
Breast
Inflammatory / infectious
Acute mastitis / abscess
Author: Kristen E. Muller, D.O.
Editorial Board Member: Julie M. Jorns, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 11 January 2021
Last staff update: 19 May 2022
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Acute mastitis breast abscess


Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Positive stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Muller, KE. Acute mastitis / abscess. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/breastacutemastitis.html. Accessed April 2nd, 2025.
Definition / general
- Infection or inflammation of breast tissue, usually bacterial, often seen in association with lactation
- If untreated, may form abscess and fistulous tracts
Essential features
- Infection or inflammation of breast tissue, usually bacterial, often seen in association with lactation
- If untreated, may form abscess and fistulous tracts
- Staphylococcus aureus most common organism
- Microscopic examination reveals a mixed dense inflammatory infiltrate, predominantly neutrophils, in breast tissue
Terminology
- Puerperal mastitis
ICD coding
- ICD-10:
- ICD-11:
Epidemiology
- Incidence in 2 - 33% of lactating women (Am J Epidemiol 2002;155:103, Med Microbiol Immunol 2018;207:83)
- 3% with mastitis have an abscess (BJOG 2004;111:1378)
- Risk factors: age (21 - 35 years old), mastitis with previous child, cracked or sore nipples, use of ointments, incorrect breastfeeding practices, peripartum antibiotic therapy (Med Microbiol Immunol 2018;207:83)
Sites
- Subareolar (nonpuerperal)
Pathophysiology
- Infection via the mammary duct system; typically occurs within 2 - 3 weeks after the start of lactation (Breastfeed Med 2014;9:239)
- Staphylococcus aureus is most common organism transmitted from skin or infant (Breastfeed Med 2014;9:239)
- Accumulation of inadequately drained milk in ducts and lobules creates a microenvironment that fosters bacterial growth (Hoda: Rosen’s Breast Pathology, 4th Edition, 2014)
- Infrequent complication is abscess formation (localized collection of purulent material)
- Milk samples show loss of bacterial diversity (J Hum Lact 2015;31:406)
- Subareolar or nonpuerperal abscesses most often a consequence of squamous metaplasia of lactiferous ducts (SMOLD) (J Pathol Transl Med 2015;49:279)
Etiology
- Associated with lactation and cracks in nipple
- Common scenarios: infrequent feeding, oversupply of milk, rapid weaning, illness in mother or child, clogged duct (J Hum Lact 1998;14:101)
- Also associated with eczema, nipple dermatoses and postreduction mammoplasty
- Bacteria often not isolated from culture
- Pregnancy related infections are usually due to Staphylococcus
- Usually unilateral, often methicillin resistant Staphylococcus aureus (MRSA) (Arch Surg 2007;142:881, Asian J Surg 2009;32:55)
- Also Staphylococcus epidermidis (BMC Microbiol 2009;9:82, J Hum Lact 2015;31:406)
- Streptococcus usually causes diffuse infections leading to scarring but is uncommon today (J Hum Lact 2020;890334420965147)
- Tuberculosis may occur in endemic areas (Med Princ Pract 2009;18:245, Int J Infect Dis 2019;87:135)
- Nonpregnancy related infections may be polymicrobial or associated with diabetes (Am J Med Sci 2009;338:123)
Clinical features
- Erythema, swelling, firmness, breast pain, fever, malaise, decreased milk outflow
- Abscess: well circumscribed fluctuant mass in addition to above features
- African Americans may have higher risk of abscess formation (World J Surg 2009;33:2582)
- Obesity (BMI > 30) and smoking risk factors for abscess (World J Surg 2009;33:2582)
- Zuska disease (periductal mastitis): clinical scenario of recurring subareolar abscesses and sinus formation (Am J Surg 1951;81:312)
- Fungal mastitis: rare
- Actinomycosis may develop in nipple and form a sinus tract
- Candida infection may interfere with breast feeding but Candida albicans is not present in milk ducts in women with clinical symptoms of ductal candidiasis (Breastfeed Med 2009;4:57)
Diagnosis
- Based on history and clinical findings
- Ultrasound preferred imagining modality (Radiol Bras 2020;53:405)
- Biopsy may be warranted for suspected abscess, atypical presentation, recurrent infection or treatment failure; Gram stain and culture (aerobic and anaerobic) with sensitivities to guide antibiotic selection (rarely needed)
- FNA can be used to drain (Am Fam Physician 2008;78:727)
Radiology description
- Ultrasound (preferred modality): abscess shows hypoechoic lesion of purulent material, well circumscribed, macrolobulated, irregular or ill defined with septa and thick echogenic rim (Radiographics 2011;31:1683, Radiographics 2007;27 Suppl 1:S101)
- Mammography of limited value due to nonspecific findings
Radiology images
Contributed by Kristen E. Muller, D.O.

