
Breast
Ductal carcinoma in situ
Paget disease


Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Paget disease [TI] breast pathology
- Mammary Paget disease (MPD) is a proliferation of malignant glandular epithelial cells (in situ carcinoma) in the nipple areolar epidermis (Histopathology 2020;77:181)
- Disease is named after the pathologist and surgeon Sir James Paget, who published his findings of a relationship between a nipple rash and mammary gland tumors in 1874 (JAMA Dermatol 2018;154:335)
- Uncommon clinical presentation of breast cancer
- Most often presents as an eczematous / erythematous change of the nipple areolar skin
- Cutaneous manifestation is due to tumor cells involving the epidermis and disrupting intercellular junctions
- Underlying high grade ductal carcinoma in situ (DCIS) or invasive carcinoma is present in > 95% of patients
- Majority of Paget cells and associated underlying carcinoma are HER2+
- Mammary Paget disease
- Paget disease of the breast
- Paget disease of the nipple
- DCIS involving nipple skin
- Paget disease with dermal invasion occurs when Paget cells cross the basement membrane of the epidermis; the invasive component is usually small in size (Arch Pathol Lab Med 2013;137:72)
- Secondary Paget disease occurs when invasive carcinoma arising deep in the breast invades the skin; the invasive carcinoma is usually large in size
- ICD-O: 8540/3 - Paget disease of breast
- ICD-10: C50.019 - malignant neoplasm of nipple and areola, unspecified female breast
- ICD-11: 2E65.5 & XH3E21 - Paget disease of nipple and Paget disease, mammary
- Relatively uncommon; occurs in 1 - 4% of women and 1 - 2% of men with breast cancer (Breast Cancer Res Treat 2008;111:313)
- Wide age range of 20 - 90 years, with a peak incidence between sixth and seventh decade (mean: 64 years) (Breast Dis 2020;39:119)
- Between 20 - 30% of patients are premenopausal
- Histologic (subclinical) evidence of MPD may be more frequent
- Affects the nipple or areola region and may extend into the adjacent breast skin
- Lesions are almost always unilateral and rarely bilateral (Breast J 2005;11:355)
- May occur in supernumerary nipples (J Cutan Pathol 1994;21:283)
- 2 theories on the pathogenesis:
- Epidermotropic theory (most widely accepted): Paget cells are DCIS cells that migrate along the basement membrane of the nipple, supported by the presence of DCIS deeper in the breast identical to Paget cells in almost all cases; migration may be mediated through a motility factor heregulin α, produced by keratinocytes and exerting its effect via the HER2 receptor (J Natl Cancer Inst 2000;92:622)
- Transformation theory: Paget cells originate from malignant transformation of keratinocytes or Toker cells; it would explain rare cases (< 5%) in which cancer is not present in underlying breast (Intractable Rare Dis Res 2019;8:203)
- When no parenchymal cancer is identified, there is a possibility that the underlying tumor has gone undetected / unsampled
- Specific risk factors beyond those recognized for breast cancer have not been identified
Images hosted on other servers:

Development of Paget disease
- Majority of patients present clinically with slow onset nipple changes (Breast Cancer Res Treat 2008;111:313)
- Most common: nipple erythema, scaling crust, ulceration, eczematoid type rash, pruritus or bleeding
- Less common: bloody nipple discharge, pain, retraction or no clinically identifiable changes of the nipple
- May present as a pigmented macule and can be mistaken for melanoma (Am J Dermatopathol 2009;31:223, Br J Dermatol 2018;178:e143)
- Changes begin at the nipple / areola and may spontaneously regress or continue to progress with extension into the skin of the breast
- Approximately 50% of patients present with an associated palpable mass, usually indicating an underlying invasive carcinoma
- Affected men have similar clinical presentations as women (Am J Dermatopathol 2020;42:981)
- Clinical presentation may be mistaken for skin inflammatory disease or infection, leading to delayed diagnosis
- In symptomatic cases, the diagnosis is primarily clinical and confirmed by histologic examination
- Most commonly used techniques include skin punch or shave biopsy and less often, core needle biopsy; samples are usually small due to concern about the cosmetic appearance of the nipple (Breast J 2019;25:1328, Radiol Med 2021;126:936)
- Nipple scrape cytology can detect tumor cells on the surface of the epidermis or in the scale crust but it may be painful for the patients and is rarely used (Diagn Cytopathol 2019;47:249)
- In addition to nipple biopsy, any underlying masses or mammographic abnormalities must be biopsied, usually by core needle; in patients with a palpable lump, alternatively by fine needle aspiration cytology
- If these methodologies are not definitive for a preoperative diagnosis, an open surgical biopsy / wedge excision may be needed
- In asymptomatic / unsuspected cases, MPD may be an incidental finding in a mastectomy specimen; detecting Paget cells depends on the extent of sampling of the nipple and the use of IHC (Am J Surg 1979;138:135)
- Imaging is mainly used to detect and evaluate the extent of an underlying malignancy and enable appropriate treatment planning (Eur J Radiol 2006;60:256, Radiographics 2011;31:1973)
- Mammography is most useful in detecting masses, distortions or calcifications; however, approximately half of the patients with MPD have normal mammograms
- Ultrasound may show ductal ectasia or changes of the nipple areolar complex, such as flattening, asymmetry and thickening
- Magnetic resonance imaging (MRI) is sensitive, particularly for mammographically occult underlying disease; it may show abnormal nipple enhancement, thickened nipple areolar complex, associated enhancing DCIS or invasive tumor or a combination of these findings (J Am Coll Surg 2008;206:316)
Images hosted on other servers:

Abnormal mammogram

Normal mammogram

Ultrasound

MRI
- Prognosis largely depends on the presence, extent and characteristics of the underlying tumor
- Patients with MPD and DCIS only have excellent outcomes (> 95% survival at 20 years) (Cancer 2006;107:1448)
- Patients with isolated MPD (no parenchymal tumor detected) have even better outcomes; 5 and 10 year survival rates of 100%, compared with those with underlying DCIS of 94.7% and 75.8%, in 1 study (Am Surg 2013;79:1009)
- If invasive carcinoma is present in the underlying breast, prognosis depends on tumor size and lymph node status, with the 5 year relative survival rate declining with increasing tumor stage (stage I, 95.8%; II, 77.7%; III, 46.3%; IV, 14.3%) (Breast Dis 2020;39:119)
- In general, women presenting with MPD and a palpable mass (indicating more advanced disease) have worse survival than women without a palpable mass
- Dermal invasion arising directly from MPD in the epidermis and localized to the nipple (invasive Paget disease) is typically detected early and has a favorable outcome (Arch Pathol Lab Med 2013;137:72, Hum Pathol 2014;45:2480)
- MPD must be distinguished from inflammatory carcinoma and locally advanced invasive carcinoma ulcerating skin, as they have poorer prognoses
- 52 year old woman with Paget disease associated with invasive papillary carcinoma (BMJ Case Rep 2018;2018:bcr2017222817)
- 53 year old woman with bilateral Paget disease derived from lobular carcinoma in situ (LCIS) (Arch Pathol Lab Med 2002;126:90)
- 54 year old woman with recurrence of breast carcinoma as Paget disease of the skin along core biopsy tract (Histopathology 2004;45:416)
- 55 year old man with bilateral metachronous Paget disease of the accessory breasts (J Breast Cancer 2020;23:665)
- 63 year old woman with Paget disease involving breast skin without the involvement of nipple / areola (Pathol Res Pract 2017;213:1454)
- 68 year old woman with invasive Paget disease and axillary lymph node metastases (Int J Surg Pathol 2014;22:566)
- 73 year old woman with bilateral synchronous Paget disease associated with bilateral breast carcinoma (Breast J 2005;11:355)
- 91 year old man with mammary Paget disease (Surg Case Rep 2015;1:103)
- Extent of surgery is determined by the extent of underlying breast carcinoma (Am J Surg 2010;200:241)
- Patients with limited disease are candidates for breast conserving therapy with central lumpectomy and whole breast irradiation (J Surg Res 2019;241:178)
- Those with larger extent of disease (multicentric cancer, diffuse calcifications) undergo simple mastectomy
- Entire nipple areolar complex is removed in all cases; a variety of techniques can be used to reconstruct the nipple
- Evaluation and treatment of the axilla in MPD are the same as for any breast cancer (Am J Surg 2006;192:481)
- Recommendations regarding systemic therapy in neoadjuvant or adjuvant settings are based solely upon any associated invasive carcinoma or DCIS characteristics (Breast Cancer Res Treat 2008;112:513)
Contributed by Jennifer Tseng, M.D. and Mark R. Wick, M.D.

