
Breast
Invasive breast carcinoma of no special type and variants
Medullary
Authors: Shannon Mingo Welter, M.D., Emil Racila, M.D.
Editorial Board Member: Julie M. Jorns, M.D.
Deputy Editor-in-Chief: Gary Tozbikian, M.D.


Last author update: 25 April 2022
Last staff update: 25 April 2022
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Invasive breast carcinoma of no special type with medullary pattern
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Welter SM, Racila E. Medullary. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastmalignantmedullary.html. Accessed April 23rd, 2024.
Definition / general
- Medullary pattern is a histological pattern that can be applied to an invasive breast carcinoma of no special type that contains pushing borders, syncytial growth, high grade nuclei and prominent lymphoid infiltrate
- Represents one end of the spectrum of tumor infiltrating lymphocyte (TIL) rich invasive breast carcinomas of no special type rather than a distinct morphological subtype
Essential features
- Medullary pattern of invasive breast carcinoma no special type has 4 characteristic histological features (ideally, all 4 should be present for the diagnosis):
- Pushing border
- Syncytial growth pattern
- High grade nuclei
- Prominent lymphoid infiltrate
Terminology
- Preferred term according to WHO: invasive breast carcinoma of no special type with medullary pattern
- Historically described as medullary carcinoma, atypical medullary carcinoma, medullary features
ICD coding
- ICD-O: 8500/3 - infiltrating duct carcinoma, NOS
- ICD-11: 2C61.0 & XH7KH3 - invasive carcinoma of breast, NOS & infiltrating duct carcinoma, NOS
Epidemiology
- Often present earlier in life, median age of 53 (45 - 62) years (JAMA Netw Open 2021;4:e214123)
- Rare: less than 5% of all invasive breast cancers
Sites
- Breast
Pathophysiology
- Basal-like molecular subtype
- Same as molecular subtype matched invasive breast carcinoma of no special type (Breast Cancer Res Treat 2013;142:257)
Etiology