Ultrasound hypoechoic process
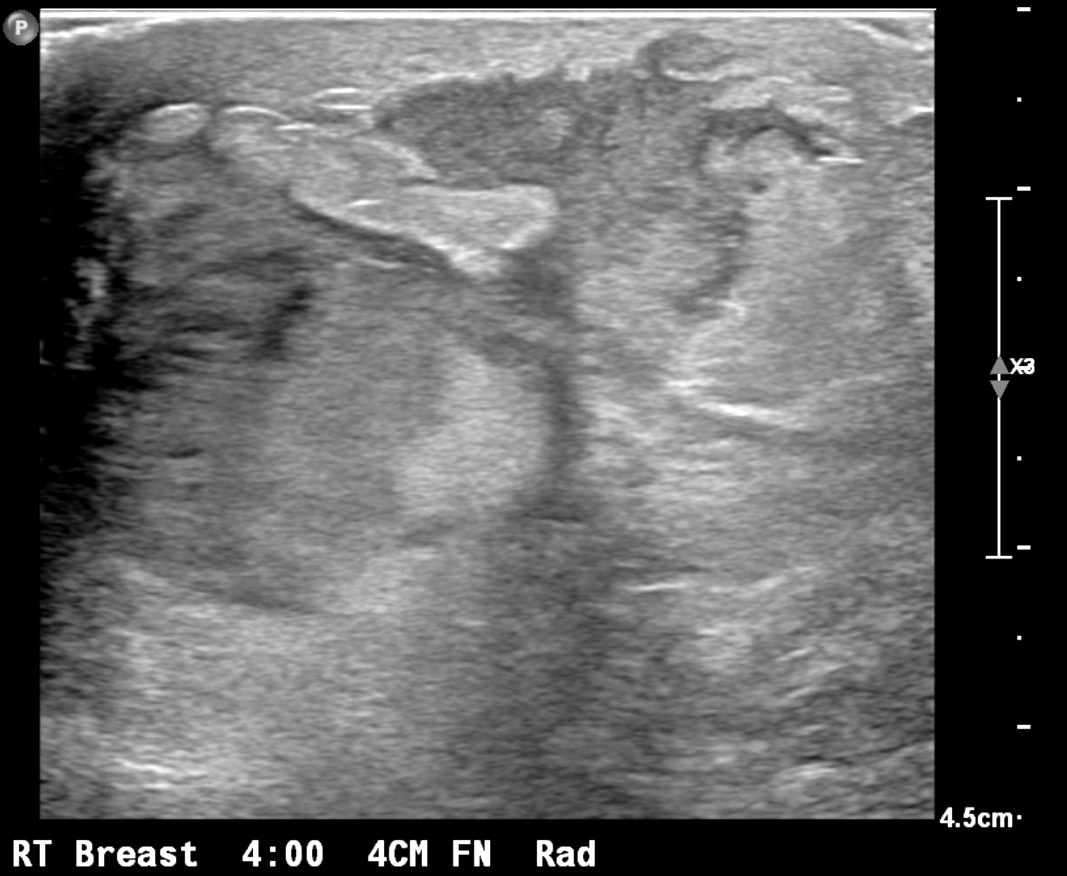
Ultrasound irregular fluid collection
Prognostic factors
- Recurrent breast abscesses are more likely to be smokers and have mixed bacterial and anaerobic infections (World J Surg 2009;33:2582)
Case reports
- 16 year old girl with MRSA abscess and toxic shock syndrome (Oxf Med Case Reports 2019;2019:omz054)
- 21 year old lactating woman with Listeria breast abscess (Cureus 2017;9:e1006)
- 22 year old woman with endogenous endophthalmitis secondary to mastitis (Indian J Ophthalmol 2020;68:2595)
- 30 year old woman with Mycobacterium fortuitum abscess following breast nipple piercing (IDCases 2020;21:e00847)
- 31 year old woman with tubercular mastitis mimicking malignancy (Prague Med Rep 2020;121:267)
- 32 year old nonlactating woman with Neisseria gonorrhoeae mastitis and abscess (IDCases 2019;18:e00620)
- 36 year old woman with Histoplasma capsulatum causing granulomatous mastitis (Arch Pathol Lab Med 2006;130:e1)
