

Bone & joints
Other chondrogenic tumors
Osteochondroma
Authors: Jose G. Mantilla, M.D., Robert Ricciotti, M.D.
Editorial Board Member: Borislav A. Alexiev, M.D.


Last author update: 29 December 2020
Last staff update: 19 January 2022
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Osteochondroma[TI] bone pathology "free full text"[SB]

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Mantilla JG, Ricciotti R. Osteochondroma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/boneosteochondroma.html. Accessed January 11th, 2025.
Definition / general
- Benign bone surface tumor composed of mature bone with a cartilage cap
- May be solitary or occur as multiple hereditary exostoses (MHE)
Essential features
- Exophytic lesion of bone surface composed of a stalk of mature bone with a cartilaginous cap; the marrow space / cancellous bone of the stalk communicates with that of the underlying bone
Terminology
- Osteocartilaginous exostosis
ICD coding
- ICD-O: 9210/0 - Osteochondroma
- ICD-11: 2E83.Y & XH5Y87 - Other specified benign osteogenic tumors and osteochondroma
Epidemiology
- Common, approximately 35% of benign bone tumors and 10% of all bone tumors
- Predominance in men (M:F = 2:1)
- Most cases diagnosed in the first 2 decades of life
Sites
- Most common in the metaphysis of long bones: femur > humerus > tibia
- Involvement of flat bones (ilium, scapula) may occur
- Involvement of small bones of the hands and feet, ribs and vertebra is rare
Etiology
- Both solitary sporadic tumors and multiple hereditary exostoses (MHE) are associated with loss of function mutations in EXT1 (8q24) and EXT2 (11p11) genes (J Genet 2015;94:749)
- In solitary lesions, EXT gene inactivation is restricted to the cartilage cap and is somatic
- MHE shows autosomal dominant inheritance (Am J Hum Genet 1998;62:346); patients have heterozygous germline EXT1/EXT2 mutation, while their tumors usually show homozygous EXT mutation
Clinical features
- Often asymptomatic (J Bone Oncol 2017;8:23, In Vivo 2008;22:633)
- May cause symptoms due to fracture, growth or impingement of other structures (J Bone Oncol 2017;8:23, In Vivo 2008;22:633)
- Multiple lesions can occur in the setting of MHE (J Bone Oncol 2017;8:23, In Vivo 2008;22:633)
Diagnosis
- Radiologic pathologic correlation is often specific
- Secondary chondrosarcoma:
- Histologic features alone are usually not definitive for diagnosis
