

Bone & joints
Osteoclastic giant cell rich tumors
Benign
Nonossifying fibroma
Resident / Fellow Advisory Board: Josephine K. Dermawan, M.D., Ph.D.
Editorial Board Member: Jose G. Mantilla, M.D.


Last author update: 25 October 2021
Last staff update: 29 February 2024
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Nonossifying fibroma

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Anjum S, Chundriger Q, Ud Din N. Nonossifying fibroma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/bonemetaphysealfibrousdefect.html. Accessed December 25th, 2024.
Definition / general
- Benign fibrohistiocytic tumor arising in the metaphysis of long bones of skeletally immature individuals, composed of bland fibroblastic proliferation admixed with osteoclast-like giant cells
- Local recurrence and malignant transformation are extremely rare
Essential features
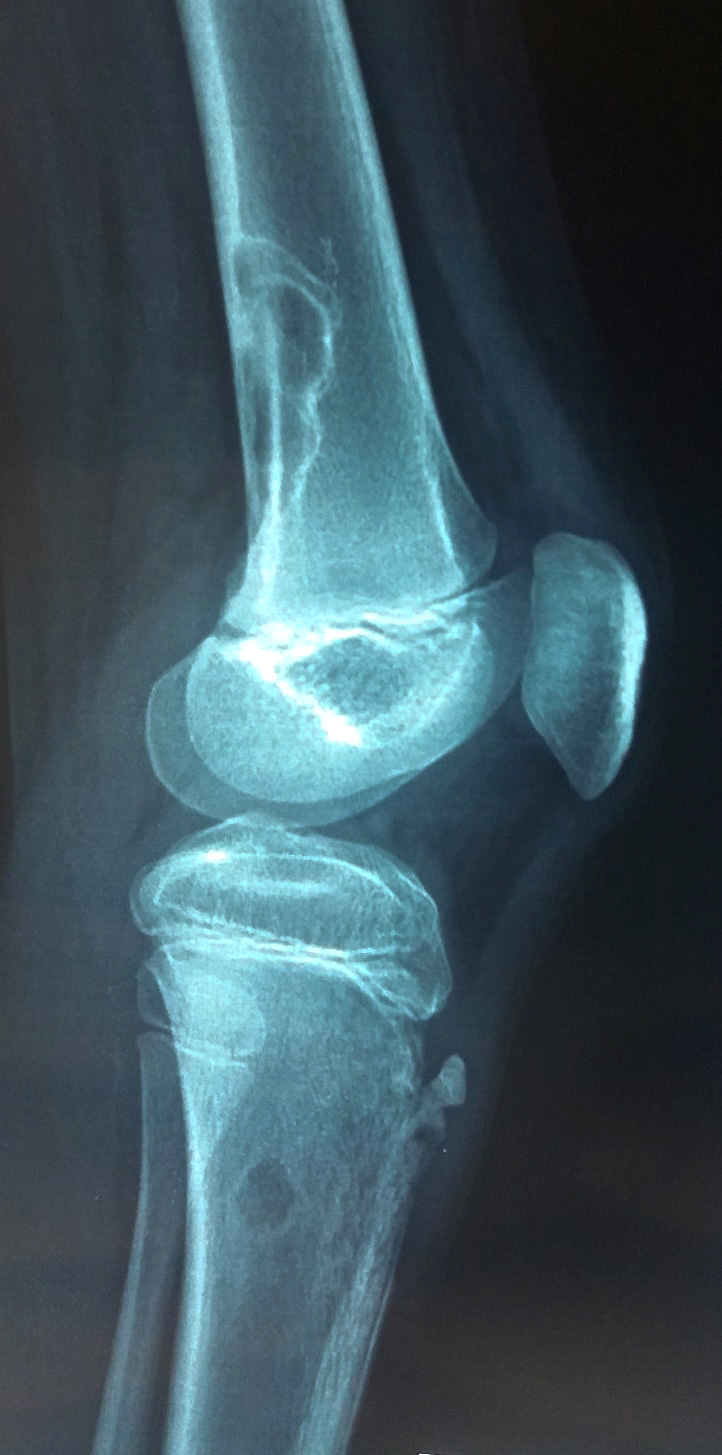
- Characteristic radiologic appearance (i.e. radiolucent eccentric location within the metadiaphysis of long bones with lobulated, well demarcated, sclerotic rim and scalloped borders)
- Histologically exhibits bland spindle shaped fibroblasts arranged in storiform pattern with interspersed osteoclast-like giant cells
Terminology
- Metaphyseal fibrous defect
ICD coding
- ICD-O: 8830/0 - benign fibrous histiocytoma
- ICD-11
- 2E85.Y & XH06N0 - benign fibrohistiocytic tumor of other specified sites & benign fibrous histiocytoma
- 2E85.Y & XA5GG8 - benign fibrohistiocytic tumor of other specified sites and bones
Epidemiology
- Accurate incidence is unknown because most of these lesions are asymptomatic and resolve spontaneously
- Mostly arises in skeletally immature individuals, peaks in second decade of life
- Up to 40% of children have an occult lesion (Chir Pediatr 1980;21:179)
Sites
- Most common:
- Metaphysis of long bones of lower extremities, especially distal femur, distal and proximal tibia and fibula (Head Neck Pathol 2013;7:203, BMC Musculoskelet Disord 2016;17:147, World J Orthop 2017;8:561)
- Less common:
- Pelvic bones, such as ileum (Int J Clin Exp Pathol 2013;6:3003)
- Gnathic skeleton, such as mandible (Head Neck Pathol 2013;7:203, Ear Nose Throat J 2015;94:E41)
- Axial skeleton (J Bone Oncol 2019;20:100274)
- Newer published data suggests that nonossifying fibromas (NOFs) arising at unusual sites, such as gnathic bones and in skeletally mature individuals, may be related to giant cell tumors of the jaw, as both of these lesions harbor KRAS and FGFR1 mutations, albeit at different codons (Adv Anat Pathol 2021;28:119, J Pathol 2019;248:127)
Pathophysiology
- Mutually exclusive hotspot mutations in KRAS and FGFR1 are pathogenic in 65 - 80% of cases (J Pathol 2019;248:116, J Pathol 2019;248:127)
- Inactivating mutations of NF1 result in activation of KRAS-MAPK pathway (J Pathol 2019;248:127)
Etiology
- Germline mutations resulting in activation of KRAS-MAPK pathway
- Unknown in sporadic cases
Diagrams / tables
Contributed by Qurratulain Chundriger, M.B.B.S.

