
Esophagus
Carcinoma
Esophageal carcinoma-overview
Author: Elliot Weisenberg, M.D.

Last author update: 1 June 2013
Last staff update: 13 December 2023
Copyright: 2003-2019, PathologyOutlines.com, Inc.
PubMed Search: Carcinoma esophagus[TIAB]
Table of Contents
Definition / general | Risk factors | Sites | Pathophysiology | Clinical features | Diagnosis | Radiology description | Overall 5 year survival | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Differential diagnosisCite this page: Weisenberg E. Esophageal carcinoma-overview. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/esophaguscarcinomageneral.html. Accessed April 23rd, 2024.
Definition / general
- < 1% of all cancers in US, ~6% of gastrointestinal cancers
- Disproportionate numbers of deaths as most patients are asymptomatic during early stages and present with advanced or metastatic disease (Wikipedia: Esophageal Cancer [Accessed 25 February 2019], eMedicine: Esophageal Cancer [Accessed 25 February 2019])
- Worldwide, 90% are squamous cell carcinoma
- In US and Western Europe, has been a shift from squamous cell carcinoma to adenocarcinoma
- Incidence of adenocarcinoma has been increasing, especially in white men and is now higher than squamous cell carcinoma in US (NIH: Esophageal Cancer [Accessed 25 February 2019]), France (Gastroenterol Clin Biol 2005;29:1258) and elsewhere
- Estimated 17,990 new cases with 15,210 deaths in US in 2013 (CA Cancer J Clin 2013;63:11)
Risk factors
- In developed world, smoking and drinking are most important risk factors
- Other risk factors are diet, especially some hot liquids, Plummer-Vinson syndrome, achalasia, stricture, webs, rings, diverticula
- Higher incidence among African Americans, city dwellers, poor
- "Esophageal carcinoma belt" extends from Northeast China to Middle East, with high incidence of squamous cell carcinoma
- Adenocarcinoma associated with Barrett esophagus
Sites
- Squamous cell carcinoma: 20% upper, 50% middle, 30% lower esophagus
- Adenocarcinoma mostly in distal esophagus
- Adenocarcinoma rarely arises in heterotopic gastric mucosa or submucosal glands
Pathophysiology
- Adenocarcinoma: dysplasia - carcinoma sequence occurs in Barrett mucosa with stepwise accumulation of genetic mutations, especially p53, also HER2 / cERB-B2, cyclin D1, cyclin E, RB, p16
- Squamous cell carcinoma: genetic alterations include p53, p16INK4a, amplification of cyclin D1, cMYC and EGFR; related to smoking, alcohol, diet, possible nutritional deficiency, genetic factors
Clinical features
- Insidious onset, dysphagia to solids, followed by dysphagia to all food
- Extreme weight loss due to loss of nutrition and tumor itself
- Squamous cell carcinoma may erode through esophagus; invades respiratory tree with fistula formation and pneumonia; aorta with exsanguination; also invades mediastinum or pericardium
- Metastasis generally occurs early even in superficial tumors due to extensive lymphatic network in esophagus that allows horizontal and longitudinal spread
- Cancers of upper esophagus metastasize to cervical lymph nodes; of mid esophagus to mediastinal, paratracheal and tracheobronchial lymph nodes; of lower esophagus to gastric and celiac lymph nodes
- Metastases to liver, lungs and pleura
- Recurrences are common
Diagnosis
- Endoscopic biopsy
- Rarely identified during resection for achalasia or for lesions not amenable to biopsy
Radiology description
- Stenosis or obstruction
- Protruding mass may be detected
Overall 5 year survival
- ~ 14% (Oncologist 2005;10:590) but 47% after resection (J Am Coll Surg 2006;202:588, Dis Esophagus 2009;22:1)
- Adenocarcinoma: < 20%
- Squamous cell carcinoma: ~9%; early detection raises to 75%
- ~0% in stage IV disease
- Presence of lymph node metastases at time of surgery greatly reduces survival
Case reports
- 47 year old man with esophageal adenocarcinoma arising from Barrett dysplasia (Clin Med Res 2006;4:184)
- 53 year old man with advanced middle esophageal cancer with multiple regional lymph node metastases (Jpn J Clin Onc 2002;32:310)
Treatment
- Generally resection if possible
- Sometimes adjuvant chemoradiation prior to resection
- Chemoradiation may achieve results similar to surgery (Ann Thorac Cardiovasc Surg 2006;12:234)
- Recommended to submit proximal margins for frozen section to rule out carcinoma underneath a normal appearing mucosa (Arch Pathol Lab Med 2005;129:1558)
- Occasionally HER2+, although this is not related to survival (Mod Pathol 2007;20:120) and anti-HER2 therapy does not appear to be effective (Int J Radiat Oncol Biol Phys 2007;67:405)
Gross description
- Adenocarcinoma is located in distal esophagus and may involve gastric cardia (note: tumors in the proximal 5 cm of the stomach are regarded as esophageal carcinomas in Edge: AJCC Cancer Staging Manual, 7th Edition, 2011)
- Flat or raised patches of intact mucosa develop into nodular masses
- Squamous cell carcinoma begins as an in situ process
- Generally starts as plaque-like lesions which grow to eventually encircle the lumen
- Mostly form protruding cauliflower-like lesions (60%), may be flat (15%) or ulcerated
Gross images
Contributed by Elliot Weisenberg, M.D.

