

Bladder & urothelial tract
Squamous cell neoplasms
Squamous cell carcinoma
Authors: Susan Prendeville, M.D., Bonnie Choy, M.D.
Editorial Board Member: Maria Tretiakova, M.D., Ph.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 15 April 2021
Last staff update: 10 April 2024
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Squamous cell carcinoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology / etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Prendeville S, Choy B. Squamous cell carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/bladdersquamous.html. Accessed May 6th, 2024.
Definition / general
- Malignant epithelial neoplasm arising in the urinary bladder, renal pelvis or ureter demonstrating a pure squamous cell phenotype
- This topic describes classic squamous cell carcinoma; please see separate topic on verrucous squamous cell carcinoma
Essential features
- Uncommon subtype of carcinoma showing pure squamous morphology without any component of conventional urothelial carcinoma
- Predisposing factors include Schistosoma infection, smoking and conditions resulting in chronic irritation for bladder tumors and nephrolithiasis, anatomic anomalies of the kidney and chronic recurrent infections for upper urinary tract tumors
- May be associated with keratinizing squamous metaplasia / dysplasia of the mucosa
- Must be distinguished from urothelial carcinoma with squamous differentiation, secondary spread of squamous cell carcinoma primary to another site, e.g. cervix, penis, anus and metastasis
Terminology
- Classic / typical squamous cell carcinoma
ICD coding
Epidemiology
- Bladder
- Incidence varies by geographic region
- 2 - 5% of bladder tumors in Western countries (nonbilharzial) (Arab J Urol 2016;14:183)
- Most common nonurothelial subtype of bladder cancer
- 20 - 30% of bladder tumors in geographic regions with high prevalence of schistosomiasis (bilharzial) including Egypt and other parts of Africa (Arab J Urol 2016;14:183)
- Frequency of squamous cell carcinoma is falling due to declining rates of Schistosoma infection (Cancer Causes Control 2008;19:421)
- Slight male predominance
- Renal pelvis / ureter
