Cite this page: Arole V, Chen W. Staging-carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/colontumorstaging8ed.html. Accessed April 1st, 2025.
Definition / general
Adenocarcinoma, poorly differentiated, high grade neuroendocrine carcinoma and squamous cell carcinomas of the colon and rectum are covered by this staging system
These topics are not covered: appendiceal carcinoma, anal carcinoma and well differentiated neuroendocrine tumor
Essential features
AJCC 7th edition staging was sunset on December 31, 2017; as of January 1, 2018, use of the 8th edition is mandatory
Staging related diagrams from AJCC 7th edition (2006)
Primary tumor (pT)
pTX: cannot be assessed
pT0: no evidence of primary tumor
pTis: carcinoma in situ, intramucosal carcinoma (involvement of lamina propria with no extension through muscularis mucosae)
pT1: tumor invades submucosa (through the muscularis mucosae but not into the muscularis propria)
pT2: tumor invades muscularis propria
pT3: tumor invades through the muscularis propria into the pericolorectal tissues
pT4:
T4a: tumor invades through the visceral peritoneum (including gross perforation of the bowel through tumor and continuous invasion of tumor through areas of inflammation to the surface of the visceral peritoneum)
T4b: tumor directly invades or adheres to other adjacent organs or structures
Notes:
pTis
Tis (carcinoma in situ) refers to intramucosal carcinoma, which invades into the lamina propria and may involve but not penetrate through the muscularis mucosae (Ann Surg Oncol 2018;25:1454)
Tumor extension through the muscularis mucosae into the submucosa is classified as pT1; a synoptic report is required for all cancers that are pT1 and beyond but not for pTis tumors
Tis includes intraepithelial carcinoma (tumor confined to epithelium by basement membrane) and intramucosal carcinoma (carcinoma invading lamina propria)
Carcinoma in polyps
Polyps with carcinoma are staged according to pT definitions for colorectal carcinomas
Polyps with invasive carcinoma confined to muscularis mucosae are pTis and pT1 if invasive component extends into submucosa of polyps' head or stalk
Polyps with carcinoma invading the submucosa (pT1) and beyond are considered malignant polyps
If the tumor is grossly / macroscopically adherent to other organs, it is cT4; if no tumor is found microscopically within the adhesion, it should be best classified as pT3 with a note
Separation of T4 into 2 categories (T4a and T4b) is based on different outcomes in multiple datasets
T4a tumors directly invade the serosal surface (visceral peritoneum)
This includes tumors with perforation where the tumor cells are continuous with the serosal surface through inflammation and when tumor is present at the ink in serosal cleft
Even in the absence of readily demonstrable tumor cells on the serosal surface in histologic sections, grossly perforated cancers should be assigned pT4a stage (Surg Pathol Clin 2017;10:961)
Some but not all studies indicate that tumors that are < 1 mm from the serosal surface show a higher risk for peritoneal relapse
Multiple levels and additional sampling should be performed
In the absence of serosal surface involvement, the tumor should be considered pT3 (Mod Pathol 2021;34:131)
Utility of elastic stain to assess the peritoneal involvement is not universally accepted due to discontinuity of elastic lamina in colonic peritoneum (particularly absent in right colon) as well as difficulties in interpreting the stain (Mod Pathol 2015;28:S95)
pT4a should not be used in nonperitonealized portions of the colorectum (posterior aspects of ascending and descending colon, lower rectum)
T4b: transmural extension into another organ or site is a must for T4b designation; intramural extension of tumor from a segment of the large intestine into an adjacent subsite does not affect the pT classification
Regional lymph nodes (pN)
pNX: cannot be assessed
pN0: no regional lymph node metastasis
pN1: metastasis in 1 - 3 regional lymph nodes
N1a: metastasis in 1 regional lymph node
N1b: metastasis in 2 - 3 regional lymph nodes
N1c: no regional lymph nodes are positive but there are tumor deposits in the subserosa, mesentery or nonperitonealized pericolic or perirectal / mesorectal tissues
pN2: metastasis in 4 or more regional lymph nodes
N2a: metastasis in 4 - 6 regional lymph nodes
N2b: metastasis in 7 or more regional lymph nodes
Notes:
Minimum of 12 lymph nodes must be recovered for lymph node staging to be considered accurate in curative resections
Number of recovered nodes has been reported to correlate with better prognosis, likely due to more accurate staging or likely from implying better host response
N category is limited to only the regional nodes that are in the lymphatic drainage area of the tumor; metastasis to lymph nodes not found along vascular arcades of the marginal artery or pericolonic, perirectal or mesorectal nodes should be considered distant metastasis (M1a)
Lymph nodes with micrometastasis (0.2 - 2 mm) as well as macrometastasis (> 2 mm) are considered positive