- 39 year old woman with nonpuerperal breast abscess due to Prevotella bivia (Clin Case Rep 2020;8:1399)
- 48 year old woman with Salmonella enteritidis breast abscess (BMJ Case Rep 2018;2018:bcr2018226075)
- 52 year old man with Trichophyton rubrum causing bilateral male breast enlargement (Breast 2006;15:263)
- 55 year old diabetic woman with Fusarium (Indian J Med Microbiol 2005;23:198)
- Report of saline filled breast implants contaminated with Curvularia in 5 patients (J Infect Dis 2005;192:170)
- Immunosuppressed patient with breast nodule due to coccidiomycosis (Arch Pathol Lab Med 1991;115:1064)
- Cryptococcus in HIV+ patient (J Infect 2008;57:82)
- 2 cases of Histoplasma capsulatum causing granulomatous mastitis (Hum Pathol 1989;20:47)
- Young woman who had nipples pierced, presented with right breast pain, erythema and drainage (Case of the Month #515)
Treatment
- Symptomatic treatment: effective milk removal via breastfeeding, pumping or hand expressing to fully empty breasts, analgesia, warm compress (Am Fam Physician 2008;78:727)
- Kneading and dispersing manipulation for early stage disease (Zhong Xi Yi Jie He Xue Bao 2009;7:1130)
- Antibiotics targeting Staphylococcus species are mainstay of treatment, although effectiveness is debated (J Hum Lact 2008;24:311, Cochrane Database Syst Rev 2013:CD005458)
- Aspiration or incision and drainage; now considered last resort for abscess management (Radiographics 2011;31:1683, Expert Rev Anti Infect Ther 2014;12:753)
- Urokinase irrigation may be useful for large abscesses (J Ultrasound Med 2009;28:449)
- Ultrasound guided drainage (Radiology 2004;232:904, Br J Radiol 2005;78:186)
- Probiotics (Benef Microbes 2014;5:169, Appl Environ Microbiol 2008;74:4650, Clin Infect Dis 2010;50:1551)
Clinical images
Contributed by Ayesha Farooq, M.B.B.S. and Julie Jorns, M.D. (Case #515)

Nipple piercing related infection
Images hosted on other servers:

Mastitis and breast abscess