Schematic presentation
Clinical features
- Most cases are asymptomatic and are discovered incidentally
- Larger lesions and those at unusual sites can present with pain and pathological fractures (J Orthop Case Rep 2020;10:106, World J Orthop 2017;8:561, J Orthop Sports Phys Ther 2008;38:434)
- Multiple lesions are commonly associated with clinical syndromes:
- Neurofibromatosis type 1 (Int J Clin Exp Pathol 2013;6:3003)
- Jaffe-Campanacci syndrome (Ital J Pediatr 2020;46:58)
- Trichorhinophalangeal syndrome (BMC Med Genet 2018;19:211)
Diagnosis
- Requires integration of radiological and histopathological findings; diagnosis can be challenging on a small biopsy specimen (e.g. cytology or needle core)
Radiology description
- Long bones:
- Well demarcated, lobulated radiolucency in the cortex with scalloped and sclerotic rim (J Child Orthop 2017;11:373)
- Aligned to the long axis of the bone (J Orthop Case Rep 2020;10:106)
- Natural history can be described using 4 Ritschl stages as follows (BMC Musculoskelet Disord 2016;17:147):
- Stage A: small cortical eccentric lesion near the epiphyseal plate without sclerotic rim
- Stage B: polycyclic lesion, away from the epiphyseal plate, with thin sclerotic rim
- Stage C: increasing sclerosis particularly towards diaphysis
- Stage D: homogeneously sclerosed lesion
- Small and flat bones:
- Regardless of the site, it appears as an expansile sharply demarcated radiolucency with variable sclerosis of the edges (Spine (Phila Pa 1976) 2003;28:E359, Head Neck Pathol 2013;7:203, J Bone Oncol 2019;20:100274)
Radiology images
Contributed by Nasir Ud Din, M.B.B.S. and AFIP images

Distal tibia

Proximal tibia

Proximal fibula

Femur with fracture
Multifocal

Nonossifying fibroma
Images hosted on other servers:


Radius (plain radiograph)

Radius (MRI)

Femur (plain radiograph)

Femur (CT scan)

Vertebral body


Mandible


Growth stages
Prognostic factors
- Excellent prognosis, local recurrence is rare but reported (J Orthop Case Rep 2020;10:106)
- Malignant transformations are extremely rare, with an example of spindle cell sarcoma and another of osteogenic sarcoma arising in NOF in 1 twin, although both harbored NOFs (J Clin Orthop Trauma 2013;4:80, J Clin Orthop Trauma 2014;5:257)
Case reports
- 6 year old boy with a lesion in the posterior arch of C1 (Spine (Phila Pa 1976) 2003;28:E359)
- 11 year old girl with recurrent forearm lesion (J Orthop Case Rep 2020;10:106)
- 45 year old man with pathological fracture of distal femur (J Clin Orthop Trauma 2013;4:80)
- 51 year old man with clinical features of neurofibromatosis type 1 (Int J Clin Exp Pathol 2013;6:3003)
Treatment
- Asymptomatic lesions can be left untreated and may resolve spontaneously (Indian J Plast Surg 2020;53:442, BMC Musculoskelet Disord 2016;17:147)
- Larger and symptomatic lesions can be treated with simple curettage
- Percutaneous cryoablation is a newer option for symptomatic cases (Diagn Interv Imaging 2015;96:107)
Clinical images
Images hosted on other servers:

Lesion in clavicle
Gross description
- Well circumscribed, red-brown with areas of yellow discoloration and having sclerotic borders (Niger Postgrad Med J 2018;25:126)
- Cut surface is firm, can exhibit cystic, hemorrhagic and necrotic areas
Gross images
Images hosted on other servers:

