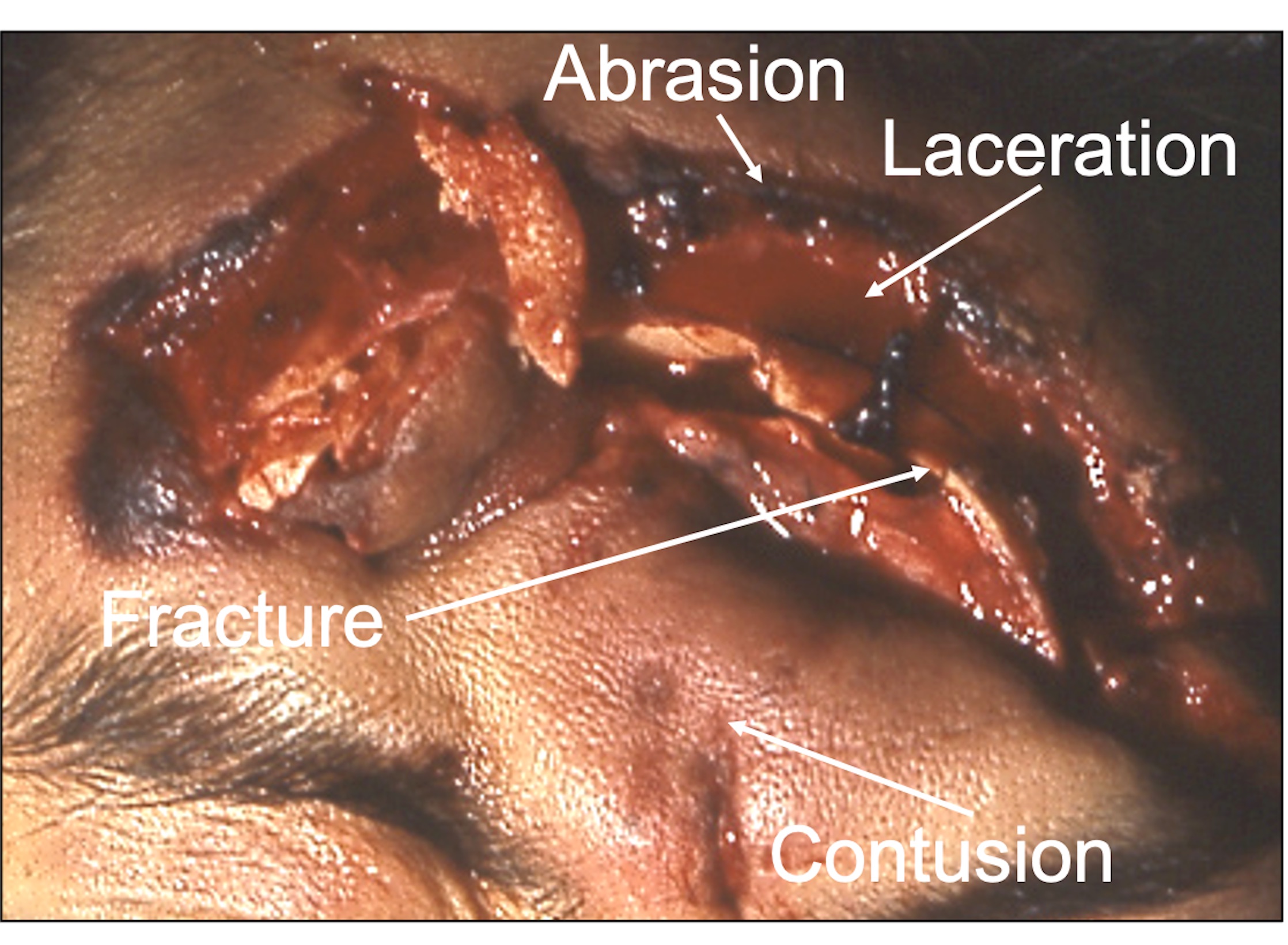
Mixed wound
Superficial abrasion with skin tags