Lactational abscess
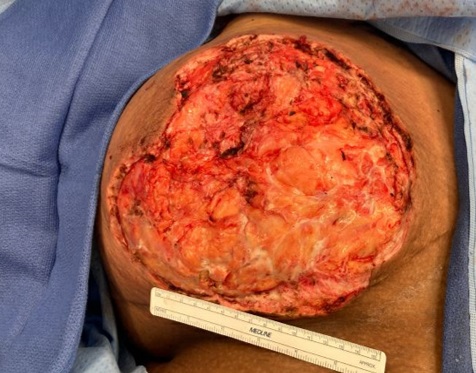
Gross description
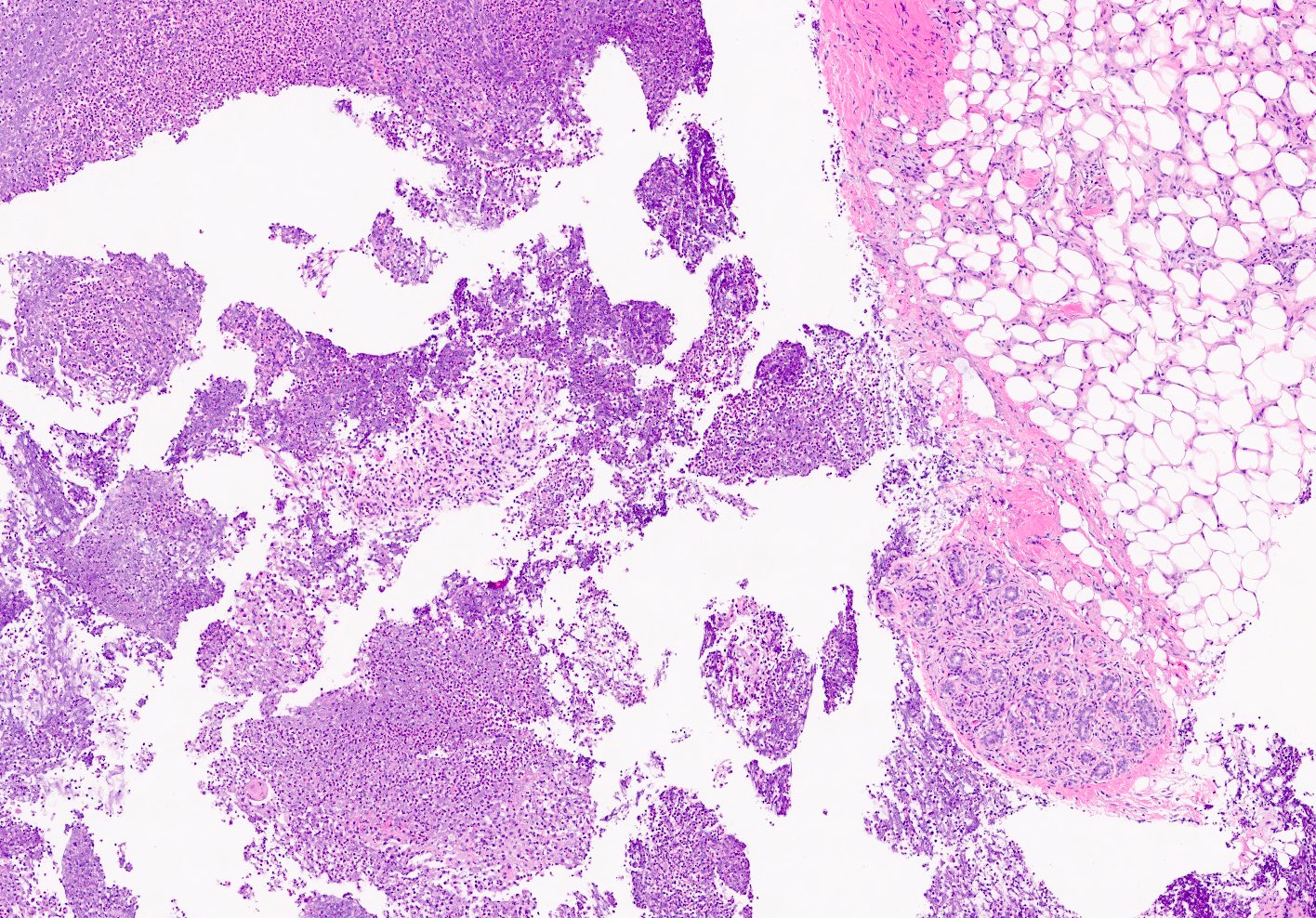
- Excisions rare; specimens usually from incision and drainage procedures and typically received in fragments
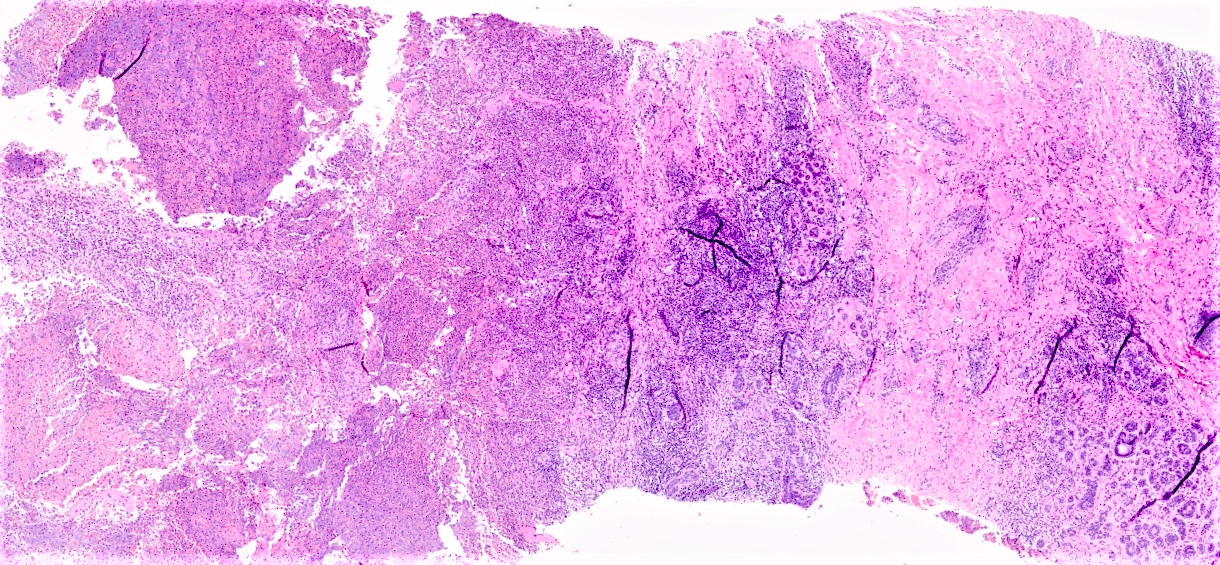
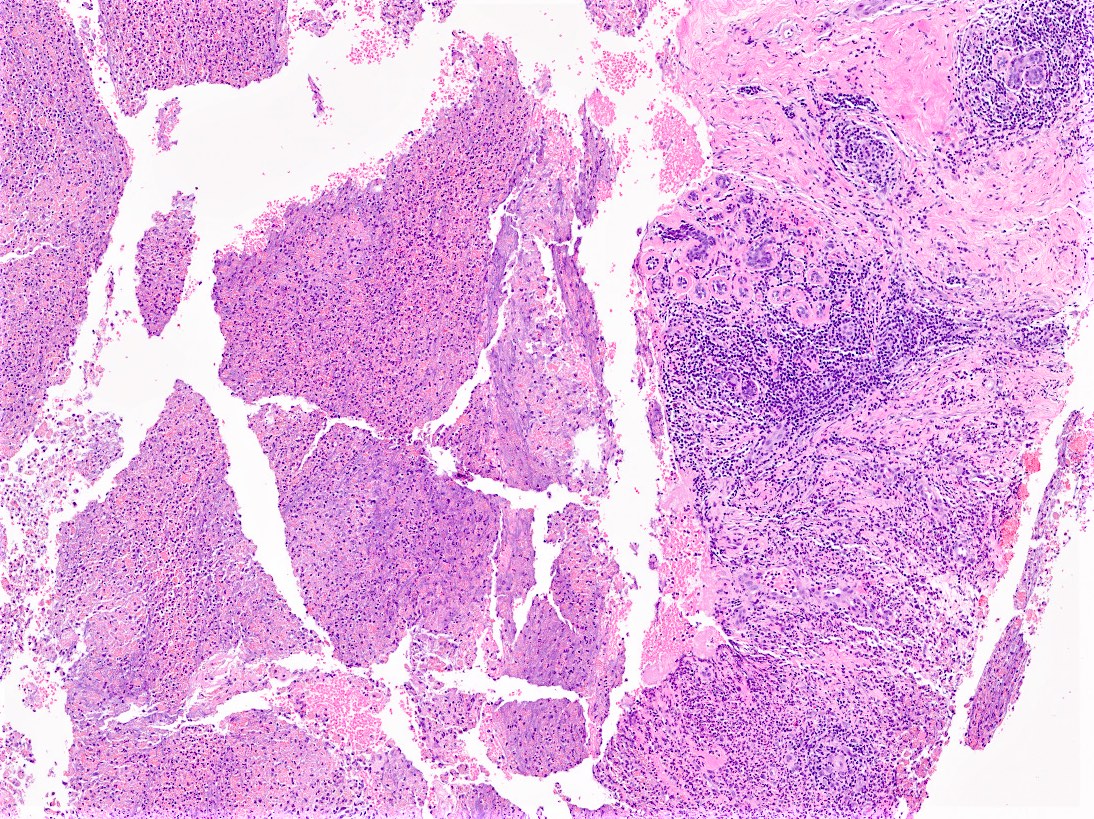
Microscopic (histologic) description
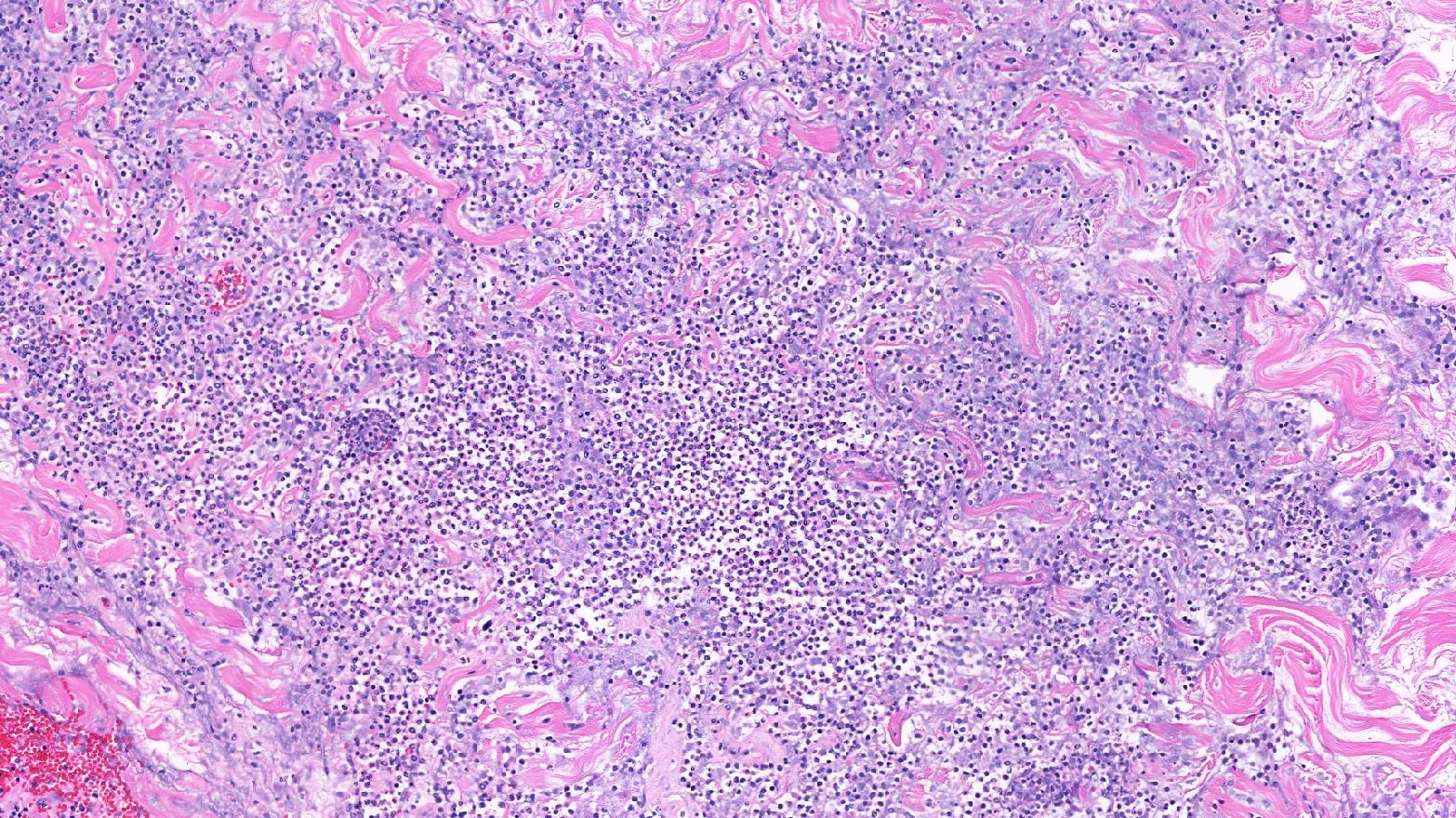
- Mixed dense inflammatory infiltrate, predominantly neutrophils, in breast tissue
- May obscure underlying normal breast tissue
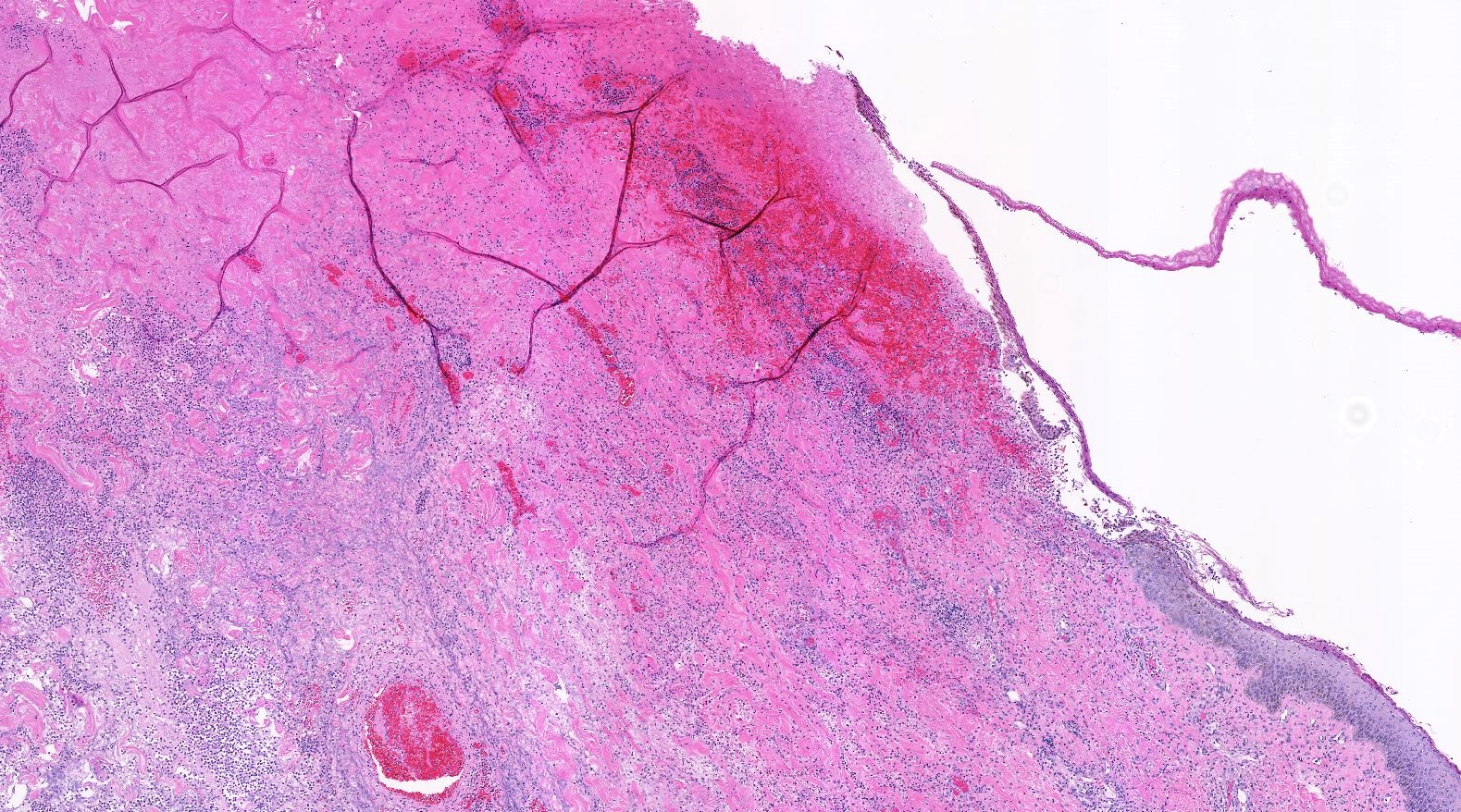
- Tissue necrosis may be present
- Gram stain for microorganisms may reveal bacterial forms (gram positive cocci) associated with neutrophilic infiltrate
- Granulation tissue and chronic inflammation with resolution
- Lymphocytes, giant cells and granulomas are not typical (J Pathol Transl Med 2015;49:279)
Microscopic (histologic) images
Contributed by Kristen E. Muller, D.O.
Acute mastitis and abscess