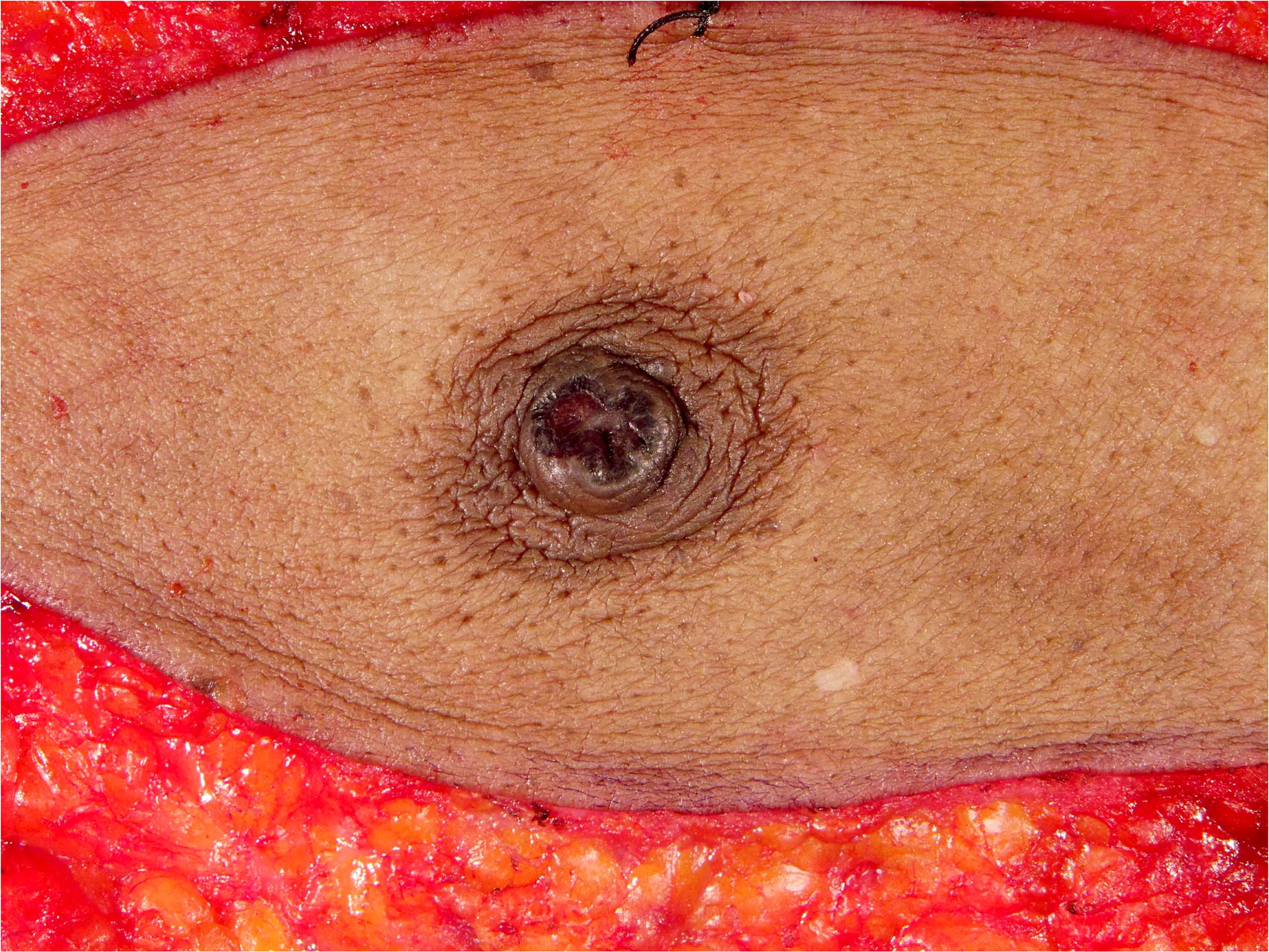
Nipple, crusted lesion

Nipple erosion and erythema
Images hosted on other servers:

Well demarcated, eczematous scaly lesion
- Nipple areolar complex with red-pink crusting lesion, discoloration, thickening, ulceration, exudate, nipple retraction, etc.
- Typically well demarcated; epidermal involvement usually does not extend beyond the grossly evident lesion (Cancer Treat Rev 2001;27:9)
- Scaling crust may be removed by skin preparation prior to surgery
Contributed by Alexis Synder, M.H.S. and Emily S. Reisenbichler, M.D.
Nipple ulceration