Clinical features
- Younger age
- Soft, palpable, circumscribed mass
- May have lymphadenopathy (due to hyperplasia rather than metastasis, which is uncommon)
Diagnosis
- Diagnostic steps are identical to invasive breast carcinoma (screening mammogram, diagnostic mammogram, ultrasound, core biopsy, etc.)
Radiology description
- Round, oval or lobulated mass on mammography
- Hypoechoic mass on ultrasound with thick echogenic halo
Radiology images
Contributed by Julie M. Jorns, M.D. and Mark R. Wick, M.D.
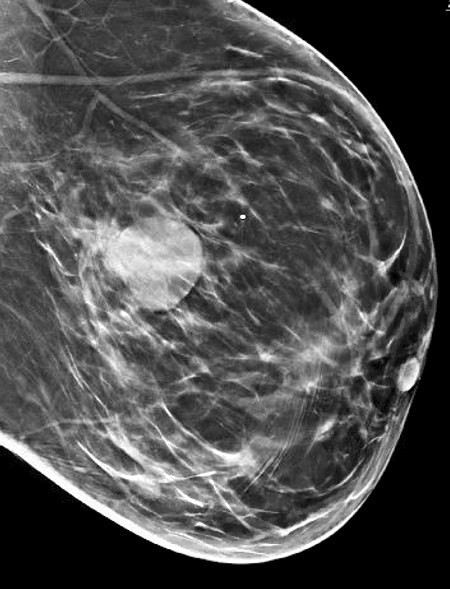
Mammogram
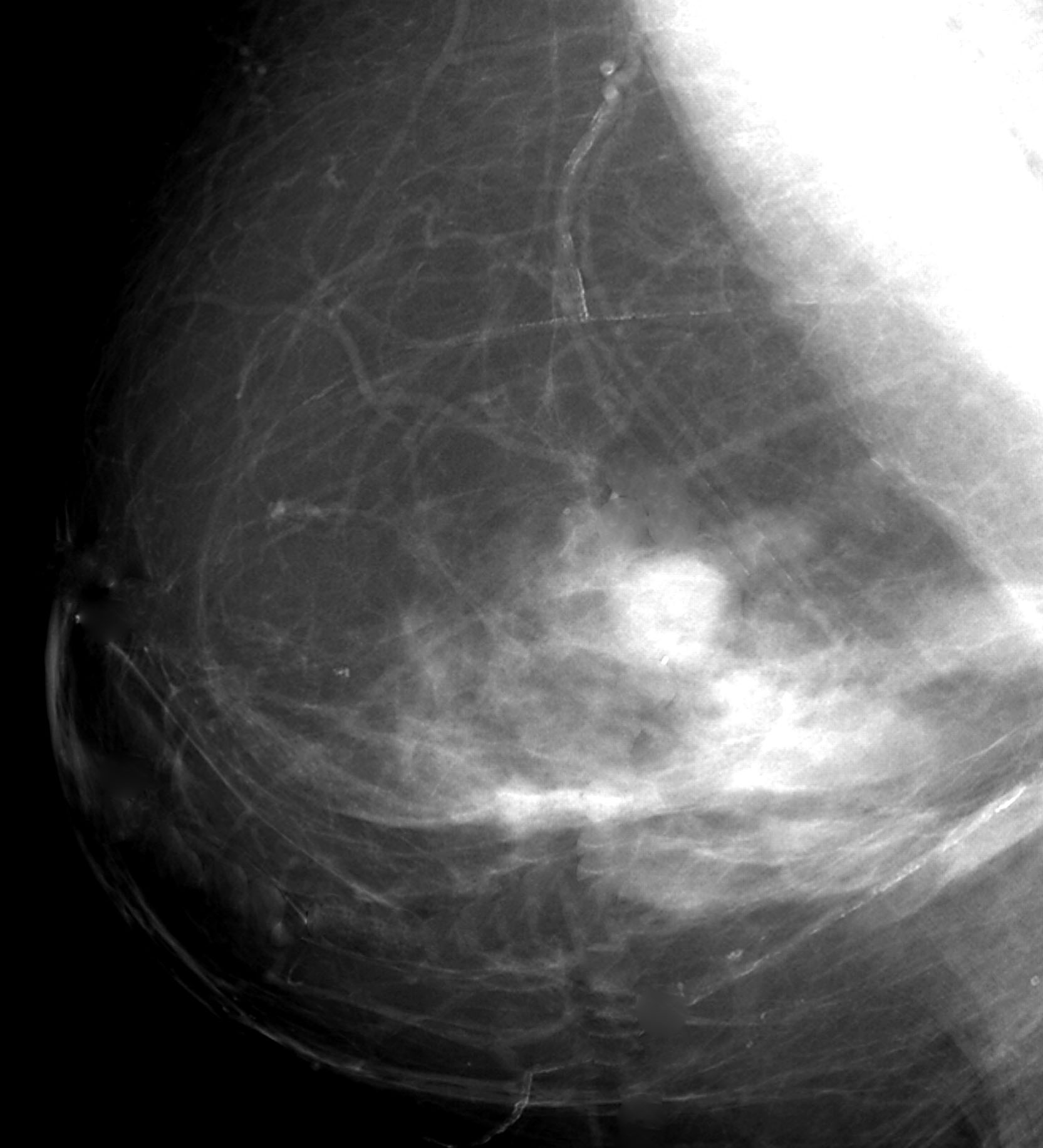
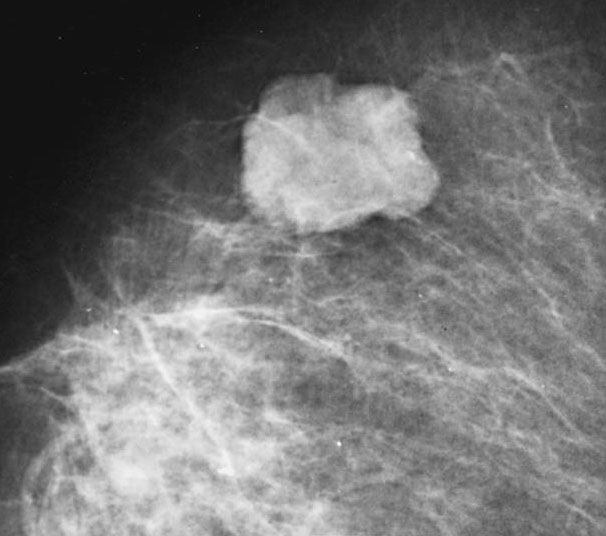
Mammogram
Prognostic factors
- Prognostic factors identical to invasive breast carcinoma of no special type: patient age, tumor histological grade, tumor stage, lymphovascular invasion, ER, PR and HER2 status, molecular subtype
- Additional prognostic factors:
- Triple negative breast cancers have more unfavorable prognosis then nontriple negative breast cancer (JAMA Netw Open 2021;4:e214123)
- Similar prognosis to stage matched grade 3 ductal carcinoma with prominent inflammation
- Better prognosis than grade 3 ductal carcinoma without prominent inflammation (Eur J Cancer 2009;45:1780)
- Tumor infiltrating lymphocytes have been shown to be of prognostic value (Ann Oncol 2015;26:259)
Case reports
- 38 year old woman who presented with a lump in both breasts for 3 months (J Cancer Res Ther 2012;8:129)
- 72 year old woman with invasive breast carcinoma with medullary pattern that had spontaneous pathological complete regression (Pol J Pathol 2019;70:139)
Treatment
- Identical to treatment options for invasive breast carcinoma of no special type with considerations for targeted therapy based on ER, PR, HER2 status
- Tumor infiltrating lymphocytes do not alter therapy currently
Gross description
- Well circumscribed, 2 - 3 cm in size, soft and fleshy (may resemble fibroadenoma)
- Homogenous with white to gray appearance
Gross images
Contributed by Mark R. Wick, M.D.