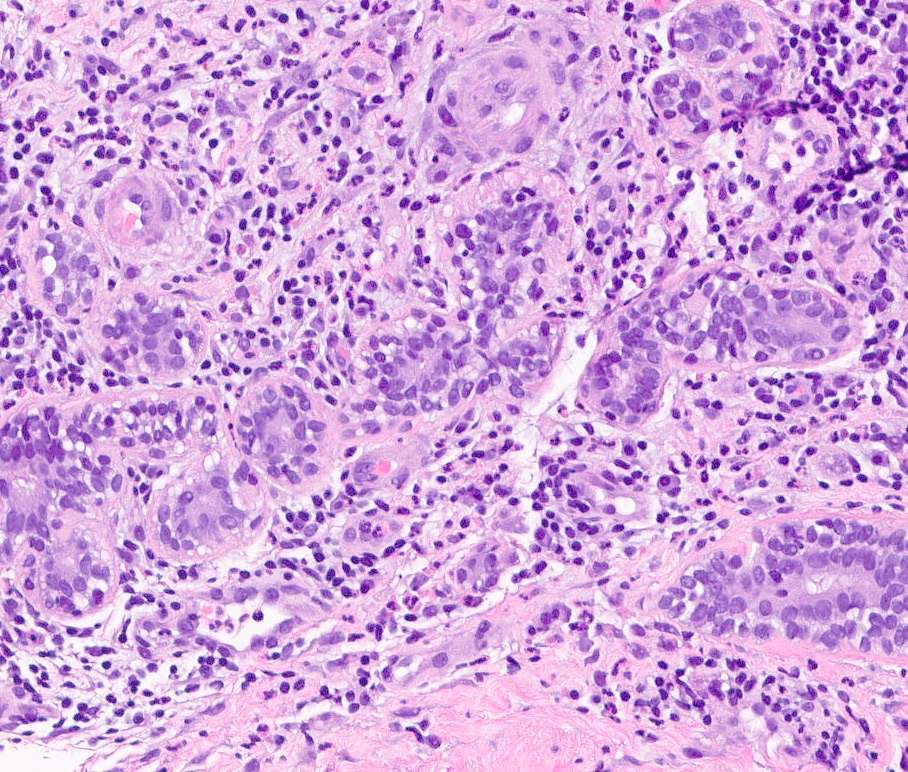
Lobular inflammation
Dense inflammatory infiltrate
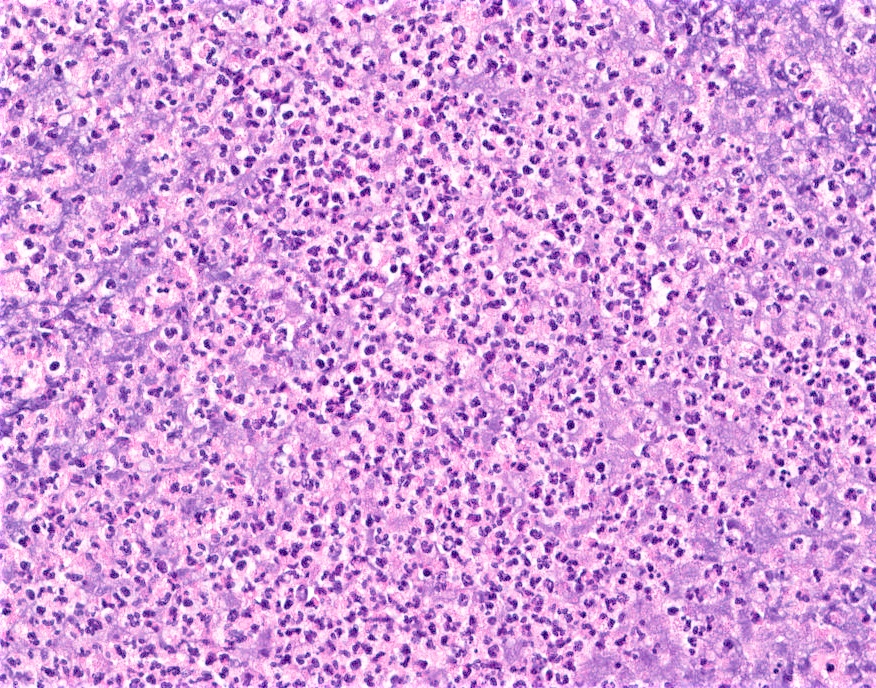
Dense neutrophilic infiltrate
Contributed by Ayesha Farooq, M.B.B.S. and Julie Jorns, M.D. (Case #515)

Nipple piercing related infection
Virtual slides
Images hosted on other servers:

Breast abscess and necrosis
Cytology description
- Background of acute inflammation and necrotic debris (Cytopathology 1992;3:281)
Positive stains
- Gram stain may highlight Gram positive bacterial forms
Sample pathology report
- Right breast, core needle biopsy:
- Breast tissue with abundant acute inflammation and bacterial forms identified on Gram stain (see comment)
- Comment: The histologic findings are compatible with acute mastitis and abscess formation in the appropriate clinical context. Clinical correlation and correlation with microbiology studies (if performed) is recommended.
Differential diagnosis
- Squamous metaplasia of lactiferous ducts (SMOLD):
- Subareolar location
