

Cervix
Benign / nonneoplastic epithelial lesions
Lobular endocervical glandular hyperplasia
Authors: Adam Lechner, B.M., Carlos Parra-Herran, M.D.
Editorial Board Member: David B. Chapel, M.D.
Deputy Editor-in-Chief: Gulisa Turashvili, M.D., Ph.D.


Last author update: 10 January 2023
Last staff update: 10 January 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Lobular endocervical glandular hyperplasia


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Lechner A, Parra-Herran C. Lobular endocervical glandular hyperplasia. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cervixlobularendocerv.html. Accessed November 27th, 2024.
Definition / general
- Rare lesion of the cervix characterized by a proliferation of discrete lobules of small, round glands showing gastric type differentiation
Essential features
- Benign (though frequent association with underlying malignancy poses a challenge for management)
- Involves the upper endocervical canal of predominantly perimenopausal women
- Not related to high risk HPV infection
- Well differentiated (minimal deviation type) gastric type adenocarcinoma is the primary differential diagnosis of this lesion
- Immunohistochemical profile: HIK1083+, MUC6+, PAX2+ (retained), CEA-, ER-, PR-
- Atypical cytologic and architectural features are associated with progression to malignancy (known as atypical LEGH; now classified as a form of adenocarcinoma in situ, gastric type)
Terminology
- Lobular endocervical glandular hyperplasia (LEGH) is part of the benign spectrum of gastric type epithelium in the uterine cervix
- Atypical LEGH is now considered to be a form of gastric type adenocarcinoma in situ (gAIS)
- Minimal deviation adenocarcinoma (MDA), also known as adenoma malignum:
- Malignant lesion, now referred to as HPV independent endocervical adenocarcinoma, gastric type; it is part of the differential diagnosis of LEGH
ICD coding
- ICD-10: N88.9 - noninflammatory disorder of cervix uteri, unspecified
Epidemiology
- Rare; first described in 1999 (Am J Surg Pathol 1999;23:886)
- 0.7% incidence in a series of 1,167 consecutive hysterectomies in Japanese women (Histopathology 2001;39:364)
- Mean age: 45 - 49 years; range: 37 - 71 years (Am J Surg Pathol 1999;23:886, Gynecol Oncol 1999;74:504)
- Incidental nature, combined with undersampling of grossly benign cervixes, may contribute to underestimation
Sites
- Located in the upper part of the endocervical canal (rather than at the transformation zone) and usually confined to the inner half of the cervix (Minerva Chir 1989;44:1107)
Pathophysiology
- LEGH is part of the spectrum of pyloric gland metaplasia in the uterine cervix (Am J Surg Pathol 2000;24:325)
- Clinical and molecular evidence have led authors to suggest that LEGH is a metaplastic process (Oncol Lett 2019;18:2592, Histopathology 2001;39:364)
- However, LEGH is frequently found in cases of gastric type adenocarcinoma (~20%) (Am J Surg Pathol 2015;39:1449)
- In addition, 3q gain and 1p loss, known to occur in gastric type adenocarcinomas, have been reported in LEGH (Am J Surg Pathol 2008;32:1807)
Etiology
- Association with Peutz-Jeghers syndrome (due to germline STK11 / LKB1 mutations) has been reported (Pathol Int 2011;61:369, Ann Oncol 2012;23:2990)
- May be associated with the recently described synchronous mucinous metaplasia and neoplasia of the female genital tract (SMMN FGT) (Histopathology 2009;54:184)
- LEGH and other gastric type cervical glandular lesions are not associated with persistent infection by high risk HPV
Diagrams / tables
Images hosted on other servers:

Gastric type cervical lesion spectrum

Proposed management algorithm
Clinical features
- Often incidental in hysterectomy or cervical loop electrosurgical excision specimens (LEEP)
- Up to half of cases present with symptoms suggestive of MDA (Am J Surg Pathol 1999;23:886):
- Watery / mucoid vaginal discharge
- Cervical mass
Diagnosis
- Constellation of features on MRI and Pap smear can yield reasonably high suspicion; however, histologic evaluation remains necessary for definitive diagnosis and exclusion of occult malignant disease
Radiology description
- Multiple large cysts encircling a smaller, central solid component in the upper cervix; termed the cosmos pattern (referring to the flower, Cosmos bipinnatus)