- Diagnosis of secondary chondrosarcoma arising in osteochondroma can be challenging and requires correlation with clinical and imaging findings (Mod Pathol 2012;25:1275, Radiology 2010;255:857, Oncogene 2012;31:1095)
- Tumor growth and thickening of the cartilage cap (usually > 2 cm) are suggestive of malignant transformation in skeletally mature patients
Radiology description
- Pedunculated or sessile
- Mature bony stalk continuous with the cortex; cancellous bone of stalk communicates with that of underlying bone
- Thin, lobulated cartilaginous cap, which may contain calcifications
- Growth perpendicular to the long axis of the bone
Radiology images
Contributed by Jose G. Mantilla, M.D., Mark R. Wick, M.D. and AFIP images
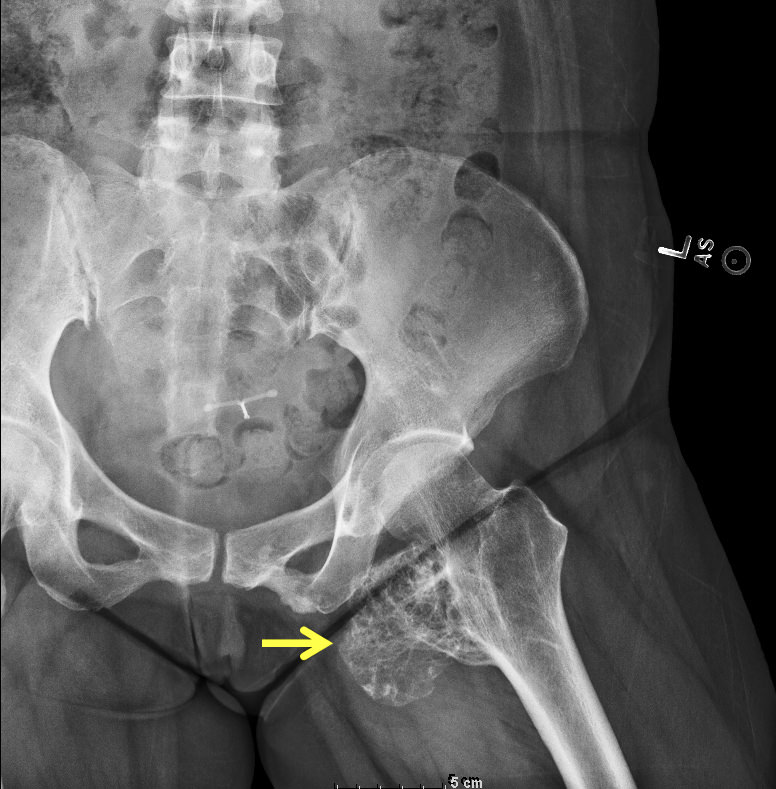
Osteochondroma arising in the proximal femur

Osteochondroma arising in the distal femur

Distal portion of femur

Metatarsal Xray

Xray
Prognostic factors
- Osteochondroma is a benign tumor (J Bone Oncol 2017;8:23, In Vivo 2008;22:633)
- Malignant transformation may occur as secondary chondrosarcoma and are usually a grade 1 to 2 conventional chondrosarcoma (J Bone Oncol 2017;8:23, In Vivo 2008;22:633)
- Solitary lesions have at most 1 - 2% risk of malignant transformation (J Bone Oncol 2017;8:23, In Vivo 2008;22:633)