Lesion in clavicle

Lesion in mandible
Microscopic (histologic) description
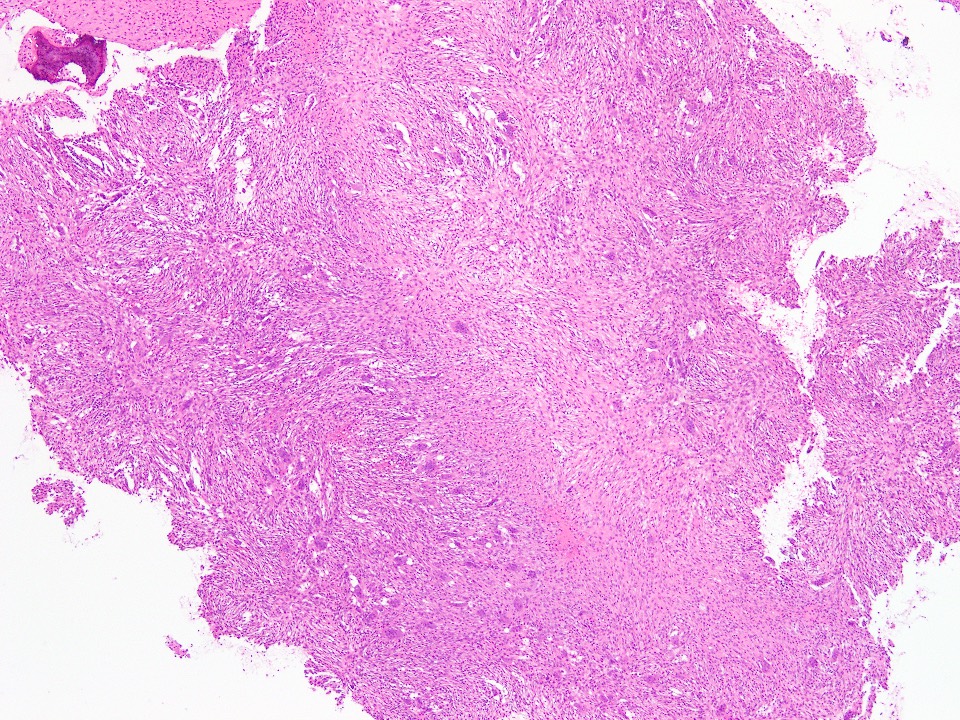
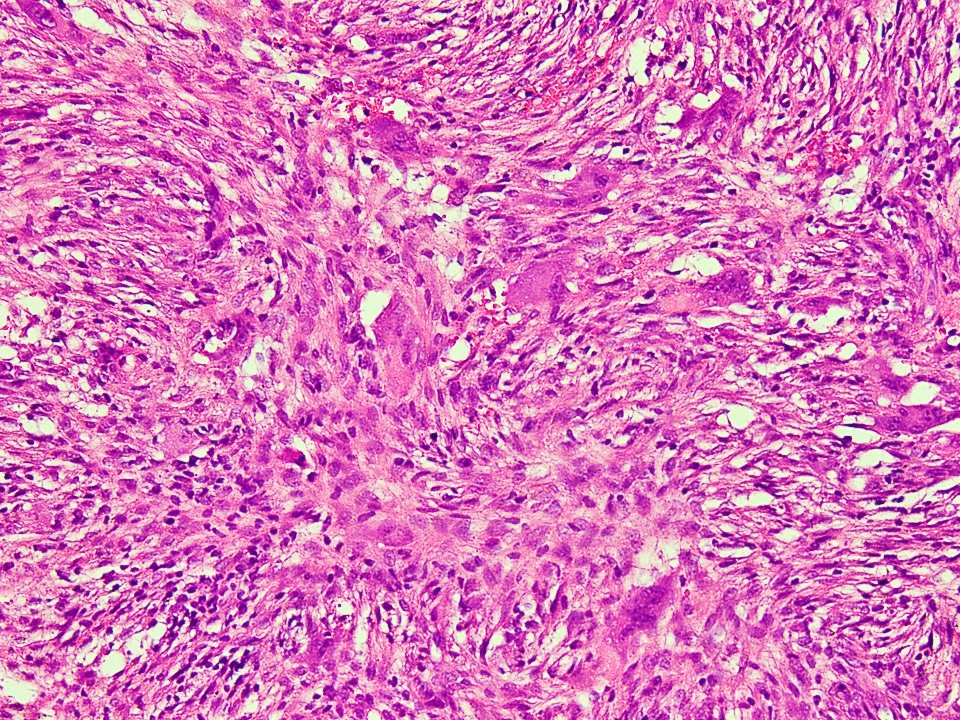
- Bland, spindle shaped fibroblasts arranged in storiform pattern, interspersed with osteoclast-like multinucleated giant cells (Ear Nose Throat J 2015;94:E41)
- Number of giant cells is much fewer than in giant cell tumor of bone