- Gastric type adenocarcinomas, including MDA, tend to present instead as predominantly solid lesions; however, some may display overlapping features (Abdom Imaging 2015;40:459)
- Observing a hypointense cosmos pattern lesion relative to the surrounding cervical stroma on T1 weighted imaging gave a specificity of 95% for gastric type, mucin positive lesions in one series (J Obstet Gynaecol Res 2021;47:745)
Radiology images
Images hosted on other servers:



LEGH with cosmos pattern
Prognostic factors
- Most of the first described lesions showed benign clinical behavior and did not recur (Am J Surg Pathol 1999;23:886)
- Retrospective review of previously miscategorized LEGH as MDA showed that these patients did not experience recurrence or metastases and were alive at follow up (Pathol Int 2003;53:440, Pathol Int 2005;55:412, Int J Gynecol Cancer 2011;21:1287)
- Subsequent reports of MDA associated with coexisting LEGH raised suspicions of possible premalignant potential (Mod Pathol 2005;18:1199, Pathol Res Pract 2008;204:683)
- A recent whole exome sequencing study has not uncovered evidence for LEGH transformation to MDA; however, the population size was small (Oncol Lett 2019;18:2592)
- LEGH with atypical cytologic or architectural features, while rare, is associated with risk of progression to malignancy
- Molecular analysis supports premalignant potential of this lesion and complete excision is recommended, although no formal management guidelines exist (Surg Pathol Clin 2016;9:243)
- Up to 41% of gastric type adenocarcinomas of the cervix have associated LEGH (Int J Gynecol Cancer 2011;21:1287)
Case reports
- 30 year old woman with diffuse, watery vaginal discharge (Eur J Obstet Gynecol Reprod Biol 2012;160:117)
- 49 year old woman with LEGH found to have mucinous adenocarcinoma in situ of the endometrium on hysterectomy (Gynecol Oncol 2011;122:686)
- 50 year old woman with LEGH diagnosed by MRI / cervical Pap smear and worsening cytology after 5 years of follow up (Gynecol Oncol Rep 2020;32:100571)
Treatment
- Pure LEGH without atypical features, diagnosed on hysterectomy, is considered benign and requires no additional treatment / follow up
- If diagnosed on biopsy, cervical LEEP or conization, conduct may vary:
- Hysterectomy may be preferred to confirm absence of coexisting MDA or gAIS; however, deferral for fertility preservation is an alternative option (Adv Anat Pathol 2013;20:227)
- Symptomatic presentation (discharge / cervical mass) warrants cautious management, which should include at least close follow up with diagnostic imaging and further sampling
- Diagnosis on biopsy should prompt consideration for cervical loop electrosurgical excision or conization
- Diagnostic algorithm with retrospective validation has been proposed for managing patients with multicystic, gastric mucin positive lesions identified on MRI and cervical Pap smear (Int J Gynecol Cancer 2011;21:1287, J Obstet Gynaecol Res 2016;42:1588)
Gross description
- Cut surface displays variably sized cystic spaces within a thickened, fibrotic cervical wall
- Typically confined to the inner half of the cervix, in the superior aspect near the internal os
- Reference: Adv Anat Pathol 2013;20:227
Microscopic (histologic) description
- Well demarcated lesion with lobular / acinar architecture composed of a central crypt, sometimes with cystic dilation, surrounded by smaller, round shaped glands and cysts arranged in a floret-like pattern
- Most cases are confined to the inner third of the cervical wall; however, larger cystic lesions may be seen deeper within the cervical wall
- Central and peripheral glands are lined by columnar cells with pale eosinophilic cytoplasm and basally oriented, small nuclei with bland morphology
- Focal intestinal metaplasia may be observed, especially within the central glands
- May have, at most, mild nuclear atypia
- No desmoplasia, no irregularly shaped glands, no mitotic figures, no squamous differentiation
- Atypical LEGH, now regarded as a form of gastric type AIS, is defined as architecturally consistent with LEGH but with ≥ 4 of the following features (Mod Pathol 2004;17:962):
- Nuclear enlargement
- Irregular nuclear contours
- Distinct nucleoli and coarse chromatin
- Loss of polarity
- Mitotic figures (occasional)
- Apoptotic bodies or luminal nuclear debris
- Intraluminal papillary projections
Microscopic (histologic) images
Contributed by Carlos Parra-Herran, M.D.