- 1 - 8% of malignancies involving the renal pelvis and ureter (J Urol 1987;138:269, J Urol 2007;178:51)
Sites
- Bladder: most commonly involving posterior and lateral walls (Am J Surg Pathol 2007;31:1777)
- Renal pelvis
- Ureter
Pathophysiology / etiology
- Bladder
- Schistosomiasis
- Schistosoma haematobium
- Major risk factor for bladder squamous cell carcinoma in geographic regions with high prevalence of schistosomiasis including Egypt and other parts of Africa
- Smoking: 5x increased risk compared with nonsmokers (JAMA 2011;306:737)
- Chronic bladder irritation / inflammation associated with:
- Long term catheterization
- Bladder calculi or foreign bodies
- Neurogenic bladder
- Bladder exstrophy (Urology 2006;67:199)
- Renal pelvis / ureter
- Nephrolithiasis, such as staghorn calculi (J Urol 1987;138:269)
- Anatomic anomalies of the kidney, such as horseshoe kidney, duplicated renal pelvis (Int J Urol 2004;11:782, Int J Clin Exp Pathol 2014;7:7957)
- Chronic recurrent infections
- Schistosomiasis
Clinical features
- Typically presents with hematuria
- May also present with dysuria, urgency and frequent urination, recurrent urinary tract infection, urinary obstruction and flank or suprapubic pain
Diagnosis
- Urine cytology
- Cystoscopy and biopsy / transurethral resection of bladder tumor
Radiology description
- Bladder: tumors may appear plaque-like, polypoid, papillary or circumferential bladder wall thickening (Radiographics 2004;24:855)
- Renal pelvis / ureter: solid mass may be seen, along with other nonspecific findings, such as hydronephrosis, calcifications and nephrolithiasis (J Urol 1987;138:269, Urology 1992;40:458, Int J Urol 2000;7:316)
- CT or MRI may be used for local staging to delineate suspected depth of tumor invasion (J Natl Compr Canc Netw 2020;18:329)
Radiology images
Images hosted on other servers:

MRI bladder

Solitary mass lower right kidney

Mass in right renal pelvis
Prognostic factors
- Prognosis determined by tumor stage (staged in the same way as urothelial carcinoma), lymph node involvement and tumor grade (Urology 1999;53:1005, J Urol 2012;187:74)
- Often advanced stage at diagnosis resulting in poor prognosis (Am J Surg Pathol 2007;31:1777, J Urol 2010;183:915)