- Some cases may resemble solid areas in aneurysmal bone cyst
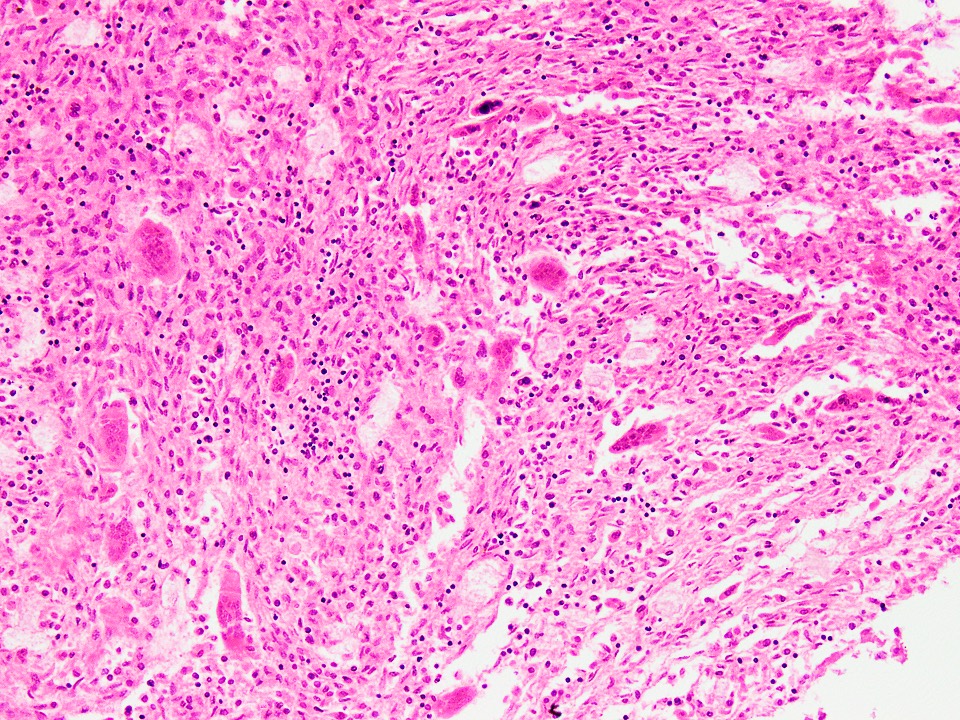
- Variable amount of foamy and hemosiderin laden macrophages (Head Neck Pathol 2013;7:203)
- Cystic changes and areas of necrosis if associated with pathological fractures
- Hemorrhage and inflammatory cells may also accompany necrosis associated with fracture