- Multiple osteochondromas in the setting of MHE have a higher risk of malignant transformation (5 - 25% overall) (J Bone Oncol 2017;8:23, In Vivo 2008;22:633, Orphanet J Rare Dis 2008;3:3)
- Secondary chondrosarcomas are usually grade 1 - 2 conventional chondrosarcoma (J Bone Oncol 2017;8:23, In Vivo 2008;22:633)
Case reports
- 12 year old girl with minute mesenchymal chondrosarcoma within osteochondroma (Hum Pathol 2018;81:255)
- 15 year old boy with painless lump in the arm (radiology) (BMJ 2016;354:i4503)
Treatment
- Growth often stops after skeletal maturity and may spontaneously regress
- Excision is typically curative in solitary lesions, with rare local recurrence
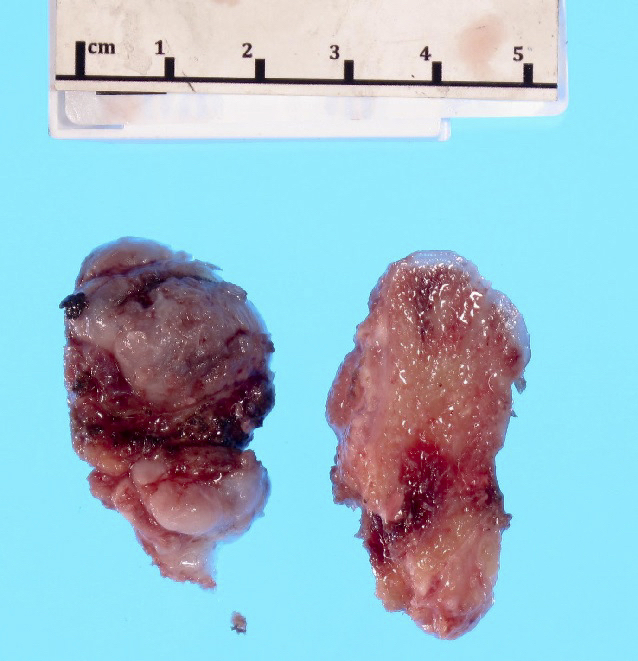
Gross description
- Pedunculated or sessile bony lesion with hyaline cartilage cap
Gross images
Contributed by Jose G. Mantilla, M.D. and AFIP images
Hyaline cartilage cap
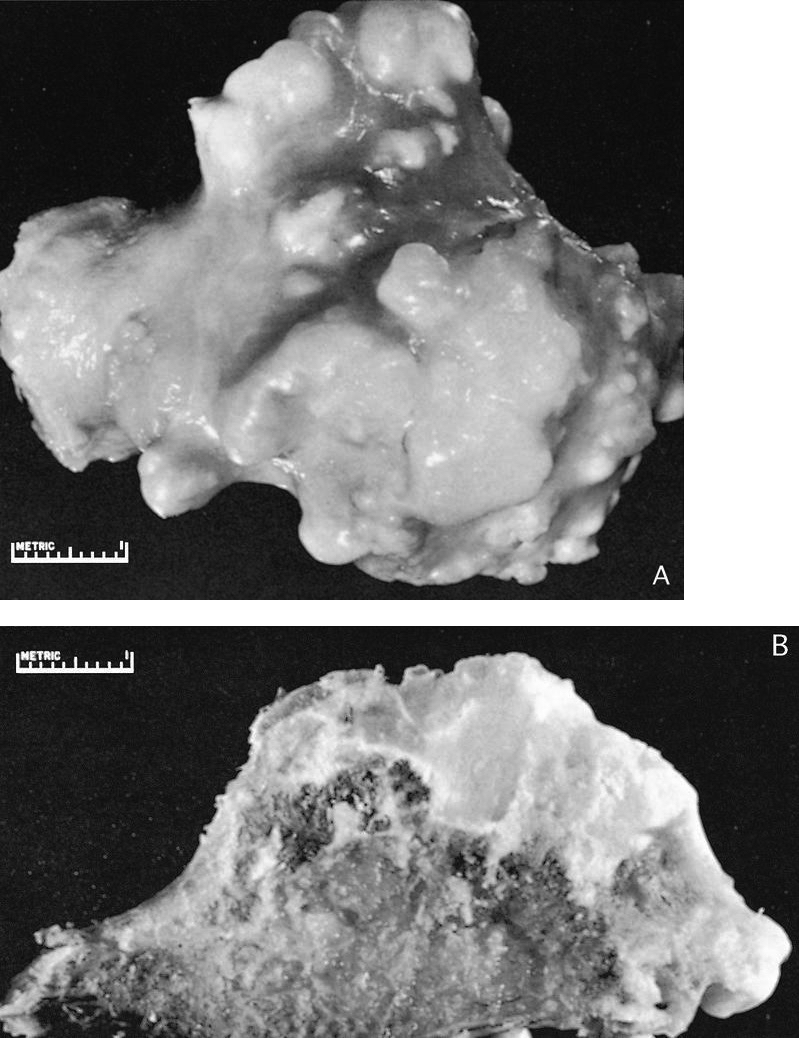
Outer and cut surfaces
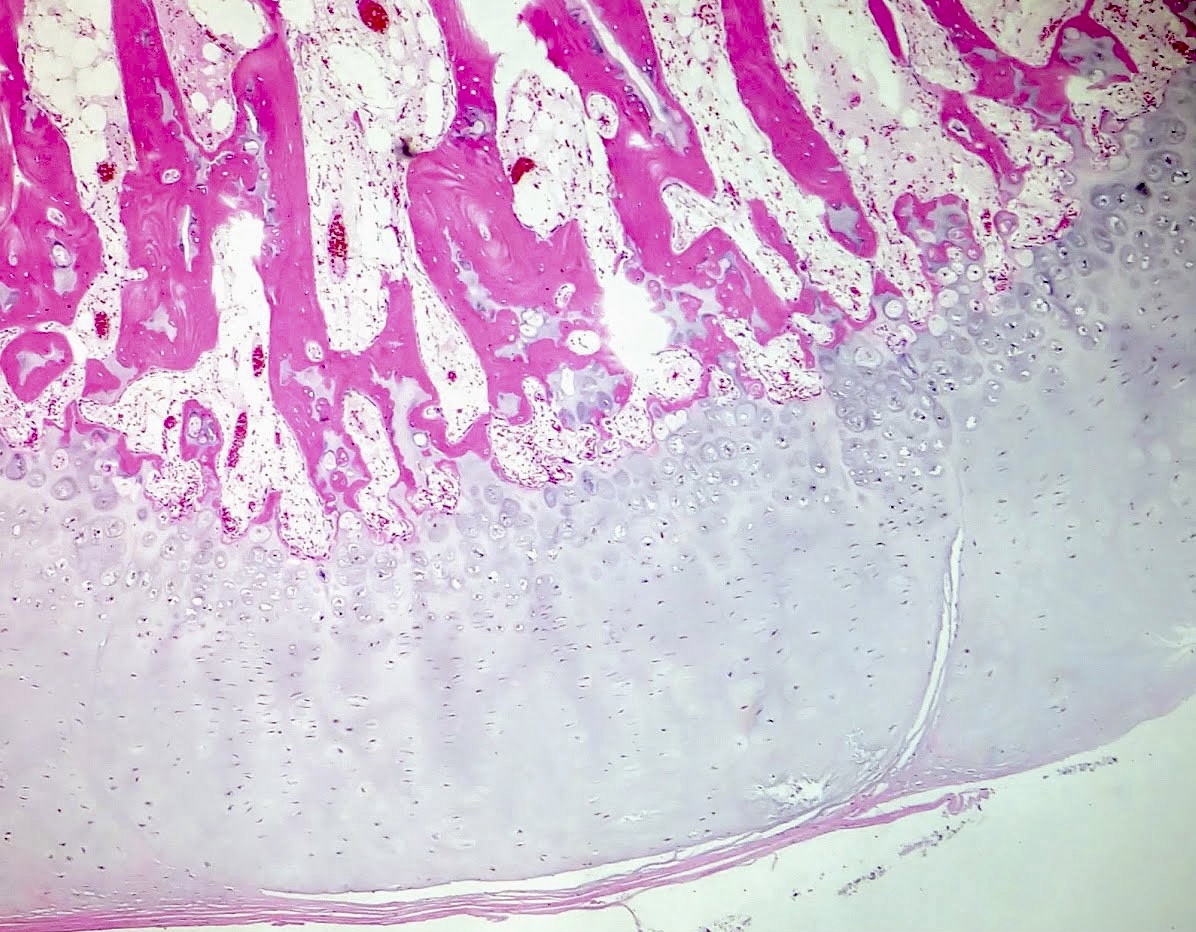
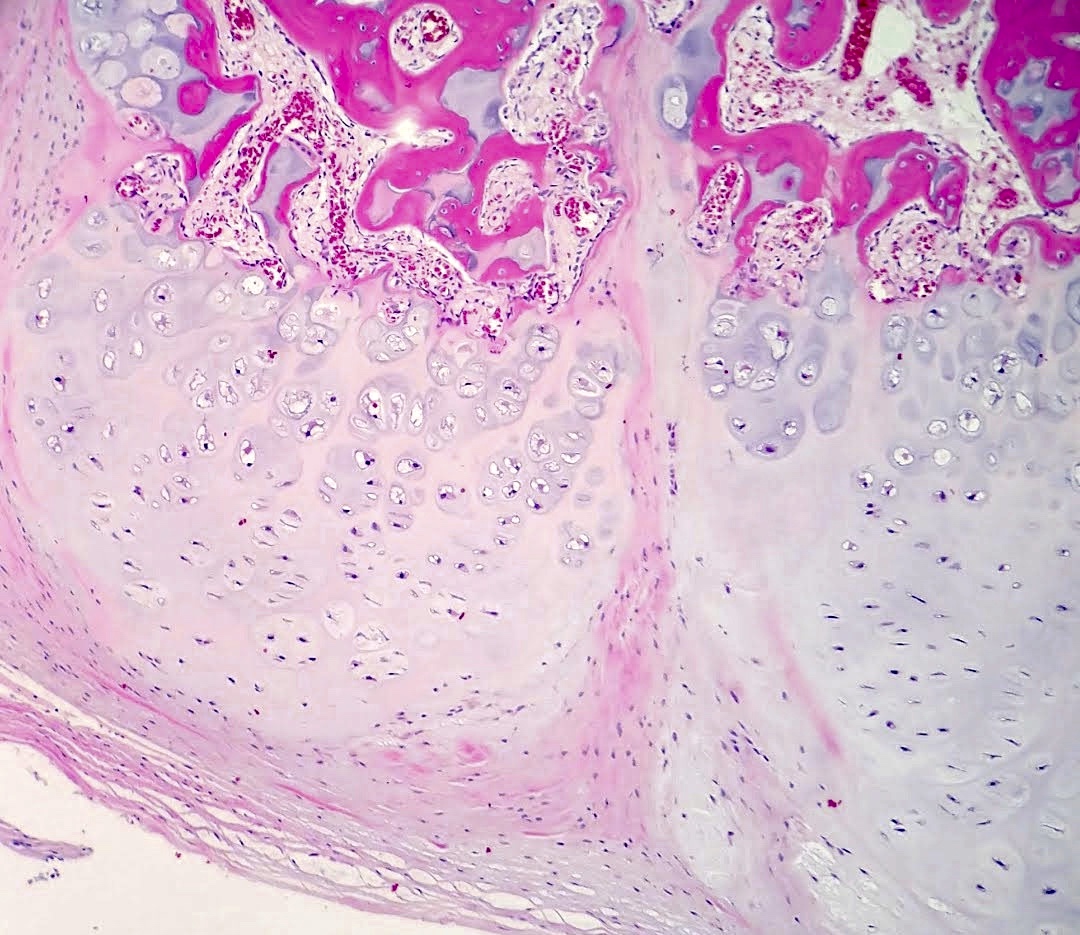
Microscopic (histologic) description
- Cap composed of mature hyaline cartilage with overlying fibrous perichondrium