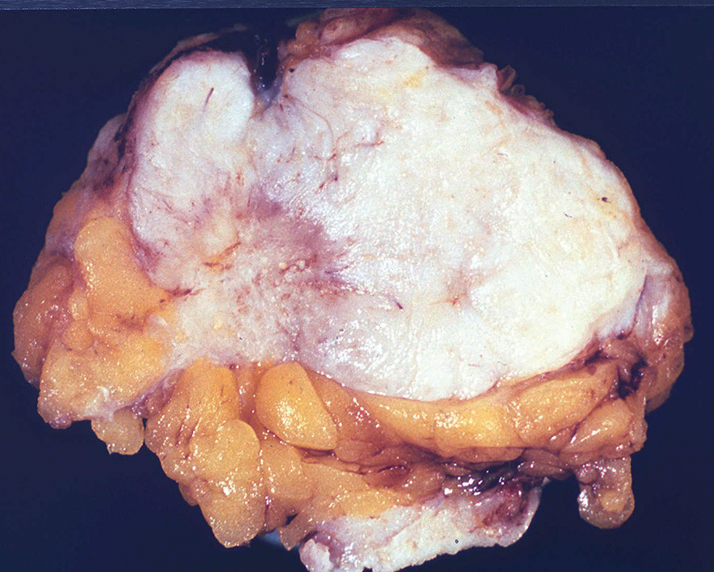
White mass
Microscopic (histologic) description
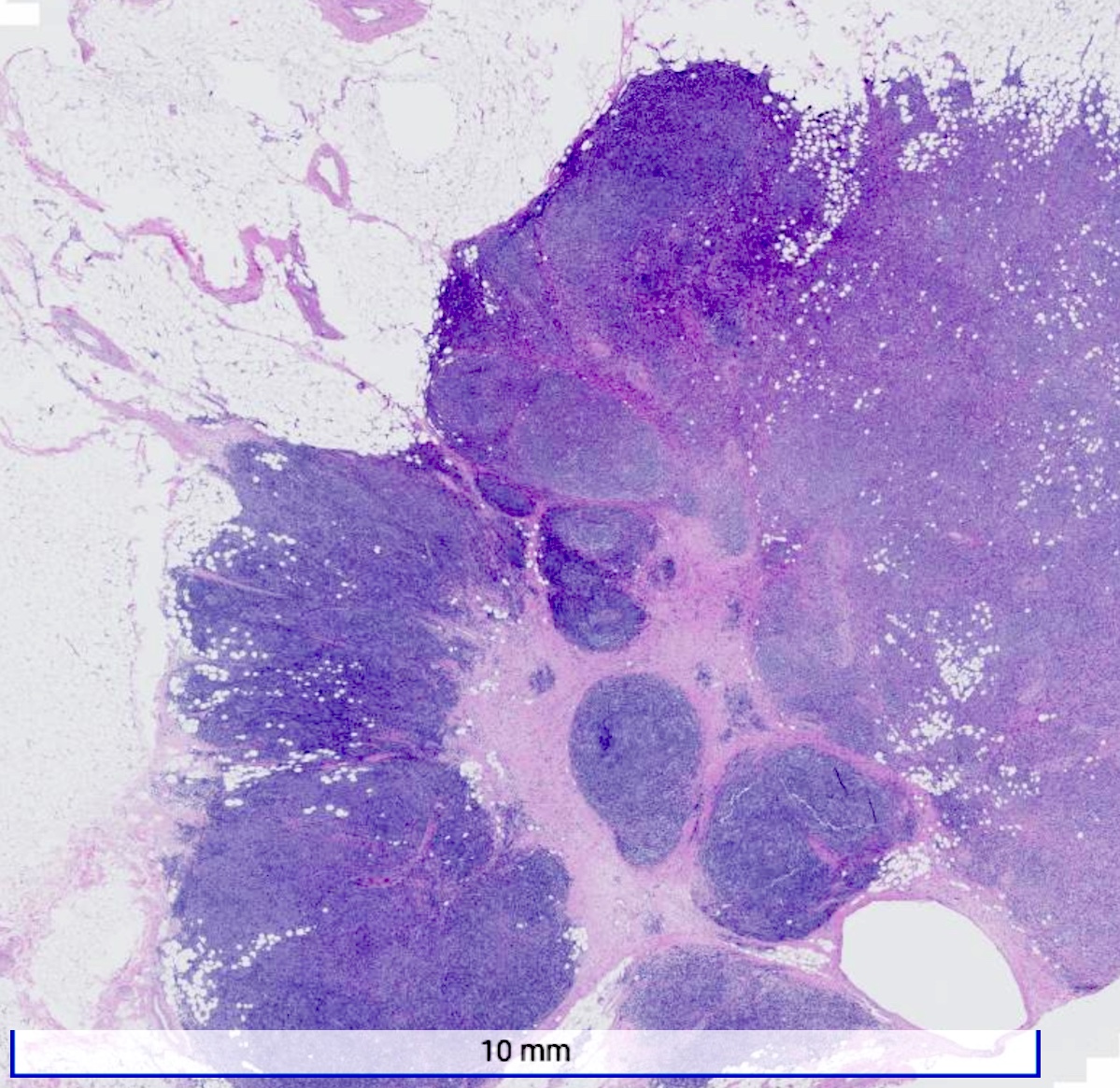
- Well circumscribed pushing border
- Cells in syncytial growth pattern with no glandular structures
- High histologic grade, high grade nuclei with prominent nucleoli
- Prominent tumor infiltrating lymphocyte infiltrate
Microscopic (histologic) images
Contributed by Shannon M. Welter, M.D. and Julie M. Jorns, M.D.