- Upper urinary tract squamous cell carcinoma presents with higher stage (and with frequent renal parenchyma invasion) than bladder squamous cell carcinoma (J Urol 2007;178:51, Clin Genitourin Cancer 2020 Dec 2 [Epub ahead of print], J Urol 2012;187:74)
- Schistosomiasis associated squamous cell carcinoma appears to have better prognosis than non-schistosomiasis associated (BJU Int 2004;93:216)
Case reports
- 45 year old woman with poorly differentiated squamous cell carcinoma arising on a background of recurrent condyloma acuminatum (Urol Case Rep 2016;7:61)
- 46 year old woman with basaloid squamous cell carcinoma of the bladder and concomitant HPV infection of the genital tract (Int J Urol 2015;22:222)
- 57 year old man with recurrent stone formation presenting with muscle invasive squamous cell carcinoma of the bladder (Clin Case Rep 2017;5:1616)
- 61 year old woman with enterovesical fistula secondary to squamous cell carcinoma of the bladder (Urol Case Rep 2015;3:201)
- 76 year old woman with squamous cell carcinoma of the upper urinary tract presenting with paraneoplastic syndrome (Urol Ann 2020;12:388)
- 79 year old woman with squamous cell carcinoma of the renal pelvis associated with staghorn calculi (Case Rep Oncol 2015;8:399)
- 80 year old woman with squamous cell carcinoma in the renal pelvis of a horseshoe kidney (Int J Urol 2004;11:782)
Treatment
- Radical cystectomy / nephrectomy / nephroureterectomy
- Neoadjuvant radiation may improve outcome (J Urol 2012;187:74, Arab J Urol 2016;14:183)
- Insufficient evidence to support the use of chemotherapy
Clinical images
Images hosted on other servers:

Bladder exstrophy
Gross description
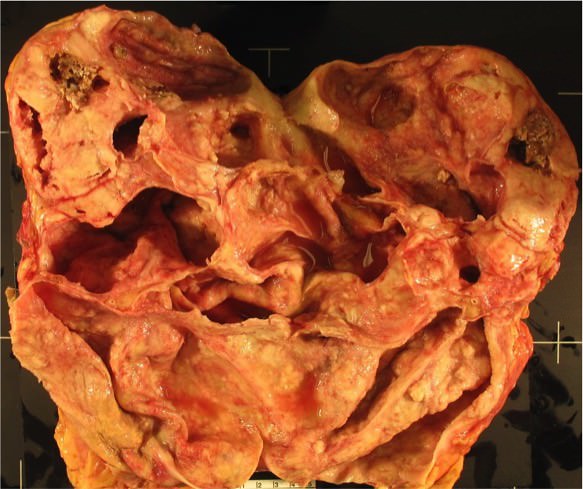
- Usually large exophytic bulky tumor; some cases are predominantly flat with ulcerating / infiltrating appearance (Am J Surg Pathol 2007;31:1777)
- Typically has tan-white coloration
- Often necrotic with flaky keratin material on the surface
Gross images
Bladder
Contributed by Susan Prendeville, M.D.
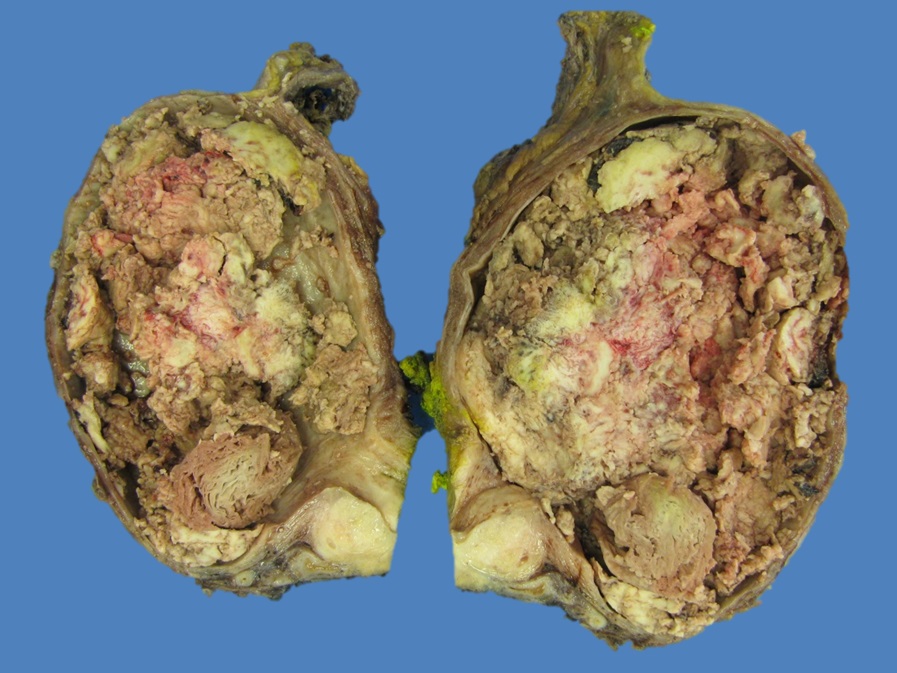
specimen
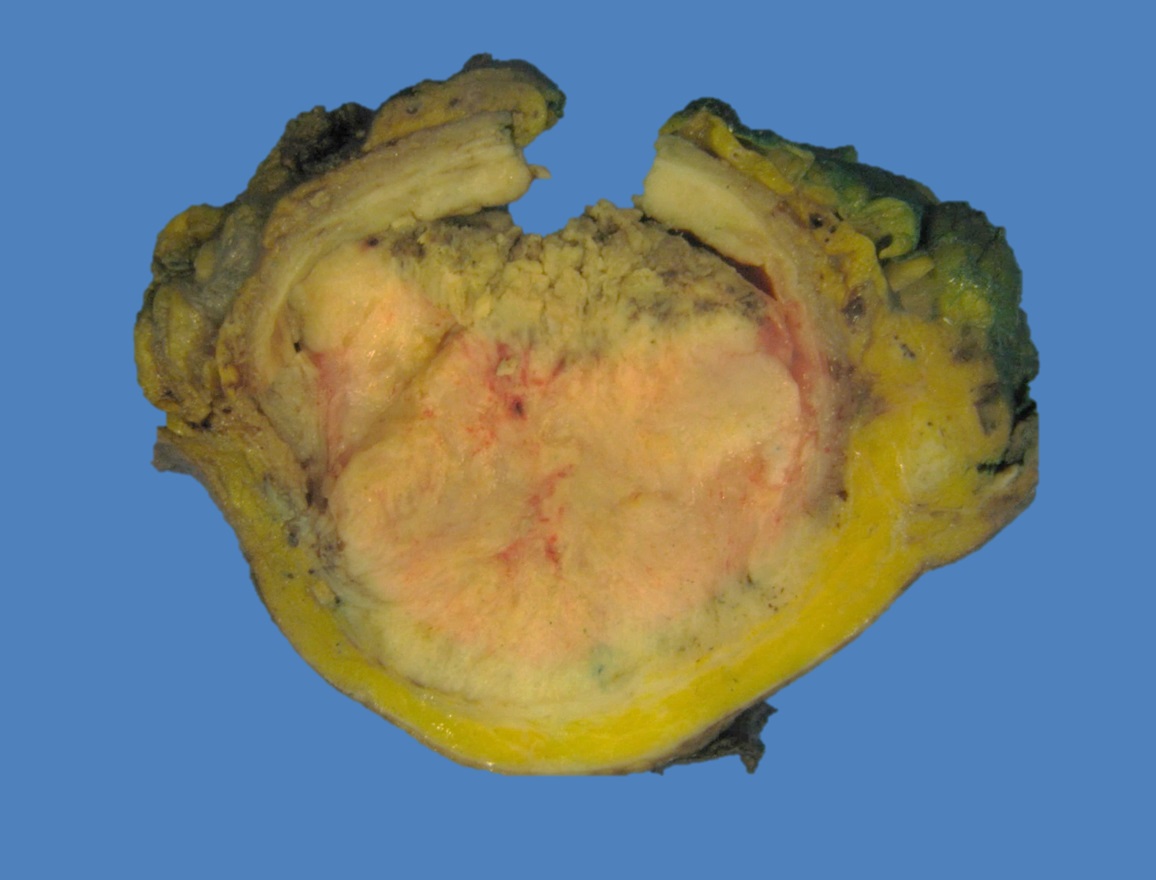
Cross section of tumor
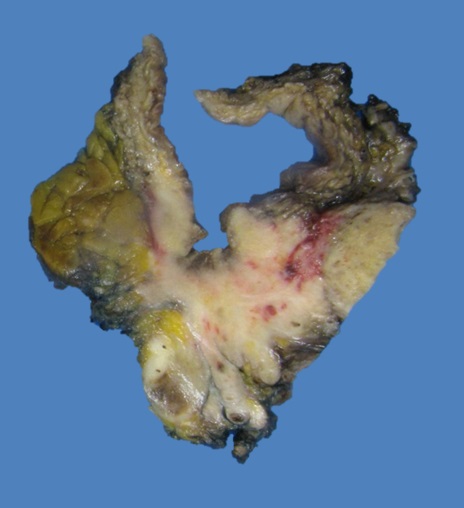
Ulcerating tumor
Renal pelvis
Contributed by Nicole K. Andeen, M.D.
