
Cervix
Other epithelial tumors
Adenosquamous carcinoma
Last author update: 3 December 2007
Last staff update: 28 February 2023
Copyright: 2007-2025, PathologyOutlines.com, Inc.
PubMed Search: Adenosquamous carcinoma cervix




Table of Contents
Definition / general | Epidemiology | Pathophysiology | Etiology | Clinical features | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Differential diagnosis | Additional referencesCite this page: Perunovic B., Sunassee A, Askeland R. Adenosquamous carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cervixadenosquamous.html. Accessed March 31st, 2025.
Definition / general
- Carcinoma containing a mixture of glandular and squamous components
- ~10% of cervical carcinomas (Virchows Arch 2009;455:253)
- Glassy cell carcinoma is a rare variant of poorly differentiated adenosquamous carcinoma; aggressive subtype with rapid growth, early metastases and poor prognosis (Cytojournal 2013;10:17, Eur J Obstet Gynecol Reprod Biol 2014;179:232)
Epidemiology
- Glassy cell carcinoma:
- Younger age group (mean 41 years), associated with pregnancy, HPV 16 and 18 in tumor cells (Cytojournal 2013;10:17)
- Peak incidence third to fourth decades (Cytojournal 2013;10:17)
- Some studies have noted an association with pregnancy
Pathophysiology
- Glassy cell carcinoma:
- The presence of HPV 18 might stimulate biphasic squamous and glandular differentiation (Int J Gynecol Pathol 2002;21:134)
- Cytokeratin expression is similar to that of reserve cells or immature squamous cells of cervix (Int J Gynecol Pathol 2002;21:134)
Etiology
- May arise from subcolumnar reserve cells in basal layer of endocervix
- More common during pregnancy
- Associated with HPV18 (Virchows Arch 2009;455:253, Int J Gynecol Pathol 2012;31:294)
- Frequent loss of ARID1A protein expression (Int J Gynecol Cancer 2012;22:208)
Clinical features
- Same prognosis as other cervical carcinomas when stratified by grade and stage but most cases are high grade
- Glassy cell carcinoma:
- 1 - 2% of cervical carcinomas
- Historically considered more aggressive with poorer prognosis than ordinary adenosquamous carcinoma or adenocarcinoma, although recent studies show less or no difference (APMIS Suppl 1991;23:119, Am J Obstet Gynecol 2004;190:67)
- May have peripheral blood eosinophilia
Prognostic factors
- Glassy cell carcinoma has poor prognostic factors
- Angiolymphatic invasion, deep stromal invasion, large tumor size
- HER2 overexpression may correlate with more aggressive behavior and worse clinical outcome (Acta Cytol 2006;50:418)
Case reports