Road rash

Patterned abrasions

Fingernail abrasions

Pressure abrasion
Postmortem abrasions

Ecchymosis

Hematoma

Visceral contusion

Tram-like bruise

Loop-like bruise

Patterned abraded contusion

Fingertip contusion
Subcutaneous hemorrhage
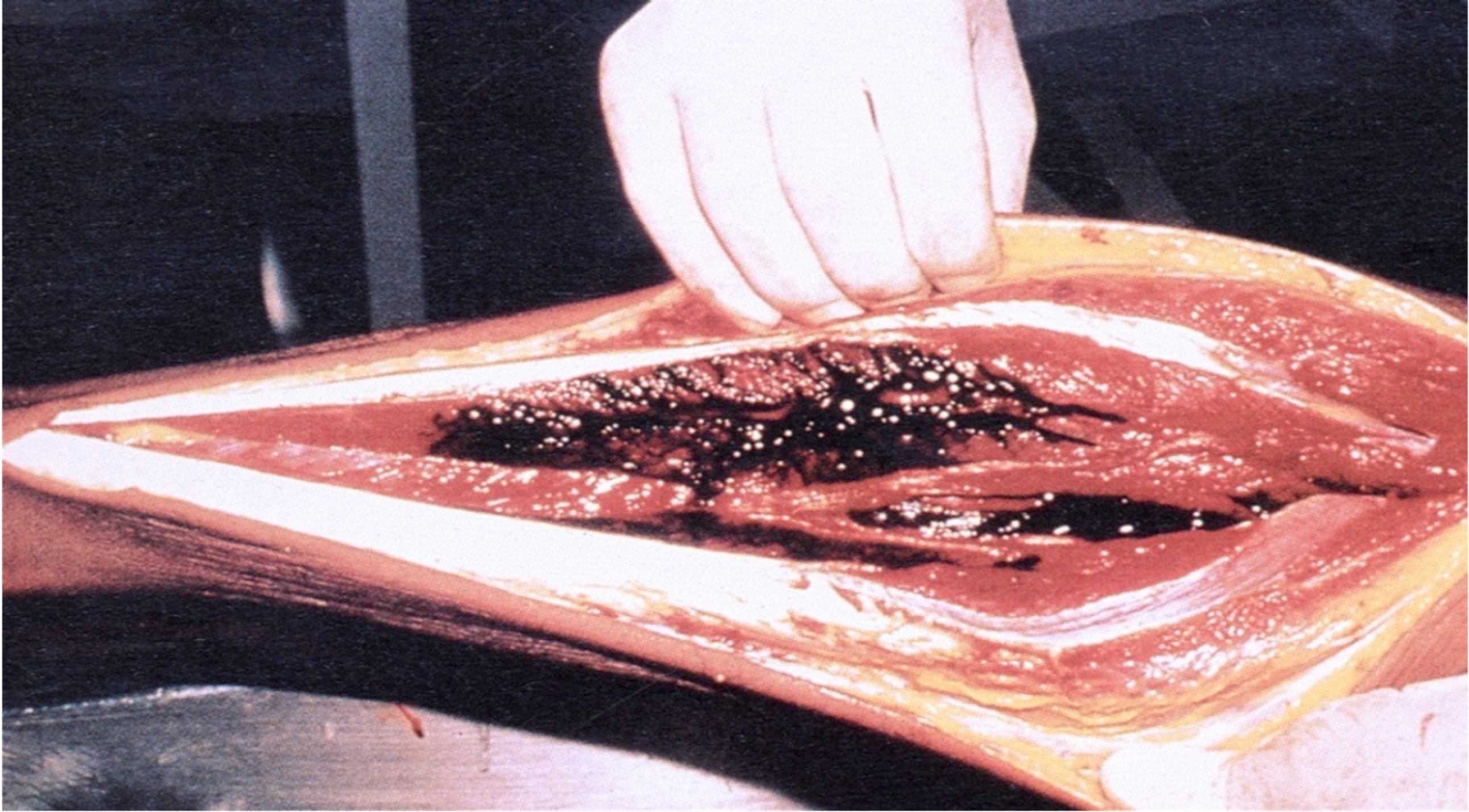
Deep soft tissue hemorrhage

Tardieu spots

Laceration

Hammer lacerations

Aortic lacerations due to motor vehicle collision
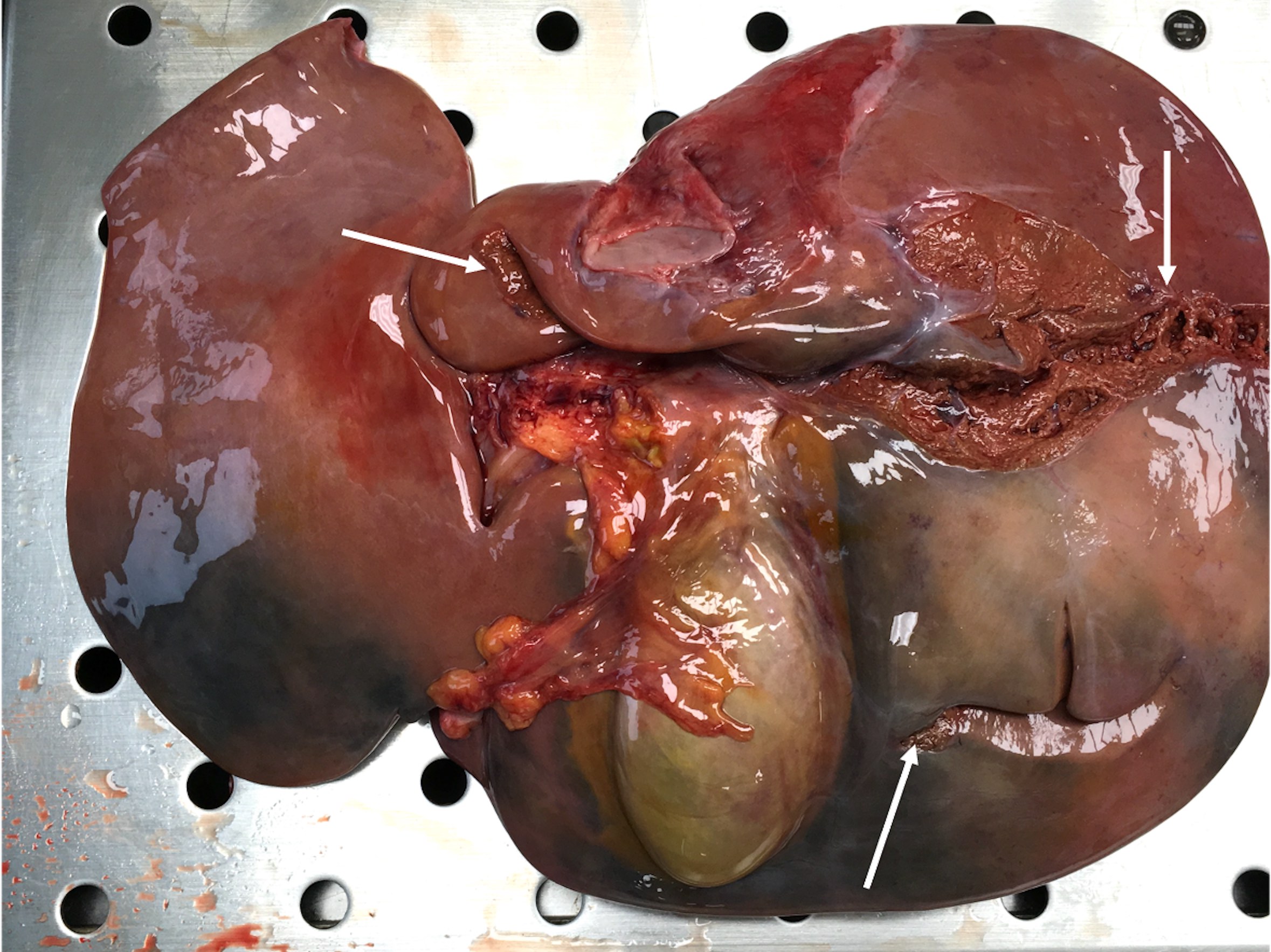
Liver laceration
Avulsion laceration