Dilated renal calyces due to reflux
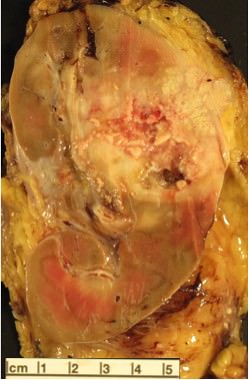
Solid, tannish white with central necrosis
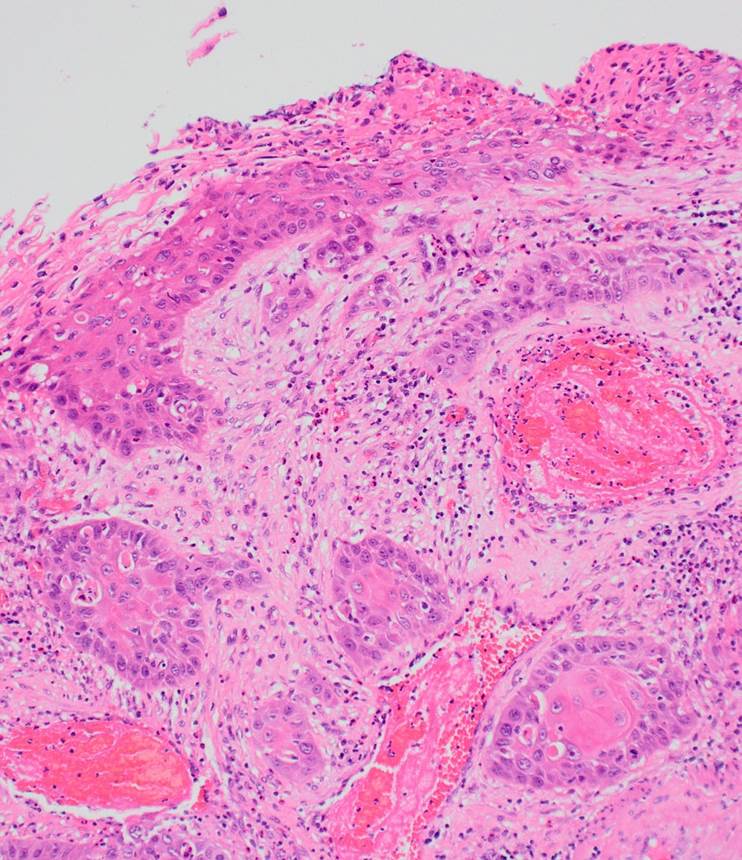
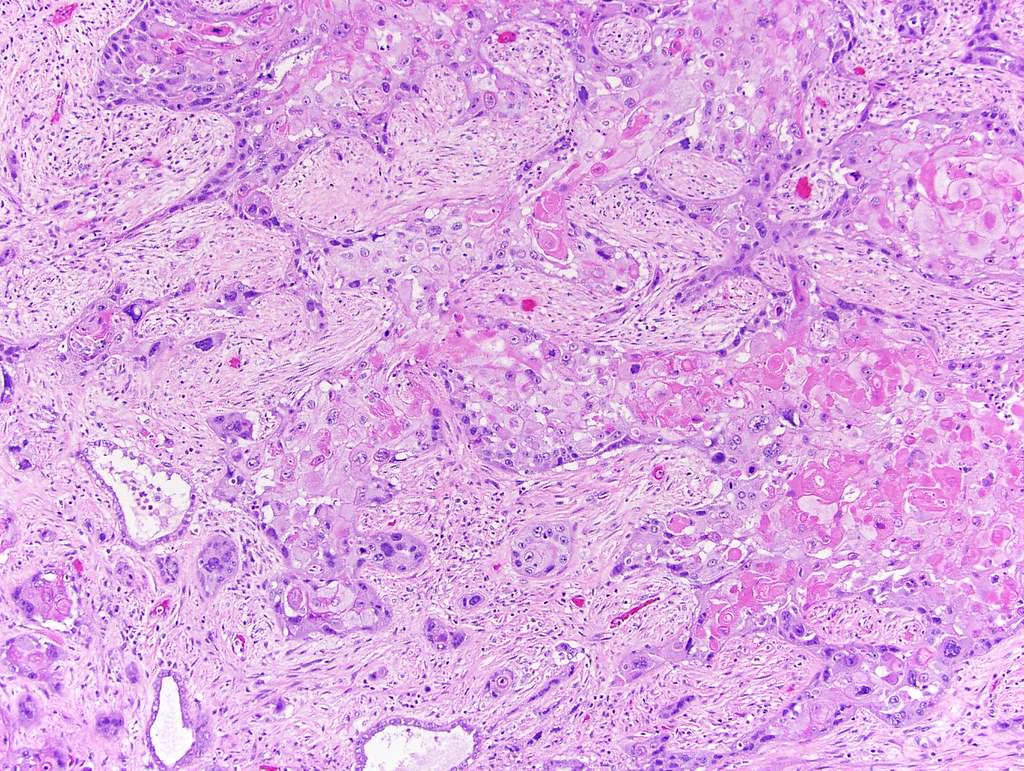
Microscopic (histologic) description
- May be well, moderately or poorly differentiated