Circumscribed tumor
Prominent lymphoid infiltrate
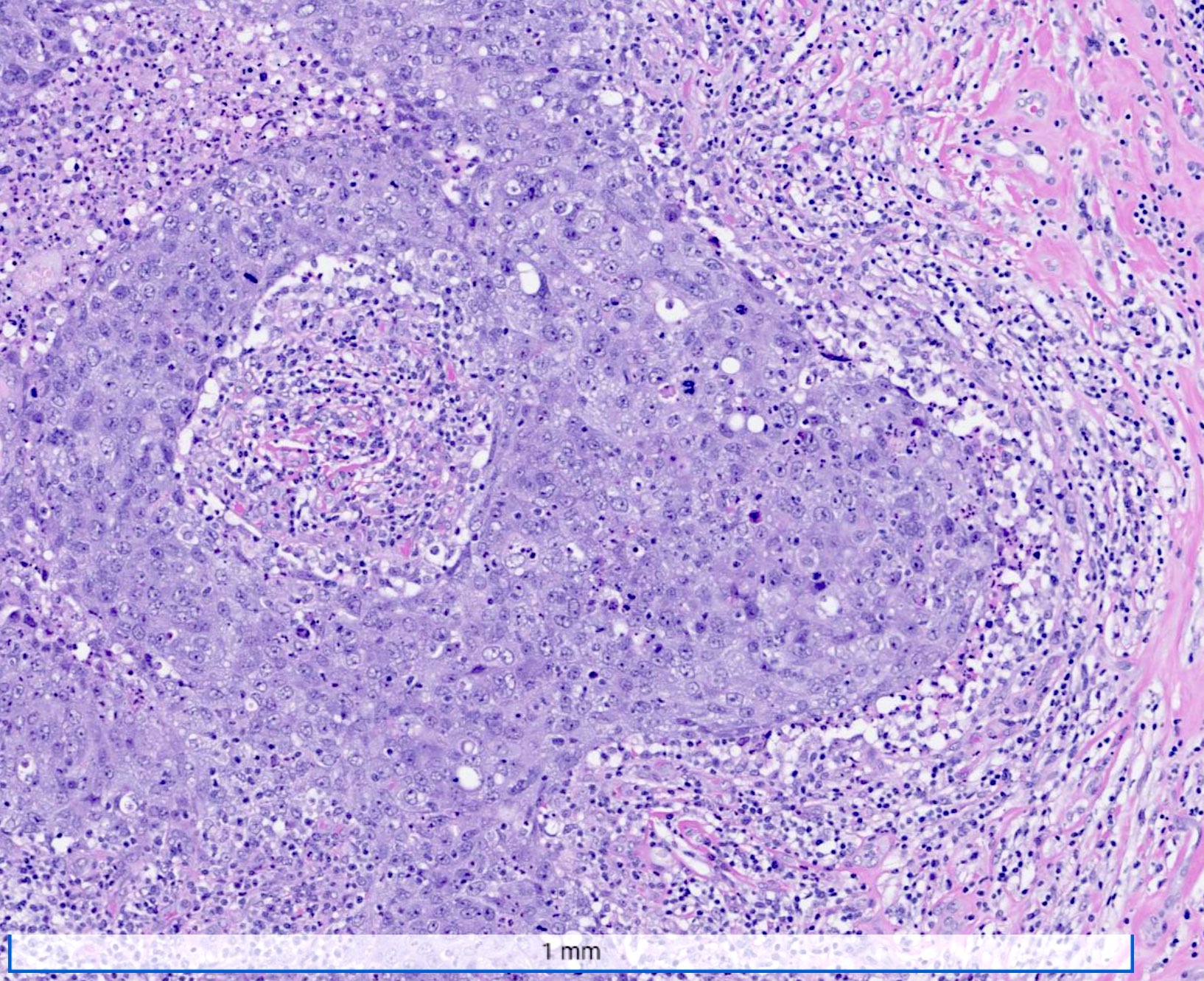
Syncytial growth pattern

Stromal lymphocytes
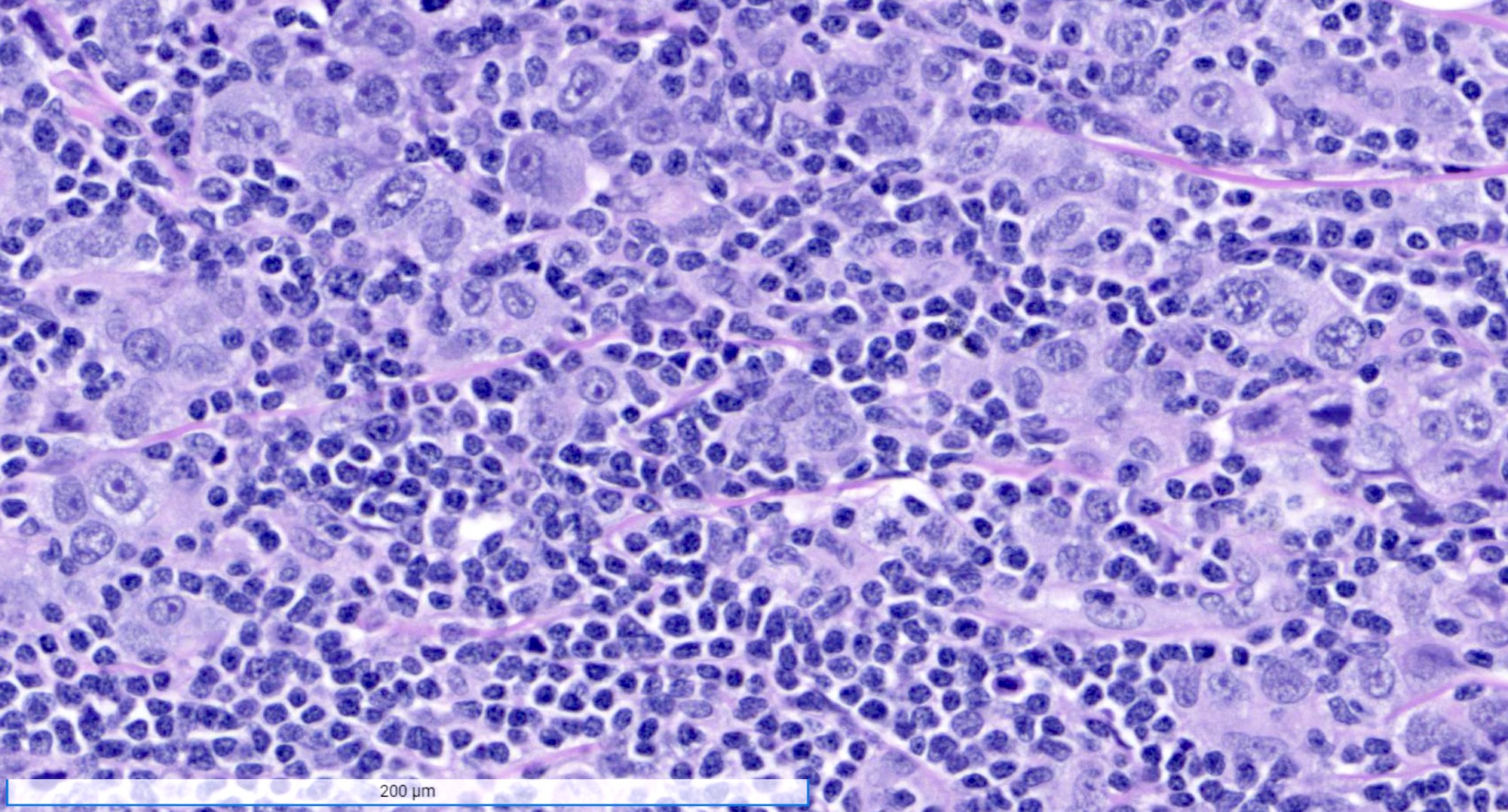
High grade nuclei
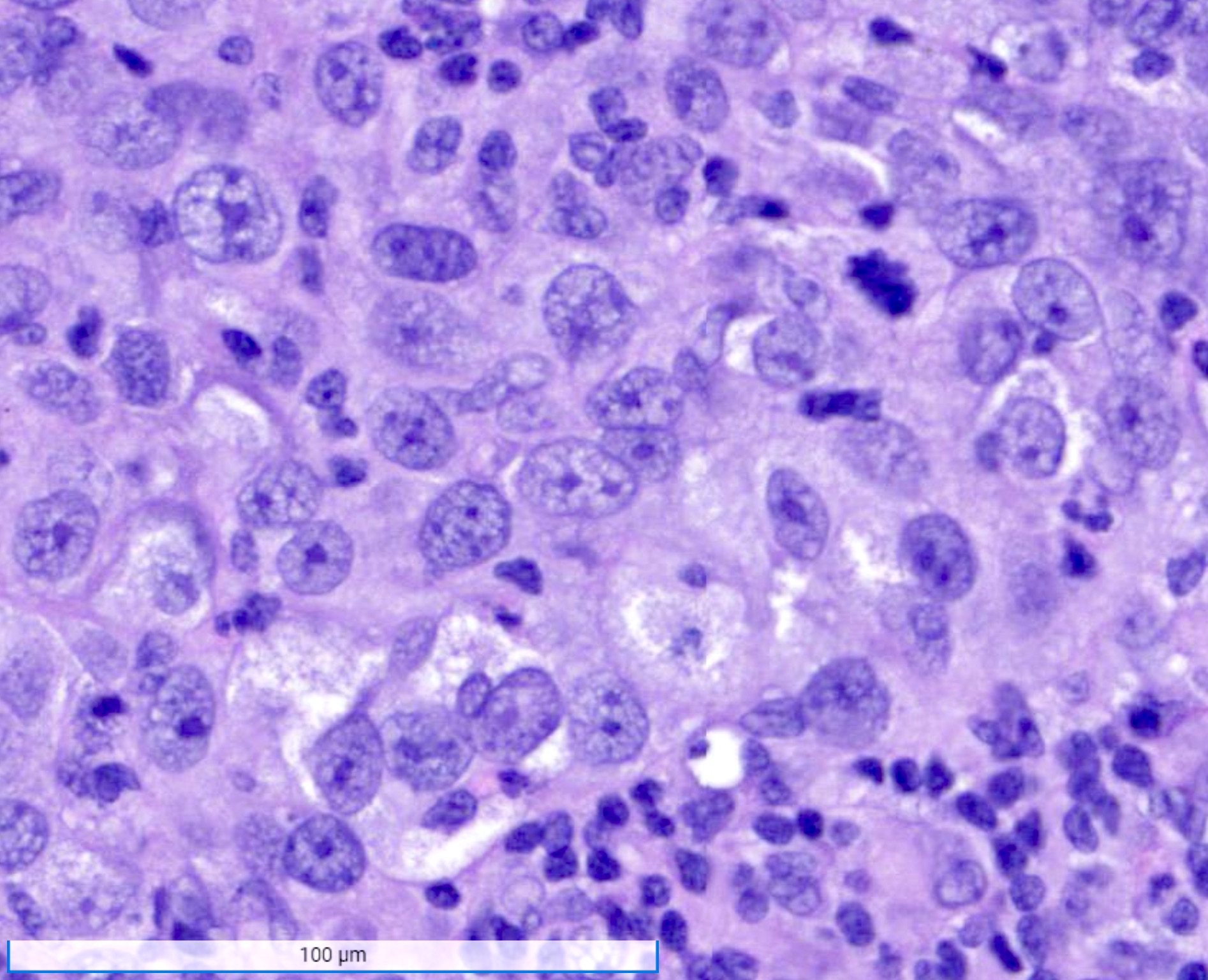
High grade nuclei
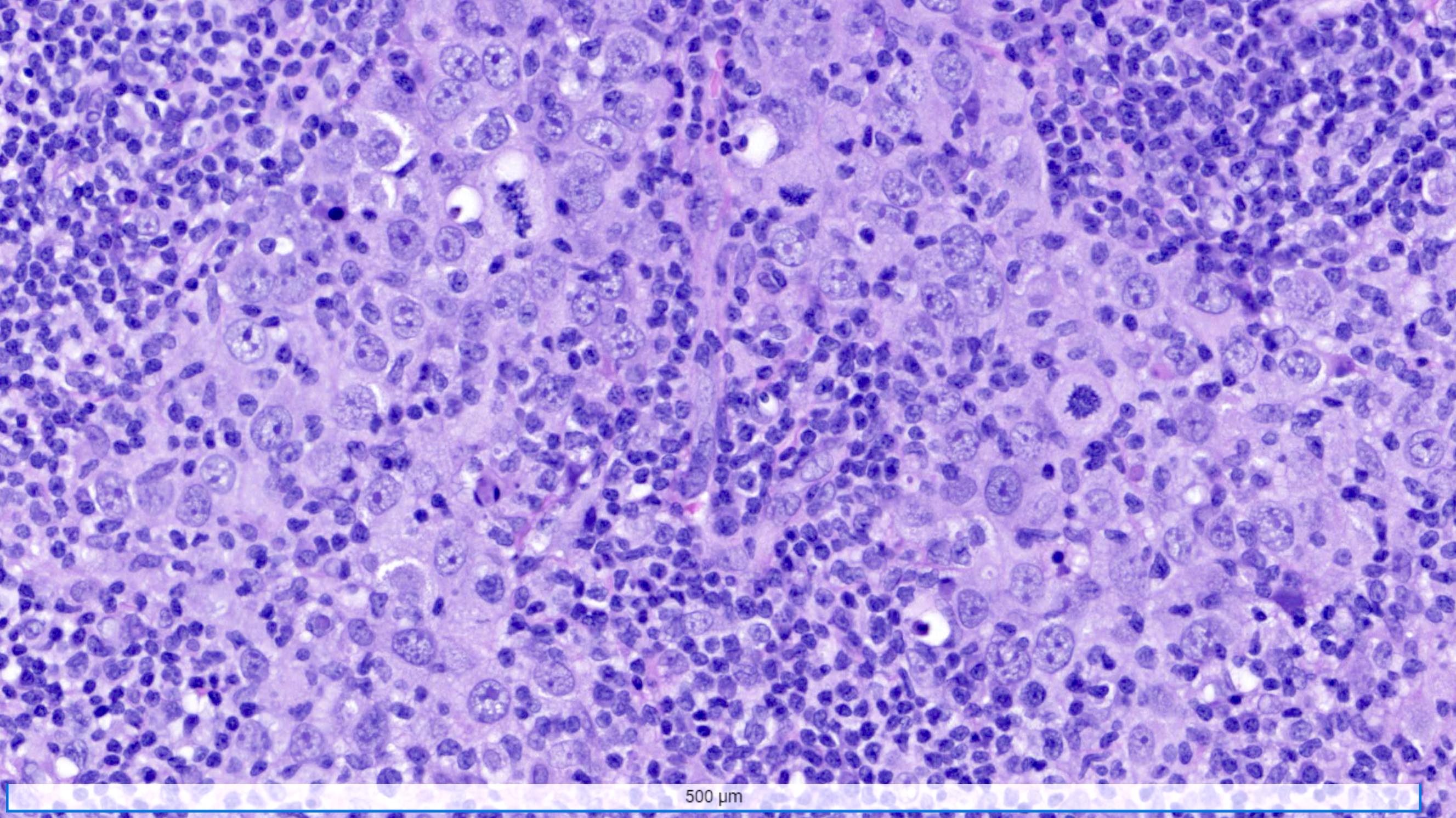
Numerous mitotic figures
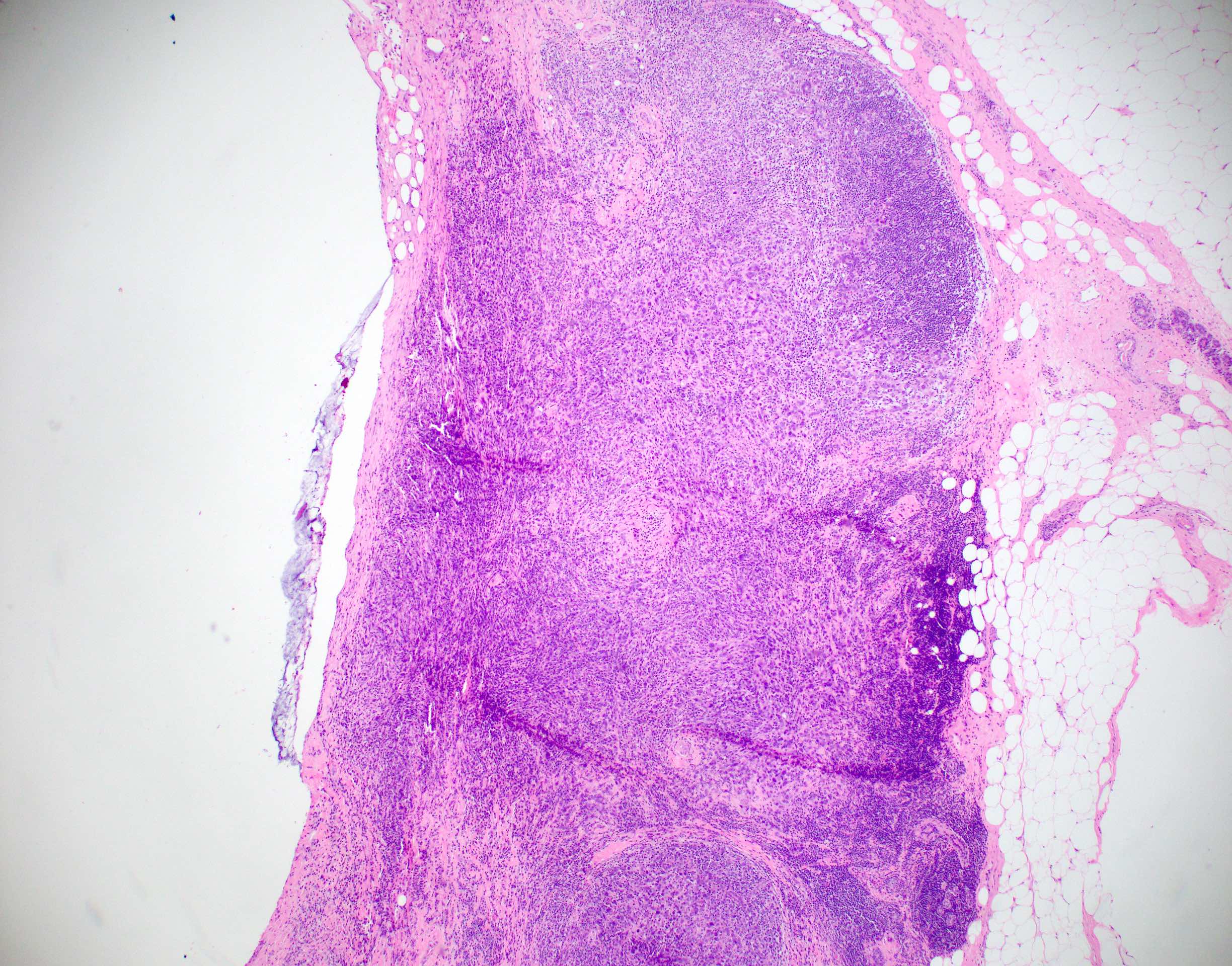
Biopsy site and circumscription
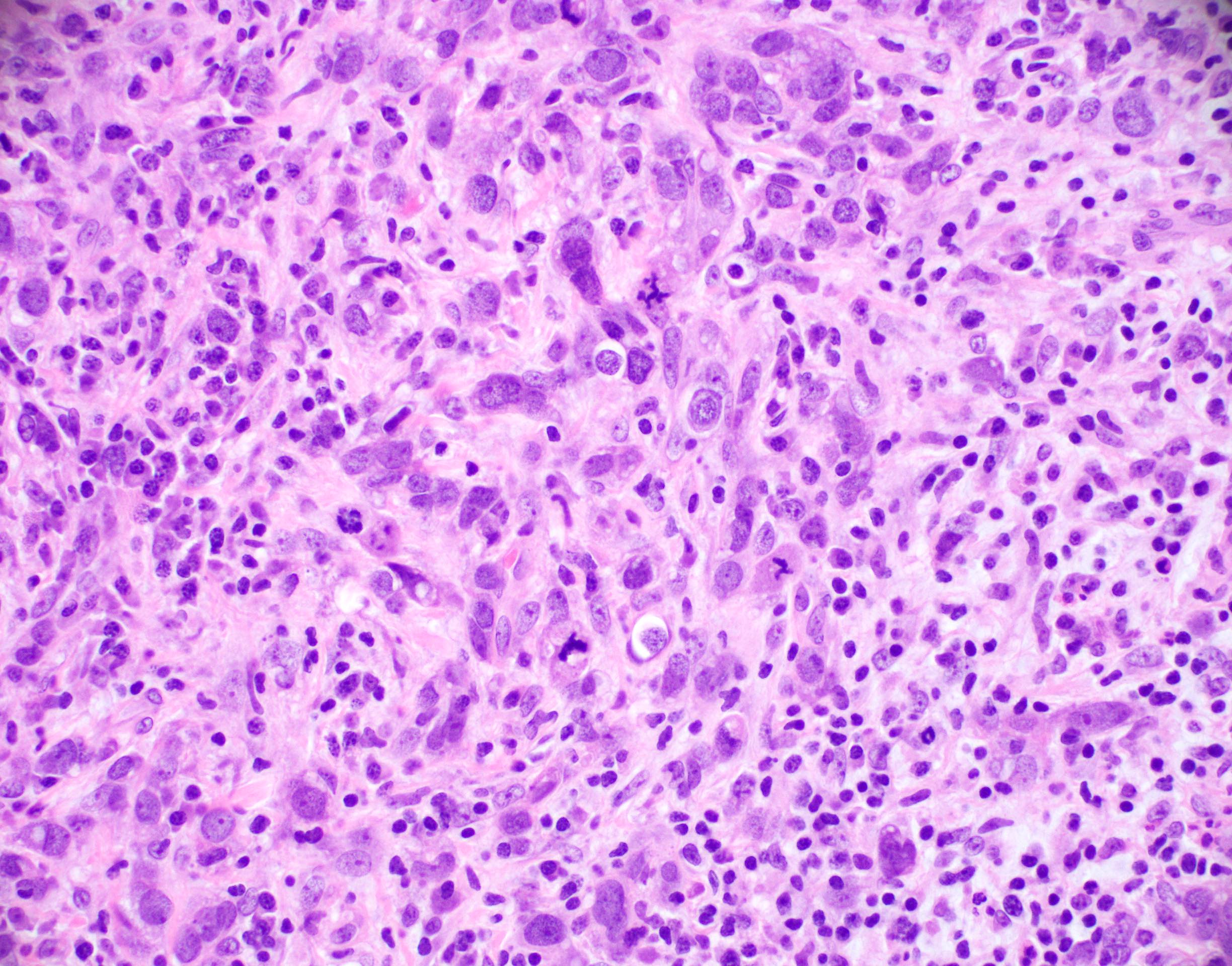
Syncytial growth and lymphoplasmacytic infiltrate
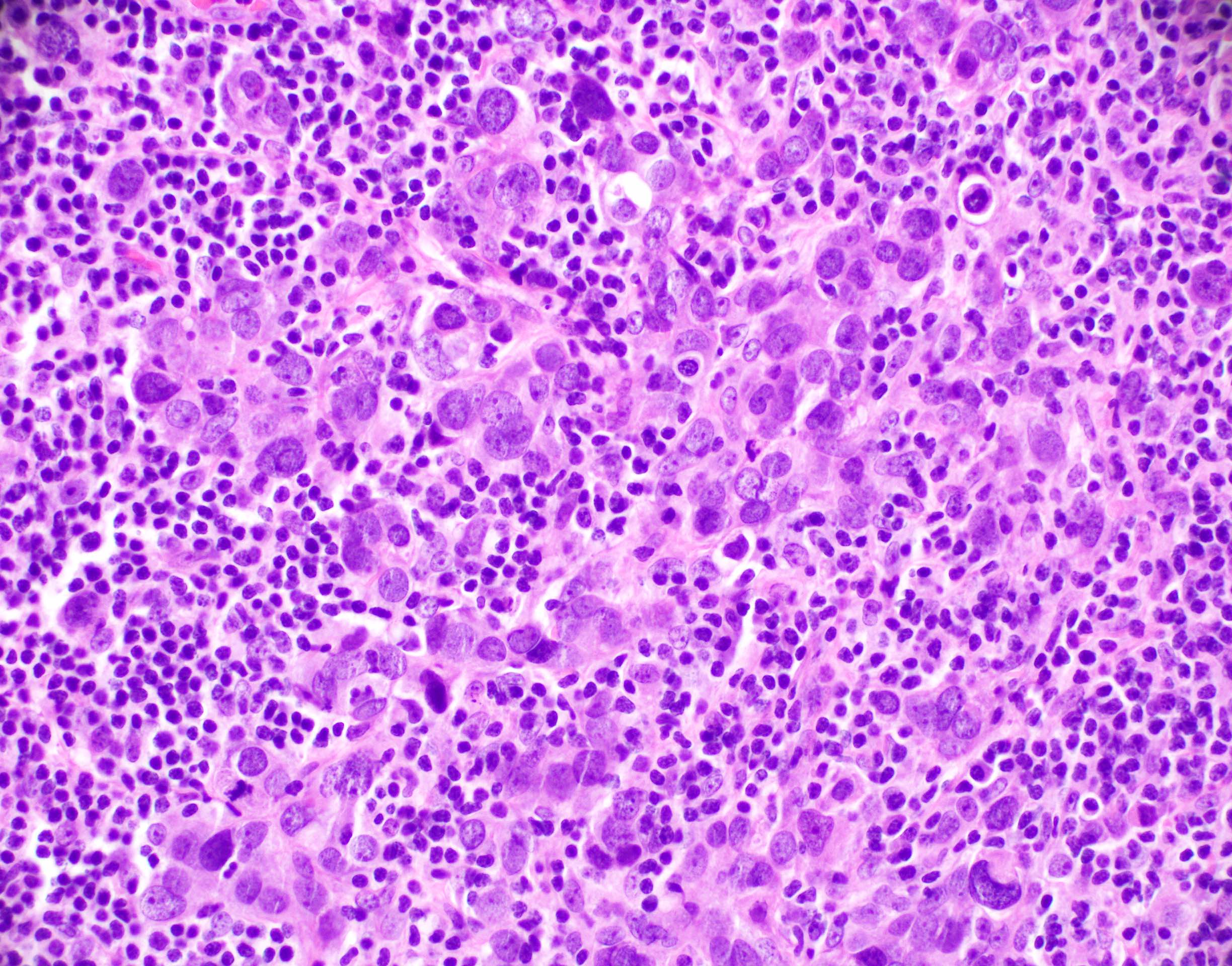
Lymphoplasmacytic
infiltrate
Virtual slides
Images hosted on other servers:

Breast cancer with medullary pattern
Cytology description
- Hypercellular specimen
- Numerous isolated cells and loose clusters
