
Breast
Breast cancer
Male invasive
Editorial Board Member: Emily S. Reisenbichler, M.D.
Deputy Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 1 April 2018
Last staff update: 29 April 2022
Copyright: 2001-2025, PathologyOutlines.com, Inc.
PubMed Search: Male breast carcinoma


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Molecular / cytogenetics description | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Diez Freire CC, Masood S. Male invasive. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastmalignantmalecarcinoma.html. Accessed April 1st, 2025.
Definition / general
- Male breast cancer is uncommon, accounting for < 1% of all male cancers and 0.1% of male cancer deaths
- Tends to occur at an older age group (60 - 70s) when compared to women (50 - 60s) and has a larger tumor size (J Clin Oncol 2010;28:232)
- Surveillance, Epidemiology and End Results (SEER) program shows a rise in the incidence across the U.S. (Cancer 2004;101:51)
Essential features
- Most are ductal carcinoma in situ or invasive ductal carcinoma
- Most are ER+ (Ann Oncol 2013;24:viii75)
- BRCA2 is the strongest familial risk factor in men (associated with 17% of male breast cancers) (Histopathology 2016;68:110)
Terminology
- Invasive ductal carcinoma, ductal carcinoma in situ
ICD coding
- ICD-10: C50 - malignant neoplasm of breast
Epidemiology