Nipple ulceration, enlarged

MPD, cut section with underlying mass
- Frozen section for intraoperative management of Paget disease has been studied more extensively in extramammary sites but not in MPD
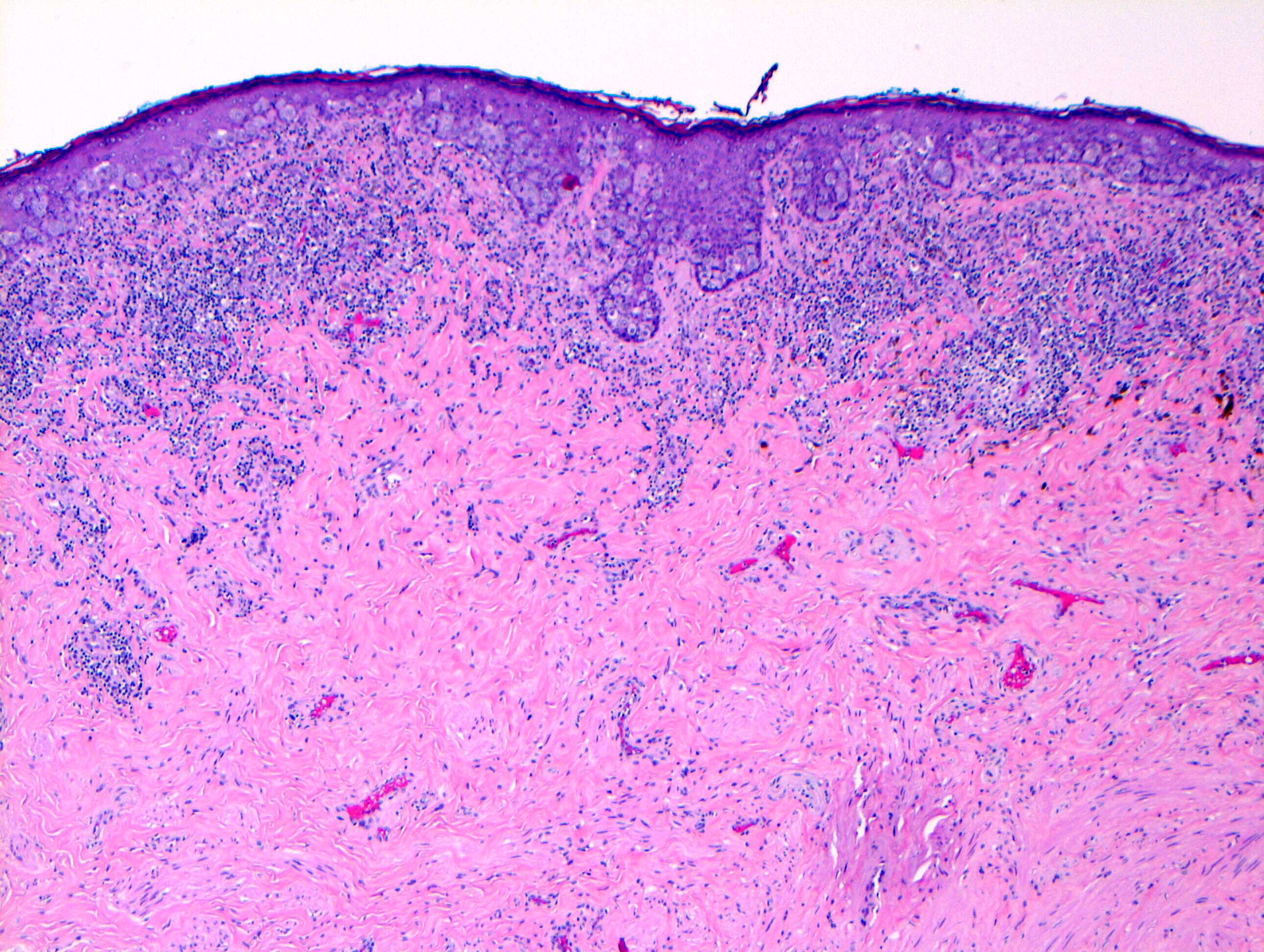
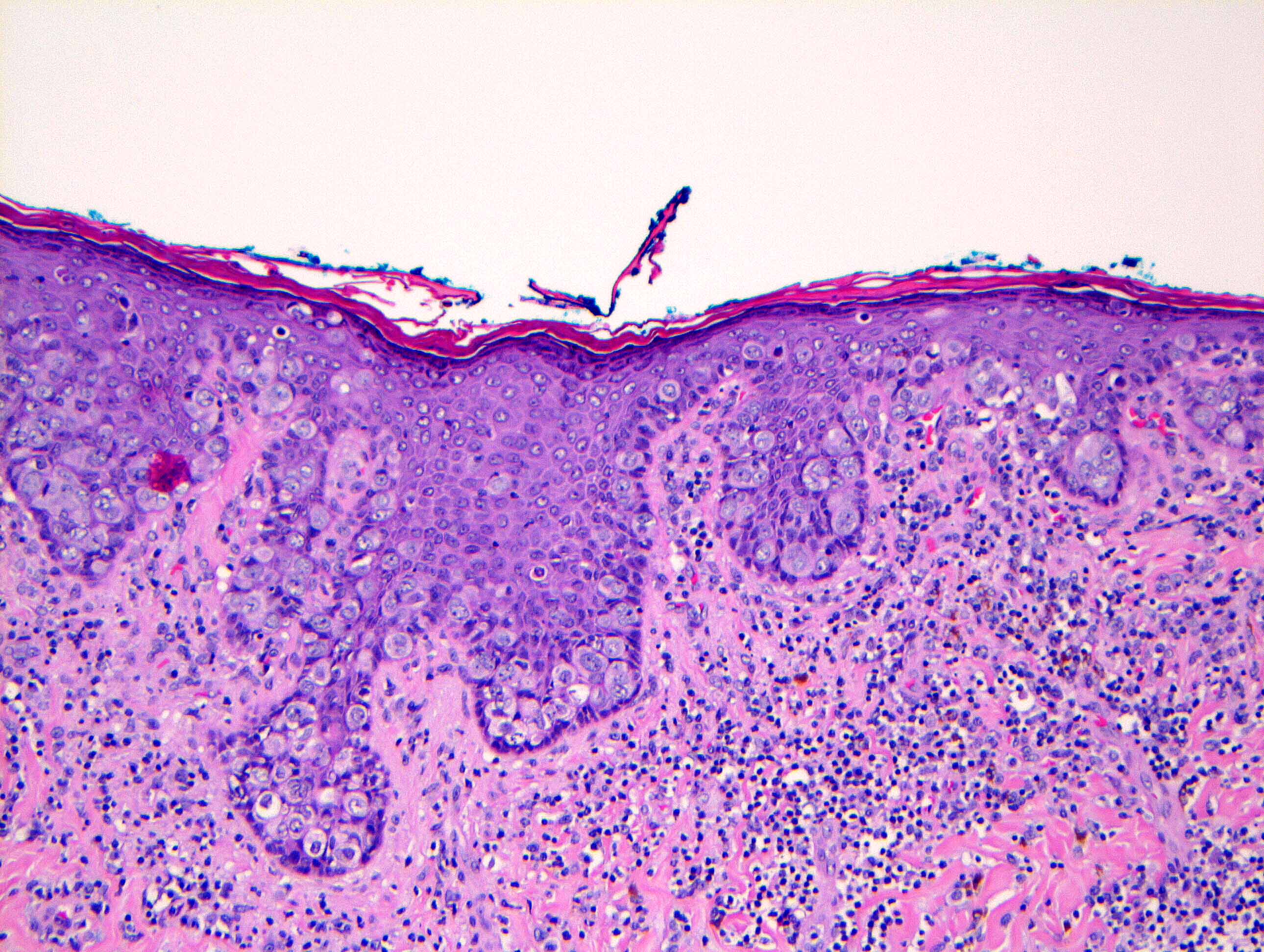
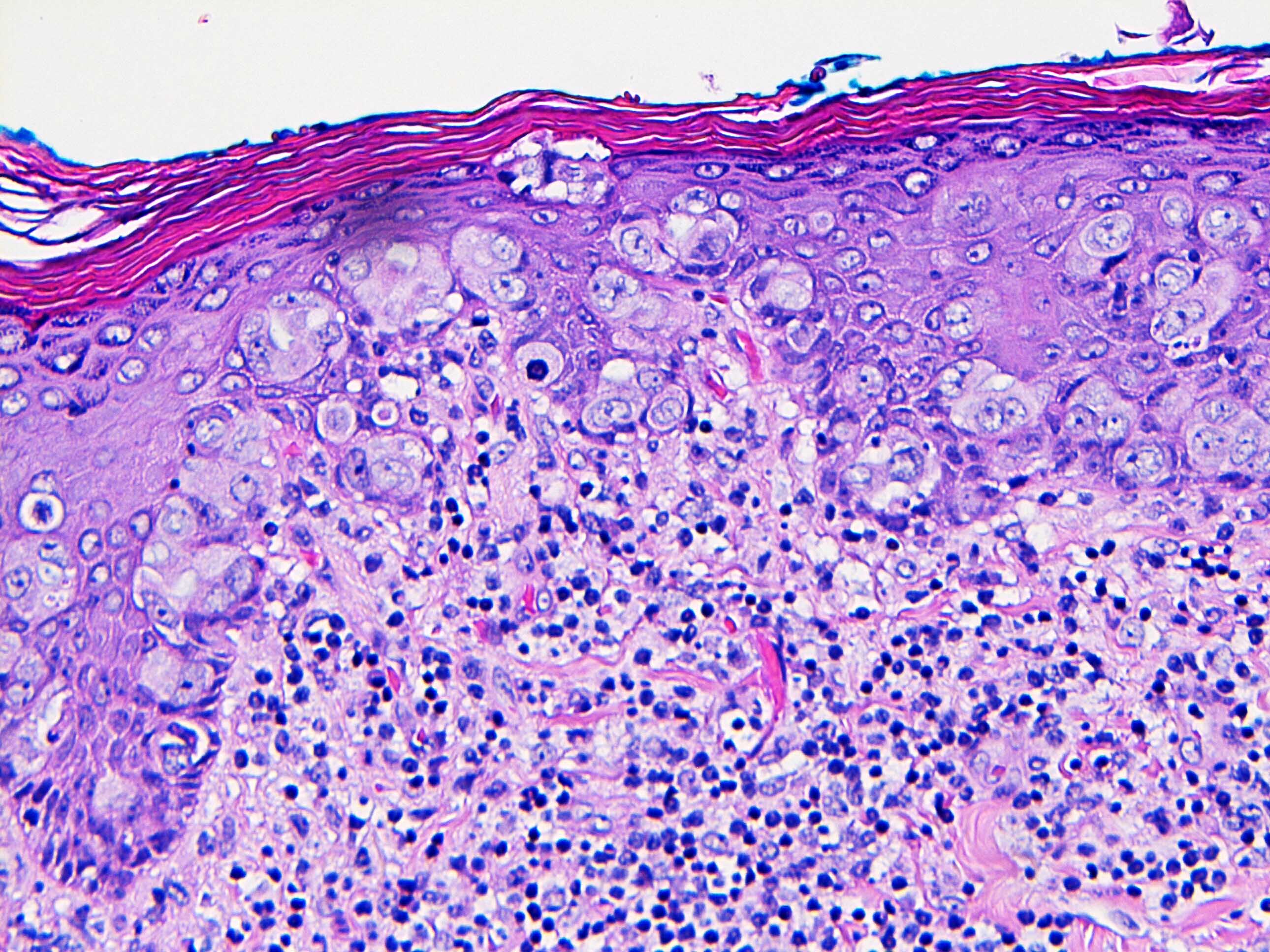
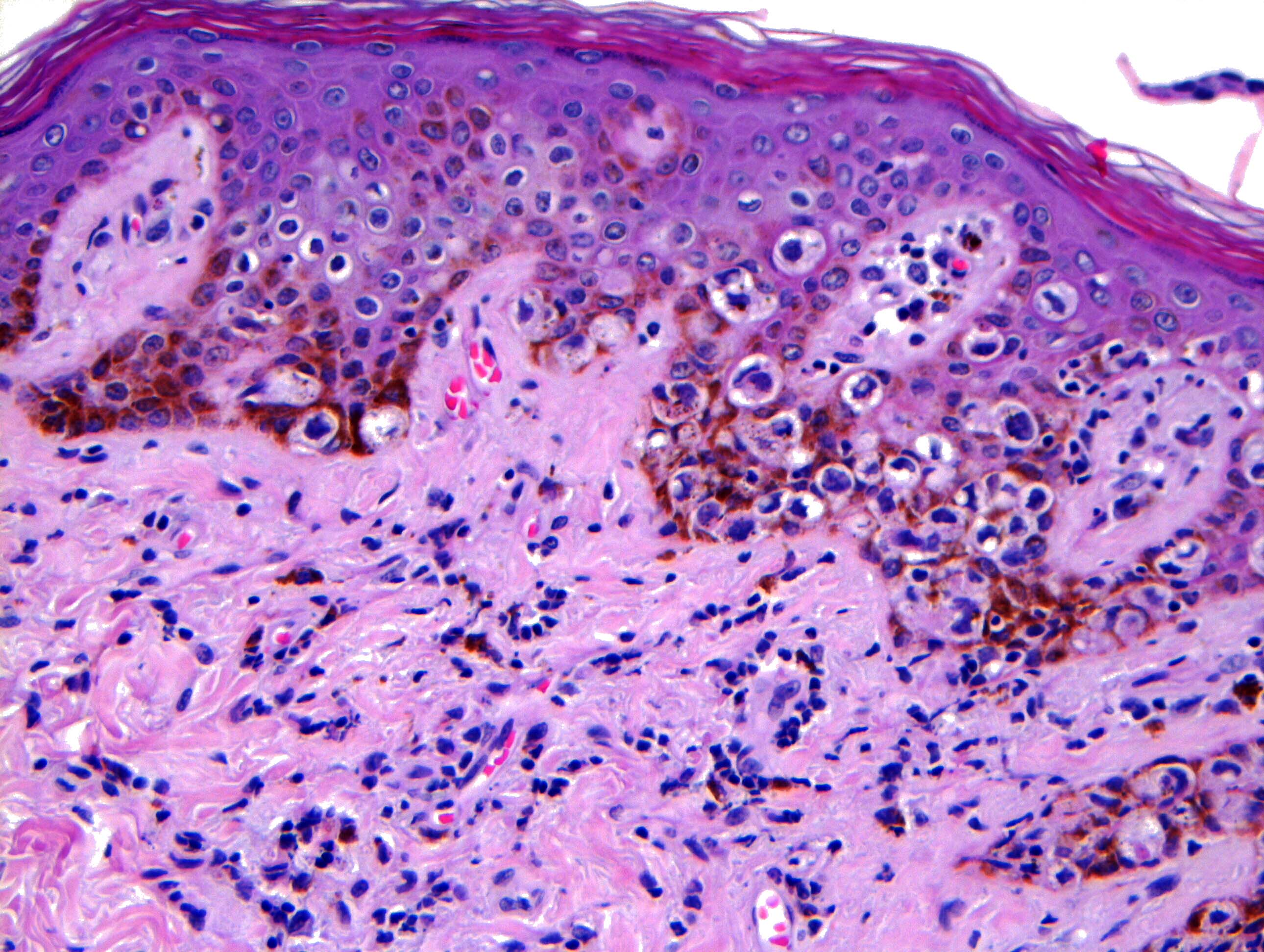
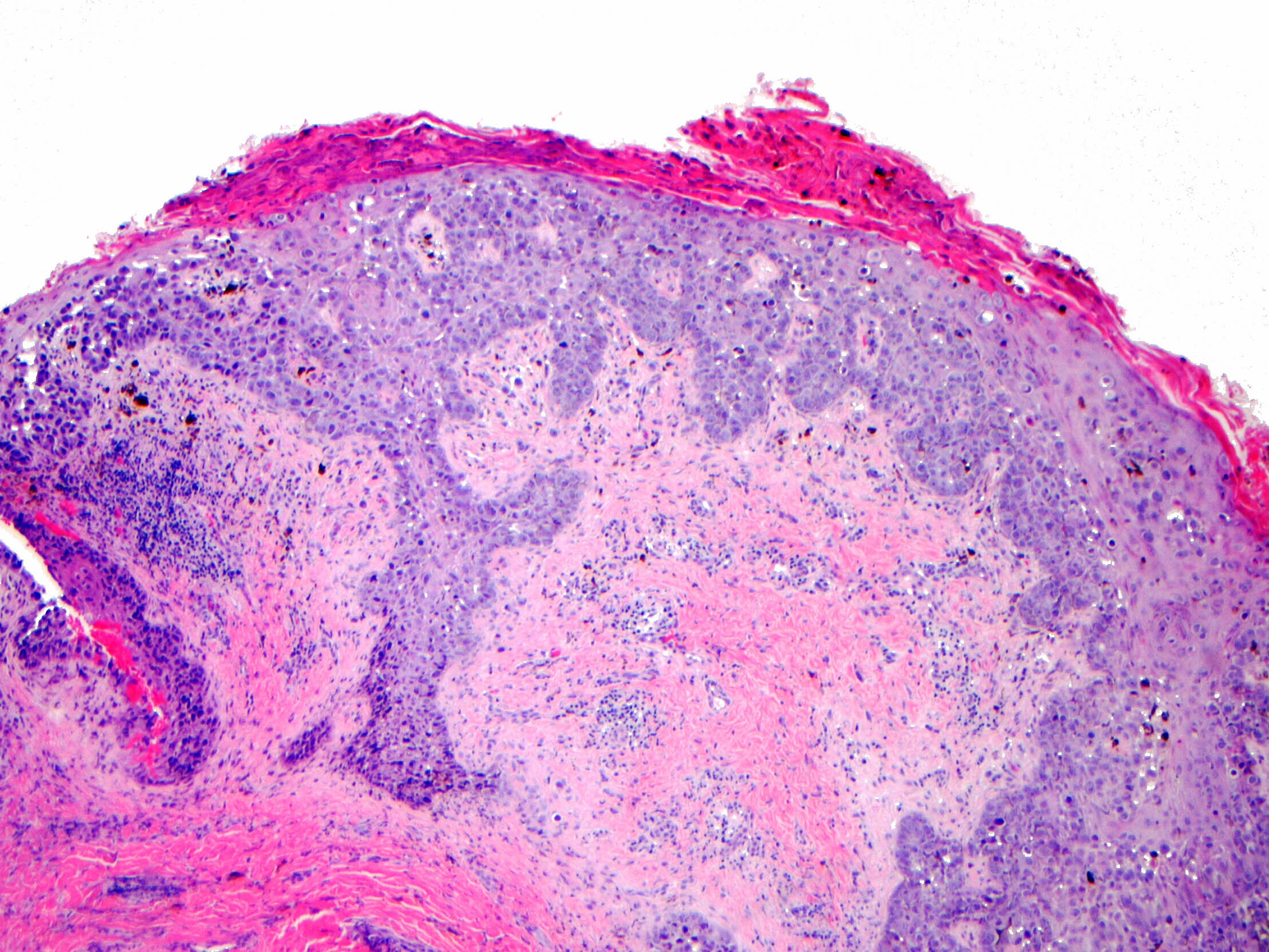
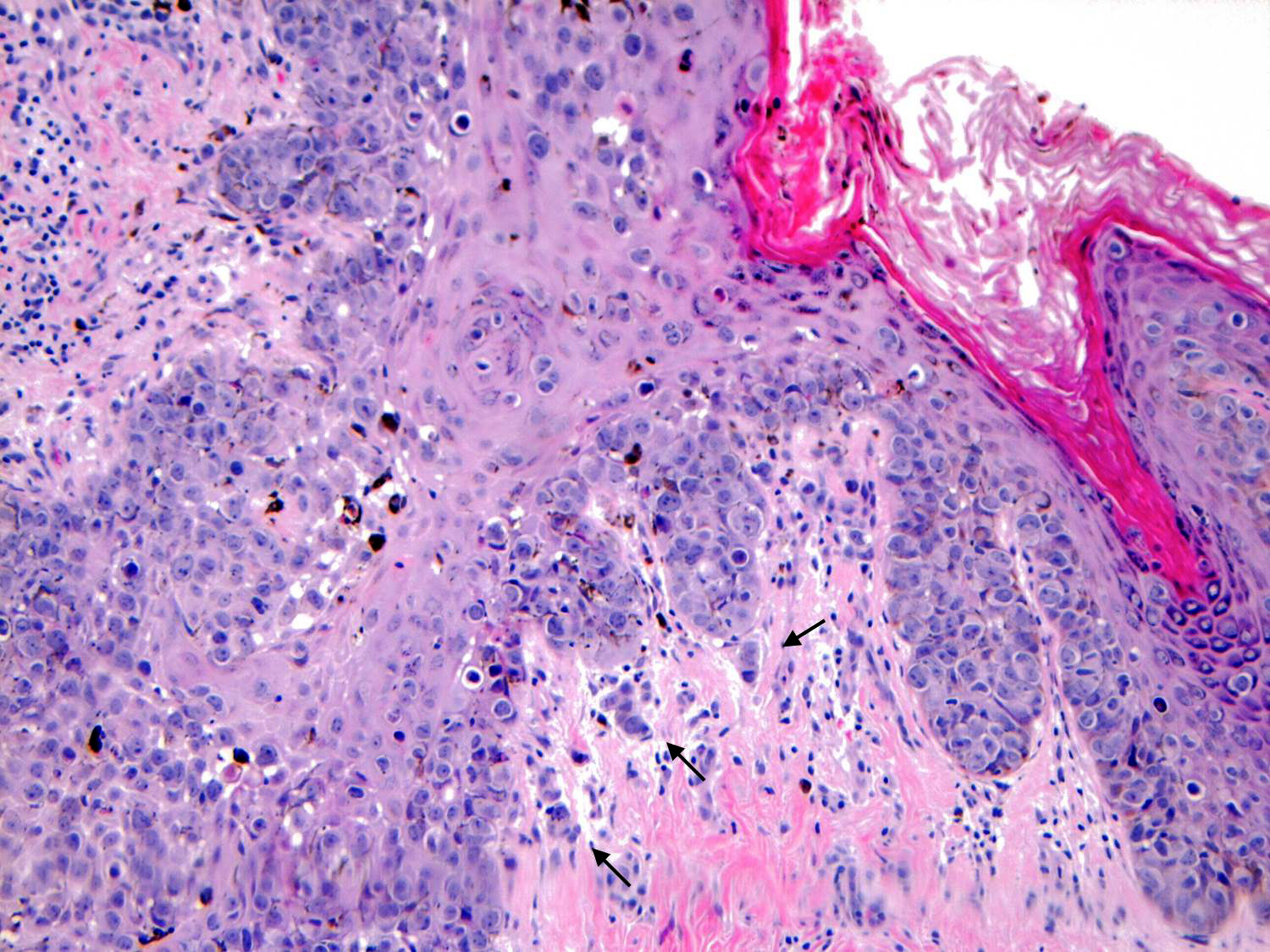
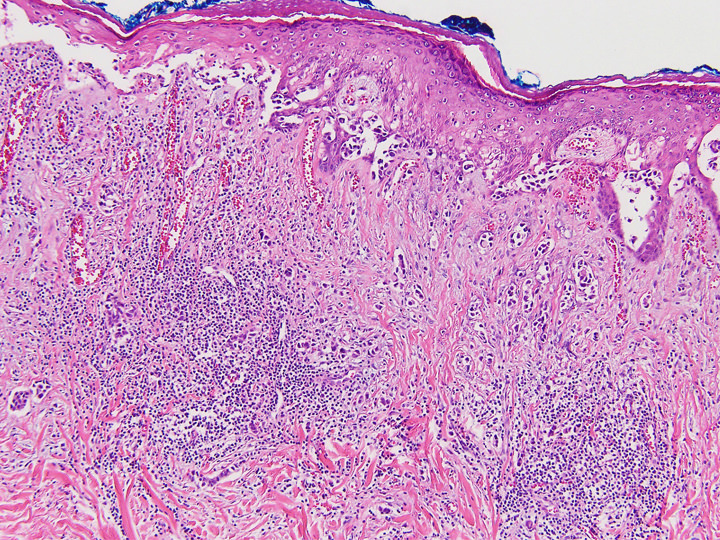
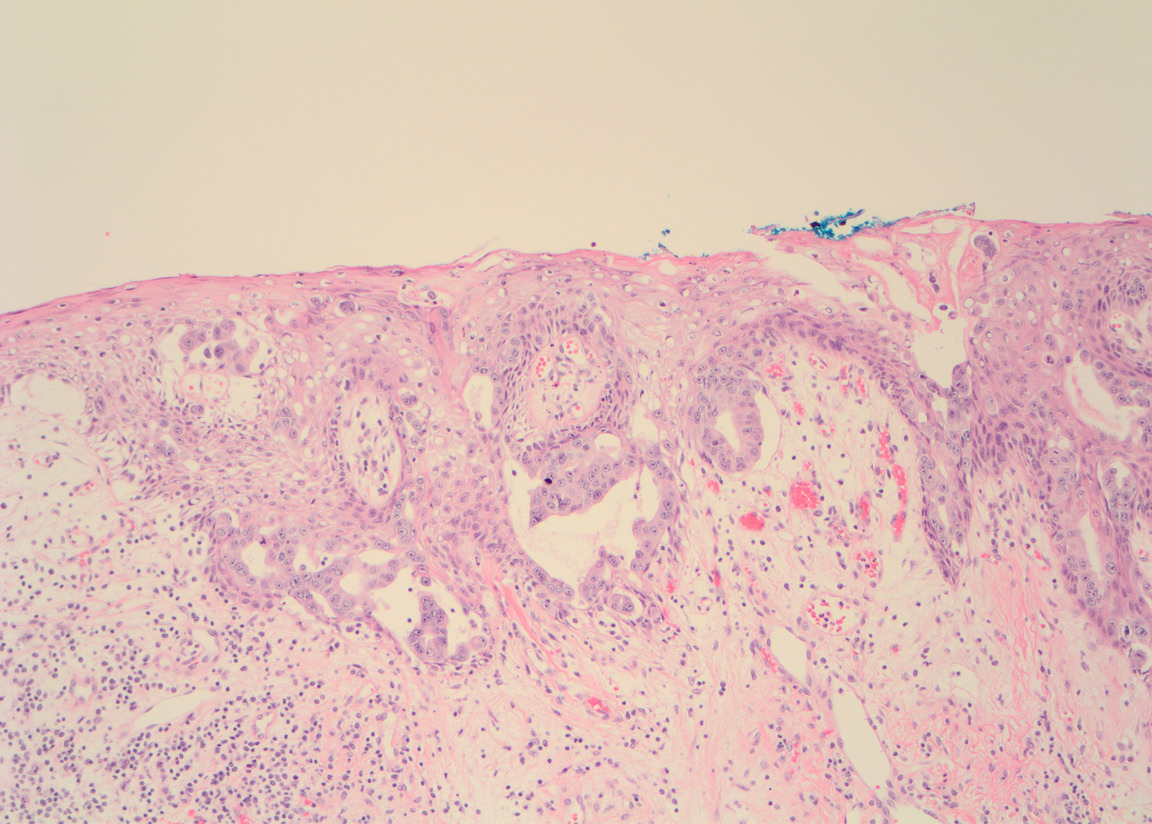