Closed fracture

Open fractures

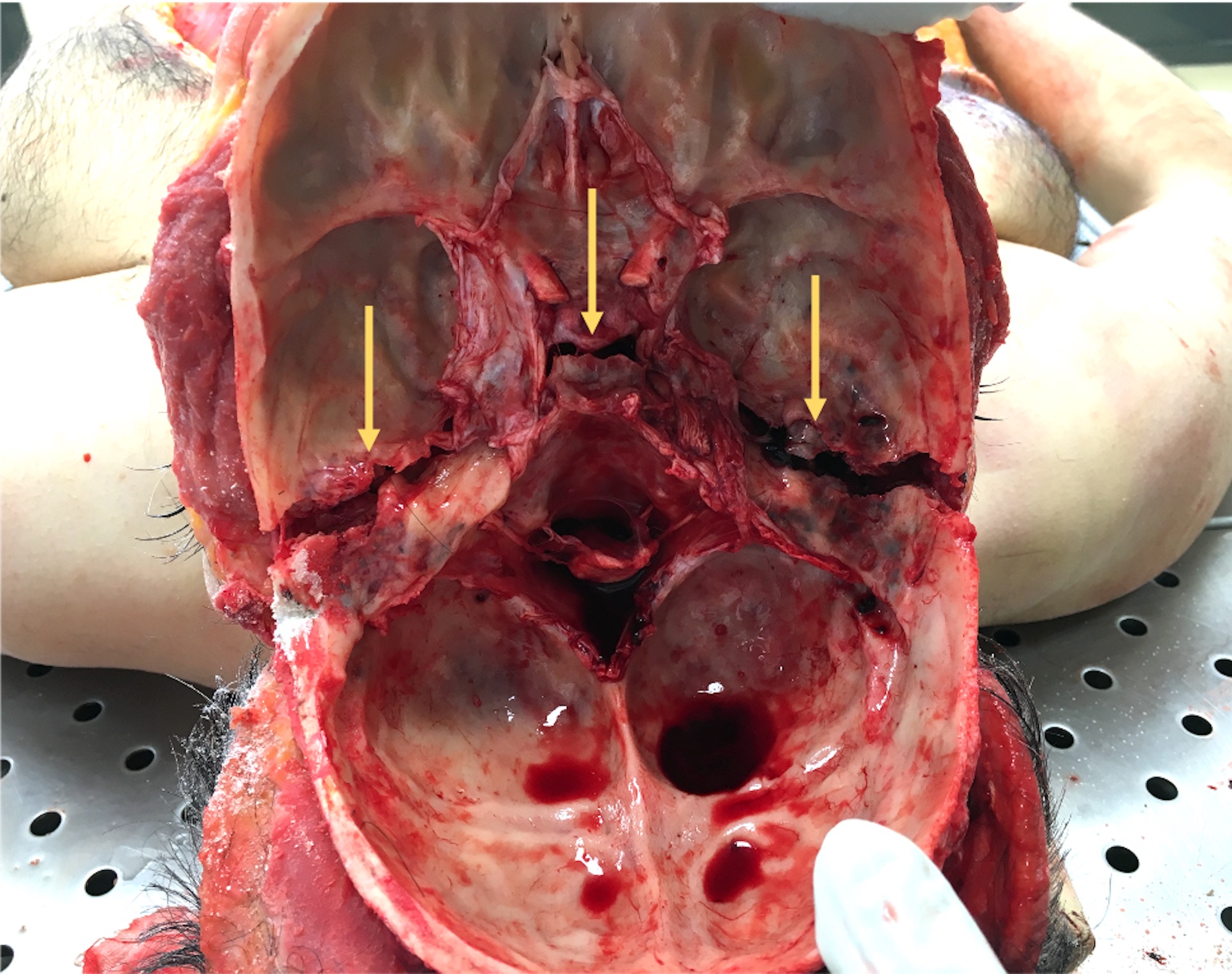
Multiple facial bone fractures
Linear fracture of the cranial vault