- 27 year old woman with stage IB2 tumor diagnosed at 19 weeks gestation (Aust N Z J Obstet Gynaecol 2015;55:94)
- 29 year old woman with signet ring cell carcinoma (Pathol Int 2004;54:787)
- 33 year old woman with history of post coital bleeding and vaginal discharge (UPMC Case #100)
- 44 year old and 67 year old women (Ceska Gynekol 1999;64:279, Ginekol Pol 2011;82:936)
- 72 year old woman with endometrial extension of cervical tumor (Int J Gynecol Cancer 2004;14:625)
- Metastasis to infusion port site (Gynecol Oncol 1999;74:130)
- Patient with myometrial recurrence during pregnancy (Gynecol Oncol 2000;76:409)
- Patient with metastasis to port site (Gynecol Oncol 1999;74:130)
Treatment
- Radical hysterectomy and chemoradiation
- Cisplatin based chemoradiation: overall survival now comparable to squamous cell carcinoma of cervix, although historically poorer prognosis
- Poorer prognosis with radiation alone (Gynecol Oncol 2014;135:208, Gynecol Oncol 2014;135:462)
Gross description
- Glassy cell carcinoma: bulky exophytic mass with barrel shape cervix (Cytojournal 2013;10:17)
Gross images
AFIP images
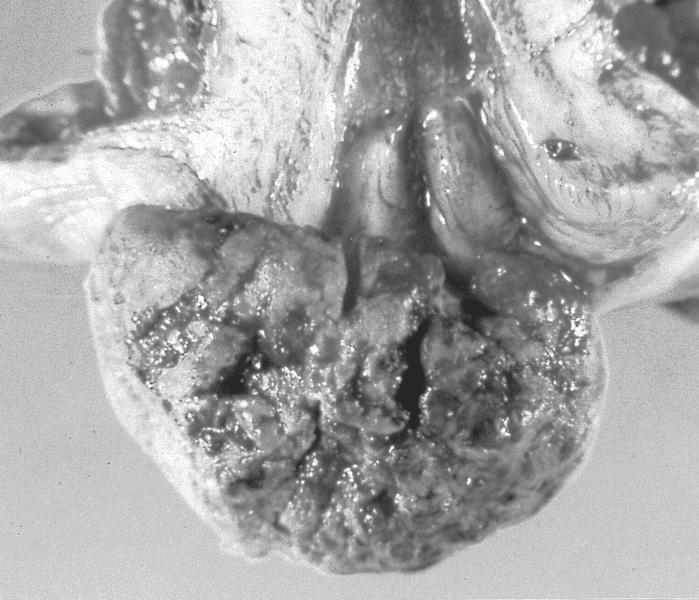
Bulky exophytic mass
Microscopic (histologic) description
- Usually defined as biphasic pattern of well defined malignant glandular and squamous components clearly identifiable without special stains
- Glandular component usually endocervical and poorly differentiated with cytoplasmic vacuoles or luminal mucin
- Squamous component also is poorly differentiated
- If endometrioid call endometrioid carcinoma with squamous differentiation
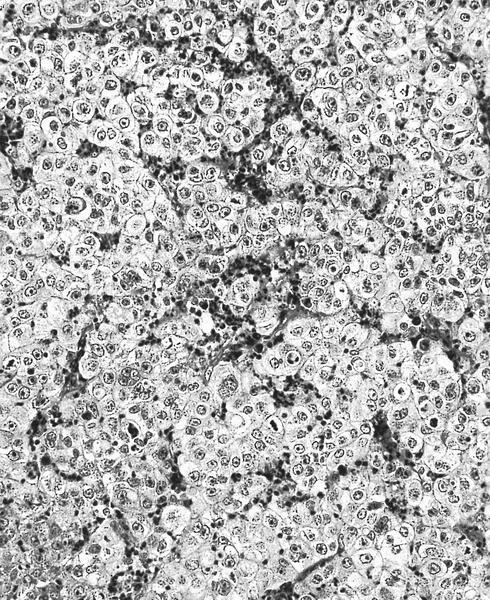
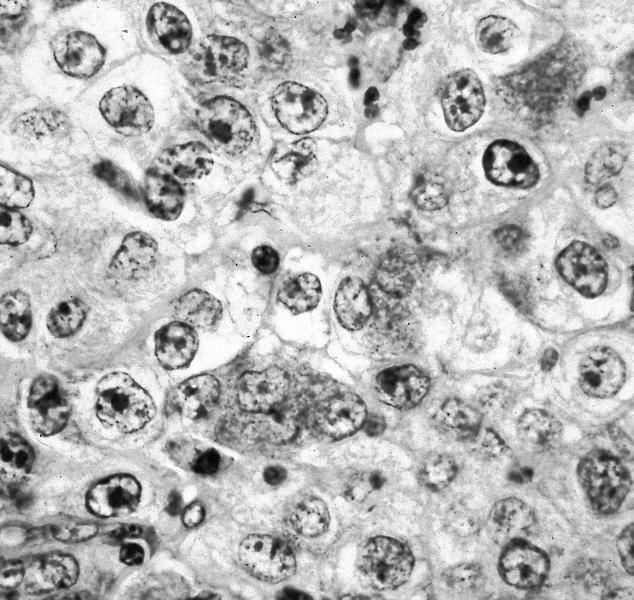
- Glassy cell carcinoma:
- Solid nests of markedly pleomorphic, polygonal tumor cells with prominent cell membrane, glassy and eosinophilic cytoplasm, large eosinophilic nuclei, prominent nucleoli, surrounded by heavy inflammatory infiltrate containing eosinophils
- Frequent mitotic figures
- Pure cases have no histologic evidence of glandular or squamous differentiation (i.e. no intracellular bridges, no dyskeratosis, no intracellular glycogen), which is detectable only by electron microscopy
- Often less invasion than is suspected
Microscopic (histologic) images
AFIP images
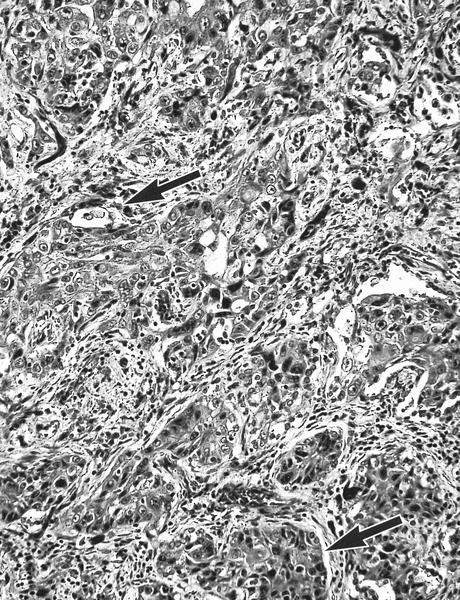
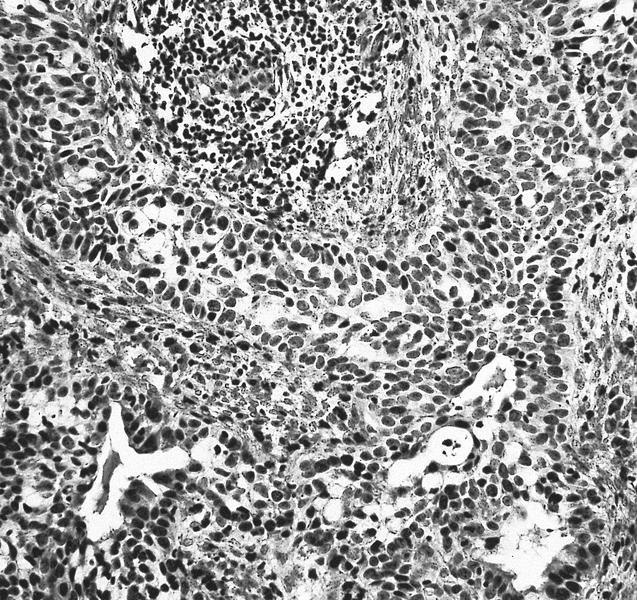
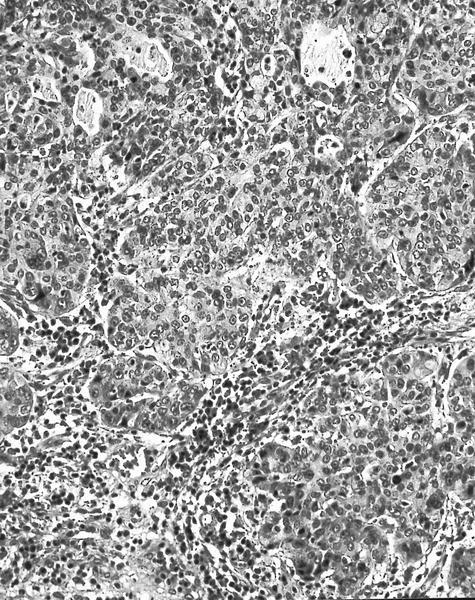
Poorly formed glands and squamous components
Sheets of cells with abundant lightly stained cytoplasm
Distinct cell border and prominent nucleoli
Cytology description
- Often not diagnosed on pap smear (Cancer Cytopathology 2004;102:210)
- Papillary subtype (thin layer cytology):