- Average age of onset of DCIS is sixth decade; for invasive carcinoma is seventh decade, although highest incidence occurs in the eighth decade of life (Breast Cancer Res Treat 2004;83:77)
- Incidence is lower in Japanese and higher in African Americans from West Africa and United States when compared to Caucasians from United States
- Death rate is higher among nonwhite men in the United States and lower among Japanese men in Japan (J Natl Cancer Inst 1978;60:1223, Am J Public Health Nations Health 1963;53:890)
- Despite the differences in the hormone receptor and HER2 status expression among the different races and ethnicities, no difference in the overall survival (Cancer 2013;119:1611)
- 2x increased risk among first degree relatives of male breast cancer patients
Sites
- Tend to be located centrally in retroareolar position and also in upper outer quadrants
Etiology
- Associated with increased serum estrogen: liver disease, obesity, exogenous therapy, antiandrogen therapy
- Associated with decreased serum androgen: Klinefelter syndrome, testicular injury / atrophy, occupational exposure to high temperatures
- Drugs, exogenous agents: digitalis, tricyclic antidepressants, marijuana, lavender oil, tea tree oil
- Radiation
- Pituitary gland dysfunction: hyperprolactinemia
- Hereditary: BRCA2 mutation carriers, PTEN mutation (Cowden syndrome), CHEK2 mutation carriers
Clinical features
- Invasive carcinoma:
- Average age of presentation is 60 to 70 years, although can present in younger men and children
- ~75% present with a palpable mass
- Can also present with nipple retraction, ulceration or nipple discharge (serous); may be nodular and cystic
- Time lapse between symptoms and clinical consultation varies from 6 months to 1 year
- Tends to present with larger size and at a higher stage in men than in women
- Lymph node metastases are more common in men than women
- Axillary nodal staging is done by sentinel lymph node biopsy
- History of breast cancer does not significantly affect the age or stage at time of diagnosis or the prognosis (Cancer 1999;86:821)
- Annual clinical screening exam recommended in men with BRCA mutations
Diagnosis
- Clinical presentation, imaging findings and ultimately image guided biopsies of the lesion provide tissue for an accurate pathologic diagnosis
Radiology description
- No guidelines recommending mammographic screening for men have been established, even with documented genetic predisposition
- Mammographic findings in men with breast cancer reveal distinct lesions with invasive margins that contrast sharply with the surrounding fatty tissue
- Microcalcifications found in 9 - 30%
- Ultrasound: round mass with calcifications and papillary components like those seen in cystic or encapsulated papillary carcinoma
- Can be used to differentiate gynecomastia from carcinoma
- Inflammatory carcinoma of the male breast produces diffuse enlargement and thickening of the skin that can be detected by MRI
Radiology images
Images hosted on other servers:

Ultrasound of lymph node metastasis
Prognostic factors
- Poor prognostic factors: lymphatic tumor emboli, tumor size over 2 cm, poor histologic differentiation, HER2 overexpression, p53 expression, amplification of CCND1 (11q13)
- Men with a prior diagnosis of breast carcinoma have a 30x increased risk of invasive carcinoma in the contralateral breast, increasing to 110x if the original diagnosis was before age 50
- Death rate is higher among nonwhite U.S. men and lower among Japanese men
- Most investigators believe men and women with the same stage disease have similar prognosis, but some believe men have poorer prognosis
- AR+ luminal type A male breast cancer (ER+ HER2-, tumor grade 1/2) has better overall survival at 5 years but not 10 years compared to female breast cancer (Breast Cancer Res Treat 2012;133:949)
Case reports
- 40 year old man with occult breast cancer first manifesting as axillary lymph node metastasis (Medicine (Baltimore) 2015;94:e1038)
- 72 year old man with acromegaly and breast cancer (BMC Cancer 2015;15:397)
- 75 year old man with bilateral synchronous breast cancer (Saudi Med J 2015;36:359)
Treatment
- Treatment recommendations for male breast cancer are based on guidelines established for female breast cancer