Raccoon eyes
Anterior cranial base fractures

Ear bleeding
Middle cranial base fractures
Depressed skull fracture

Ring fracture

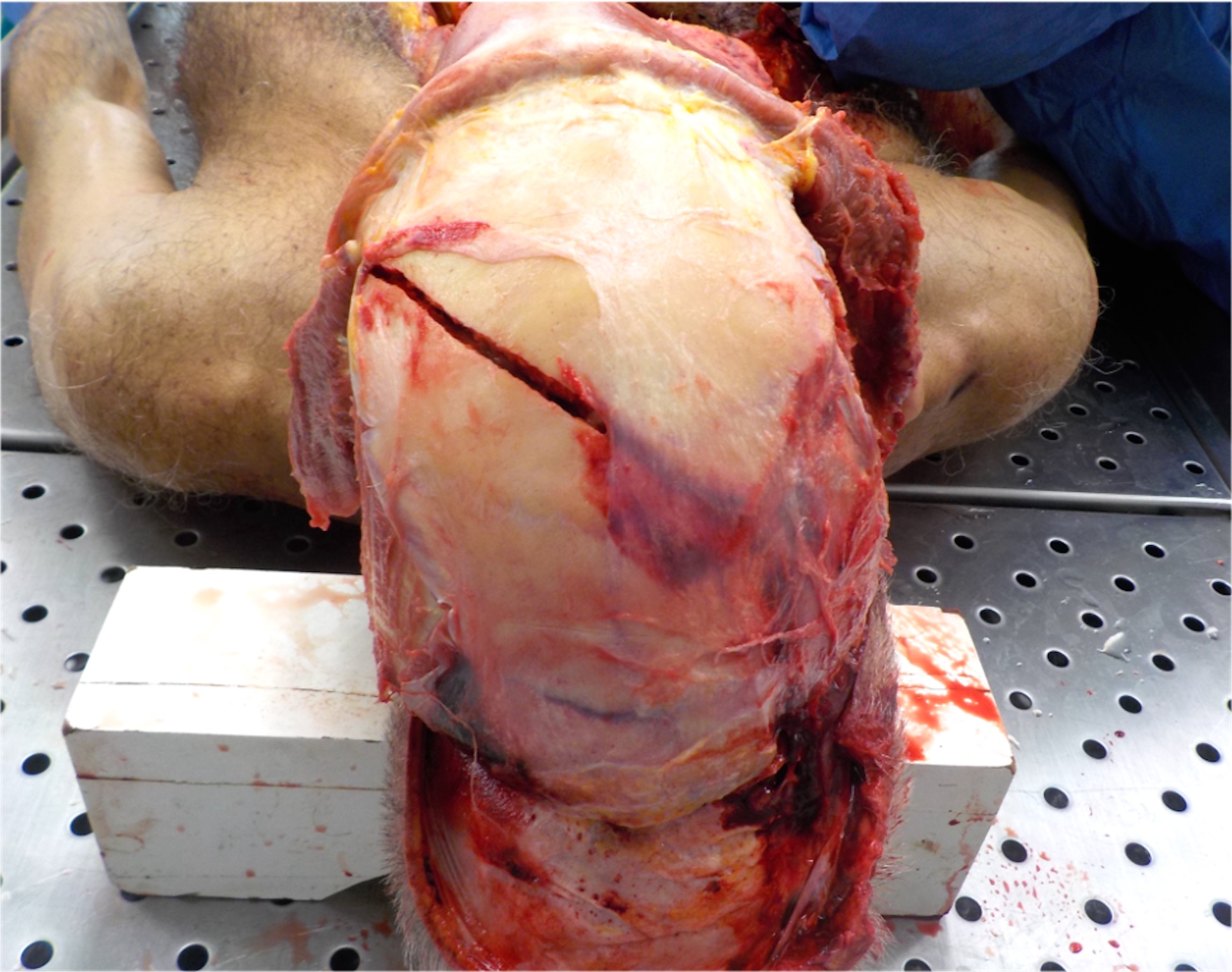
Victim of a motor vehicle collision

Chop lacerations
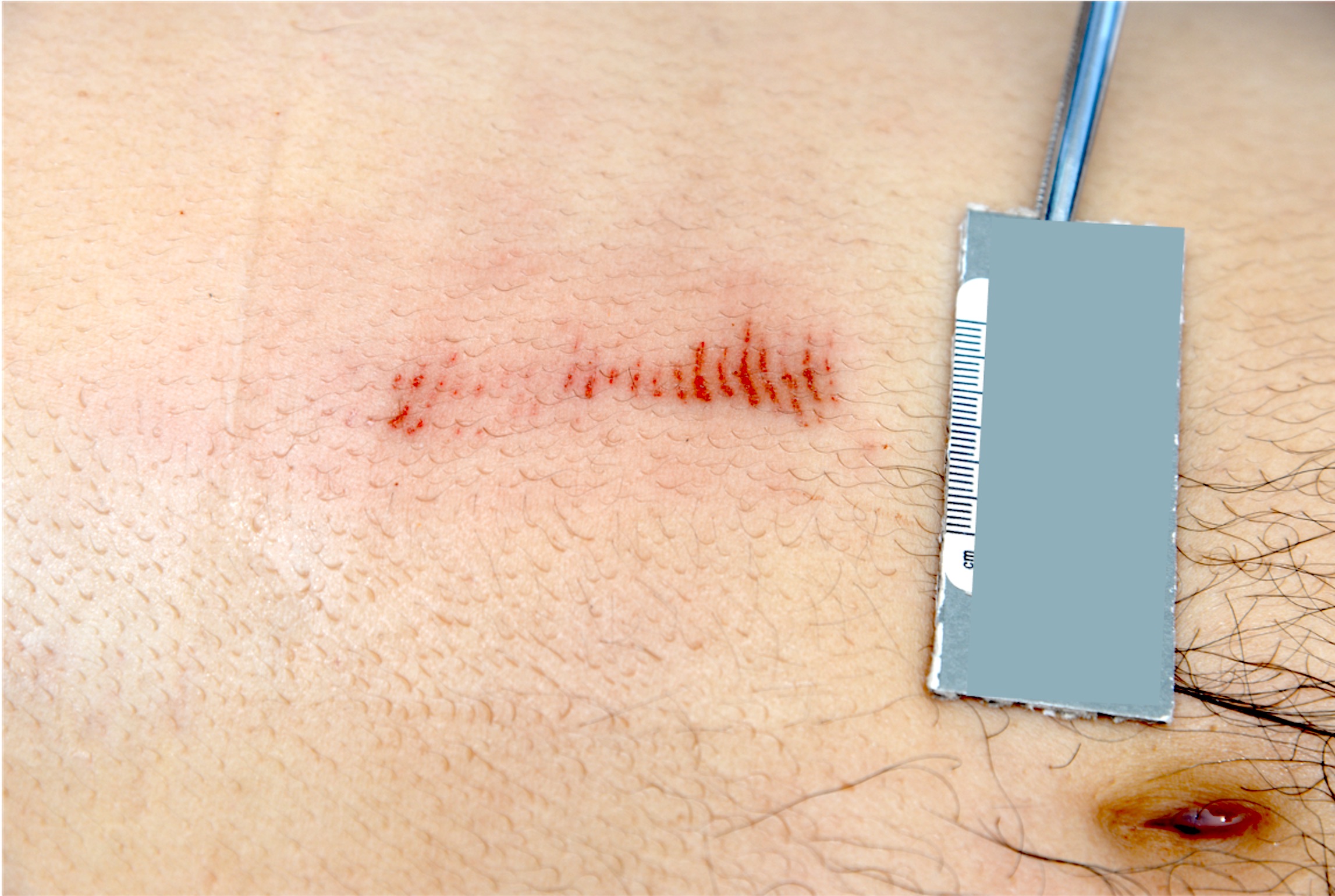
Board review style question #1