- High cellularity
- Multiple small, papillary clusters of basaloid to columnar cells
- Discernible fibrovascular cores
- Background of loosely dispersed bland looking columnar cells and high grade squamous intraepithelial lesion
- Scattered adenocarcinoma cells containing intracytoplasmic vacuoles (Acta Cytol 2003;47:649)
- Glassy cell carcinoma:
- Tumor cells arranged in sheets or clusters
- Distinct cell borders with moderate to abundant finely granular (ground glass-like) cytoplasm
- Large round/oval vesicular nuclei with one or more prominent nucleoli
- Chromatin varies from finely dispersed to coarse and irregular (Acta Cytol 2004;48:99, Zhonghua Bing Li Xue Za Zhi 2011;40:523)
- Cytoplasmic vacuolization and bizarre cells with multinucleation may be seen (Acta Cytol 2001;45:407)
- Mitotic figures frequently seen
- Background inflammatory infiltrate including frequent eosinophils, neutrophils, plasma cells, lymphocytes and necrotic debris
- Focal abortive keratin production; squamous or glandular differentiation may be present
- Focal clear cell differentiation may be present
Cytology images
Images hosted on other servers:

Abundant granular cytoplasm
Positive stains
- p63 (squamous component), CK7
- Glassy cell carcinoma:
- MUC1 / EMA, MUC2, CEA (focal), CAM5.2, p63 (Zhonghua Bing Li Xue Za Zhi 2011;40:523)
- PAS+ cell wall
- Vimentin
- Focal mucin
Electron microscopy description
- Glandular features include mucous secretory vacuoles, true lumen formation and scattered glycogen
- Tonofilaments and secretory products
- Note: most undifferentiated cervical carcinomas have ultrastructural features of squamous or glandular differentiation
- Glassy cell carcinoma:
- Glassy features may be due to cytoplasmic polyribosomes, abundant tonofilaments and abundant dilated rough endoplasmic reticulum (Am J Clin Pathol 1991;96:520)
- Adenosquamous features include well developed desmosomal complexes and microvilli
- Occasional intracellular lumina (Cancer 1983;51:2255)
Differential diagnosis
- Adenocarcinoma with coexisting SIL:
- Usually no mixing of tumor elements
- Adenoid basal carcinoma (Pathol Int 2005;55:445)
- Extension of endometrial adenocarcinoma:
- Bulk of tumor is in endometrium
- Squamous cell carcinoma with focal mucin droplets
- Large cell nonkeratinizing squamous cell carcinoma:
- Cell membrane is less well defined, cytoplasm is less finely granular, coarser chromatin distributed along nuclear membrane
- Also poor staining or fixation makes it resemble glassy cell carcinoma
- Lymphoepithelioma-like carcinoma (Acta Cytol 1999;43:285)
Additional references