- Most men are treated with mastectomy and axillary lymph node dissection
- Radiation, hormonal therapy and chemotherapy are also used
- Breast conservation therapy may be possible, especially in older patients
- Tamoxifen has less mortality when compared to aromatase inhibitors in men with stage I - III ER+ carcinoma (Breast Cancer Res Treat 2013; 137:465)
Clinical images
Images hosted on other servers:

Bilateral tumors
Gross description
- Male breast cancers are grossly identical to female breast cancers; cystic papillary carcinomas can be striking
Gross images
Images hosted on other servers:

Intracystic papillary carcinoma
Microscopic (histologic) description
- In situ carcinoma with papillary architecture is the most common pattern; also cribriform, micropapillary and solid patterns
- Most (~85%) male breast carcinoma is poorly differentiated infiltrating ductal carcinoma, followed by papillary carcinoma and other types similar to female breast cancer
- Lobular carcinoma represents 2% of cases
Microscopic (histologic) images
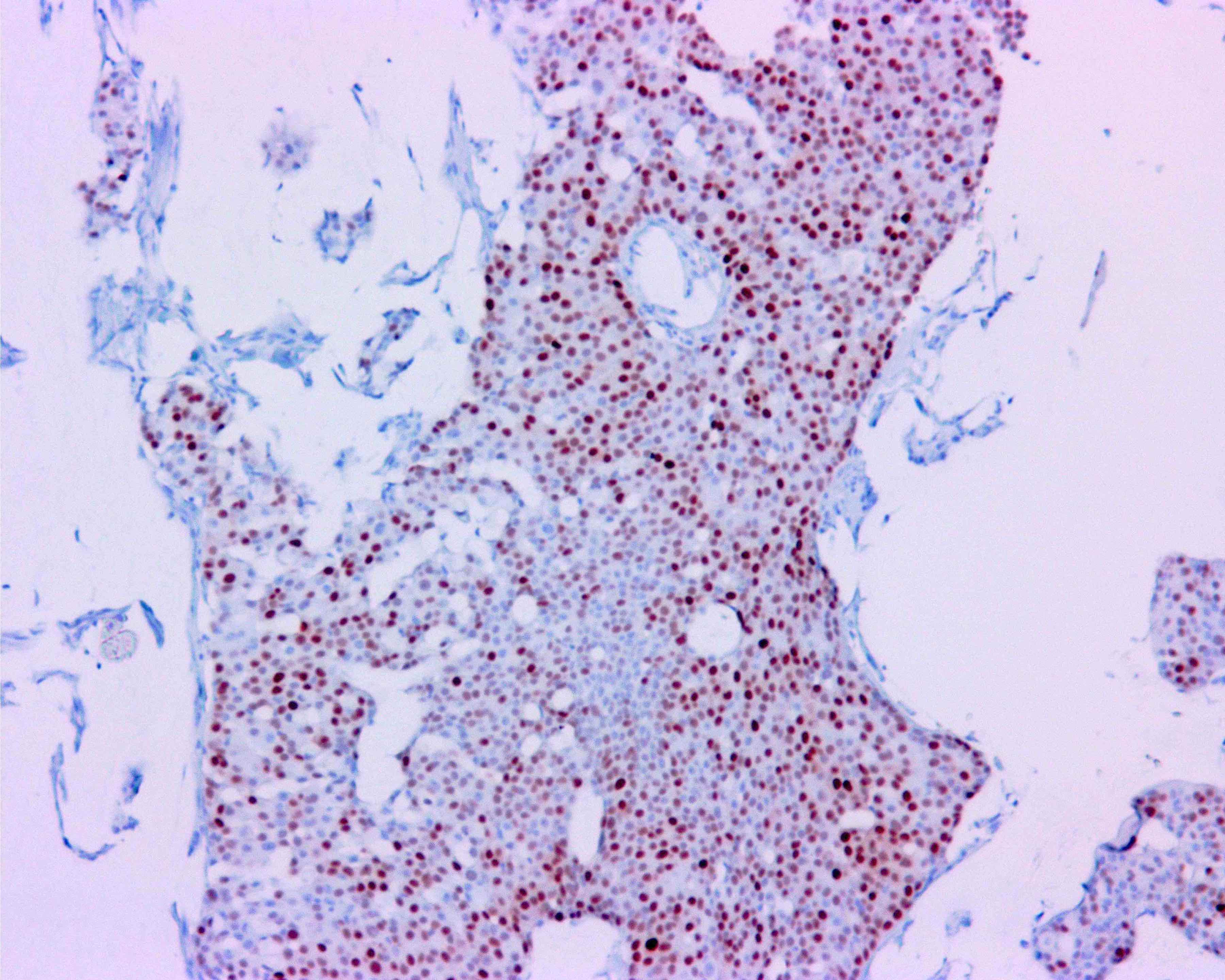
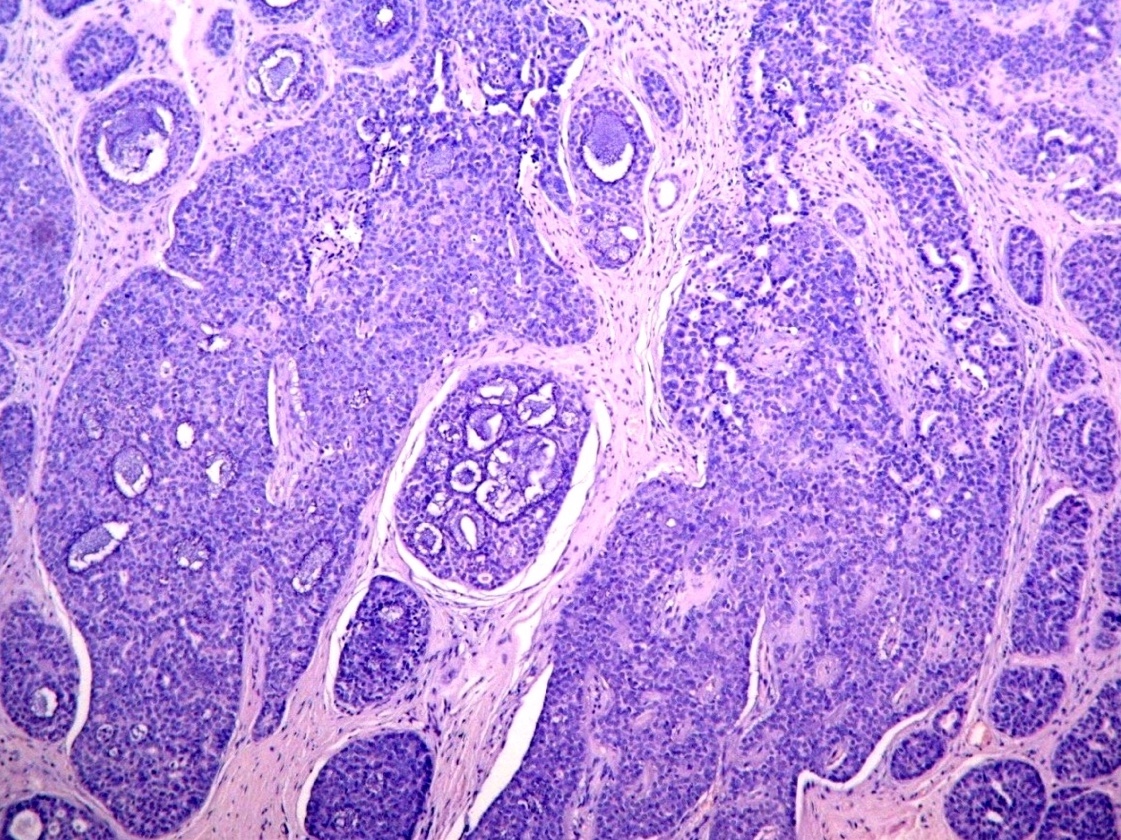
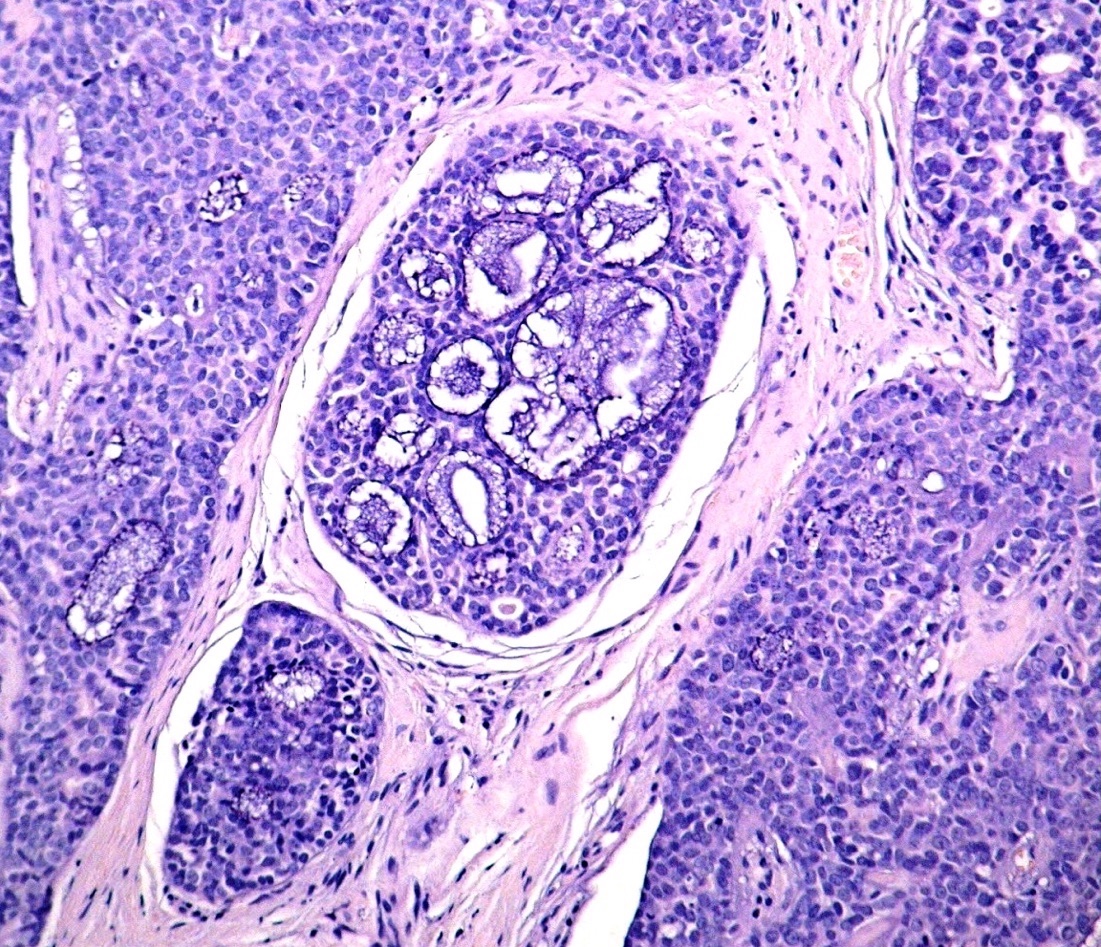
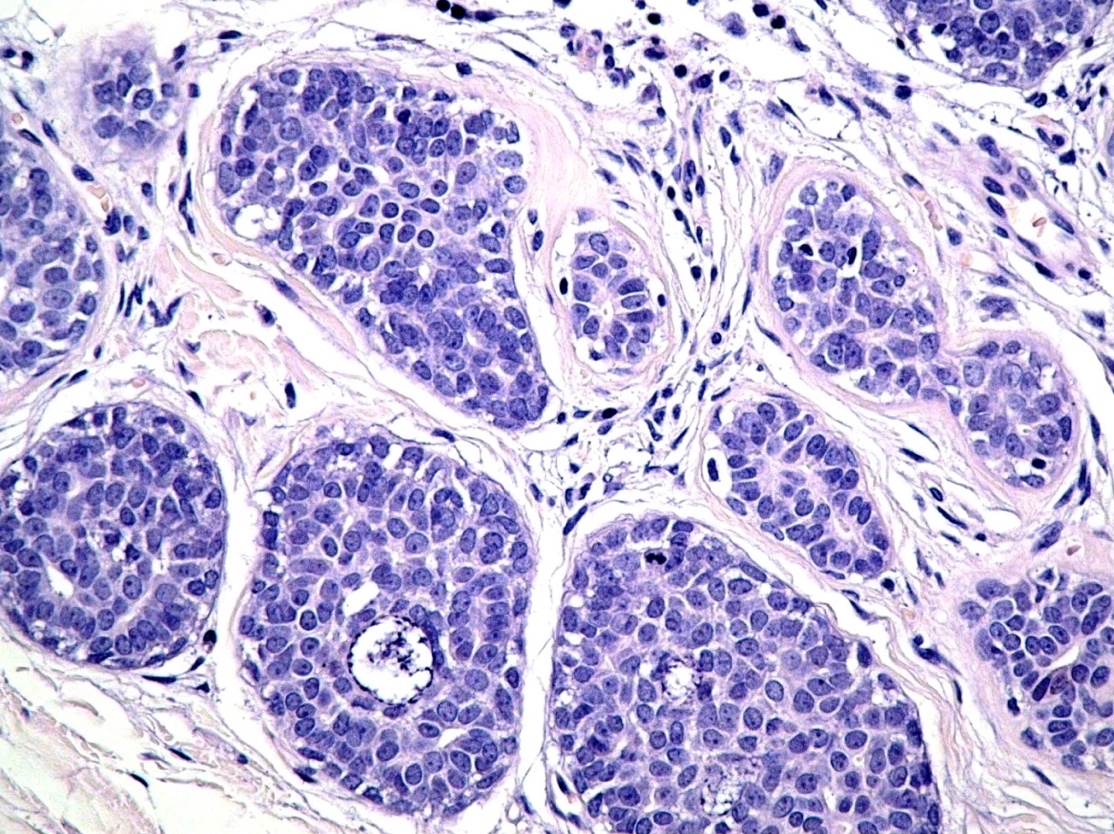
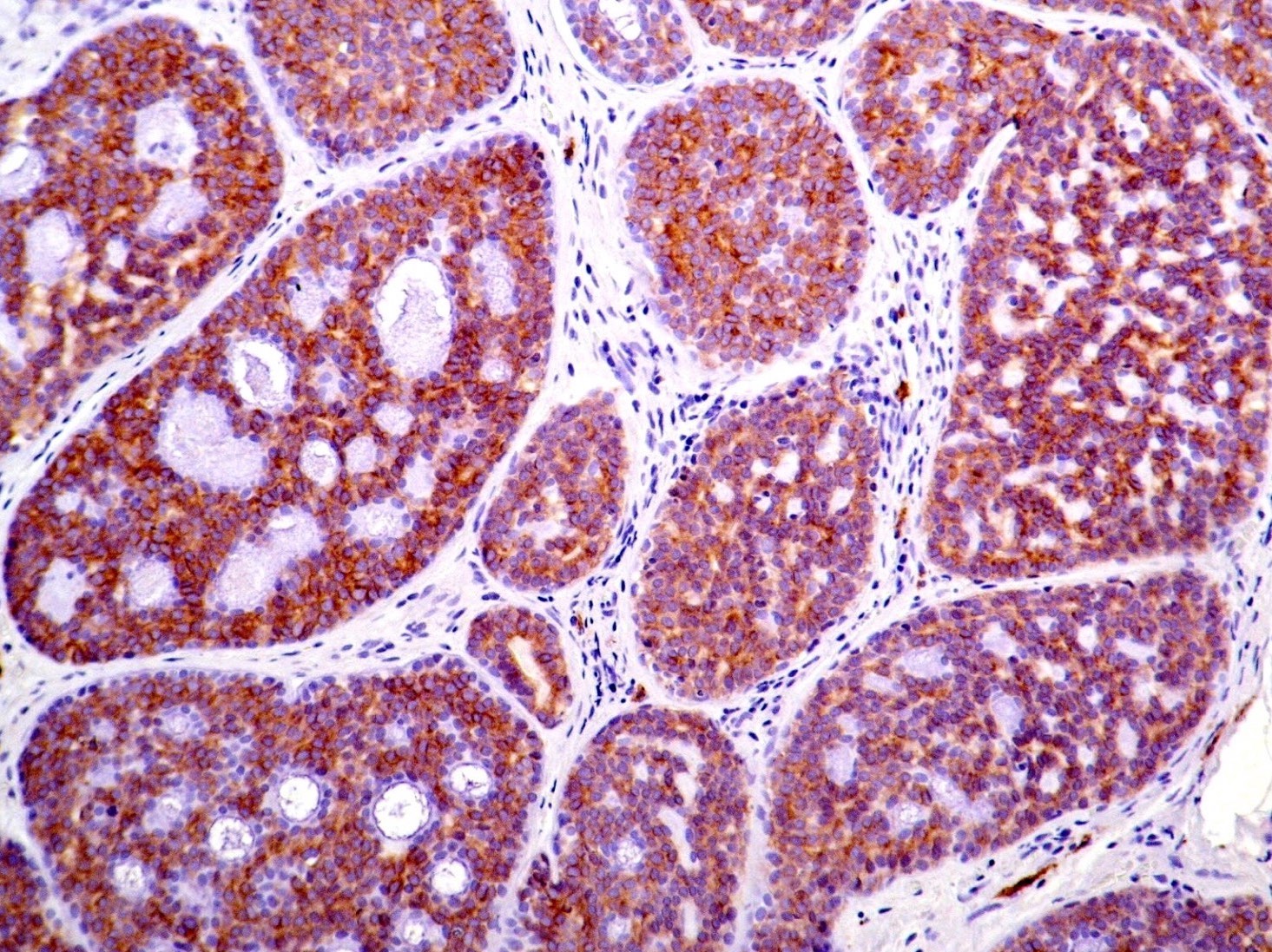
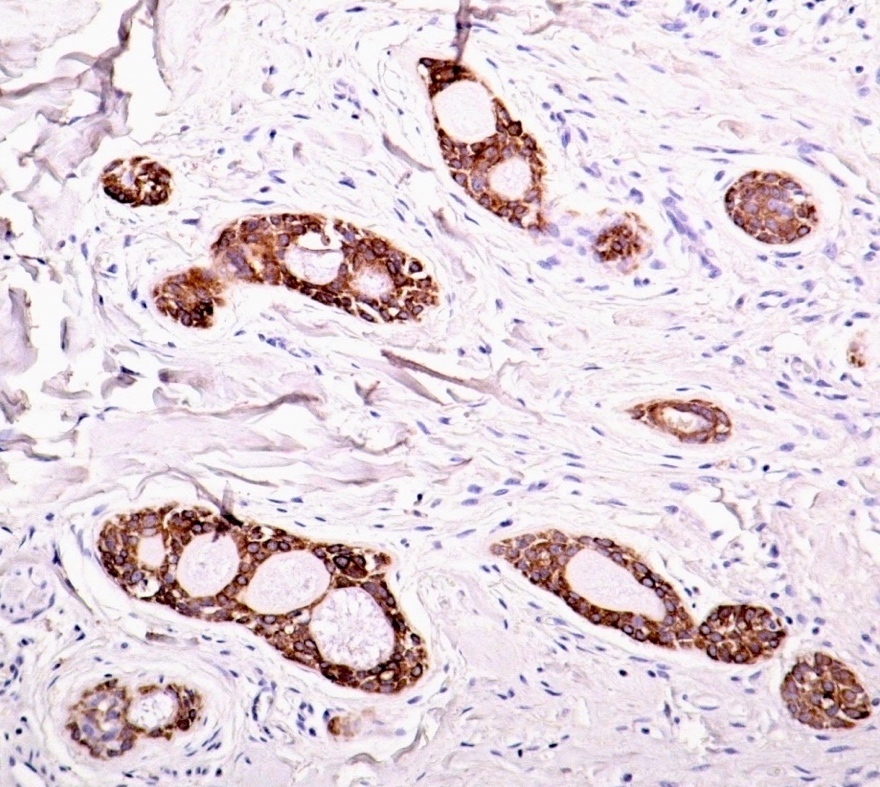
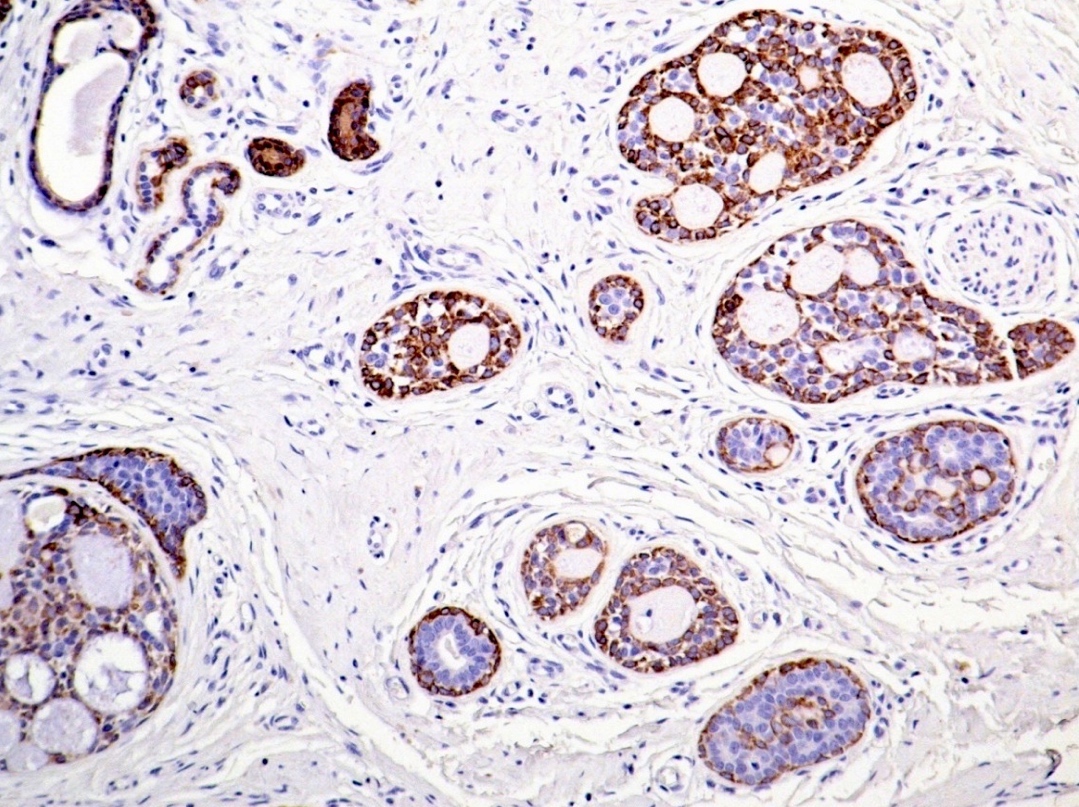
Contributed by Carlos C. Diez Freire, M.D.