- Single cells or clusters of cells spread throughout the epidermis
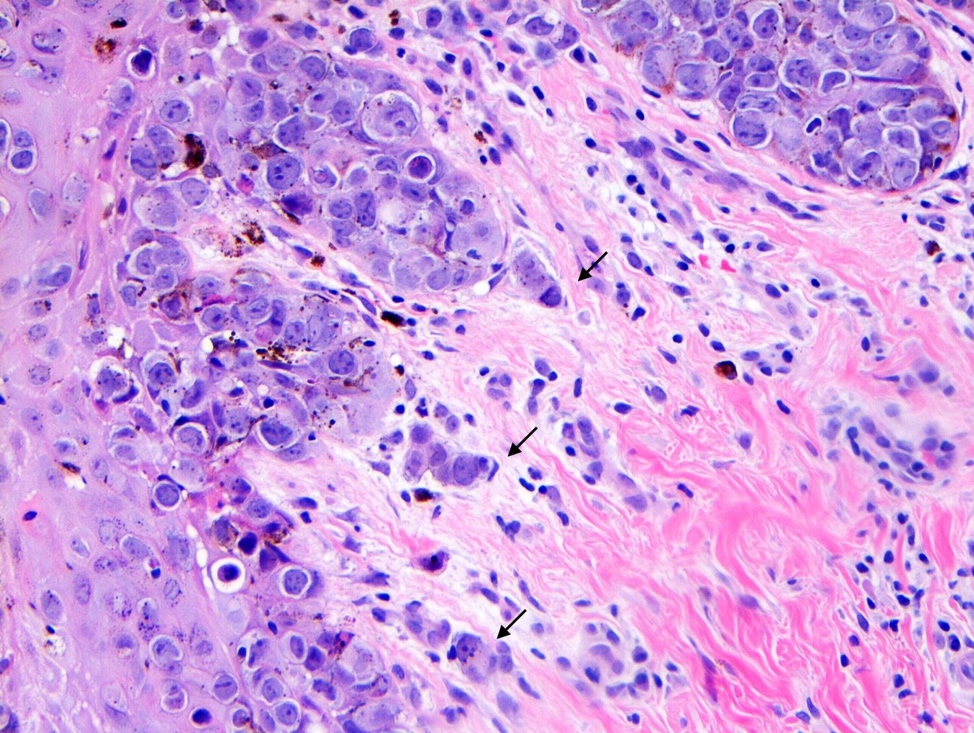
- Cells have abundant pale cytoplasm, large irregular nuclei with prominent nucleoli
- Underlying dermis may have chronic inflammation
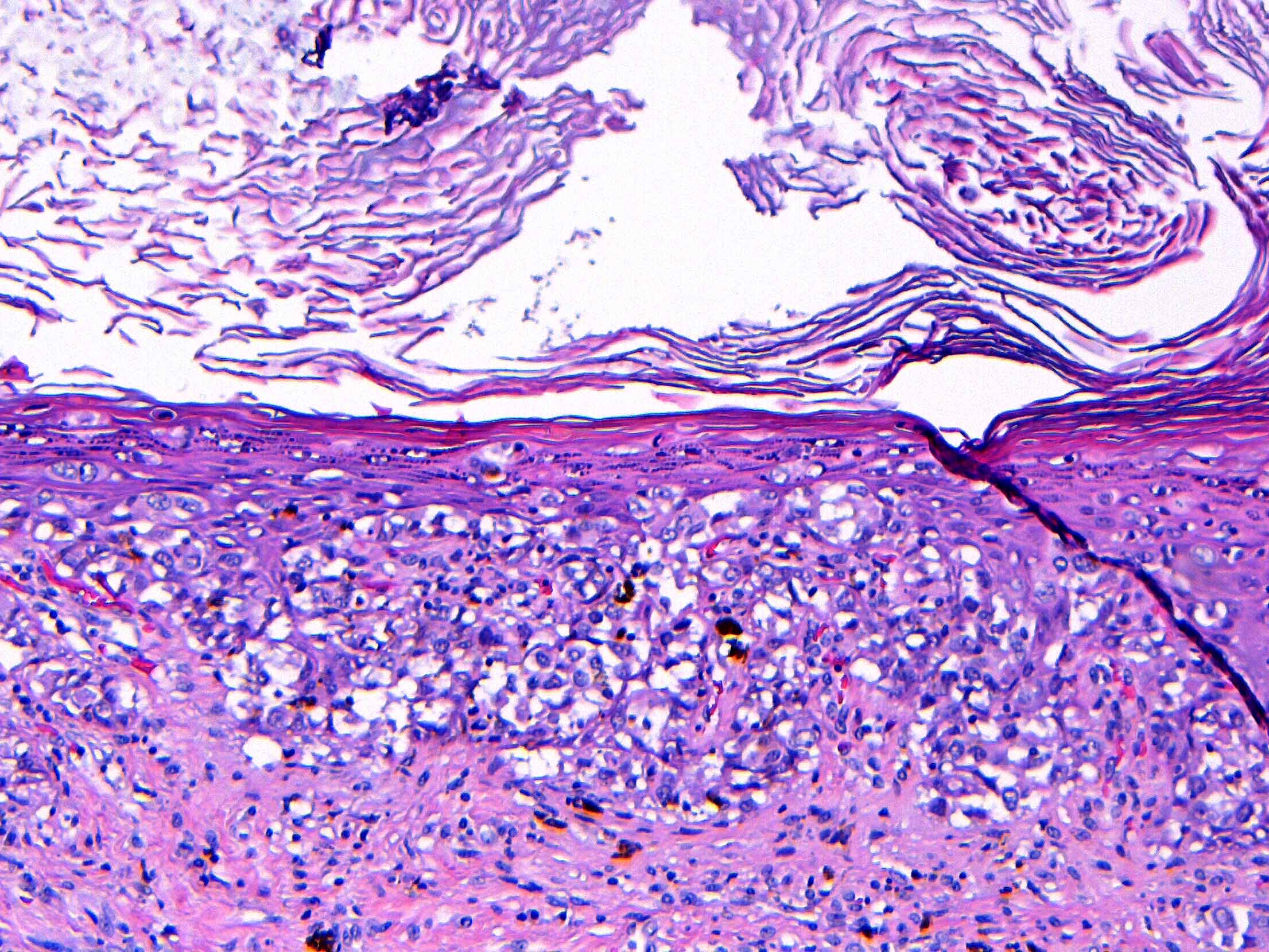
- Epidermis with hyperkeratosis and possibly ulceration
- Florid cases can show gland formation
- Paget cells may phagocytose melanin, mimicking melanocytes