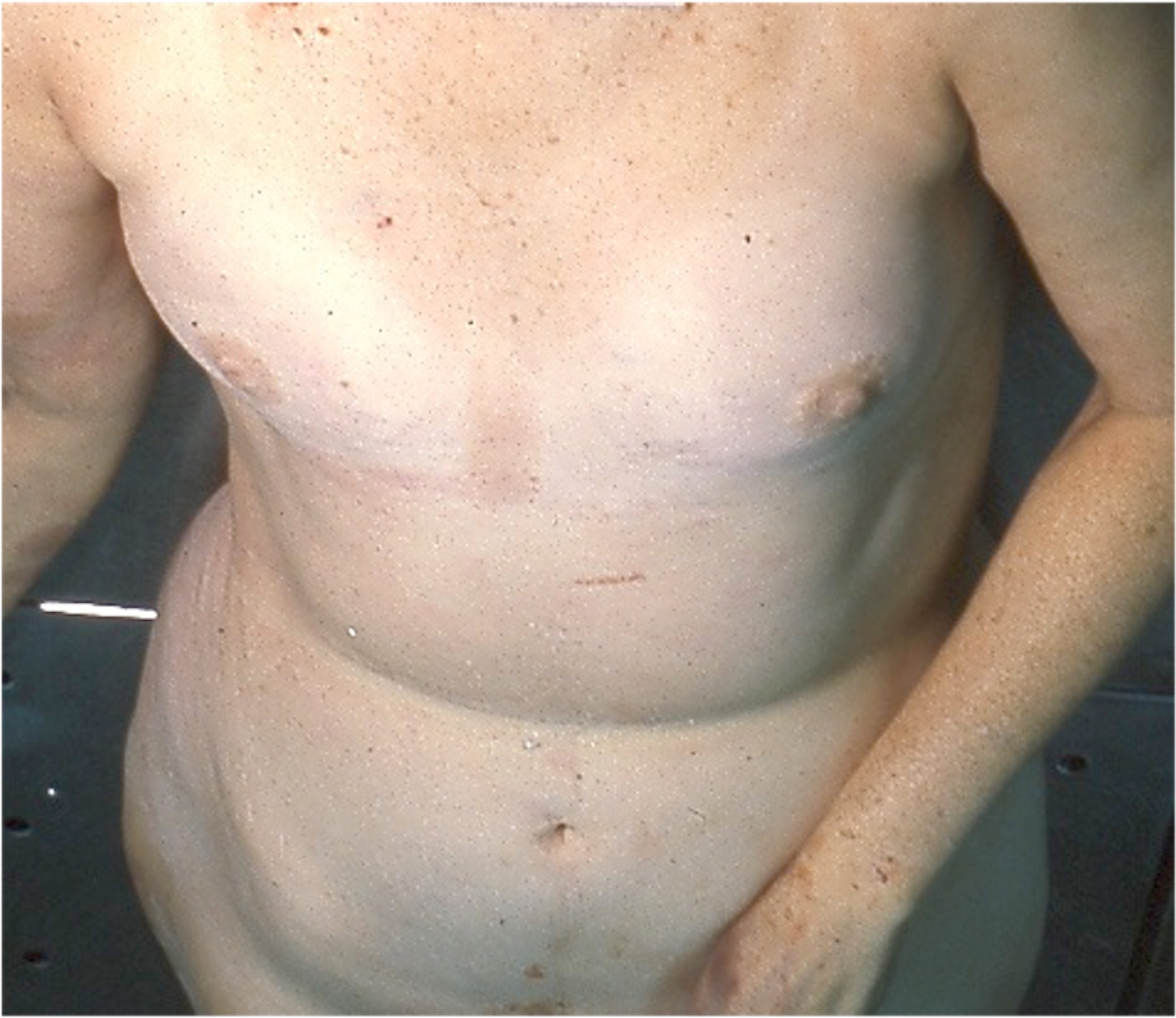
How are the lesions shown in the image best characterized?
- Contact dermatitis
- Electrocution
- Postmortem insect activity
- Road rash
- Third degree thermal burn
Board review style answer #1
D. Road rash. This is an antemortem abrasion typically observed in traffic accidents when the body slides against the rough asphalt, producing injuries with a burnt appearance (also called brush burns). Postmortem abrasion shows a leathery, yellow-brown parchment appearance. Postmortem insect activity (typically ants) usually produces abrasion along the edge of clothing or floor irregularities if the body is in contact with the floor (e.g. edges of cobblestones). Third degree burns are full thickness burns that go through the dermis and affect deeper tissues. Electrical burn typically consists of a depressed leathery area of