Isolated tumor cells (single tumor cells or groups < 0.2 mm in maximum dimension) are classified as N0 as they were found to have no adverse prognosis (Eur J Surg Oncol 2014;40:263)
Tumor deposits are discrete tumor nodules of any shape, contour or size that lack associated lymphoid tissue, vascular structures or neural structures found within the lymph drainage area of the primary carcinoma
Only in the absence of unequivocal lymph node metastases, tumor deposits are recorded as N1c; in cases with lymph node metastasis, the number of tumor deposits is not added to the number of positive lymph nodes
There is no consensus opinion on assigning lymph nodes with acellular mucin pool deposits as positive (N1) or negative (N0) (Mod Pathol 2020;33:153)
Distant metastasis (pM)
M0: no distant metastasis by imaging; no evidence of tumor in other sites or organs (this category is not assigned by pathologists)
M1a: metastasis confined to 1 organ or site without peritoneal metastasis
M1b: metastasis to 2 or more sites or organs is identified without peritoneal metastasis
M1c: metastasis to the peritoneal surface is identified alone or with other site or organ metastases
Notes:
Metastasis to lymph nodes outside of the drainage area of the tumor (nonregional lymph nodes) should be considered distant metastasis (M1a)
Multiple metastases in an organ, even paired organs (ovaries, lungs), are still M1a disease
Pathologist should not assign the global designation pM0, as metastasis unknown to the pathologist may be present
Prefixes
c: clinical (cTNM)
p: pathological (pTNM)
y: postneoadjuvant chemoradiation therapy (ycTNM or ypTNM)
r: recurrent tumor stage (rTNM)
a: cancer discovered incidentally during autopsy (aTNM)
Notes:
Current clinical practice involves neoadjuvant chemoradiation for cT3 and cT4 rectal cancers
Microscopic evidence of residual disease has been shown to be associated with better prognosis than gross residual disease, which mandates thorough sectioning of specimens from neoadjuvant treated cancers
Tumor regression should be assessed in the primary tumor and not based on nodal metastasis assessment
Although acellular mucin is considered to represent completely eradicated tumor and recommendations are not to use mucin pools without viable tumor cells in assigning pT or pN category, there seems to be lack of consensus among pathologists across the world (Mod Pathol 2020;33:153)
When the mucin pools are present at the radial margin without any viable cells, the practice among most pathologists is to render the margin status negative (Mod Pathol 2020;33:153)
Grading of quality and completeness of the mesorectum in a total mesorectal excision (TME)
Complete: intact and smooth mesorectum, defects (if present) are < 5 mm, there is no coning and the circumferential resection margin is smooth and regular
Nearly complete: mesorectum is moderately bulky and irregular with defects > 5 mm but none extending to muscularis propria, no areas of visibility of the muscularis propria except at the insertion site of the levator ani muscle, there is moderate coning and an irregular circumferential resection margin
Incomplete: little bulk to mesorectum, the muscularis propria is visible through defects, there is moderate to marked coning and on transverse sectioning, very irregular circumferential resection margin
Circumferential resection margin (CRM) or nonperitonealized margin involvement strongly predicts local recurrence and is found to be associated with poor survival (J Clin Oncol 2008;26:303, Ann Surg 2002;235:449)
Although there is some controversy in the definition of positive margin, if the tumor is identified within 1 mm of inked CRM / radial margin, it should be regarded as positive (Ann Surg 2022;275:e549)
Acellular mucin identified on the margin in treated / treatment naïve carcinomas are considered negative (Mod Pathol 2015;28:S95)
There is no consensus on the issue of positive lymph node at the CRM (Ann Surg 2022;275:e549)
AJCC prognostic stage groups
Stage 0:
Tis
N0
M0
Stage I:
T1 - T2
N0
M0
Stage IIA:
T3
N0
M0
Stage IIB:
T4a
N0
M0
Stage IIC:
T4b
N0
M0
Stage IIIA:
T1 - T2
N1 / N1c
M0
Stage IIIA:
T1
N2a
M0
Stage IIIB:
T3 - T4a
N1 / N1c
M0
Stage IIIB:
T2 - T3
N2a
M0
Stage IIIB:
T1 - T2
N2b
M0
Stage IIIC:
T4a
N2a
M0
Stage IIIC:
T3 - T4a
N2b
M0
Stage IIIC:
T4b
N1 - N2
M0
Stage IVA:
any T
any N
M1a
Stage IVB:
any T
any N
M1b
Stage IVC:
any T
any N
M1c
Prognostic tools for colon and rectum cancer meeting all AJCC quality criteria
Which of the following findings corresponds to T1 pathological stage (pT1) in colorectal carcinoma?
Polyp with high grade dysplasia and no invasion
Tumor invading and limited to lamina propria
Tumor invading into muscularis mucosae
Tumor invading through muscularis mucosae into submucosa
Board review style answer #1
D. Tumor invading through muscularis mucosae into submucosa. Answers B and C are incorrect because tumor invasion that is limited to lamina propria and invasion into muscularis mucosae describe pTis. Answer A is incorrect because a polyp with high grade dysplasia and no invasion is not invasive carcinoma.