- Markedly enlarged, vesicular nuclei
- Prominent, often irregular macronucleolus
- Many lymphocytes and some plasma cells
Positive stains
- Variably expresses basal markers such as CK5/6, CK14, EGFR (HER1) and p53
- Higher rate of PDL1 expression (83.1%) as compared to other triple negative breast cancers (Eur J Breast Health 2019;15:235)
Negative stains
- Most often negative for hormone receptors (ER and PR) and HER2 (triple negative breast cancer)
Molecular / cytogenetics description
- Genomic instability is common
- Majority of these tumors fall within the basal-like molecular profile
- Approximately 15% of tumors in BRCA1 mutation carriers are classified as invasive breast carcinoma with medullary pattern (J Natl Cancer Inst 1998;90:1138)
Sample pathology report
- Breast, right, segmental mastectomy:
- Invasive breast carcinoma of no special type with medullary pattern (see synoptic report)
- Carcinoma contains 90% stromal tumor infiltrating lymphocytes
Differential diagnosis
- Metastatic high grade carcinoma to the breast from another site:
- Lacks a coexistent in situ component
- May be within a lymph node or have abundant associated angiolymphatic invasion
- Immunohistochemistry is often needed for distinction
- Lymph node:
- Contains capsule or subcapsular sinus; both may have germinal centers
- Lymphoma:
- Tumor cells will stain with lymphoid markers, cytokeratin negative
Additional references
Board review style question #1