tissue necrosis, occasionally with blistering. Contact dermatitis is a red, itchy rash caused by direct contact with a specific item or substance and typically resembles the allergen's shape.
Comment Here
Reference: Blunt force injuries
Comment Here
Reference: Blunt force injuries
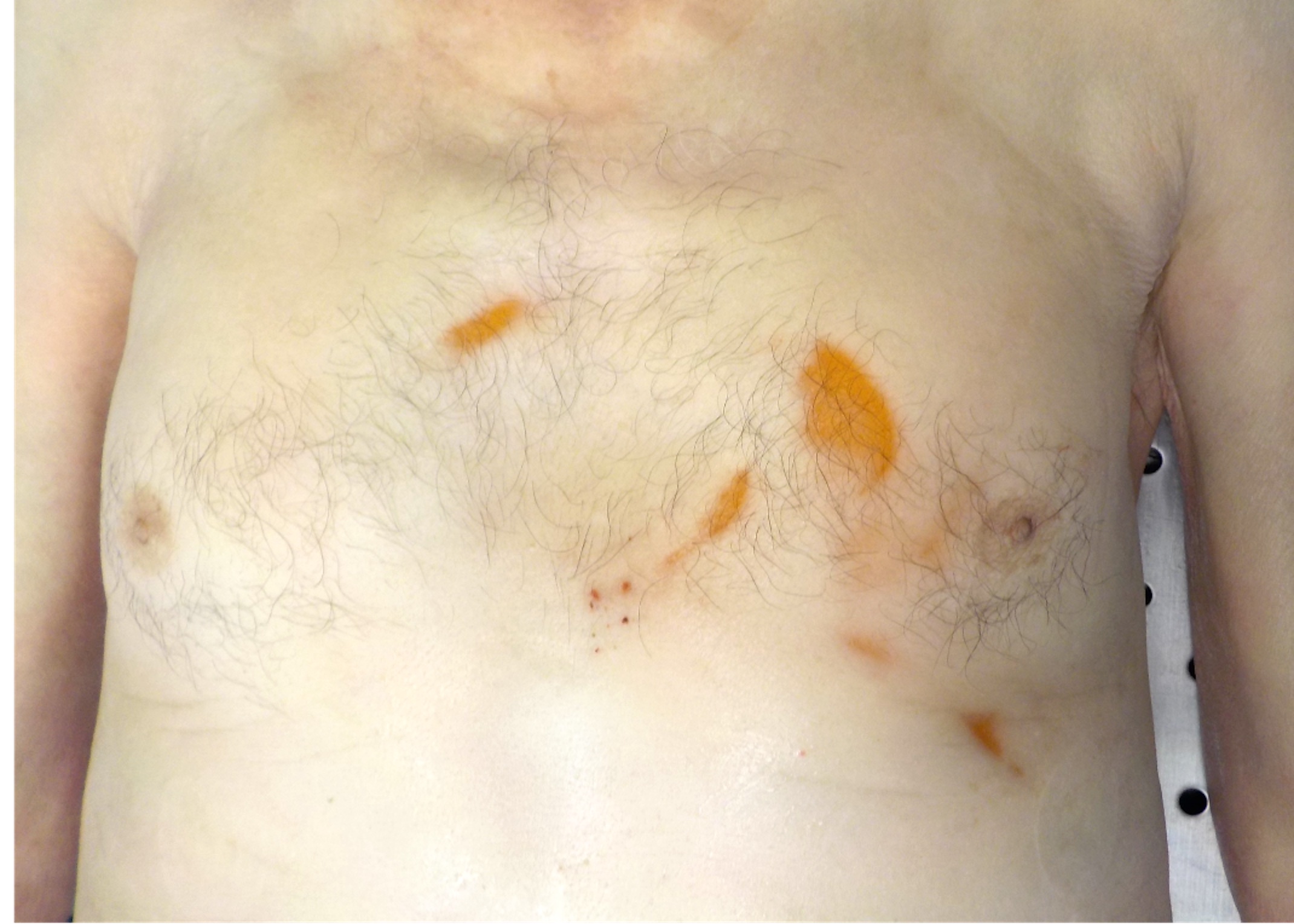
Board review style question #2
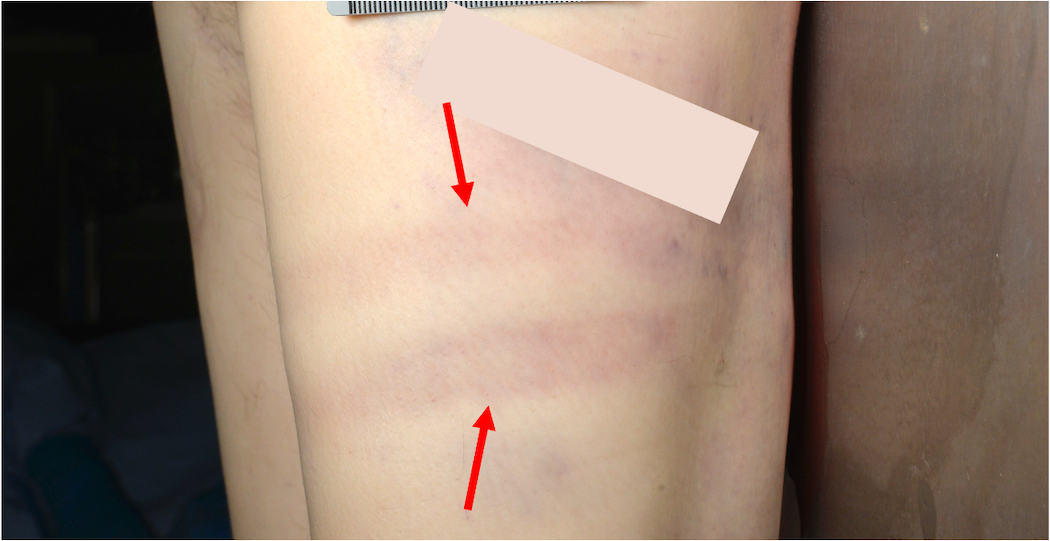
What weapon / mechanism most likely caused the injury depicted by the 2 red arrows?
- Hammer: striking the skin at a shallow angle
- Metal pipe tube: 2 bruises due to 2 distinct hits
- Metal pipe tube: single injury due to one hit in the center
- Postmortem artifact: lividity
- Shoe: kicking
Board review style answer #2
C. Metal pipe tube: single injury due to one hit in the center. This is a typical tram track bruise due to cylindrical or rod-like objects (e.g. metal