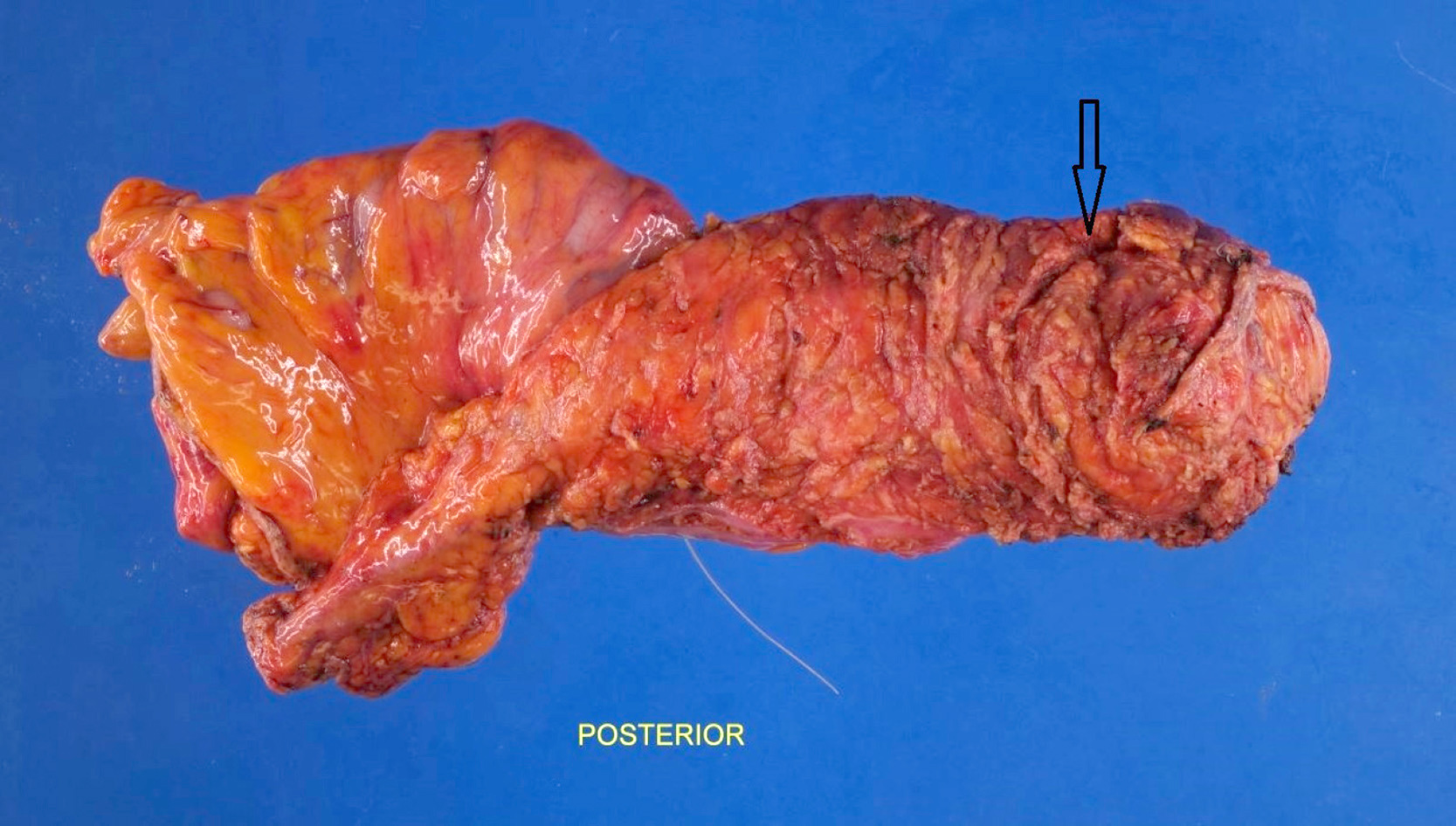
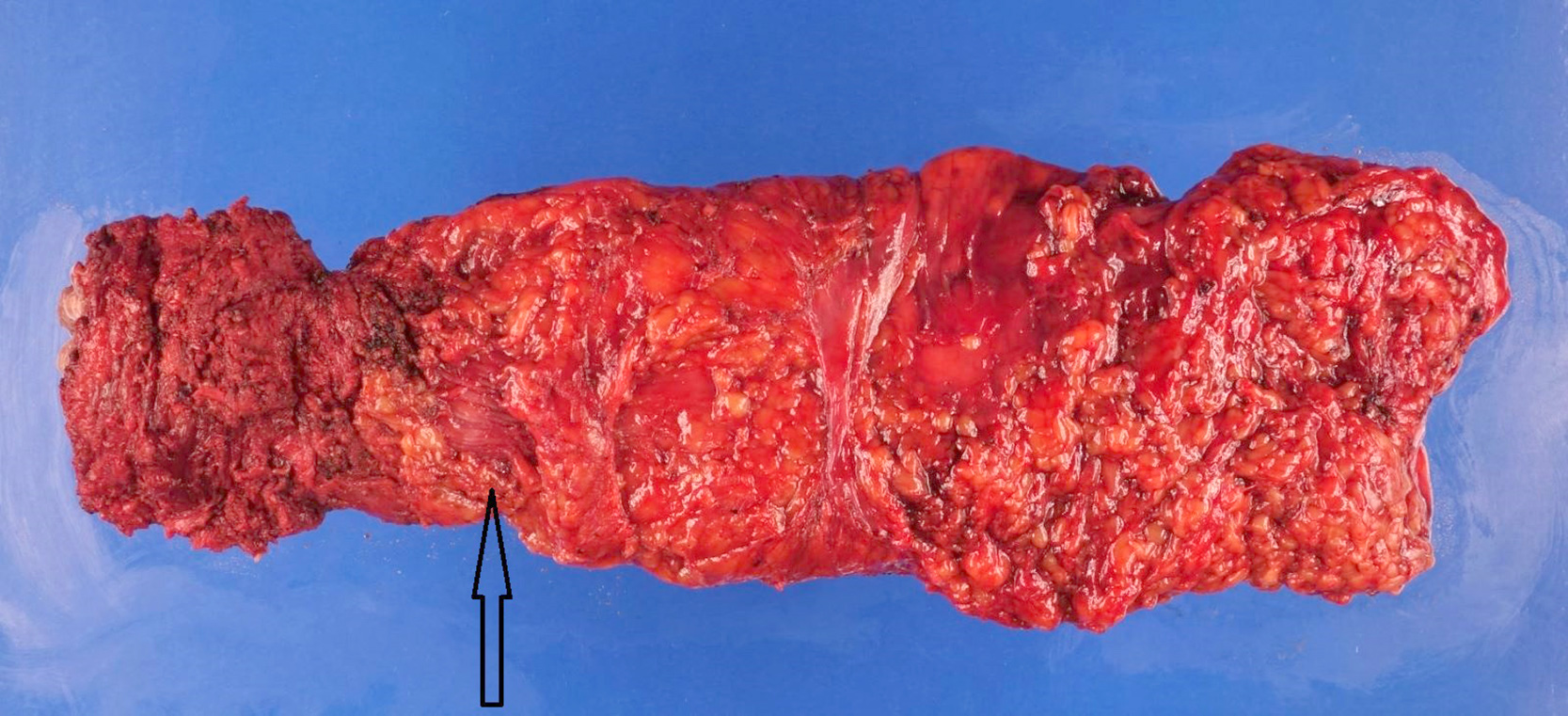
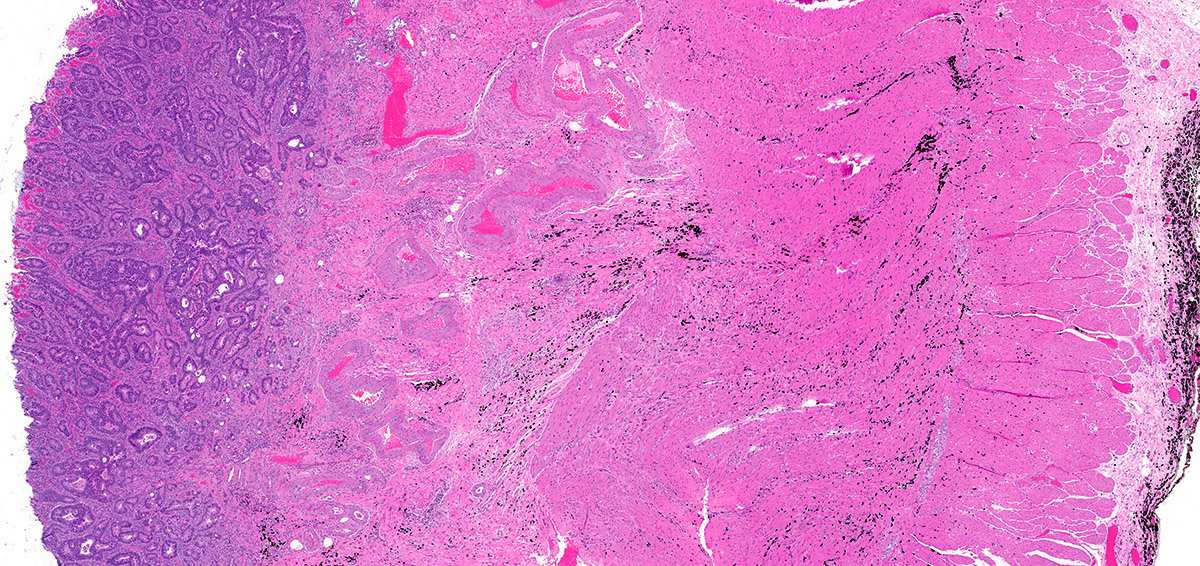
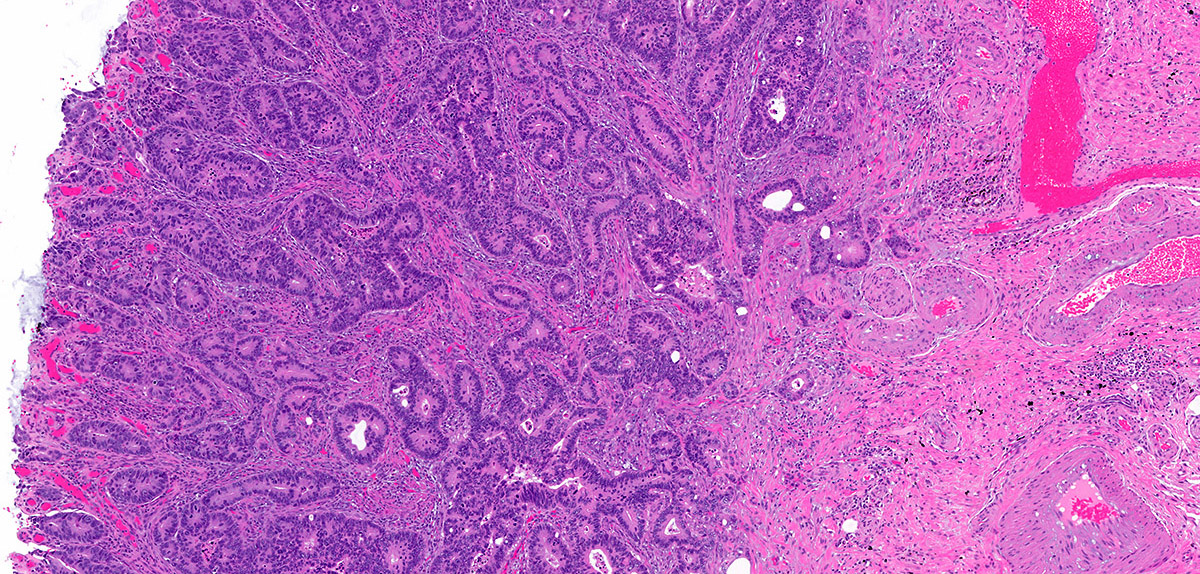
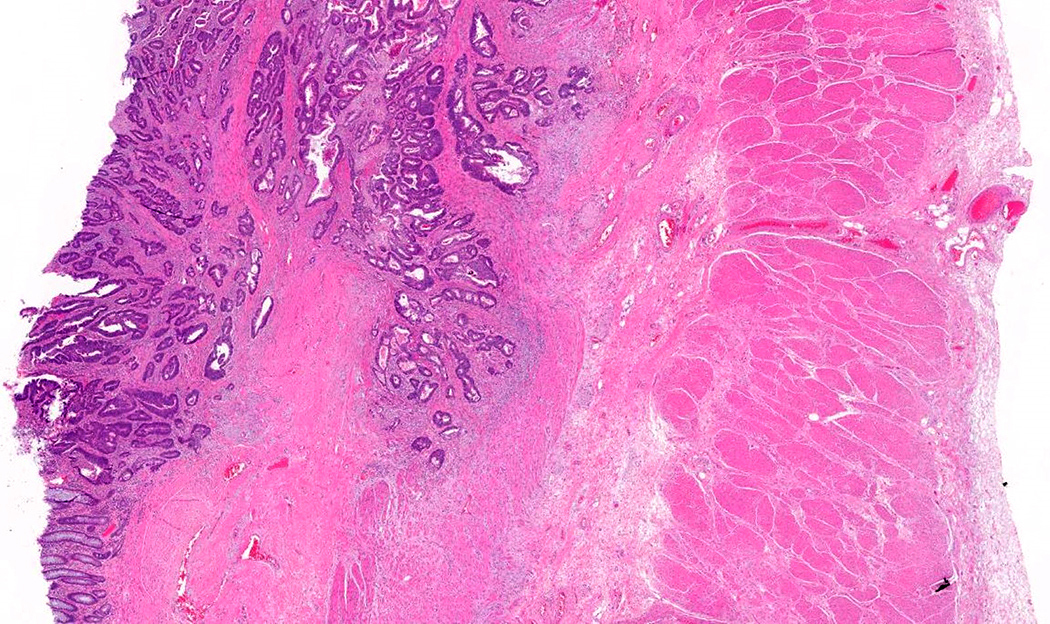