- Moderately or poor differentiated tumors are most common
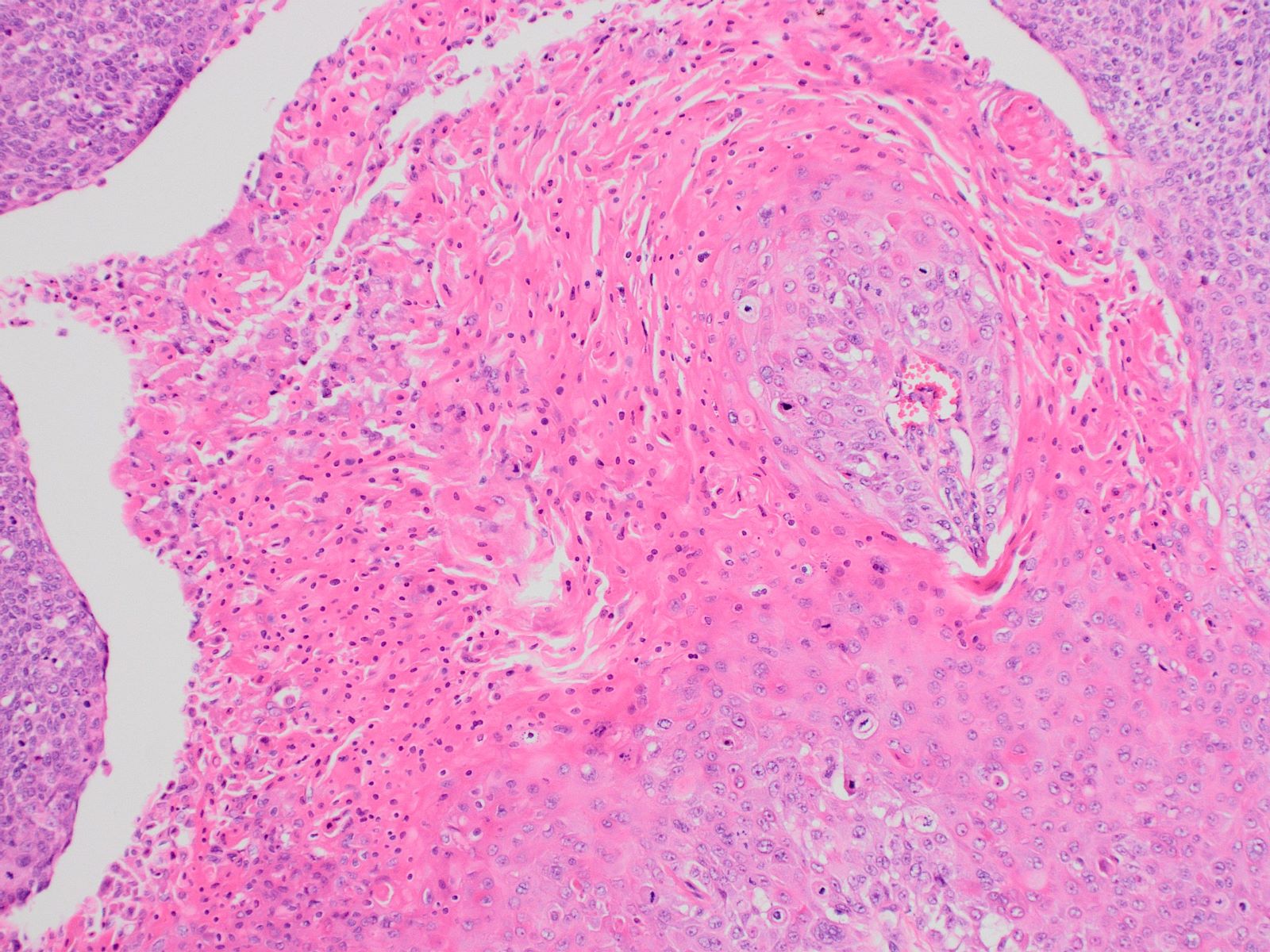
- Irregular infiltrating nests or sheets of malignant squamous cells with destructive stromal invasion
- Squamous differentiation in the form of