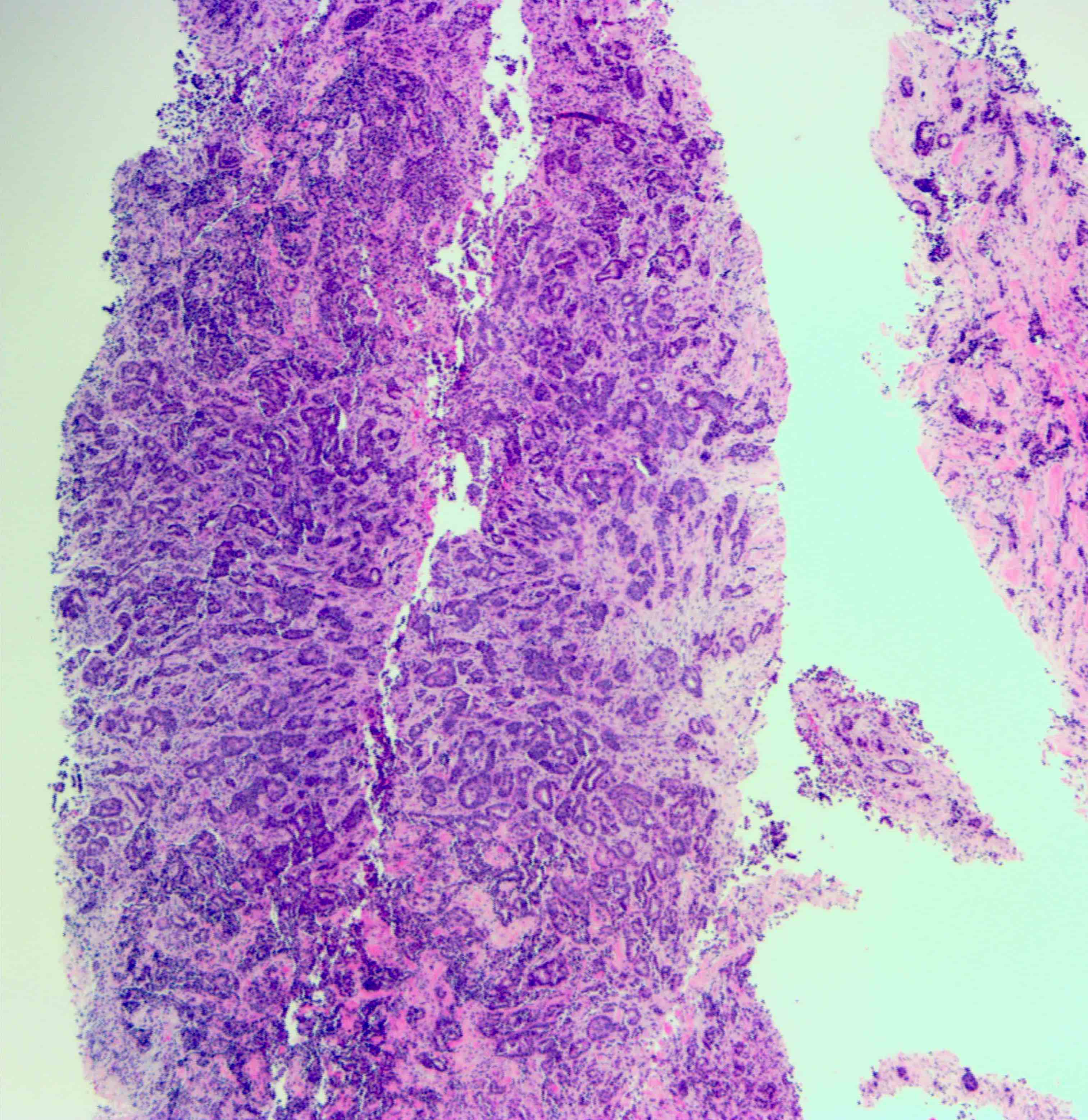

Male invasive ductal carcinoma

ER
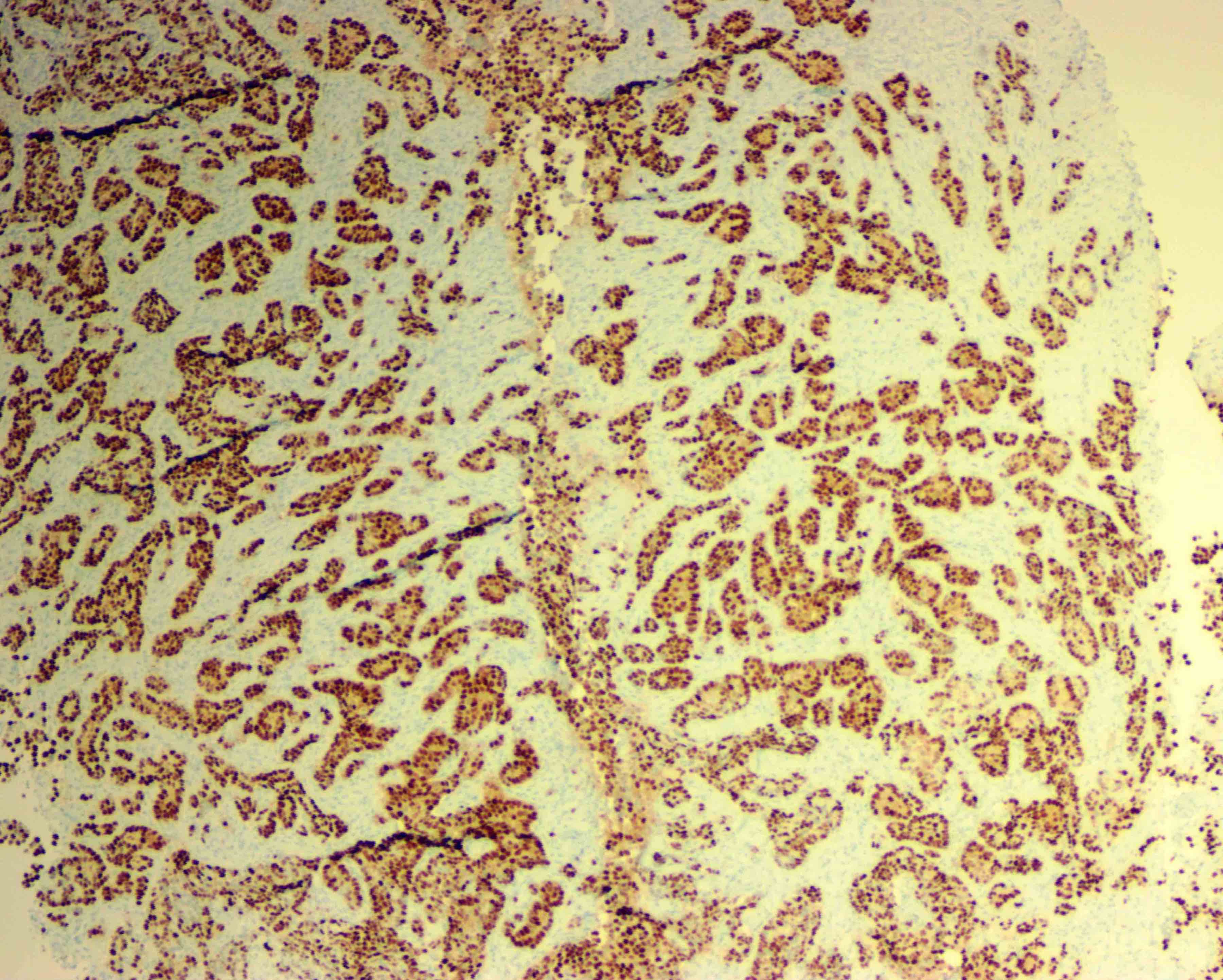
PR
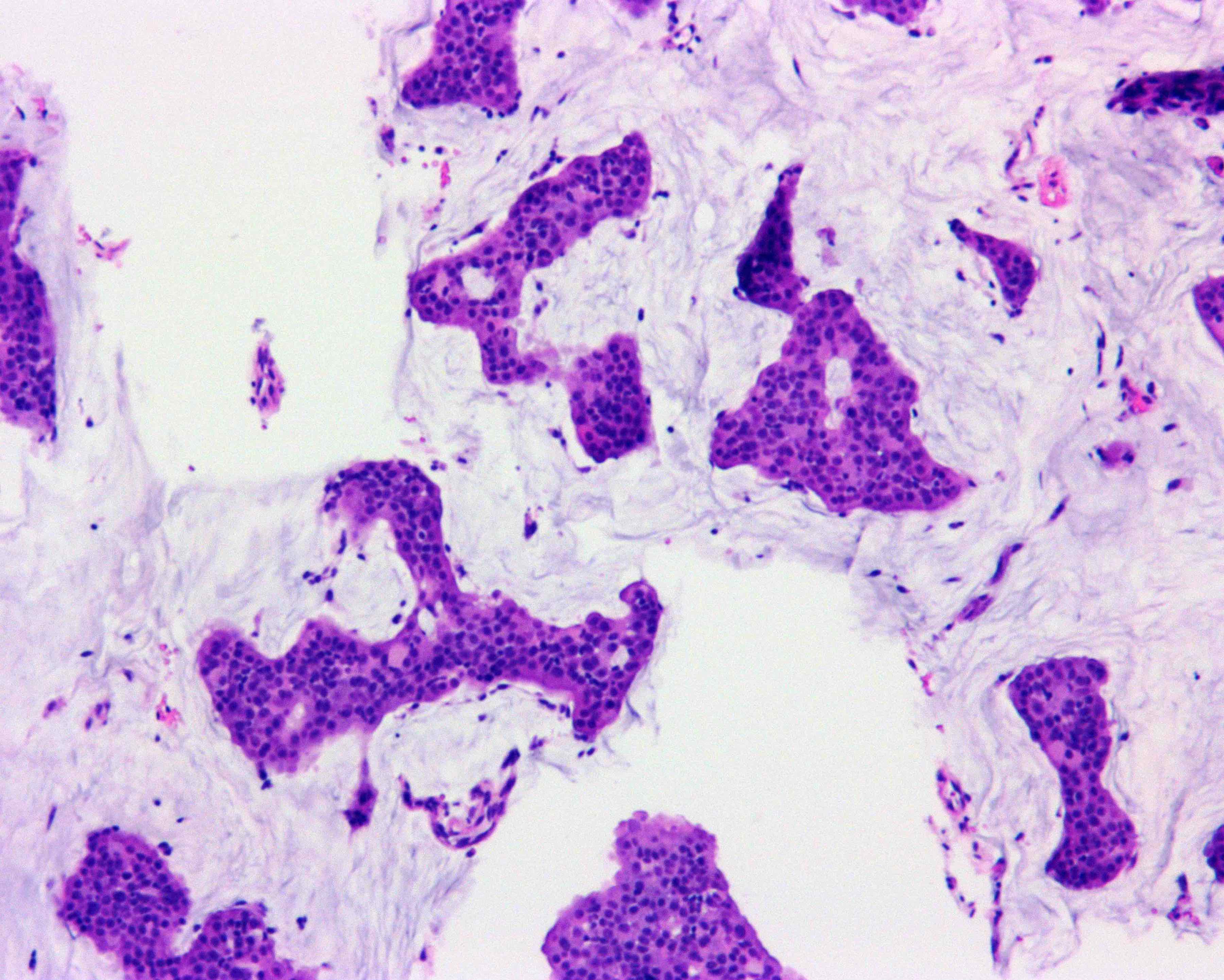
Male mucinous carcinoma
Lymph node metastasis, mucinous

Male mucinous carcinoma, ER
Male mucinous carcinoma, PR
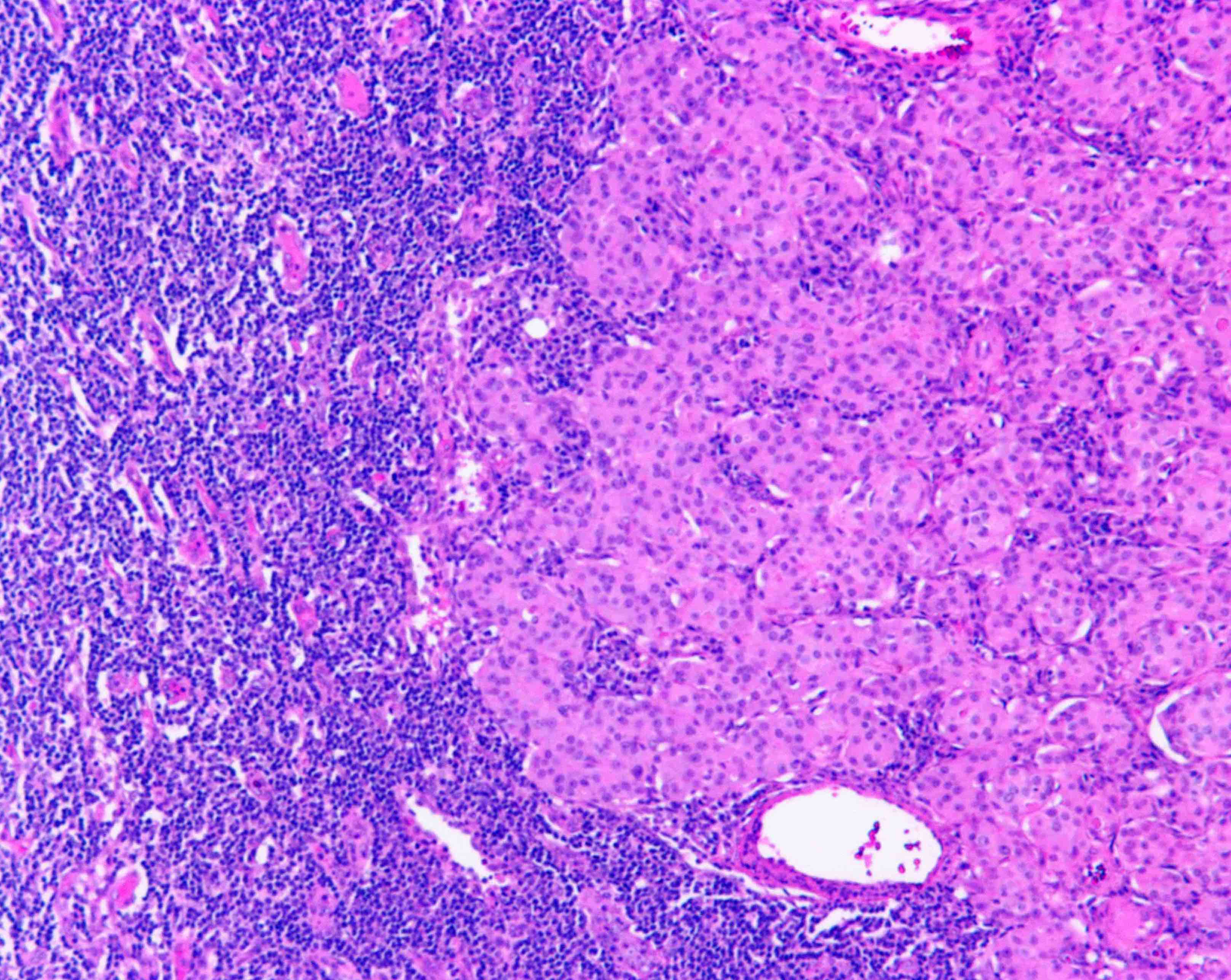
Contributed by Semir Vranić, M.D., Ph.D.
Man with adenoid cystic carcinoma
c-kit
CK14
Cytology description
- Reliable but underused
- Dispersed epithelial cells with atypical features and high N/C ratio
- Cell clusters can be present in papillary tumors
- Gynecomastia present with sparsely cellular aspirate with loosely cohesive sheets of cells
Positive stains
Negative stains
- HER2 (usually)
Molecular / cytogenetics description