- Underlying carcinoma is most commonly high grade invasive carcinoma of no special type (NST; 53 - 64%) or DCIS (24 - 43%) (Histopathology 2020;77:181)
Contributed by Anna Biernacka, M.D., Ph.D. and Mary Ann Gimenez Sanders, M.D, Ph.D.
Paget disease with dermal reaction
Paget cells in basal location
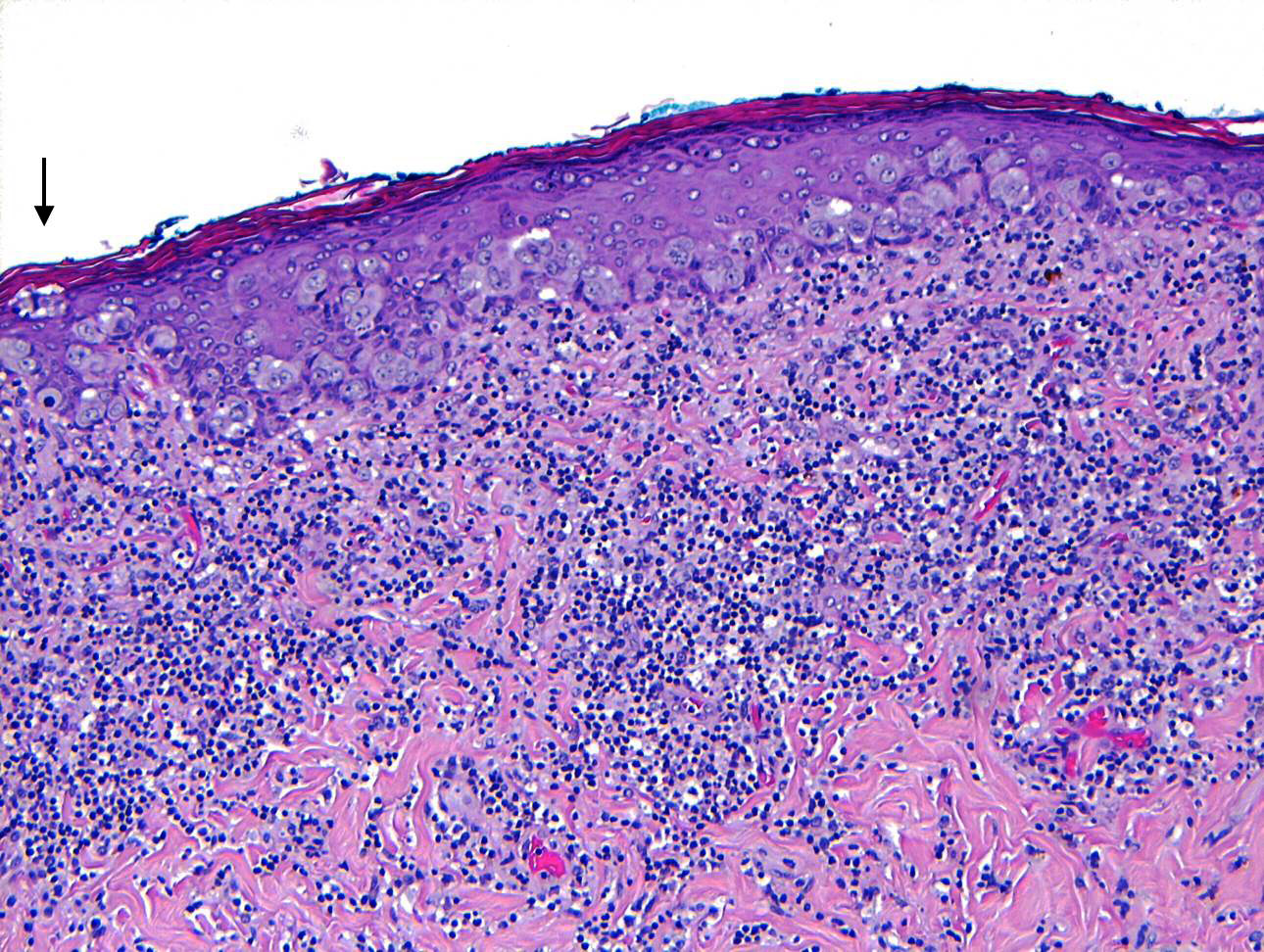
Superficial extension and inflammation
Cytologic features
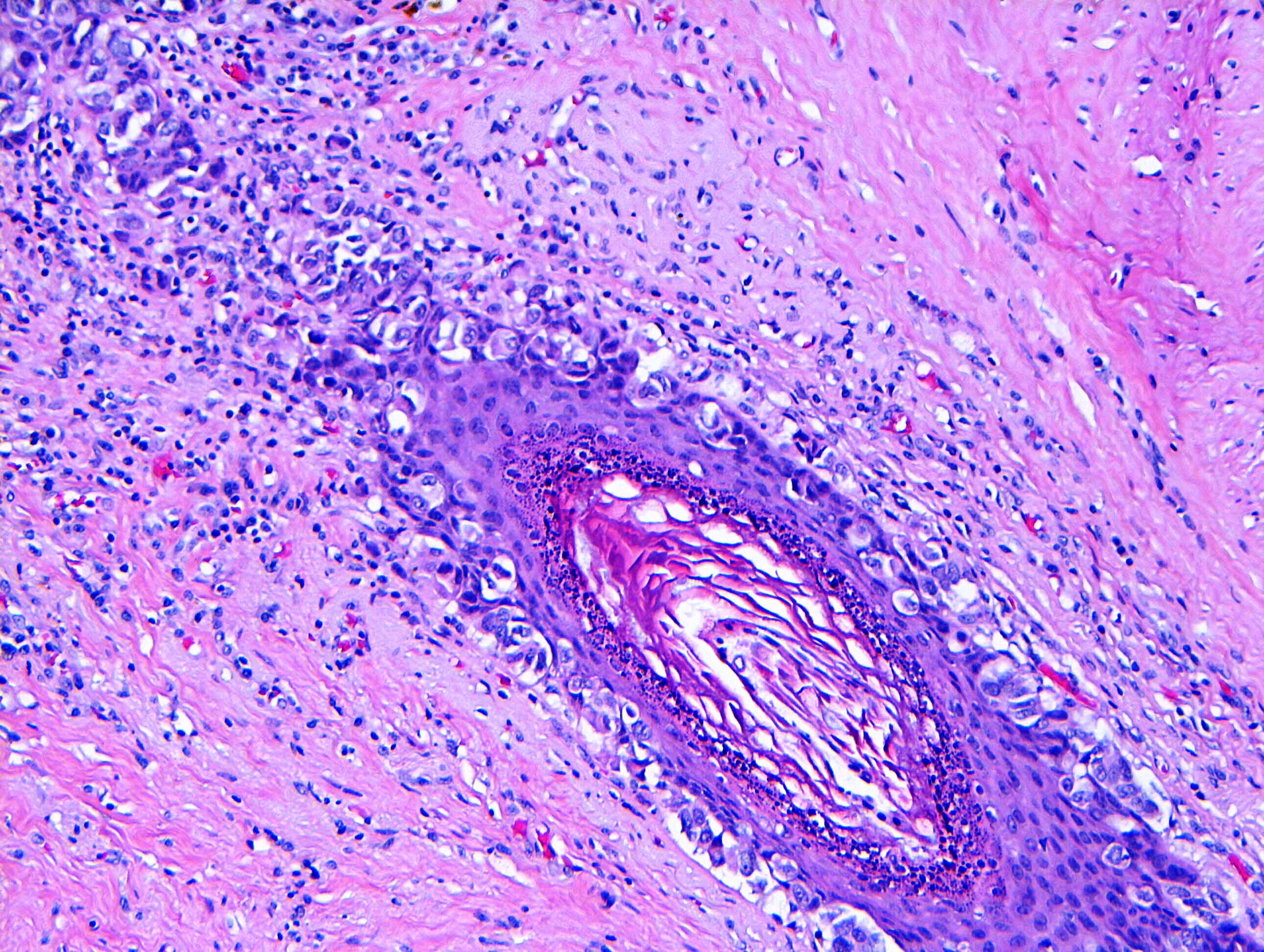
Spread to skin adnexa
Paget cells, shrinkage artifact
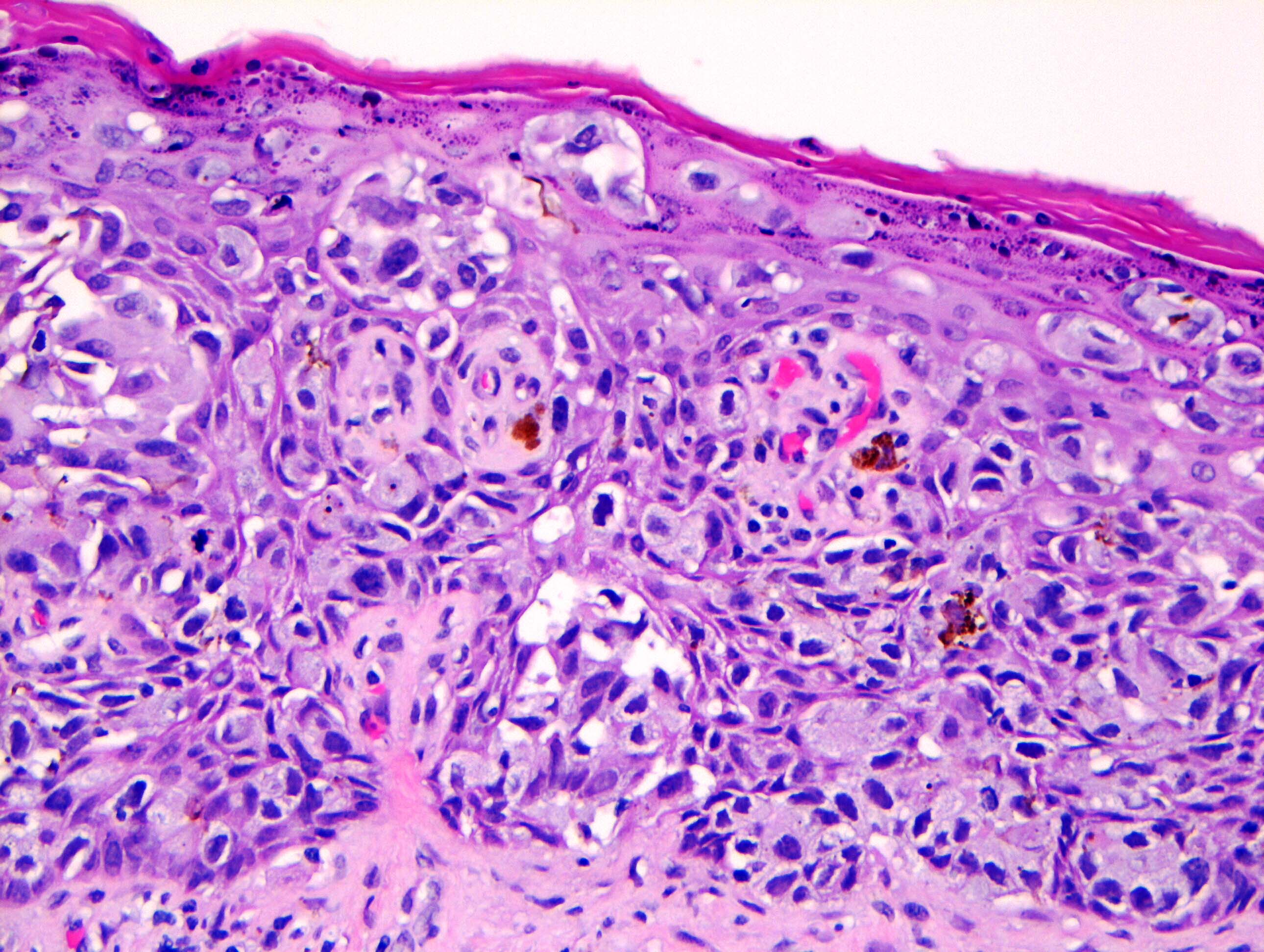
Paget cells, melanin uptake
Melanocyte hyperplasia