- Areas of reactive woven bone formation may be seen (Spine (Phila Pa 1976) 2003;28:E359)
Microscopic (histologic) images
Contributed by Nasir Ud Din, M.B.B.S.
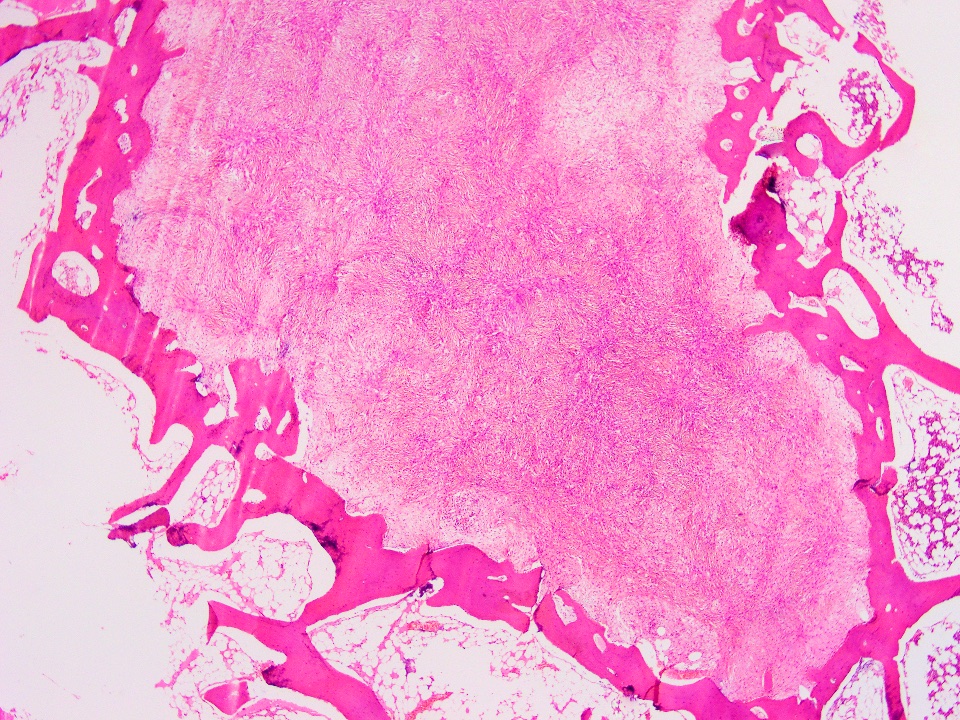
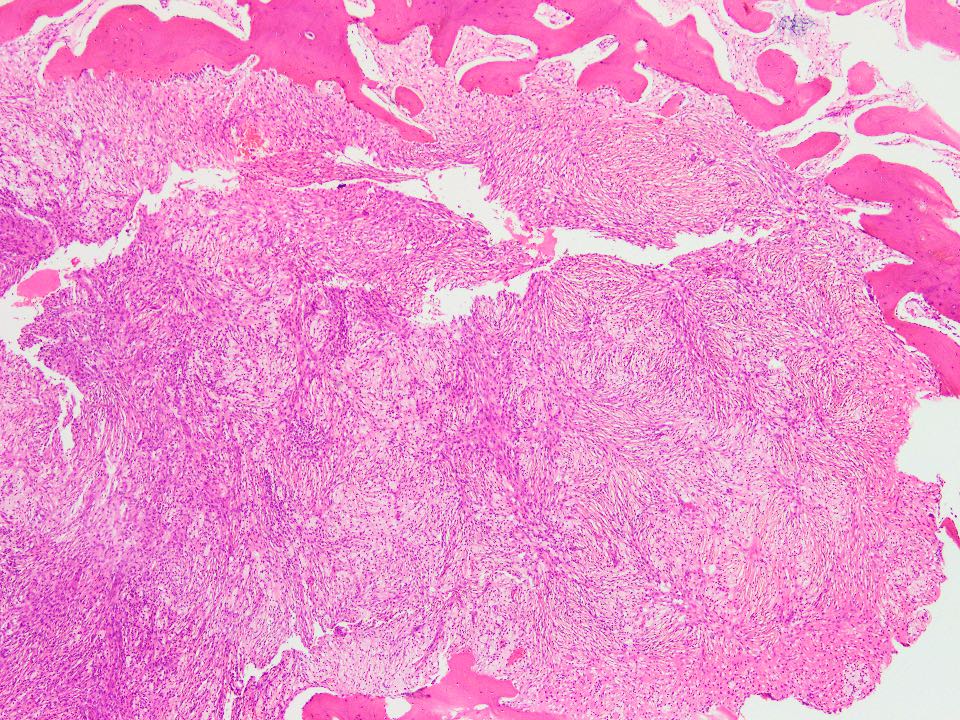
Circumscribed border on resection
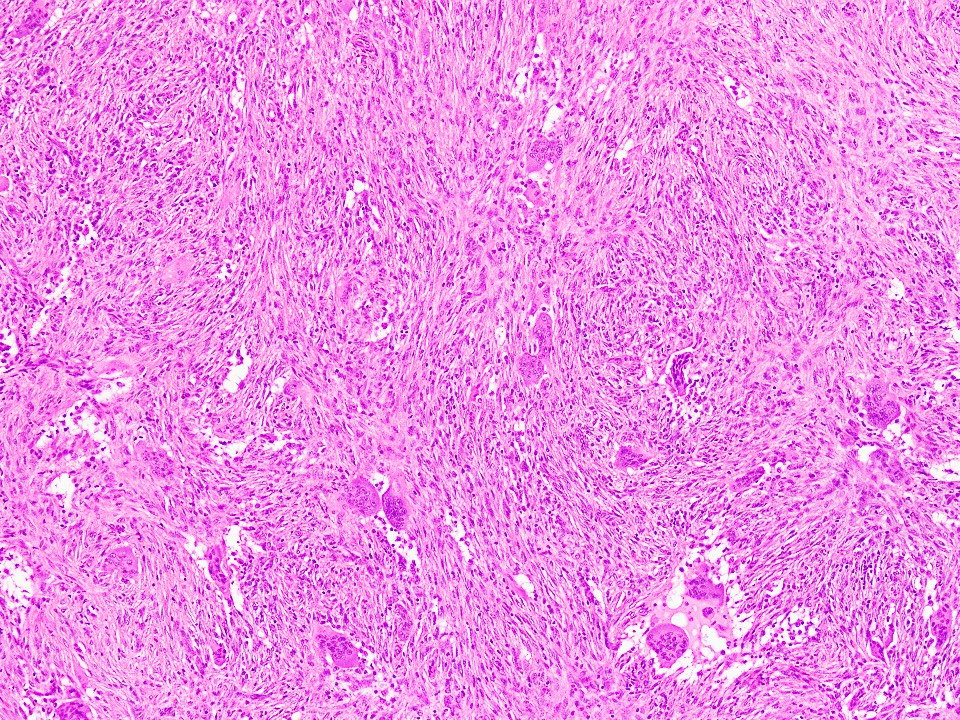
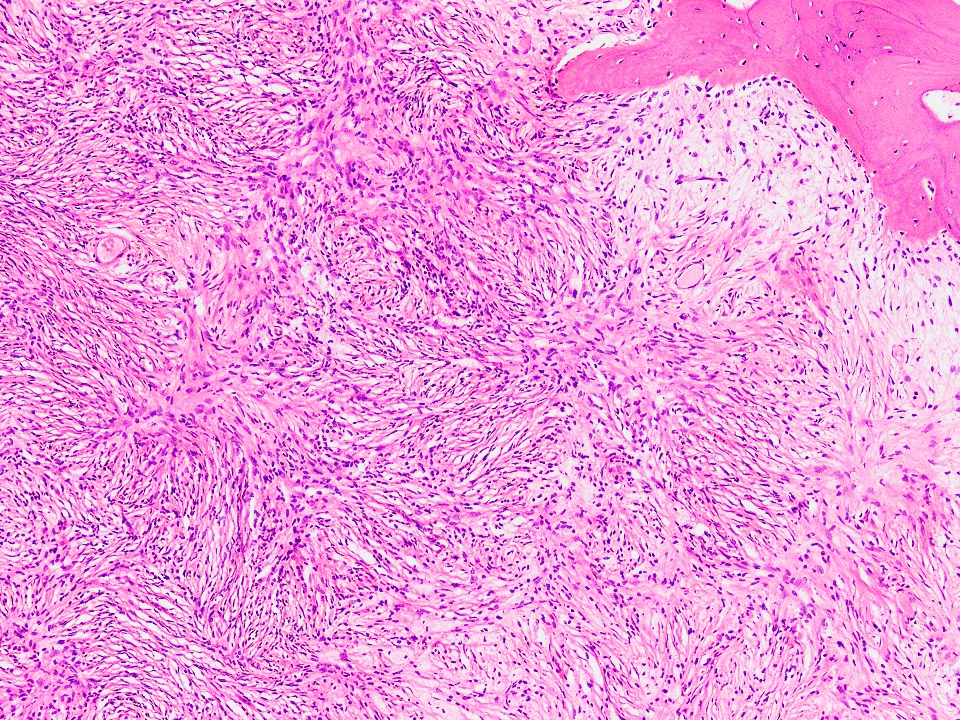
Storiform arrangement