pipe). When the weapon strikes the body, the skin is compressed and there is no damage to the underlying vessels but the blood accumulates laterally to the point of impact due to the rupture of blood vessels on either side of the impacting object. The resulting bruise appears as a pale, undamaged central area lined on either side by 2 parallel lines of bruising. Kicking usually results in patterned abrasions / bruises resembling the morphology of the shoe sole. Lividity is usually bilateral and symmetrical, uniform in color, shows pallor on digital pressure and is preferentially located in the body's dependent portions. Hammer injuries are usually focal and resemble the shape of the hammer’s head.
Comment Here
Reference: Blunt force injuries
Comment Here
Reference: Blunt force injuries
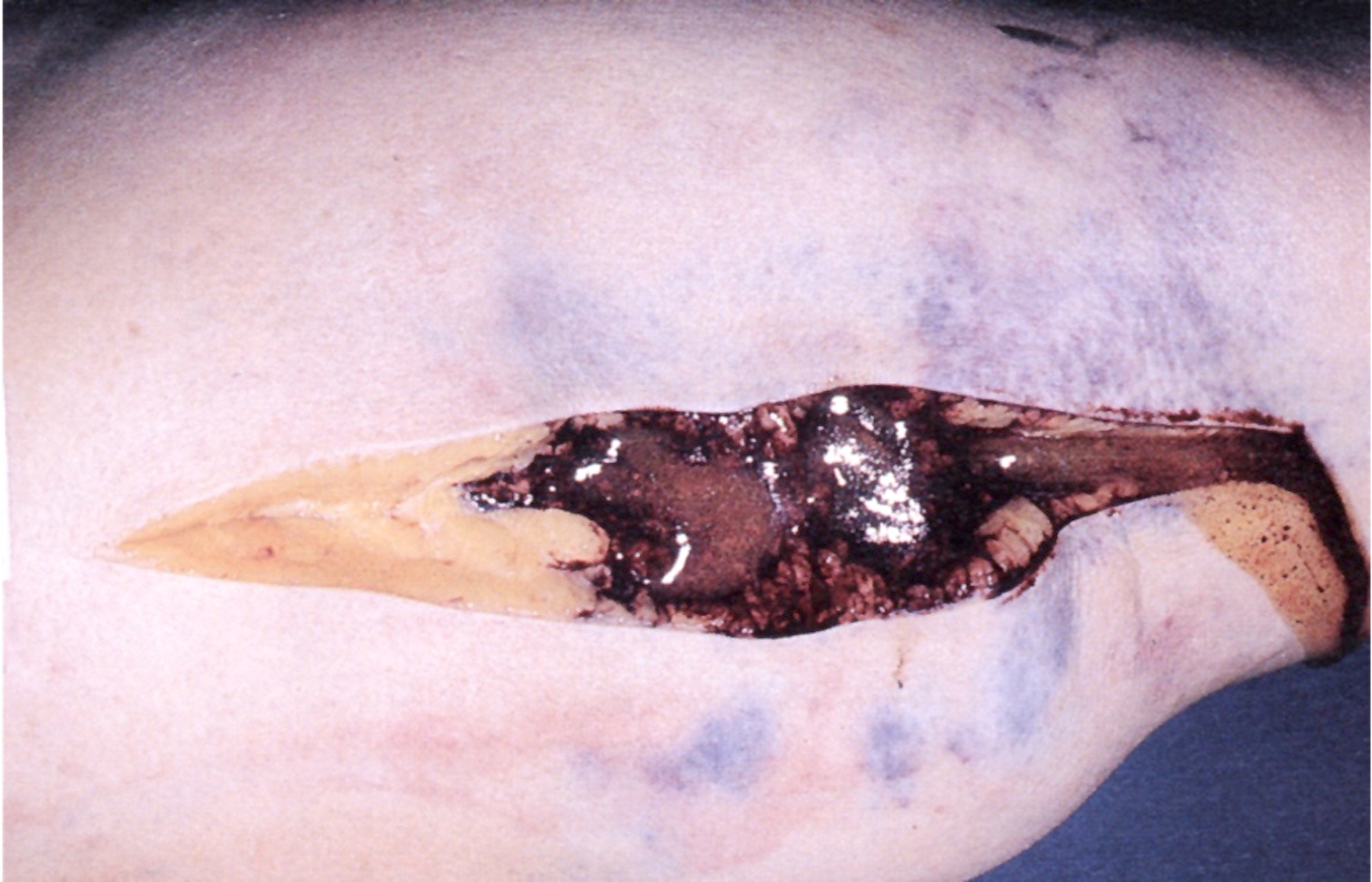
Board review style question #3