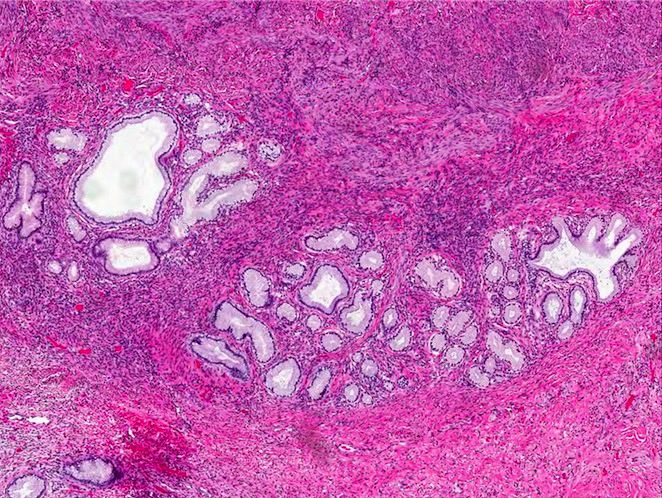
Densely packed glands
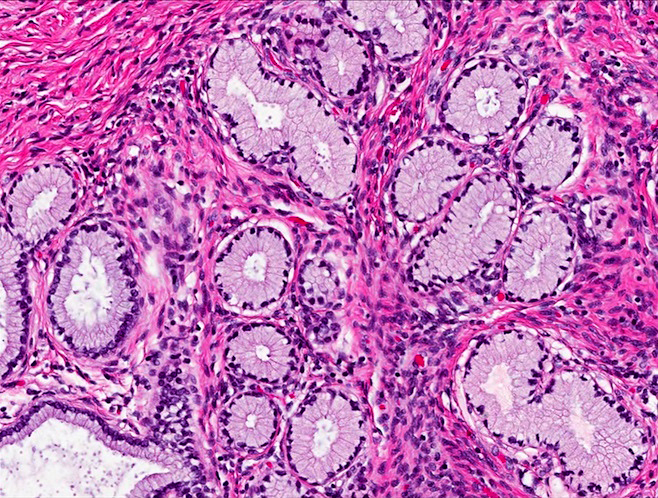
Round mucinous glands
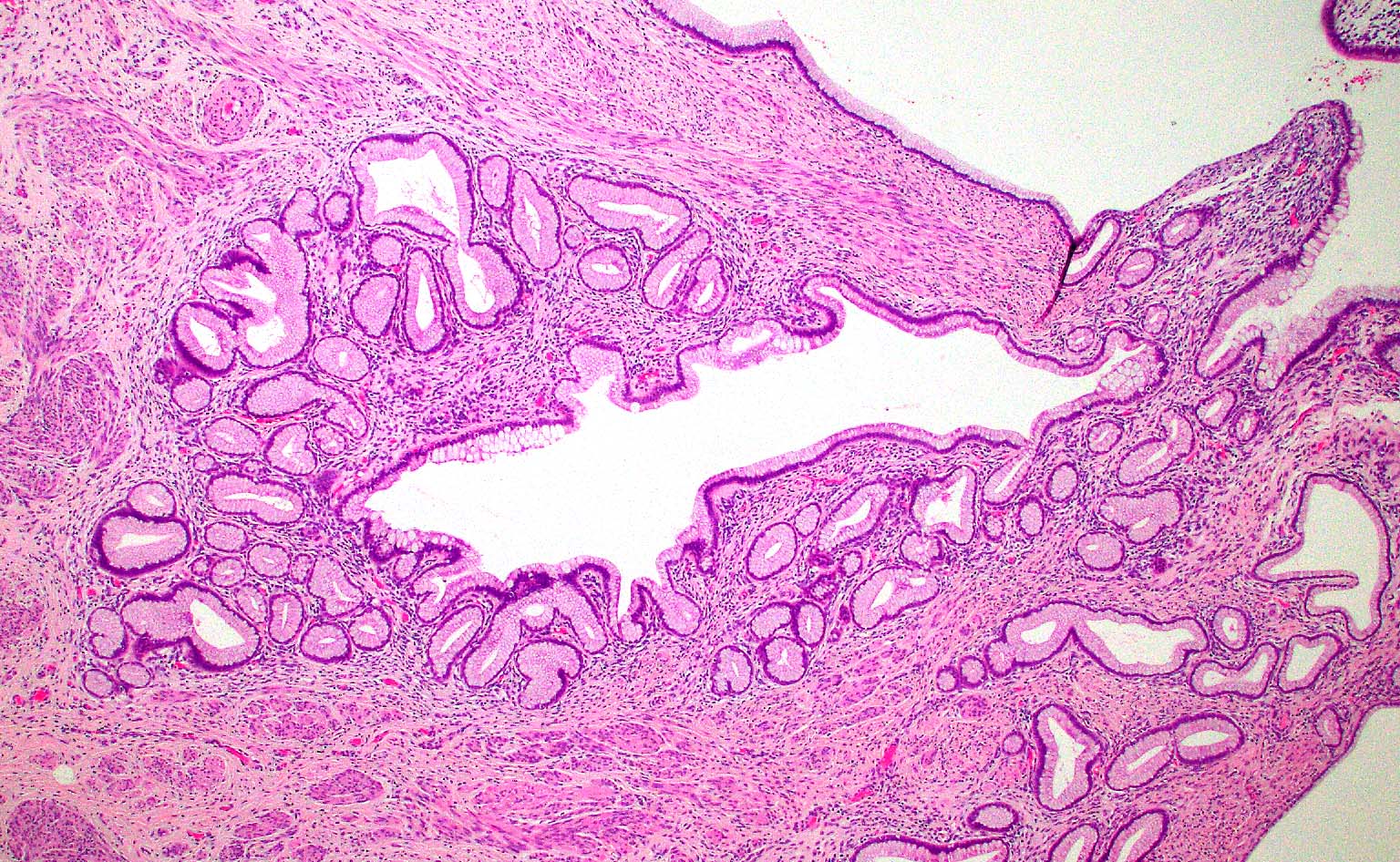
Lobulated / floret-like appearance
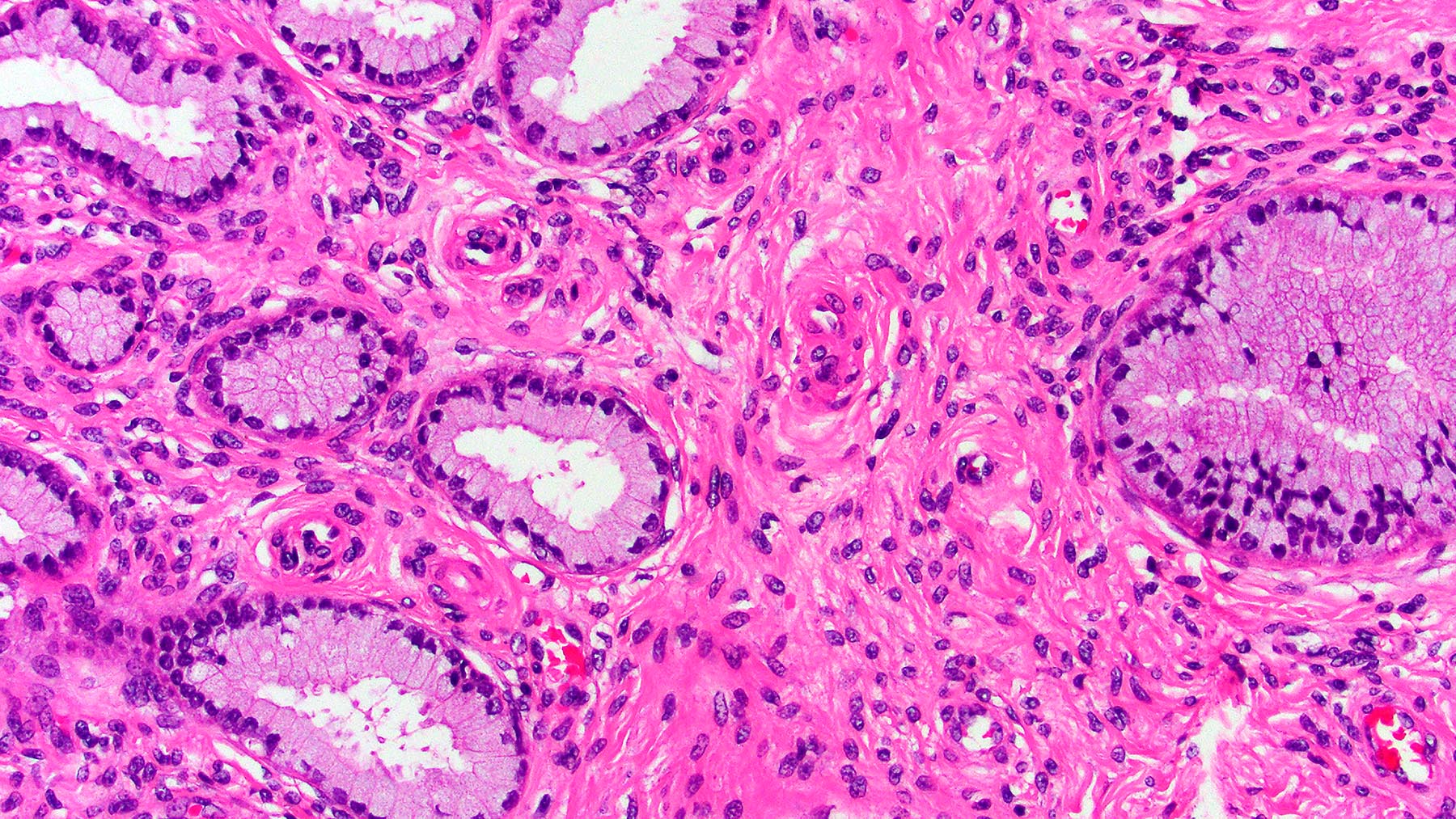
Glands lined by benign columnar cells
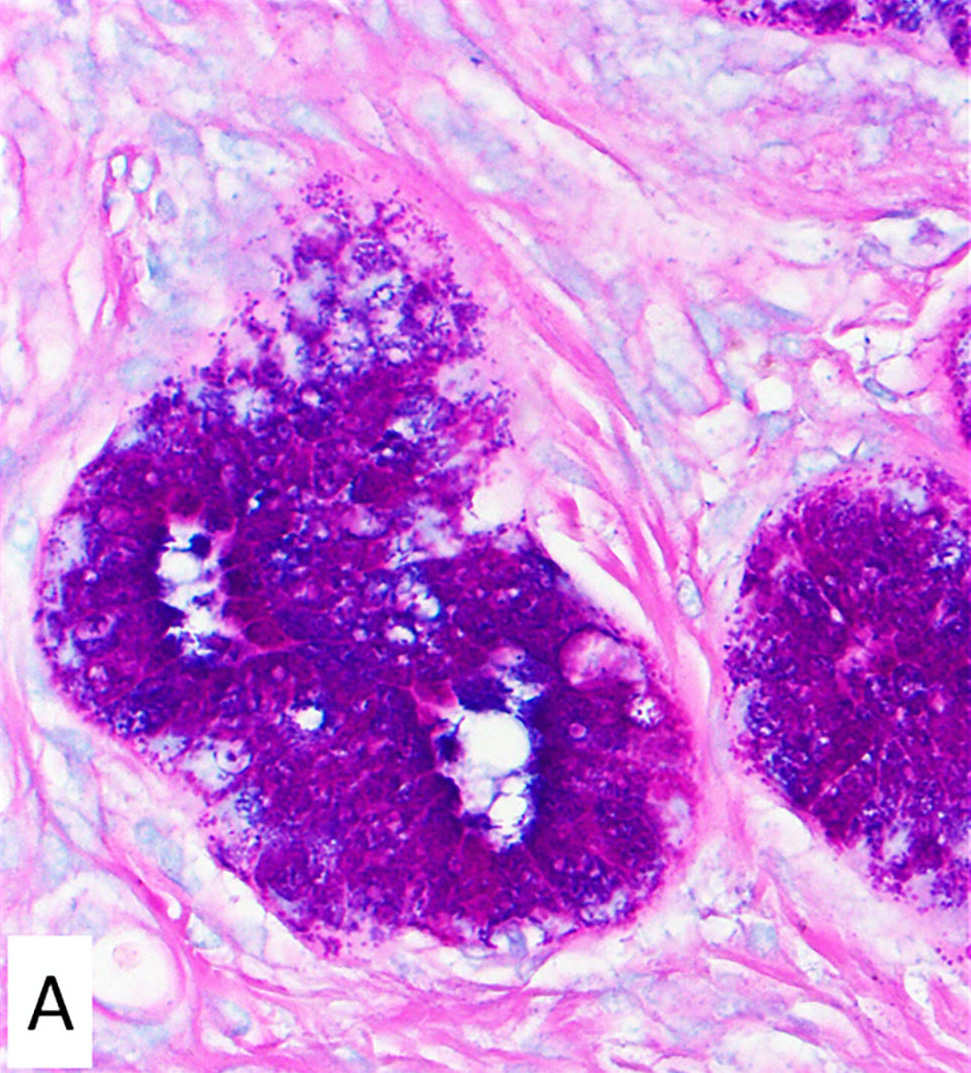
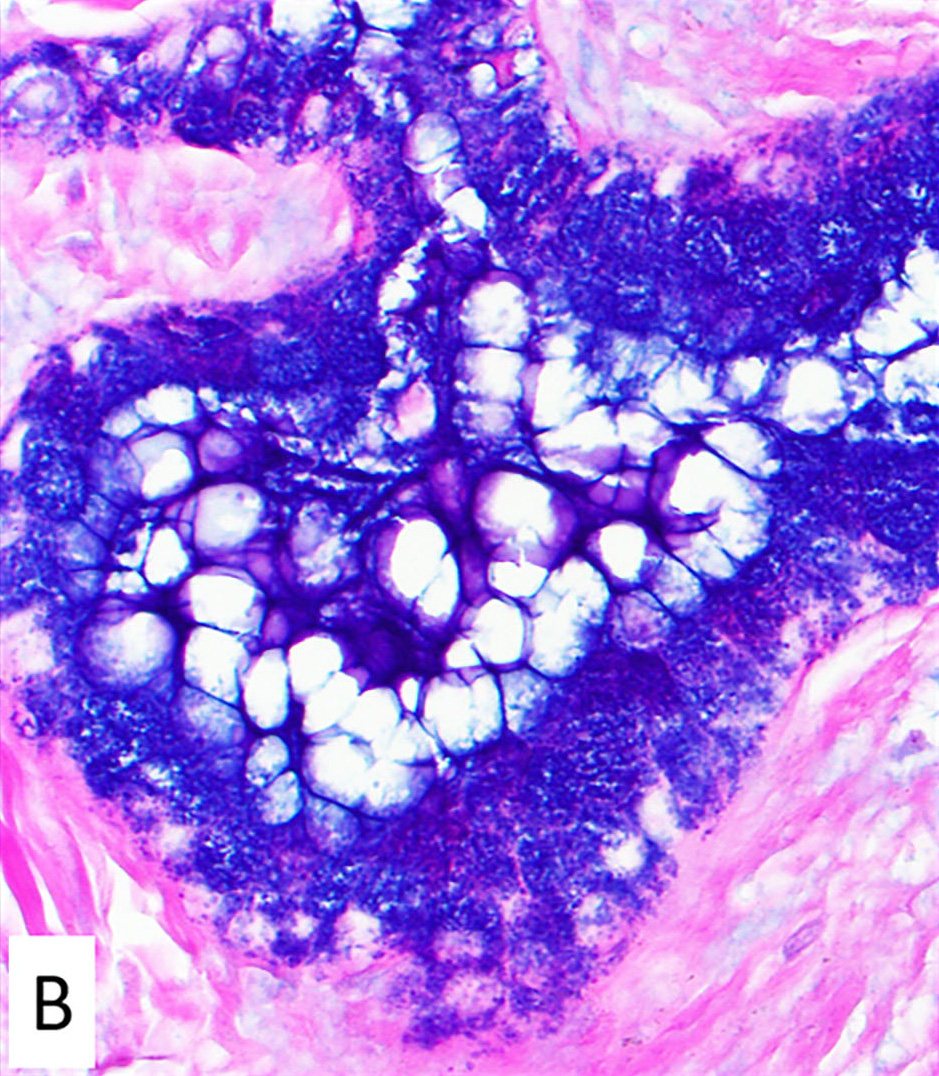
PAS - Alcian blue stain
Contributed by @MirunaPopescu13 on Twitter
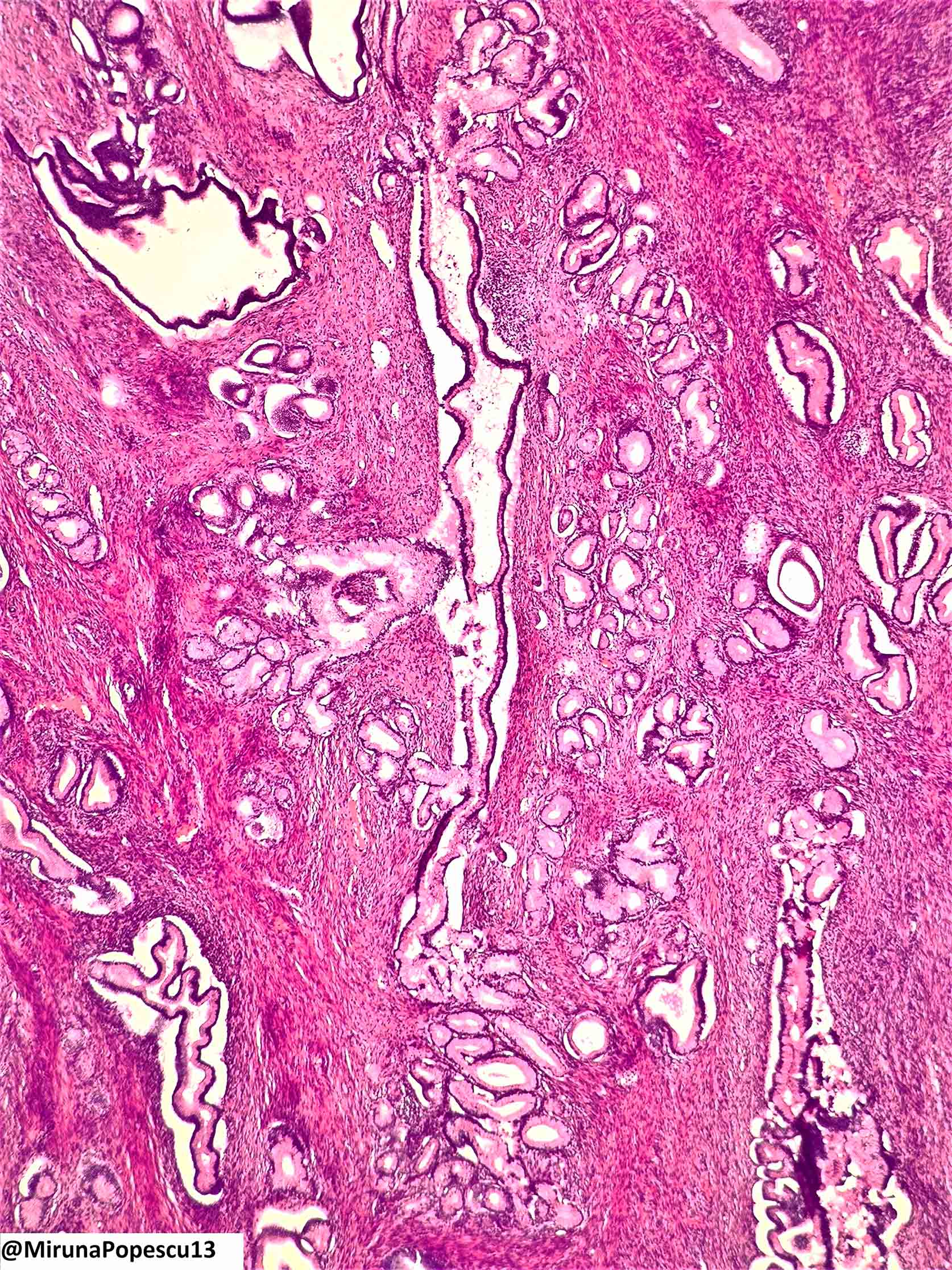
Lobular endocervical glandular hyperplasia
Cytology description
- High columnar mucinous cells with smooth nuclear contours, no atypia and no / rare mitotic figures