- In young patients, transition between bone and cartilage cap resembles growth plate, showing endochondral ossification into mature bone; cartilage cap diminishes and may essentially be absent in older adults
- Marrow elements may be present within bony stalk; marrow space / cancellous bone contiguous with that of the native bone
Microscopic (histologic) images
Contributed by Jose G. Mantilla, M.D. and AFIP images
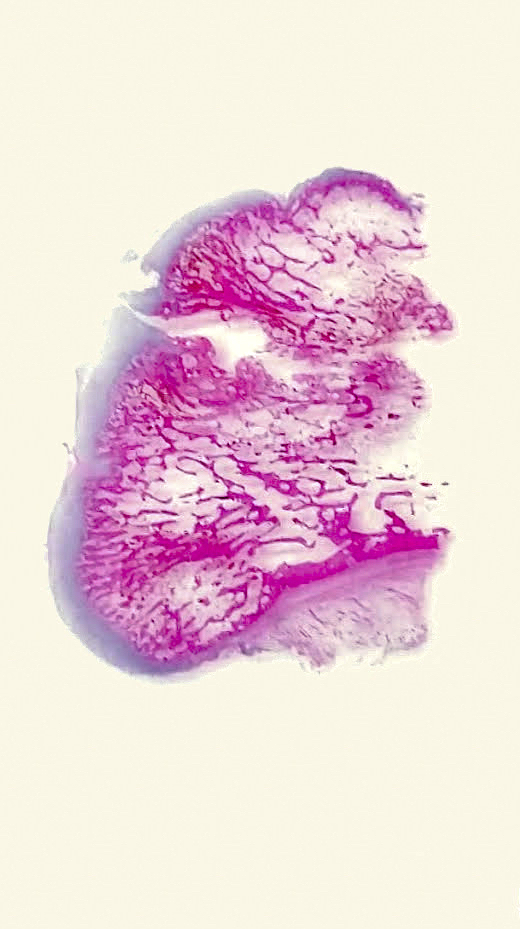
Whole slide
Cartilage cap
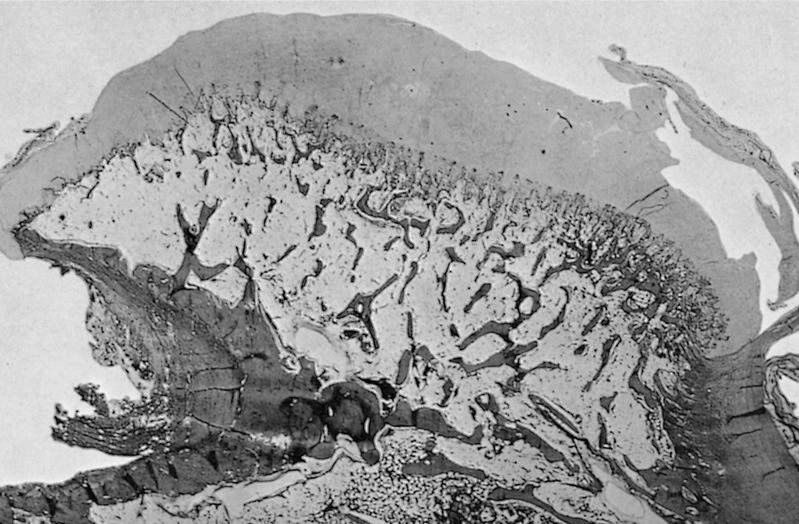
Whole mount section
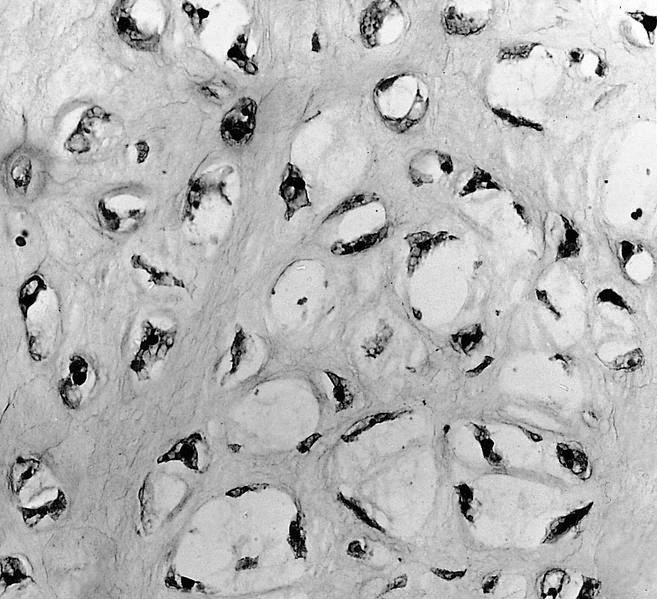
Cellular cartilaginous foci
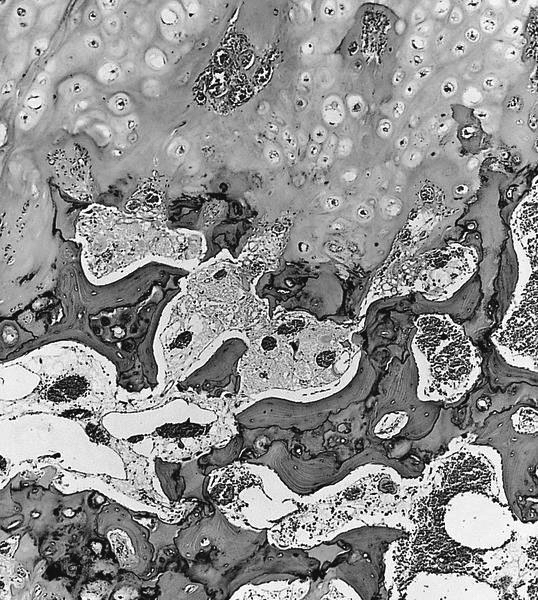
Junction of cartilage cap and underlying bone
Molecular / cytogenetics description
- Solitary osteochondroma and MHE associated with EXT1 and EXT2 mutations
Sample pathology report
- Knee mass, excision:
- Osteochondroma
Differential diagnosis
- Bizarre parosteal osteochondromatous proliferation (Nora lesion):
- Disorganized growth of bone and cartilage with characteristic blue bone
- Typically located in the distal extremities (J Orthop 2018;15:138)
- Florid reactive periostitis:
- Mixture of reactive woven bone and fibrous tissue without zonation
- Typically arises in the periosteum of fingers
- Parosteal osteosarcoma:
- Similar location and age group
- More aggressive growth areas of neoplastic woven bone formation and fibroblastic areas
- Can have a cartilage cap in up to 25% of cases
- Secondary chondrosarcoma:
- Infiltrative growth with permeation of bone or extension into soft tissue
- Usually well differentiated but with invasion into surrounding tissue
Board review style question #1
Which of the following is true about the epidemiology of osteochondromas?
- Congenital lesions are relatively common
- Female predominance
- Most lesions arise in long bones
- Most common in the elderly
- Multiple lesions are more common
Board review style answer #1
Board review style question #2
Which of the following is true regarding secondary chondrosarcoma?
- Most common subtype is clear cell chondrosarcoma
- Patients with multiple osteochondromas have a higher overall risk of developing chondrosarcoma
- Risk of malignancy in patients with multiple hereditary exostosis is near 50%
- Risk of malignancy in solitary osteochondromas is high
Board review style answer #2
B. Patients with multiple osteochondromas have a higher overall risk of developing chondrosarcoma
Comment Here
Reference: Osteochondroma
Comment Here
Reference: Osteochondroma