keratin pearls, individual cell keratinization or intercellular bridges; findings may be focal in poorly differentiated tumors
- Often associated with surface keratinizing squamous metaplasia and dysplasia / squamous carcinoma in situ (Am J Surg Pathol 2007;31:1777)
- Must not show any component of conventional urothelial carcinoma or urothelial carcinoma in situ
- If present, even focally, tumor is designated as urothelial carcinoma with squamous differentiation
Microscopic (histologic) images
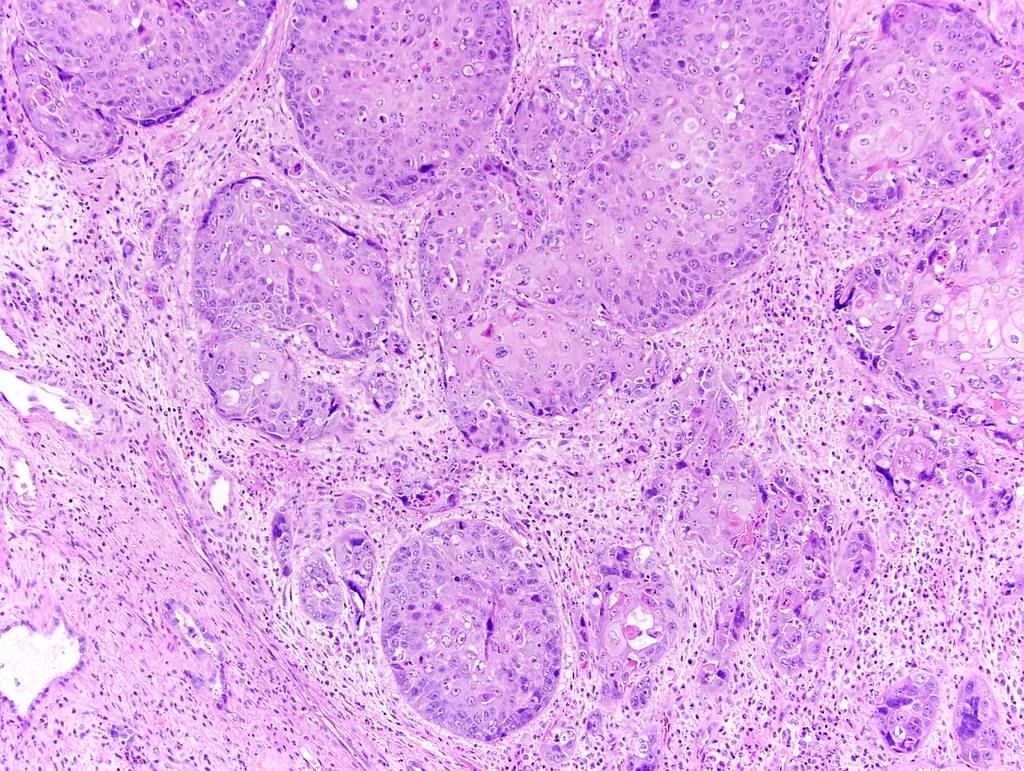