Full thickness with erosion
Invasive Paget disease
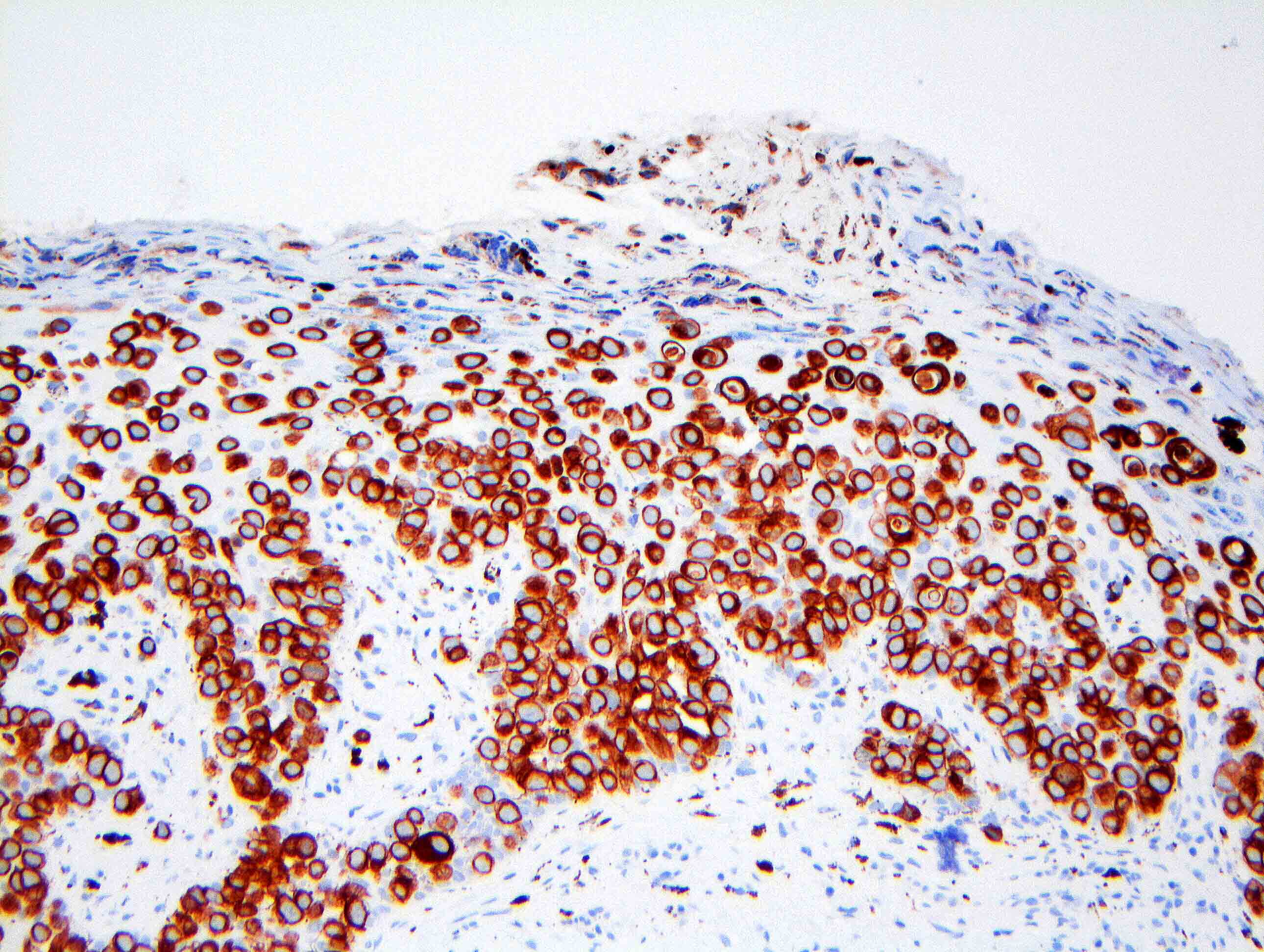
Mammary Paget disease CK7
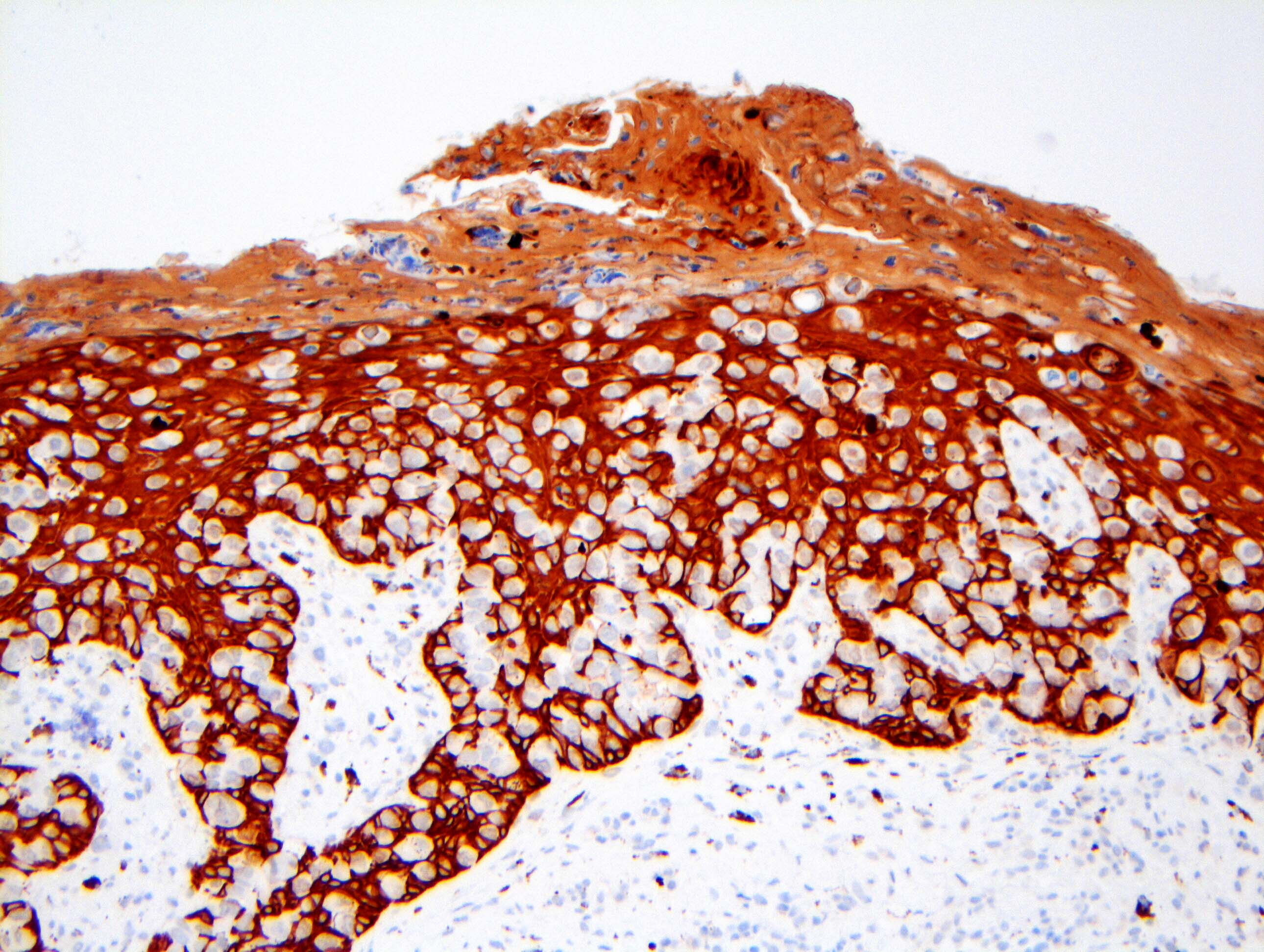
Mammary Paget disease CK5/6
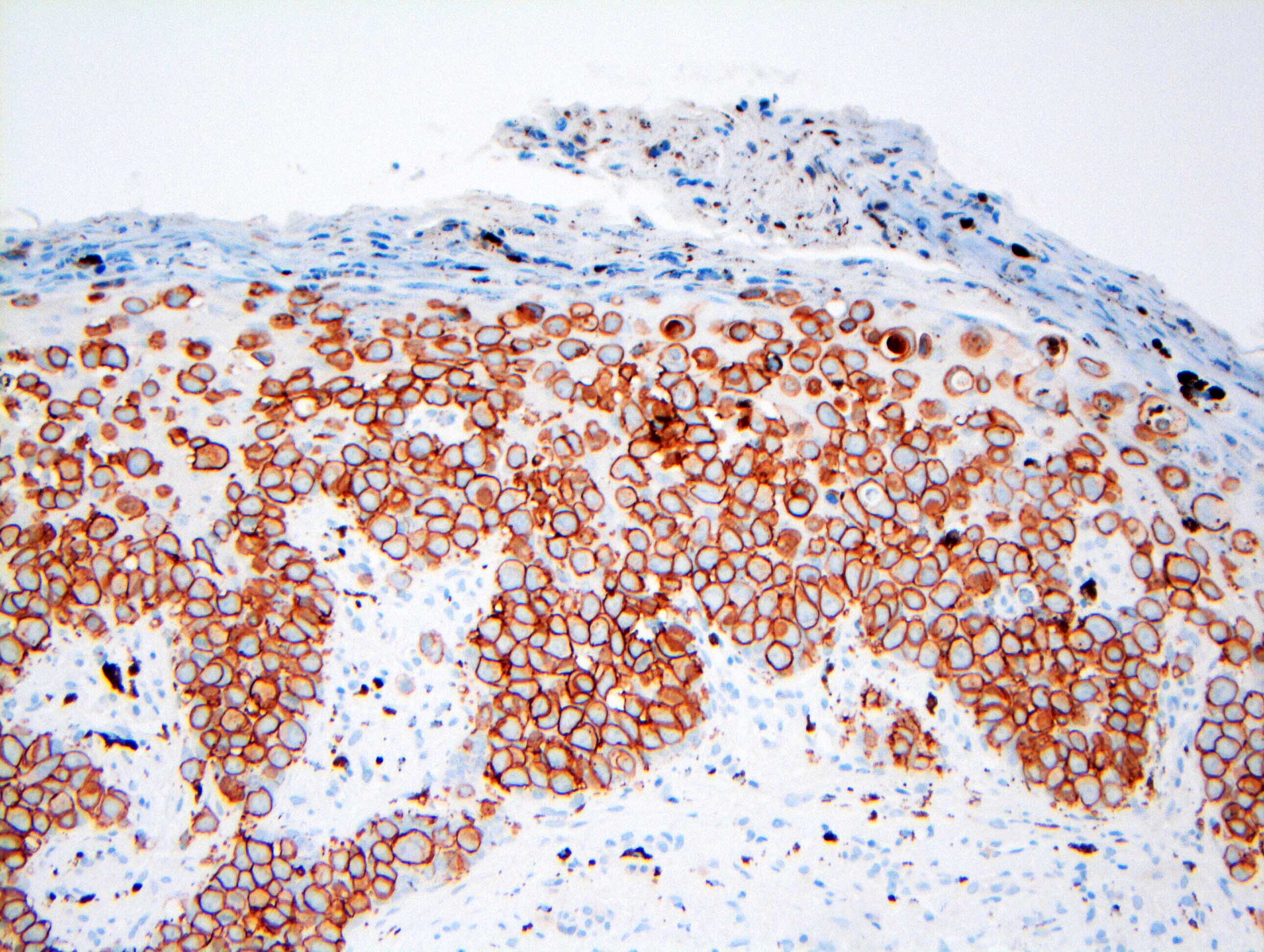
Mammary Paget disease HER2
Secondary Paget disease
Florid Paget disease
Images hosted on other servers:

Paget cells involving nipple ducts
- Tumor cells are often present on the surface of the epidermis and in the scale crust
- Nipple scrape preparation can be performed by using a scalpel to scrape the nipple, smearing it on 2 slides and performing either a Papanicolaou or May-Grunwald-Giemsa (MGG) stain
- 1 study, by comparing scrape smears and histological specimens, found that nipple scraping correctly detected MPD in 91.4% of cases (Diagn Cytopathol 2019;47:249)
- Cytomorphologic features include isolated and loosely clustered malignant glandular cells with enlarged nuclei, prominent nucleoli and pale cytoplasm, detected among squamous cells
- Cytologic differential diagnoses include nipple adenoma and squamous cell carcinoma detected
- In cases of clinical doubt, a punch biopsy may be indicated in parallel to scrape smears
Images hosted on other servers:

Dyscohesive cell groups
- CK7 (> 90%)
- HER2 (80 - 100%)
- CAM5.2 (70 - 100%)
- ER (10 - 40%)
- PR (0 - 30%) (Breast Cancer Res Treat 2013;141:1)
- CK7 negative Paget disease is rare and can be a diagnostic pitfall (Pathol Res Pract 2016;212:279)
- HMB45 (<1%)
- MelanA (<1%)
- CK5/6 (0 - 2%)
- CK20 (0 - 1%)
- S100 (0 - 25%)
- References: Breast Cancer Res Treat 2013;141:1, Am J Dermatopathol 2011;33:e54, J Am Acad Dermatol 2011;65:247, Am J Dermatopathol 2011;33:e54
- Desmosomal attachments have been identified between Paget cells and adjacent epidermal keratinocytes (Am J Pathol 1969;57:49)
- Same authors described a pre-Paget cell with an electron microscopy appearance intermediate between that of a keratinocyte and a Paget cell, suggesting that epidermal cells can acquire the characteristics of ductal cells as they undergo malignant transformation (transformation theory)
Images hosted on other servers:

Large, pale intraepidermal Paget cells

Single Paget cell
- No association with a specific gene mutation has been reported
- Paget cells are genetically similar to the underlying carcinoma cells in 80% of cases (Histopathology 2020;77:181)
Brief overview of Paget disease with pathologic images by Pathology mini tutorials
- Right nipple areolar complex, biopsy:
- Ductal carcinoma in situ involving the nipple epidermis (Paget disease) (see comment)
- Comment: The tumor cells are positive for CK7 and HER2 (3+) by immunohistochemistry, supporting the above diagnosis of Paget disease. ER and PR show no staining of in situ nuclei.
- For synoptic reporting, the appropriate AJCC T category is Tis (Paget) if no underlying DCIS is present or Tis (DCIS) if underlying DCIS is present
- If there is associated invasive carcinoma in the underlying breast parenchyma, the T category is based on the size of the invasive tumor
- If there is invasion from MPD into the dermis, only the size of the invasion should be used as size for T classification
- Differential diagnosis for MPD includes squamous cell carcinoma in situ (Bowen disease) and melanoma, although these diseases very rarely involve the nipple (Am J Dermatopathol 2017;39:419)
- Carcinoma in situ of skin / Bowen disease (Am J Dermatopathol 2017;39:419):
- Melanoma in situ:
- Toker cells and pagetoid dyskeratosis (Histol Histopathol 2009;24:367):
- CK5/6
- CK20
- ER
- HER2
- PR
Comment Here
Reference: Paget disease
Which of the following is true regarding the lesion identified in the nipple in the image shown above?
- Invasion into the dermis is associated with a poor prognosis
- Lesional cells can contain melanin pigment
- Lesional cells have a specific recurring genetic alteration
- Most disease is an extension of lobular carcinoma in situ (LCIS) from the underlying ducts
- Nipple always has eczematoid change
Comment Here
Reference: Paget disease