Adenocarcinoma
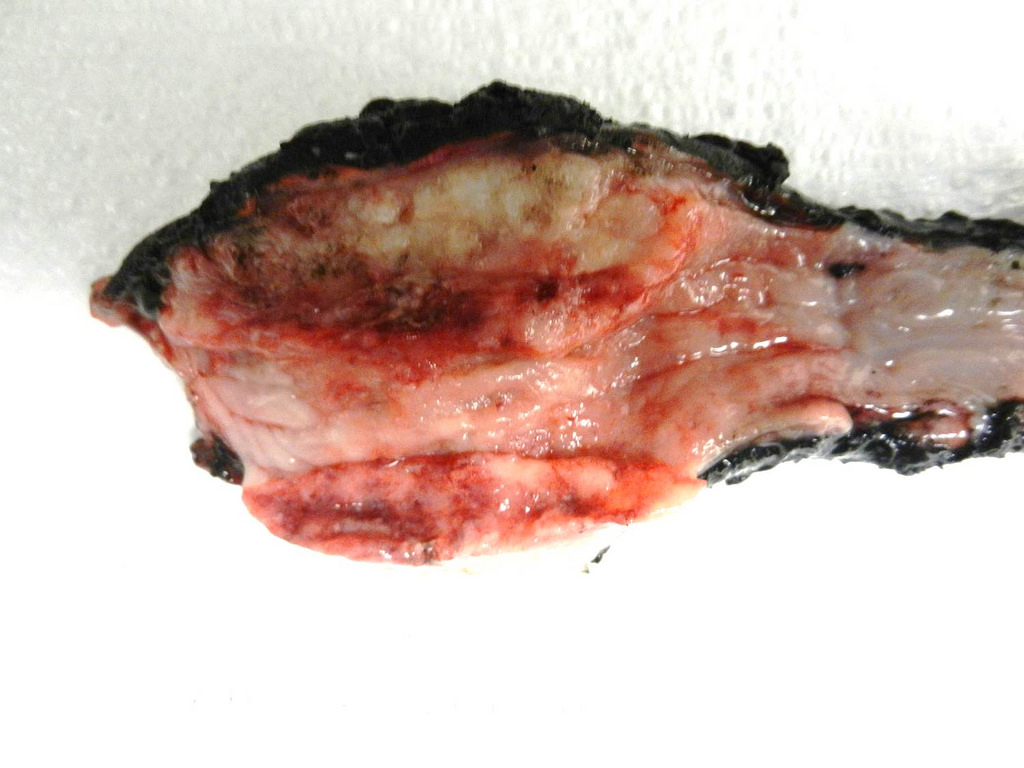
Squamous cell carcinoma
Microscopic (histologic) description
- Overwhelming majority of carcinomas of esophagus are adenocarcinoma and squamous cell carcinoma
- Diagnosis usually simple
- Generally mucin secreting adenocarcinomas, less often signet ring cell carcinoma
- Usually foci of dysplastic mucosa adjacent to cancer
- Squamous cells carcinoma tends to be well or moderately differentiated; histologic variants include verrucous, spindle cell or basaloid
- Other carcinomas are adenoid cystic carcinoma, adenosquamous carcinoma, mucoepidermoid carcinoma
- Special stains only rarely needed for diagnosis
Microscopic (histologic) images
Contributed by Elliot Weisenberg, M.D.