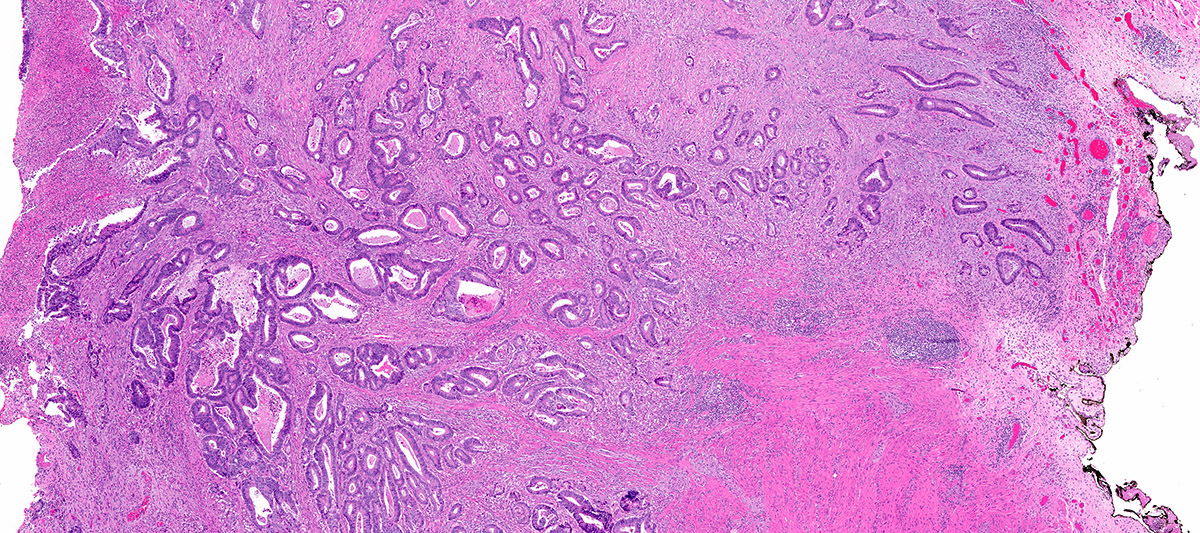
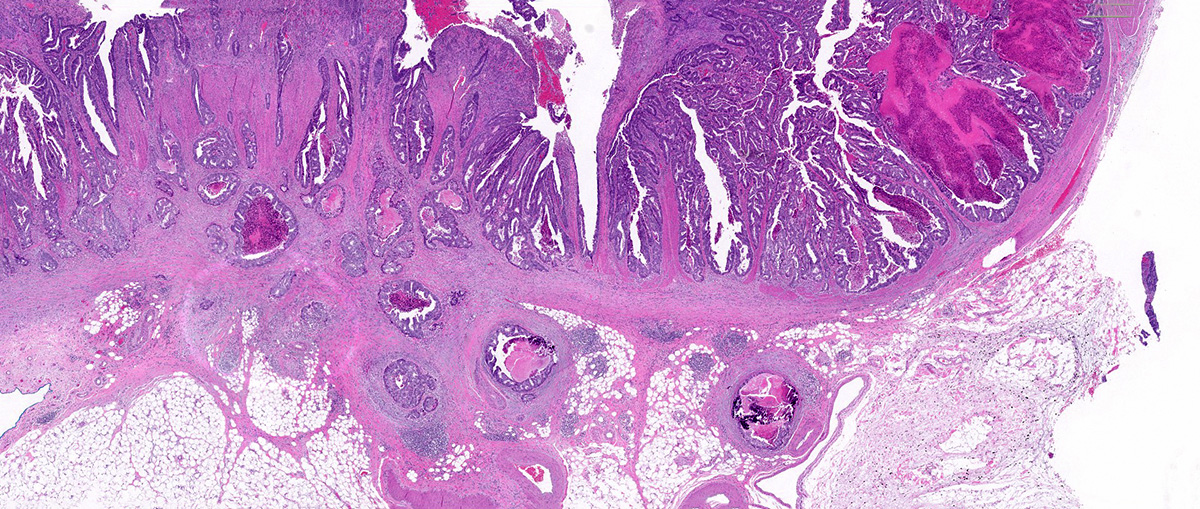
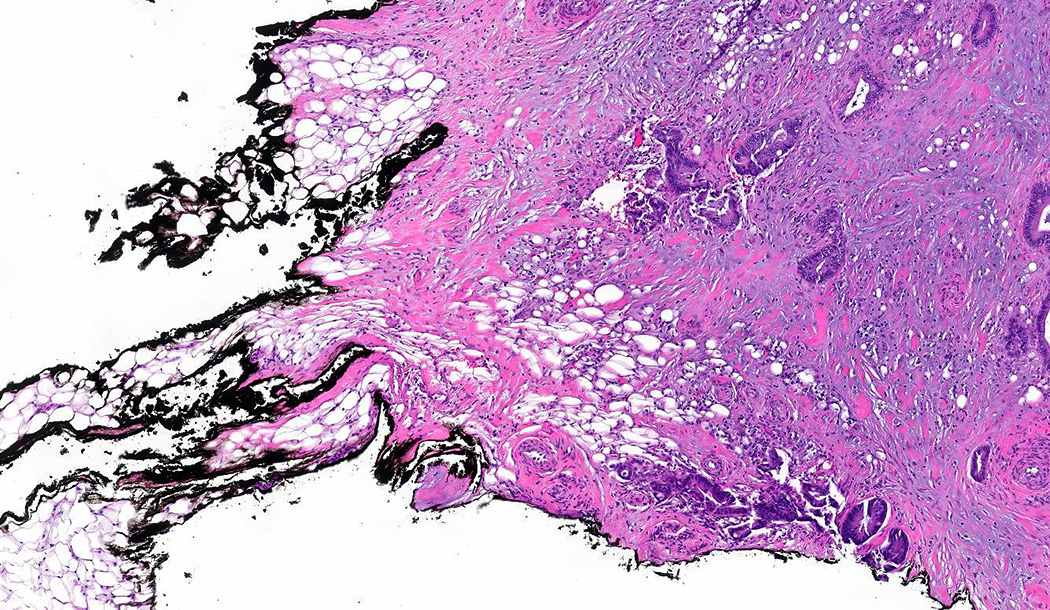
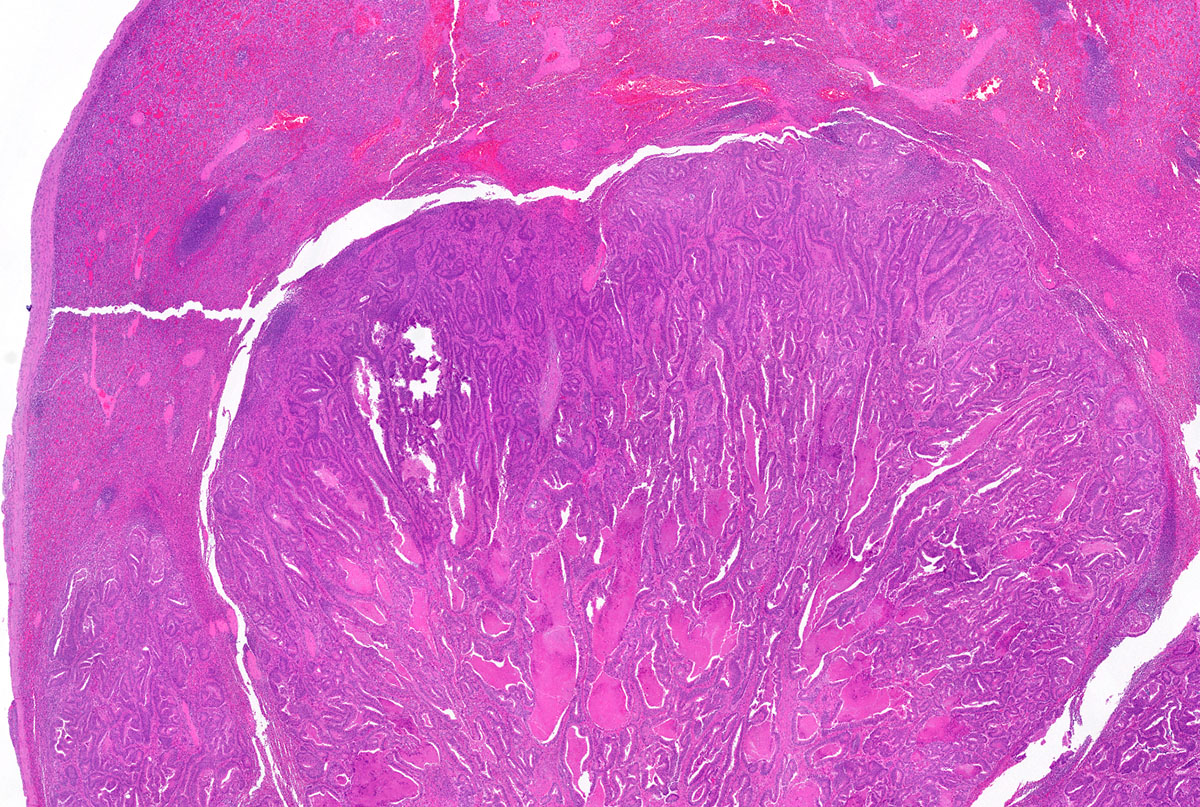