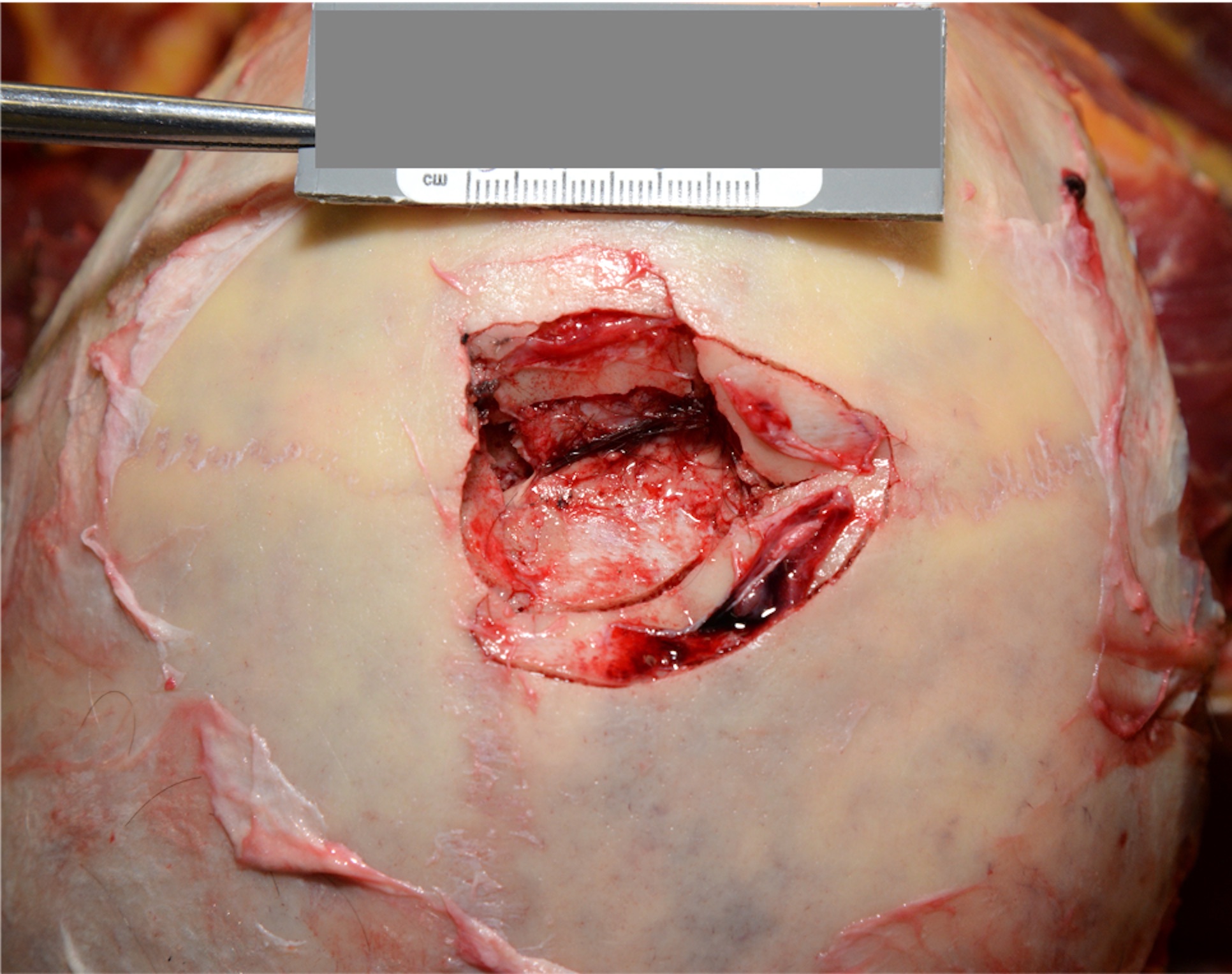
What is the best description for the injury depicted in the yellow circle in this victim of a traffic accident?
- Avulsion laceration
- Chopping injury
- Necrotizing fasciitis
- Stab wound injury
- Tissue procurement artifact
Board review style answer #3
A. Avulsion laceration. The finding is consistent with a typical avulsion laceration, a severe form of laceration in which the soft tissues, musculature or bone are torn away from the normal points of attachment. The tissues are often completely detached and these injuries may bleed profusely. A stab wound is a penetrating injury to the skin that results from a sharp or similar pointed object. Chopping wounds are injuries produced by heavy blunt objects that also possess a sharp edge that shows both sharp force (cuts) and blunt force (abrasion and contusion). Necrotizing fasciitis is a rare bacterial infection that spreads quickly in the body and results in diffuse necrosis of fascia, skin and subcutaneous tissue.
Comment Here
Reference: Blunt force injuries
Comment Here
Reference: Blunt force injuries