Adenocarcinoma
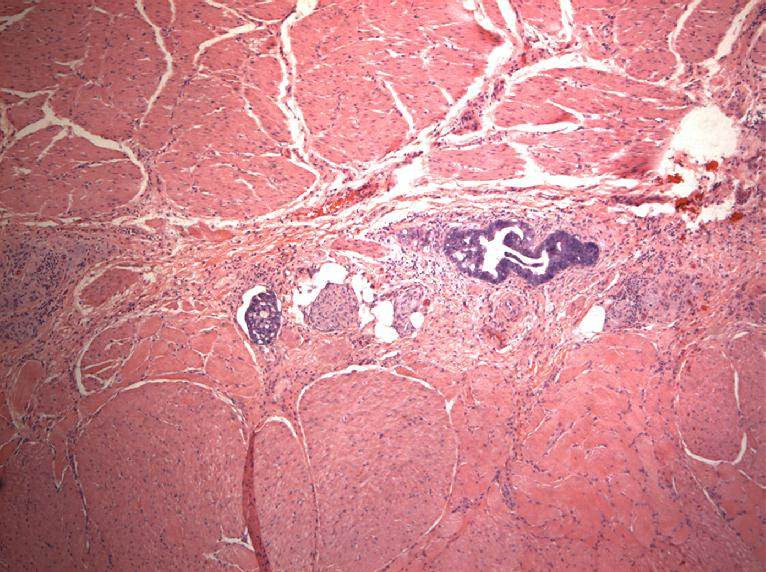
Adenocarcinoma in lymphatics
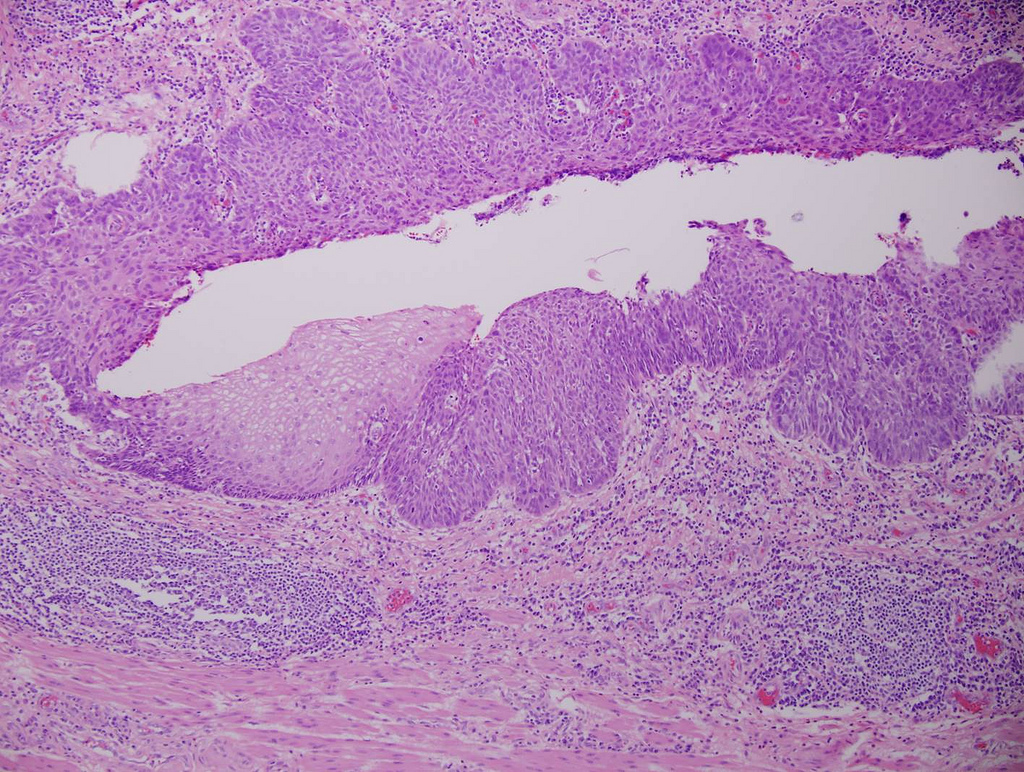
Squamous cell carcinoma in situ
Differential diagnosis
- Chemoradiation induced atypia: enlarged hyperchromatic nuclei with prominent mitotic figures but relatively mild pleomorphism in inflammatory background
- Reparative processes: atypical cells in granulation tissue but with fine chromatin, few mitotic figures; cells mature at deeper levels, keratin negative