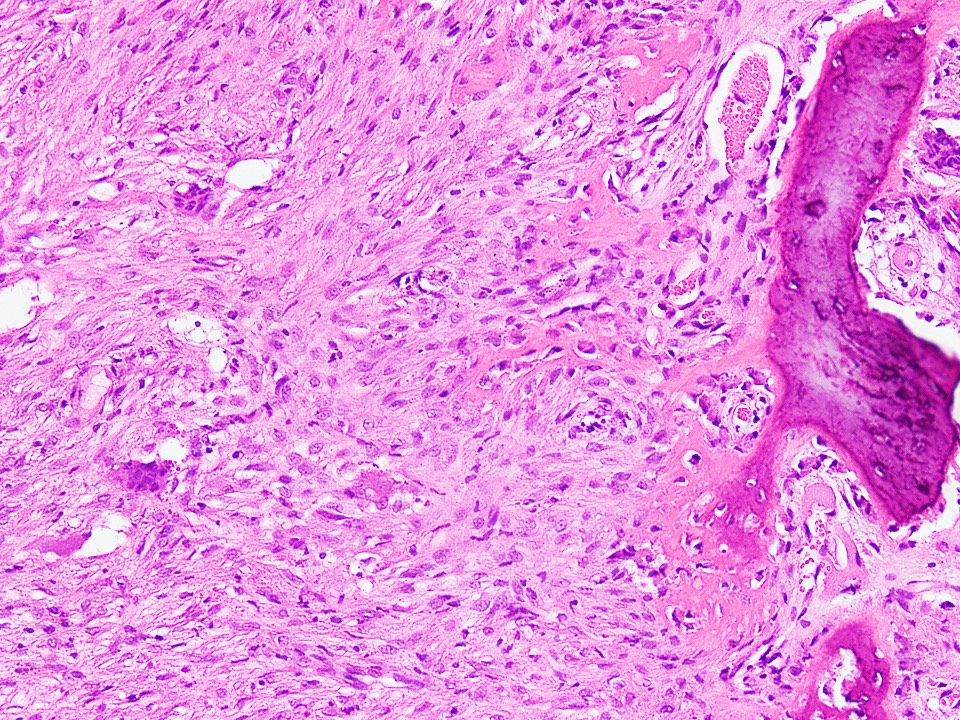
Interspersed giant cells

Few giant cells
Resembling ABC
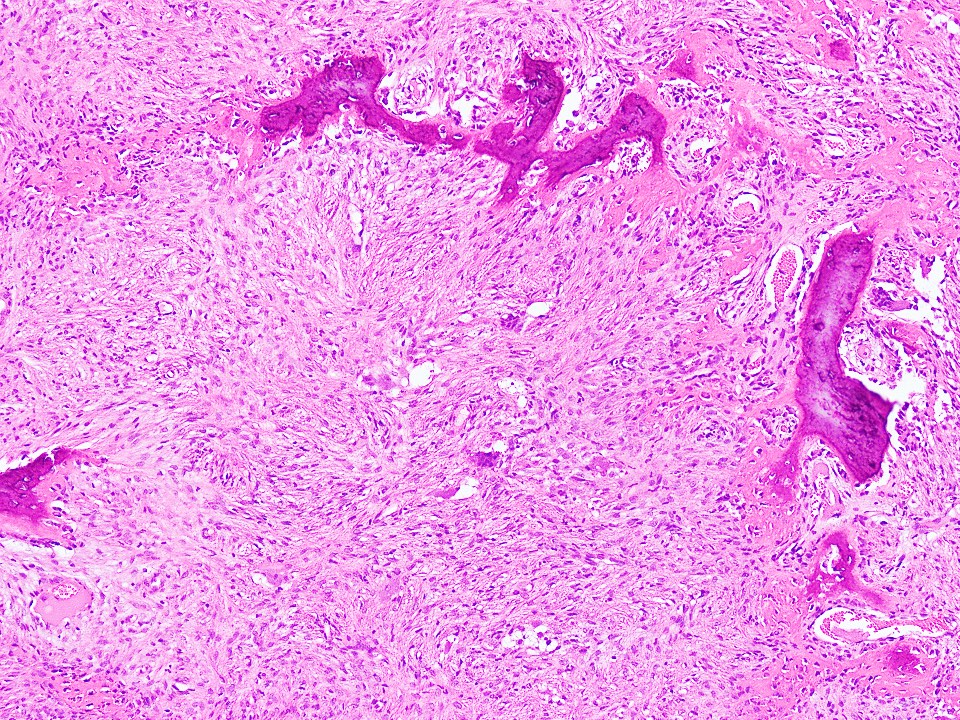
Reactive woven bone
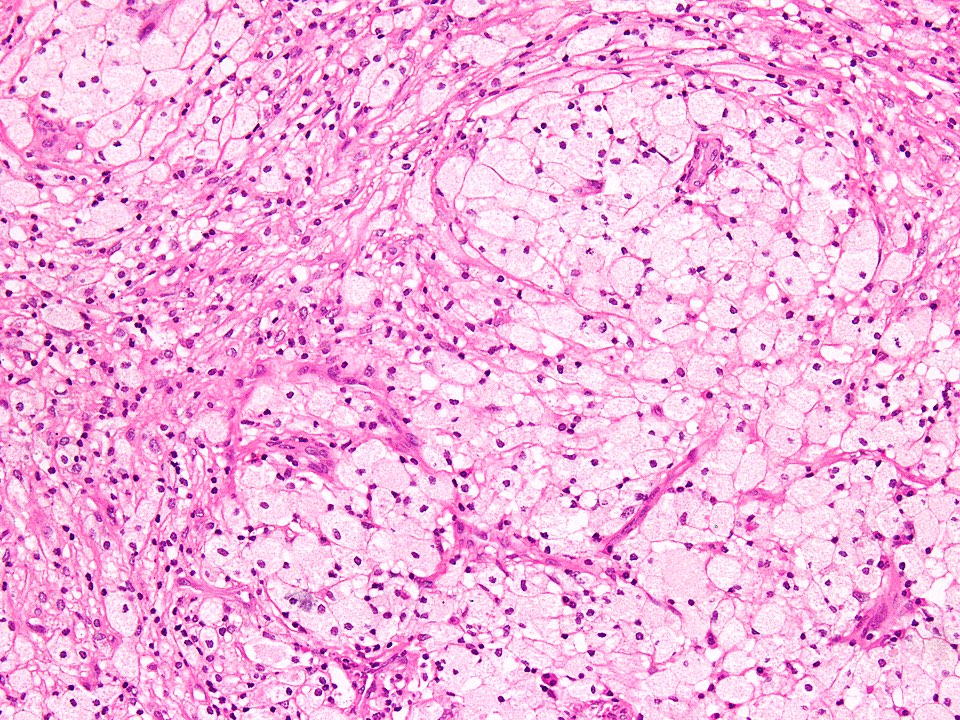
Aggregates of foamy macrophages
Hemorrhage and inflammatory cells