The tumor in the above image is found in the breast of a 45 year old woman. The tumor was round and soft on palpation and had pushing borders on microscopy. What is the most likely diagnosis?
- Ductal carcinoma in situ
- Invasive breast carcinoma with medullary pattern
- Invasive lobular carcinoma
- Secretory carcinoma
Board review style answer #1
B. Invasive breast carcinoma with medullary pattern
Comment Here
Reference: Invasive breast carcinoma of no special type with medullary pattern
Comment Here
Reference: Invasive breast carcinoma of no special type with medullary pattern
Board review style question #2
Which of the following is a feature of invasive breast carcinoma with medullary pattern?
- Extensive surrounding ductal carcinoma in situ
- Low histologic grade
- Present as calcifications on mammography
- Prominent lymphocytic infiltrate
Board review style answer #2
D. Prominent lymphocytic infiltrate
Comment Here
Reference: Invasive breast carcinoma of no special type with medullary pattern
Comment Here
Reference: Invasive breast carcinoma of no special type with medullary pattern
Board review style question #3
This breast tumor most often falls into which molecular profile?
- Basal-like
- HER2 enriched
- Luminal A
- Luminal B
Board review style answer #3
A. Basal-like
Comment Here
Reference: Invasive breast carcinoma of no special type with medullary pattern
Comment Here
Reference: Invasive breast carcinoma of no special type with medullary pattern