- Lactiferous ducts with squamous metaplasia
- Multinucleated giant cells associated with keratin debris
- Strong association with smoking
- Fat necrosis:
- Infarcted adipocytes, lipid laden macrophages, foreign body giant cell reaction
- Initially acute inflammatory infiltrate may be present, chronic inflammation predominates in older lesions
- History of surgery, prior biopsy, radiation, trauma
- Idiopathic granulomatous mastitis:
- Granulomatous inflammation (lymphocytes, plasma cells, histiocytes, multinucleated giant cells)
- Lobulocentric pattern, may obliterate lobules
- May have neutrophils forming microabscesses surrounding empty microcysts; features overlap with cystic neutrophilic granulomatous mastitis, which may have gram positive bacilli within microcysts (Corynebacterium)
- Duct ectasia:
- Foamy histiocytes within lumen and within wall and epithelium of ducts, periductal fibrosis
- Inflammatory cells typically chronic; acute inflammatory infiltrate rarely present
Additional references
Board review style question #1
What is the most appropriate diagnosis for this breast biopsy from a 32 year old postpartum woman?
- Acute mastitis
- Duct ectasia
- Fat necrosis
- Idiopathic granulomatous mastitis
- Invasive lobular carcinoma
Board review style answer #1
Board review style question #2
Which of the follow is true regarding acute mastitis?
- Abscess may form as a complication if left untreated
- Acute mastitis typically occurs in postmenopausal women
- Granulomas are common
- Most common organism isolated is Streptococcus species
Board review style answer #2
A. Abscess may form as a complication if left untreated
Comment Here
Reference: Acute mastitis / abscess
Comment Here
Reference: Acute mastitis / abscess
Board review style question #3
What is a common causative microorganism associated with nipple piercing related infection?
- Salmonella
- Shigella
- Staphylococcus
- Stenotrophomonas
Board review style answer #3
