

CNS nontumor
Infections
Acute viral infections
CMV infections
Author: Mark Cohen, M.D.
Last author update: 1 June 2014
Last staff update: 4 December 2020
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Cytomegalovirus [title] CNS

Table of Contents
Definition / general | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Differential diagnosisCite this page: Cohen M. CMV infections. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cnscmv.html. Accessed April 25th, 2024.
Definition / general
- Cytomegalovirus (CMV) is the largest of the human herpes viruses and may cause a variety of clinical manifestations ranging from asymptomatic to fatal
- Severe, often fatal central (CNS) and peripheral nervous system infections are usually seen in patients with compromised immune systems or in maternal fetal infections in utero (Ther Adv Neurol Disord 2012;5:279)
Epidemiology
- The vast majority of CMV CNS infections occur in patients with severe suppression of cell mediated immunity; infections are only rarely reported in apparently immunocompetent patients
- Prior to combined antiretroviral therapy, CMV nervous system infections usually occurred in AIDS patients; currently, they are seen as complications of organ transplantation, especially bone marrow and hematopoietic stem cell (Rev Inst Med Trop Sao Paulo 2010;52:305, PLoS One 2013;8:e77805)
- Cytomegalovirus is also the most common pathogen causing congenital fetal infection, resulting in severe neurological damage
Sites
- May infect all levels of the nervous system but classically, CMV encephalitis causes damage to subependymal regions of the cerebrum, cerebellum and brainstem
- Spinal cord and nerve root infection is also common in immunocompromised hosts
Pathophysiology
- Cytomegalovirus is easily transmitted from person to person via a variety of secretions
- Maternal fetal infection usually occurs transplacentally but may also be transmitted via general secretions or breast milk
- CMV may also be transmitted by transplanted organs
- In the general population, asymptomatic infection usually occurs early in life and remains latent in immunocompetent individuals
- Impaired cell mediated immunity appears to be required for viral infection of the mature nervous system (Curr Immunol Rev 2010;6:38, PLoS Pathog 2012;8:e1002849)
Etiology
- Lesions are caused by lytic destruction of infected cells within the brain, spinal cord or peripheral nerve roots
Clinical features
- Adult cytomegaloviral encephalitis usually produces no unique symptomatology, beyond that of clinical encephalitis
- Similarly, spinal cord and nerve root infections demonstrate no symptomatology specific to this virus
- Congenital cytomegaloviral infection often results in a constellation of abnormalities referred to as cytomegalic inclusion disease, including microcephaly, hearing loss, intracranial calcifications, hepatosplenomegaly and thrombocytopenic purpura
Diagnosis
- Due to the absence of specific clinical symptomatology, diagnosis usually requires polymerase chain reaction amplification of cytomegaloviral genome from cerebrospinal fluid or other specimens (Emerg Infect Dis 2013;19:1470)
Laboratory
- Cytomegaloviral infection of the nervous system generally manifests with typical CSF findings of increased protein and pleocytosis
- Features specific to CMV have not been identified
Radiology description
- Cytomegaloviral encephalitis tends to localize to the ependymal and subependymal regions
- Although MRI may demonstrate signal changes along the lateral ventricles, septum pellucidum, corpus callosum and fornices, these changes are usually quite subtle on conventional T1 and T2 weighted images, even after contrast administration
- Recent studies indicate that diffusion weighted imaging abnormalities along the ependymal lining is a more sensitive indication of cytomegaloviral encephalitis
Radiology images
Images hosted on other servers:

Ventricular dilatation

Curvilinear high signal intensities
Prognostic factors
- Specific prognostic factors have not been extensively elucidated but recent studies indicate that T cell depleted hematopoietic stem cell transplantation appears to predispose to central nervous system infection (BMC Infect Dis 2012;12:238)
Case reports
- Boy infant with severe late onset multisystemic Cytomegalovirus infection (BMC Pediatr 2013;13:142)
- 20 year old man with diffusion MRI findings of Cytomegalovirus associated ventriculitis (Br J Radiol 2011;84:e179)
- 33 year old woman with CMV associated encephalitis and antineuronal autoantibodies (BMC Neurol 2012;12:87)
Treatment
- Antiviral prophylaxis and therapy generally includes ganciclovir, cidofovir or foscarnet (Antiviral Res 2009;83:207)
Gross description
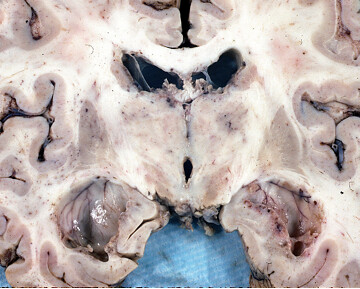
- At autopsy, coronal sectioning through the thalamic nuclei of an adult with AIDS and central nervous system Cytomegalovirus infection demonstrates necrotizing ependymitis with fibrinous exudate lining the ventricular system
- Hydrocephalus can also be appreciated (especially in the temporal horns of the lateral ventricles), which is secondary to aqueductal stenosis consequent to similar inflammatory necrosis within the ependymal lining (shown in the second gross image)
- Congenital cytomegalic inclusion disease secondary to transplacental fetal infection manifests as microencephaly with hydrocephalus (gross image 3 and 4)
Gross images
Contributed by Mark Cohen, M.D.
Coronal section

Inflammatory necrosis
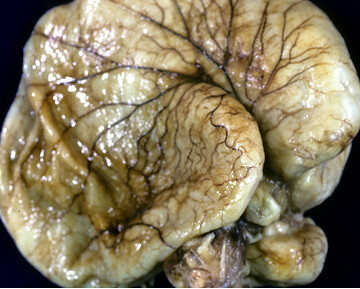

Microencephaly with hydrocephalus
Microscopic (histologic) description
- Although immunohistochemical staining for Cytomegalovirus may be used as a confirmational assay, the distinctive nuclear and cytoplasmic cytopathic changes on routinely stained sections are diagnostic
Microscopic (histologic) images
Contributed by Mark Cohen, M.D.
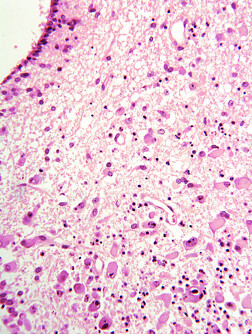
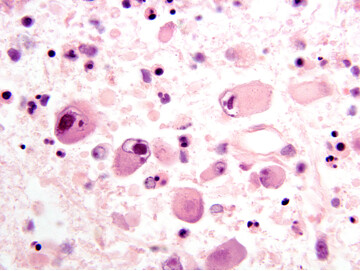
Low and high power, H&E
Differential diagnosis
- As in other organs, the differential diagnosis includes a variety of viral infections, though none demonstrate the characteristic cytological cytomegaly with both cytoplasmic and nuclear viral inclusions
- In congenital Cytomegalovirus inclusion disease, gross differential diagnosis includes a variety of other encephaloclastic fetal diseases, most notably intrauterine ischemia