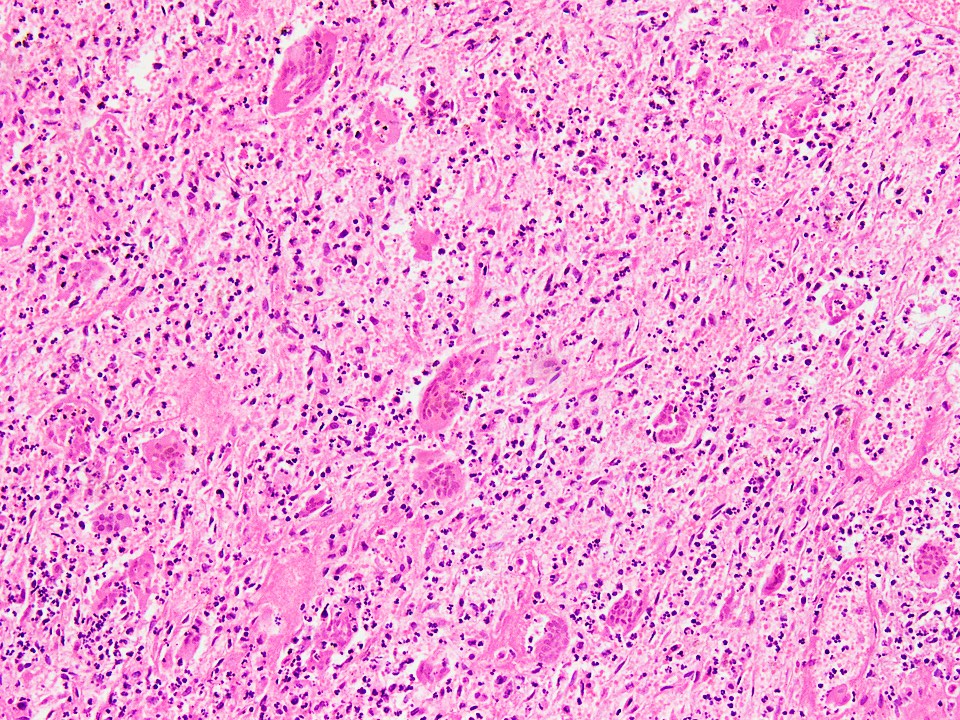
Necrosis after fracture
Cytology description
- Admixture of benign stromal cells and scattered osteoclast type giant cells in the smears (BMC Med Genet 2018;19:211)
Cytology images
Images hosted on other servers:

Lesion in femur
Positive stains
- Nonossifying fibroma does not require immunohistochemistry for diagnosis
- Vimentin (Ear Nose Throat J 2015;94:E41)
- Phosphorylated p44 / 42 MAPK (ERK1/2) (J Pathol 2019;248:116)
- CD68 (in giant cells)
Negative stains
Molecular / cytogenetics description
- Not required for reaching diagnosis
- KRAS and FGFR1 mutation analysis may be helpful in ambiguous cases (J Pathol 2019;248:127, Adv Anat Pathol 2021;28:119)
Videos
Bone and cartilage tumors
Sample pathology report
- Left distal femur, curettage:
- Benign spindle cell lesion with features consistent with nonossifying fibroma (see comment)
- Comment: Correlation with radiological findings is essential.
Differential diagnosis
- Giant cell tumor of bone:
- Arises in epiphyses of long bones in adults
- Uniform distribution of osteoclast type giant cells among mononuclear cells
- Mononuclear cells in GCT are oval shaped and not spindled as seen in NOF
- Giant cell nuclei are like mononuclear cell nuclei in GCT, which is not seen in NOF
- Stromal mononuclear cells of GCT are positive for H3.3 G34W
- GCT may have areas indistinguishable from NOF; positive staining of stromal cells for G34W will help resolve the issue
- Benign fibrous histiocytoma:
- Extremely rare, infiltrative lesion of soft tissue which causes destruction of adjacent bones, arising from primitive mesenchymal cells (Medicine (Baltimore) 2019;98:e17144)
- Primary lesions of bone are even rarer, with cases reported to involve the spine and distal portions of long bones (J Bone Oncol 2018;12:78)
- Fascicular and storiform growth of spindle cells with interspersed multinucleated giant cells resembles nonossifying fibroma microscopically
- Extensive excision is required to prevent recurrence, which is common due to infiltrative growth (Medicine (Baltimore) 2019;98:e17144)
- Solid aneurysmal bone cyst:
- Arises in the metaphysis of long bones as expansile lytic lesion with circumscribed borders
- Septal enhancement on contrast; fluid-fluid levels on MRI
- Solid ABC often shows reactive woven bone formation within tumor and storiform pattern is not prominent
- USP6 gene rearrangement by FISH, not detected in NOF
- Fibrous dysplasia:
- Common fibro-osseous lesion arises in long and craniofacial bones
- Most cases are asymptomatic but may come to attention due to pain and fracture
- Radiology shows diaphyseal or metadiaphyseal intramedullary sharply demarcated lesion with ground glass-like appearance, while NOF is eccentrically placed in metaphysis
- Histology shows irregular curvilinear trabeculae of woven bone in a background of bland spindle cells
- Multinucleated giant cells may be seen, along with myxoid change and foamy histiocytes but these are not a common feature
Board review style question #1

A 15 year old girl had a fall during marathon practice and sustained a fracture of the distal tibia. Radiological appearance is given in the picture above. Curettage was done and microscopic examination showed a lesion shown in the given photomicrograph. The most helpful feature for establishing the correct diagnosis in this case is
- Areas of chicken wire-like calcification surrounding the fibroblasts
- Curvilinear trabeculae of woven bone in background of spindle cells
- Linear trabeculae of woven bone surrounded by osteoblasts
- Pools of hemorrhage surrounded by multinucleated giant cells
- Storiform growth of bland spindle cells with scattered giant cells
Board review style answer #1
E. Storiform growth of bland spindle cells with scattered giant cells. The photomicrograph shows a tumor comprised of bland spindle cells growing in a storiform pattern. There are scattered multinucleated giant cells within the tumor. These findings are characteristic of nonossifying fibroma (NOF). The fact that the lesion was asymptomatic and caused pathological fracture due to trauma is another supportive feature in this case. Curvilinear trabeculae of woven bone are a feature of fibrous dysplasia of bone. Linear trabeculae of woven bone may be seen in some cases of NOF but they are not diagnostic of this lesion, per se. Similarly, pools of hemorrhage can be seen in cases of NOF secondary to an associated fracture. This feature, however, is a diagnostic primary finding of an aneurysmal bone cyst.
Comment Here
Reference: Nonossifying fibroma
Comment Here
Reference: Nonossifying fibroma
Board review style question #2
Which of the following genetic mutations has been found to be common in nonossifying fibroma?
- BRAF
- GNAS
- H3F3B
- KRAS
- TBXT
Board review style answer #2
D. KRAS mutations are seen in up to 80% of nonossifying fibromas. GNAS mutations are a feature of fibrous dysplasia of bone. H3F3B is mutated in chondroblastoma and mutations involving TBXT are a feature of notochordal tumors. USP6 mutations are commonly seen in cases of aneurysmal bone cyst and nodular fasciitis in soft tissues.
Comment Here
Reference: Nonossifying fibroma
Comment Here
Reference: Nonossifying fibroma