- Monolayered sheets, no glandular complexity, no loss of polarity
- Extracellular or intracellular golden yellow mucin on Papanicolaou stain, reflecting gastric type differentiation (Diagn Cytopathol 2002;27:80)
- Intranuclear cytoplasmic inclusions usually are present; less likely in MDA (Diagn Cytopathol 2008;36:535)
- PAS shows neutral mucin filling entire cytoplasm
- Apical localization of neutral mucin is a feature suggestive of atypical LEGH or invasive adenocarcinoma (Diagn Cytopathol 2017;45:842, Acta Cytol 2020;64:556)
Cytology images
Images hosted on other servers:

LEGH and MDA
Positive stains
- Pale red or magenta cytoplasmic staining in PAS - Alcian blue stain (stains neutral mucin; in contrast, endocervical type mucin is acid type and will stain dark blue / purple) (Histopathology 2007;50:843)
- A neutral mucin profile has 63% sensitivity and 84% specificity in distinguishing gastric type from nongastric type adenocarcinomas (Am J Surg Pathol 2007;31:664)
- Pyloric gland mucin (HIK1083)
- MUC6 (sensitive but not specific for gastric type neoplasia) (Histopathology 2019;75:552)
- PAX2 (retained nuclear staining, normal result)
- Chromogranin A in scattered neuroendocrine cells (absent in nongastric type lesions) (Mod Pathol 2004;17:962)