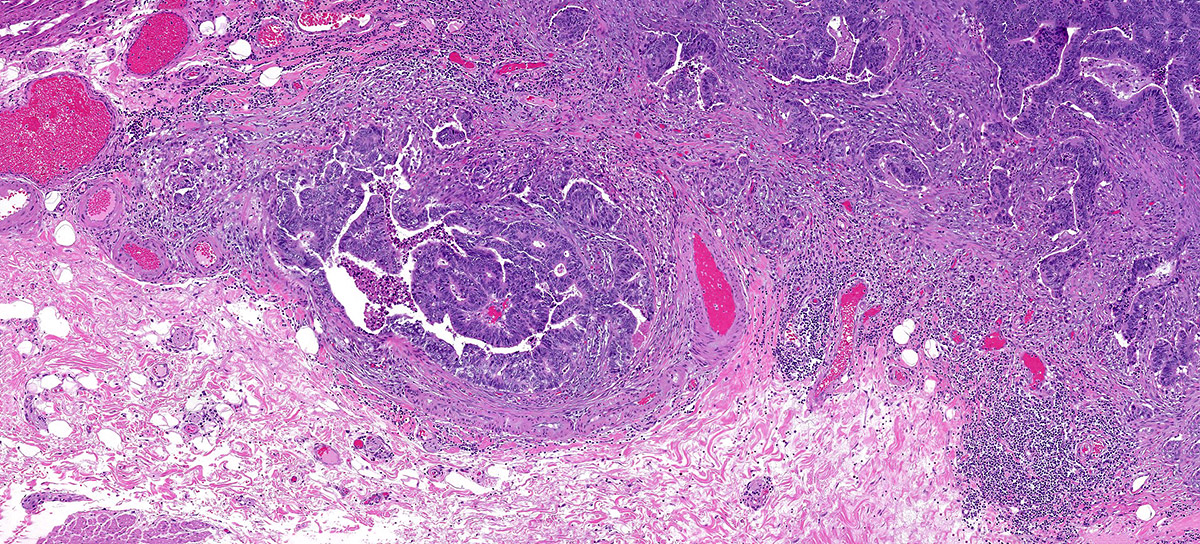
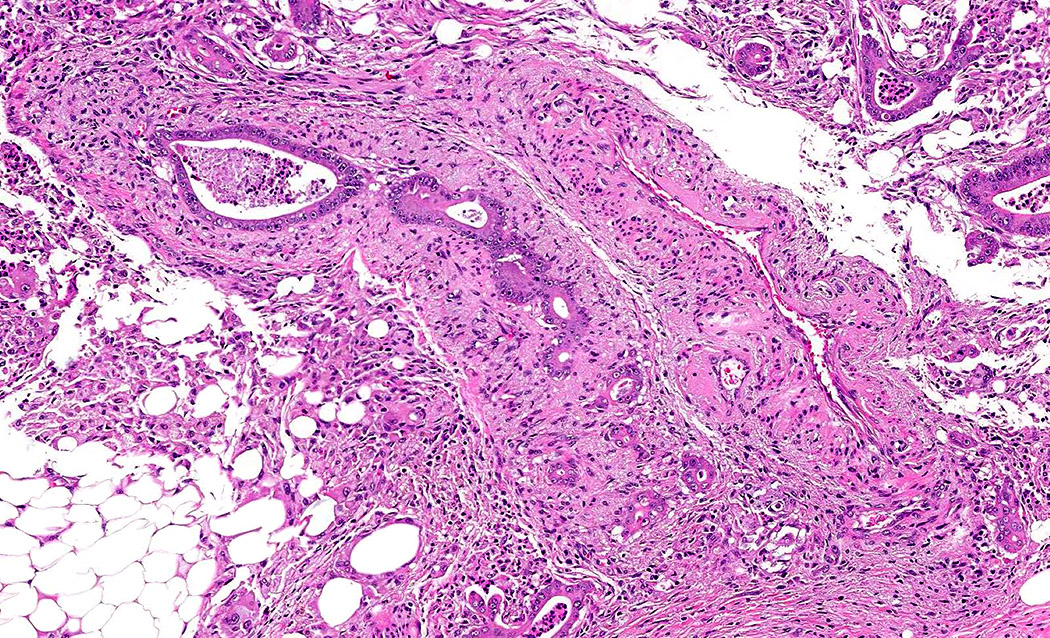
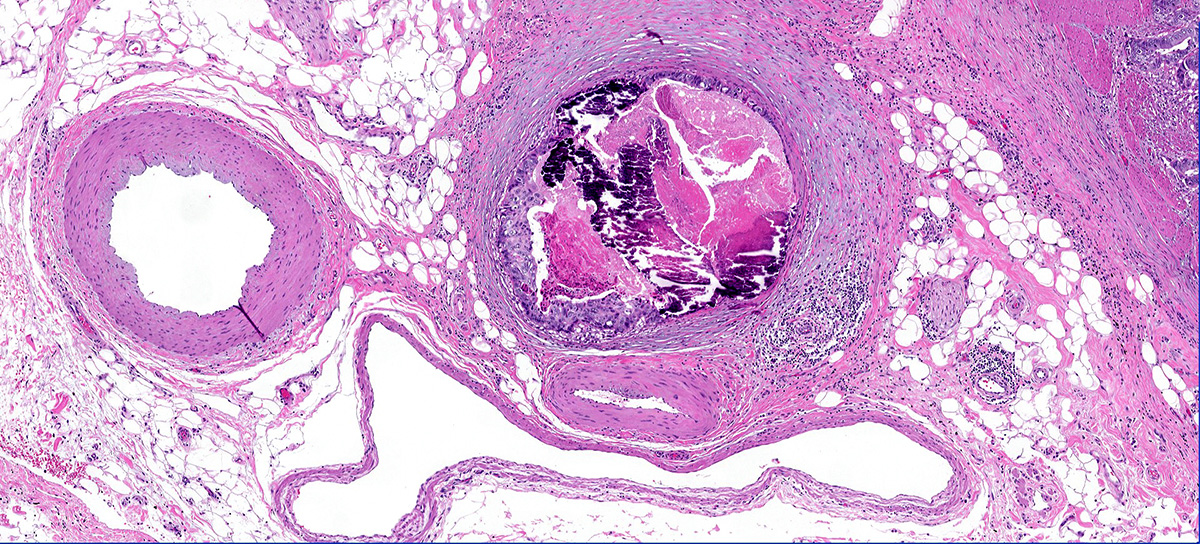
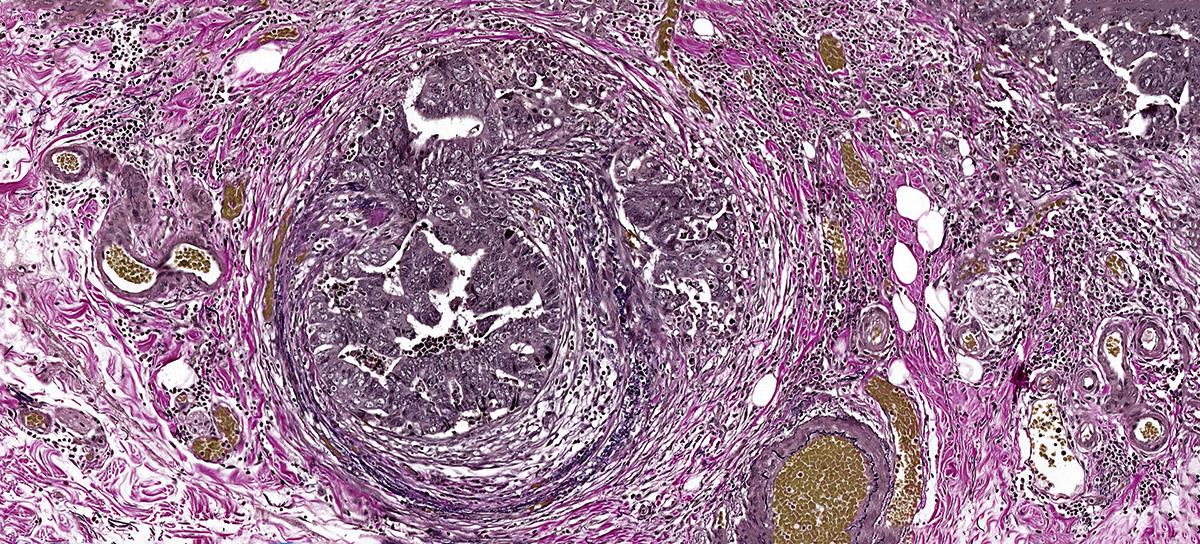
What is the pathologic stage for this ascending colon cancer based on the above images?
pT1
pT2
pT3
pT4
Board review style answer #2
A. pT1. The tumor is invading and confined to the submucosa. Note the tumor glands are next to the thick walled vessels of the submucosa. Answer B is incorrect because pT2 would be tumor invading into (but not through) the muscularis propria. Answer C is incorrect because pT3 would be tumor invading through the muscularis propria into the pericolorectal soft tissue. Answer D is incorrect because pT4 would be invasion of serosa or adjacent structures.