- p53 mutations in exon 6 found in over 90% of male cases compared to 33% of females with p53 mutations in exon 5 and 6 (Neoplasma 1996;43:305)
- Gene expression performed in 66 male breast cancer tumors revealed 2 unique subgroups (luminal M1 and M2) that were different in biologic features and outcome when compared to female breast cancers (Breast Cancer Res 2012;14:R31)
- EGFR and CCND1 genes are amplified more in male than female breast cancers
- High methylation status of MSH6, WT1, PAX5, PAX6, GATA5 and CDH13 correlates with more aggressive phenotype and poor survival
- Male and female breast cancers share many of these methylated genes but many genes are less frequently methylated in males
- Methylation of RASSF1A (downregulation of ER alpha and micro RNAs) is more common in male than female breast carcinomas
Differential diagnosis
- Gynecomastia: especially with radiation induced changes
Additional references
Board review style question #1
What is the most common type of male breast carcinoma?
- Invasive lobular carcinoma
- Invasive papillary carcinoma
- Mucinous carcinoma
- Poorly differentiated invasive ductal carcinoma
- Well differentiated invasive ductal carcinoma
Board review style answer #1
D. Poorly differentiated invasive ductal carcinoma. Approximately 85% of male breast carcinomas are poorly differentiated infiltrating ductal carcinomas, followed by papillary carcinomas and other forms similar to those found in female breast cancer. Lobular carcinomas represent 2% of cases.
Comment Here
Reference: Male invasive breast carcinoma
Comment Here
Reference: Male invasive breast carcinoma