- Atypical LEGH has elevated Ki67 index (between 1% and 10%) and abnormal p53 expression (in a subset of cases, 22%) (Histopathology 2009;55:362, Am J Surg Pathol 2017;41:1023)
Negative stains
- CEA (may be weakly positive in apical cytoplasm only)
- ER / PR (absence of staining)
- p16 (absent or patchy staining)
- HPV in situ hybridization
- References: Histopathology 2001;39:364, Histopathology 2005;46:130
Molecular / cytogenetics description
- Up to 58% harbor mutually exclusive mutations in GNAS, STK11 or KRAS (8, 2, and 1 out of 19, respectively) (Am J Surg Pathol 2014;38:370)
- Some reports suggest acquisition of STK11 mutations may allow progression from LEGH to MDA (Virchows Arch 2013;462:645)
- Whole exome sequencing in 3 cases of pure LEGH demonstrated a lack of known carcinogenic mutations, supporting a hypothesis of metaplasia (Oncol Lett 2019;18:2592)
- Driver mutations may therefore only occur in late lesions (i.e., atypical or MDA associated LEGH)
- Atypical LEGH shares molecular alterations with MDA, including 3q gain and 1p loss (Mod Pathol 2004;17:962)
- HPV negative (Int J Gynecol Pathol 2005;24:296)
Sample pathology report
- Uterus, hysterectomy:
- Cervix with lobular endocervical glandular hyperplasia
- Cervix, loop electrosurgical excision:
- Lobular endocervical glandular hyperplasia (see comment)
- Comment: Lesion appears completely excised; margins are negative.
- Cervix, biopsy:
- Gastric type glandular proliferation, favor lobular endocervical glandular hyperplasia (see comment)
- Comment: The epithelial proliferation has a lobular configuration. The epithelial cells have a gastric phenotype, which includes tall pale to foamy mucinous cytoplasm, as well as neutral type mucin on PAS - Alcian blue stain, positive HIK1083 and negative ER / PR. PAX2 is normal (retained). By itself, LEGH is considered benign but it is associated with other gastric type proliferations in the cervix, including gastric type adenocarcinoma. Consideration for excisional sampling or at least close monitoring and imaging to exclude the presence of a cervical mass is recommended.
Differential diagnosis
- HPV independent endocervical adenocarcinoma, gastric type:
- Haphazard distribution with deep invasion, desmoplastic stromal response, malignant cytologic features
- These can be subtle or focal in highly differentiated cases, so called minimal deviation type
- PAX2 is lost (abnormal expression); p53 can be abnormal (mutant type) (Pathol Int 2005;55:412, Am J Surg Pathol 2010;34:137, Am J Surg Pathol 2011;35:633)
- Haphazard distribution with deep invasion, desmoplastic stromal response, malignant cytologic features
- Gastric type adenocarcinoma in situ:
- Can be lobular (namely, atypical LEGH) or not
- Architectural and cytologic atypia in the form of papillary or cribriform intraglandular growth, nuclear enlargement, loss of polarity, prominent nucleoli (Pathology 2018;50:122)
- Pyloric type metaplasia:
- Simple, bland epithelium in the surface or in normal appearing endocervical crypts
- Lack of lobular glandular architecture
- Tunnel clusters (type A):
- Low cuboidal epithelium with an involutional appearance that may show gastric differentiation
- Often admixed with type B clusters that are dilated with flattened epithelium and mucinous secretions
- Mesonephric remnants / hyperplasia:
- Can have a lobulated pattern (most forms of hyperplasia, however, are of the diffuse type)
- Cuboidal epithelium with mucin free cytoplasm and eosinophilic hyaline material within lumina
- GATA3+
- Microglandular hyperplasia:
- Tightly packed glands with little intervening stroma
- Squamous metaplasia and acute inflammation
- Subnuclear vacuoles
Additional references
Board review style question #1
A 40 year old woman presents with watery vaginal discharge and is found to have a multicystic, cervical lesion on MRI. The lesion (shown above) displays well defined lobules of endocervical glands lined by columnar cells with eosinophilic cytoplasm and small, bland nuclei. Immunostain for HIK1083 and MUC6 is positive. PAS staining shows pale red cytoplasm in lesional cells. Desmoplastic response is not seen. Which of the following distinguishes this lesion from gastric type endocervical adenocarcinoma?
- Absence of haphazard growth
- HIK1038 / MUC6 positivity
- Lack of association with high risk HPV infection
- Pale red cytoplasmic staining on PAS
Board review style answer #1
A. Absence of haphazard growth. Like lobular endocervical glandular hyperplasia (LEGH), very well differentiated forms of gastric type endocervical adenocarcinoma (formerly known as minimal deviation endocervical adenocarcinoma) are characterized by well differentiated endocervical glands that express gastric type mucin, which stains pale red (neutral) on PAS and is positive for HIK1083 and MUC6. Diagnosis of malignancy is reached when glands with the previously described features infiltrate the cervical stroma haphazardly, unlike LEGH, which has a distinct floret-like lobulated configuration. Haphazard growth in adenocarcinoma is often associated with at least focal desmoplastic response and cytologic atypia. None of the glandular lesions with gastric type differentiation of the cervix are associated with HPV infection.
Comment Here
Reference: Lobular endocervical glandular hyperplasia
Comment Here
Reference: Lobular endocervical glandular hyperplasia