Bladder
Contributed by Susan Prendeville, M.D.
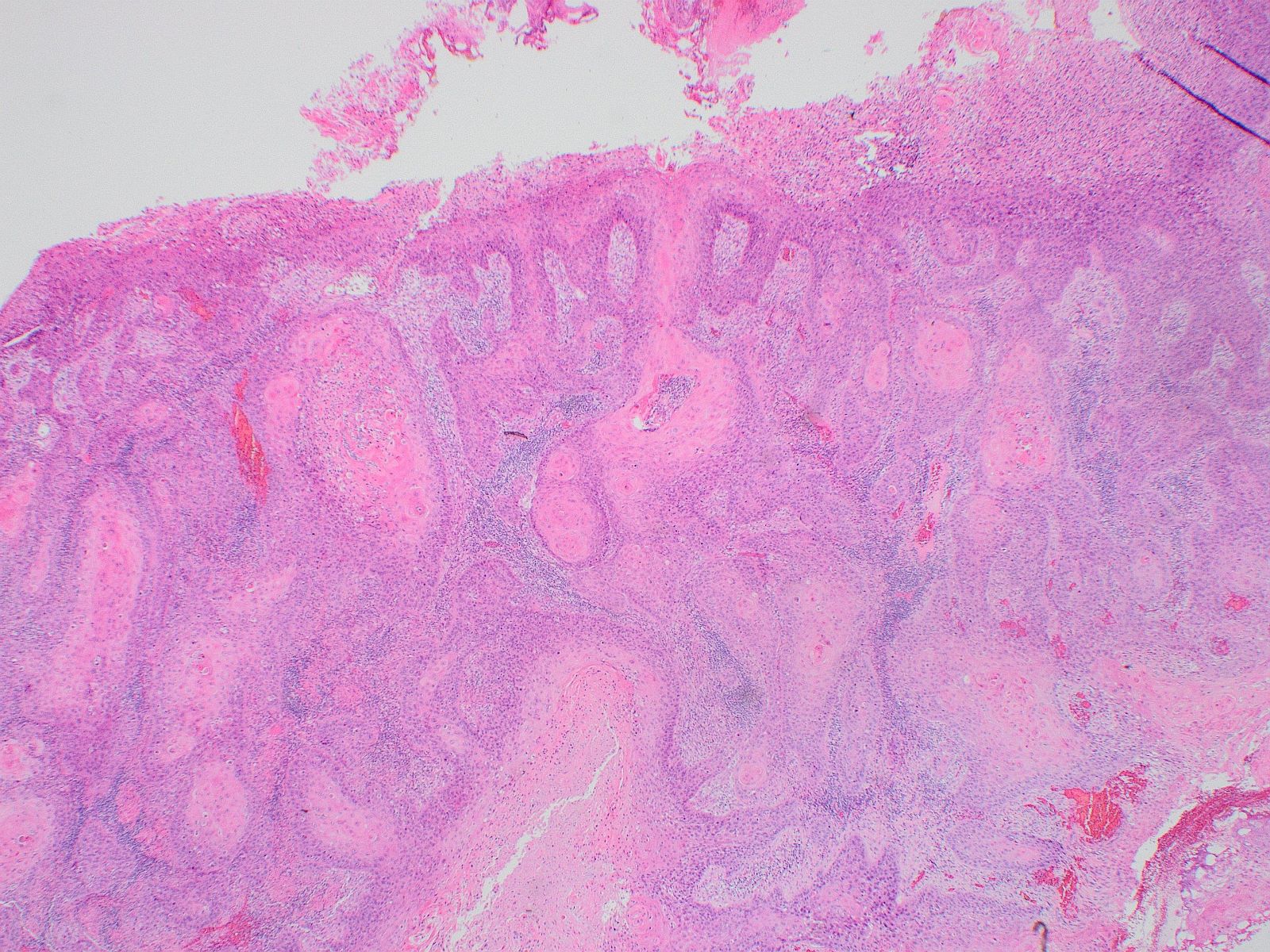
Destructive stromal invasion
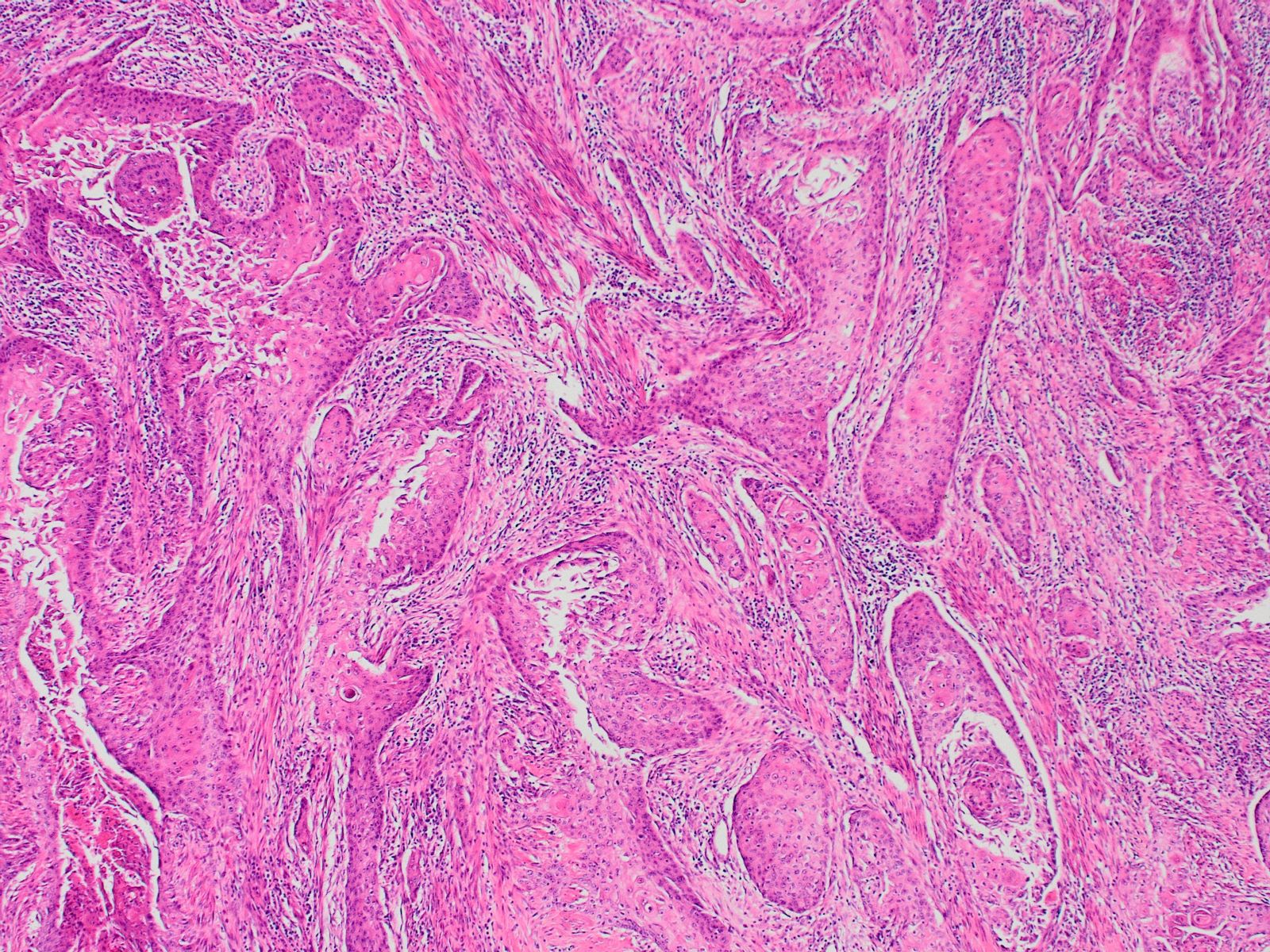
Irregular squamous nests
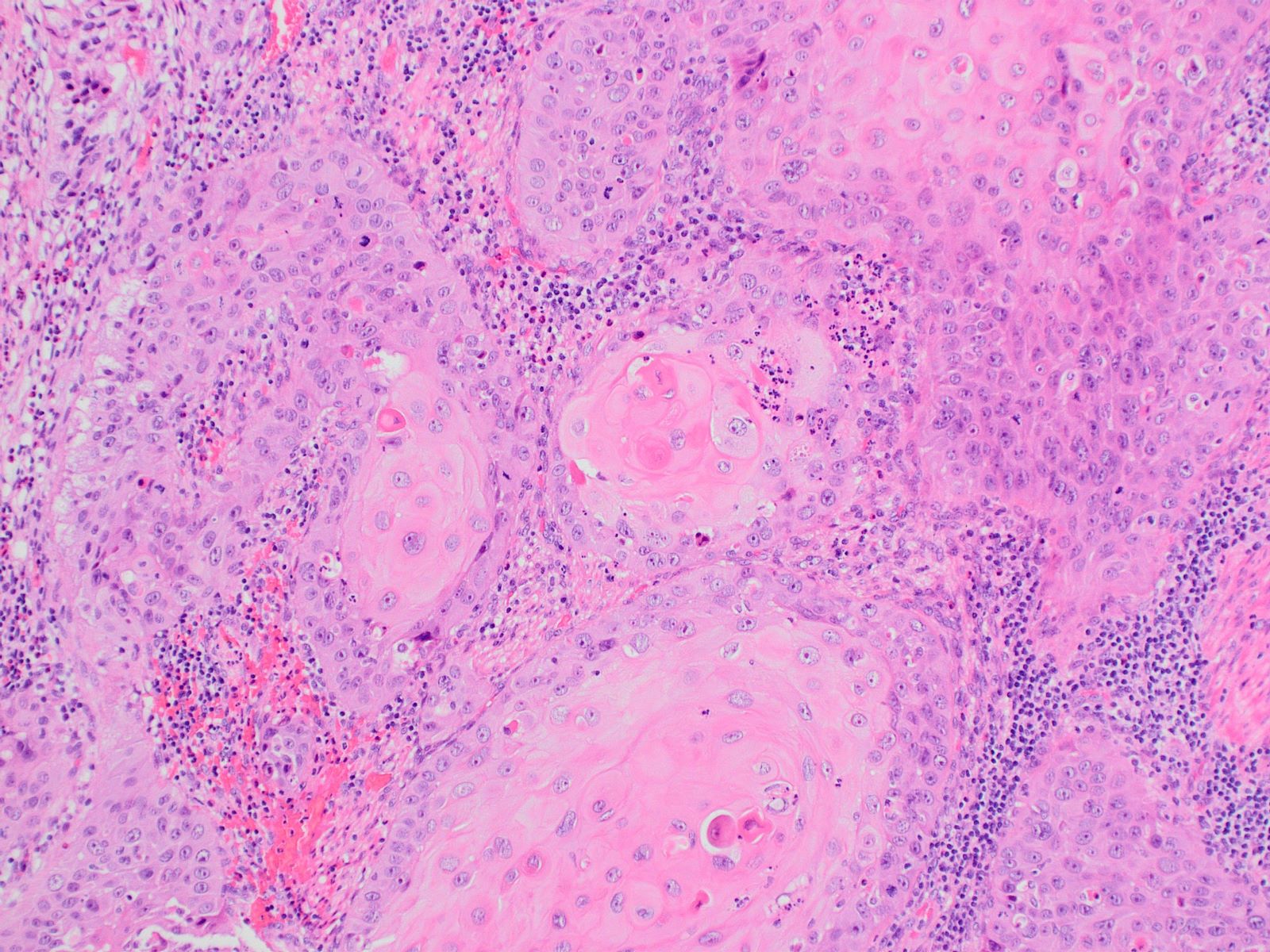
Keratin pearls
Prominent keratinization
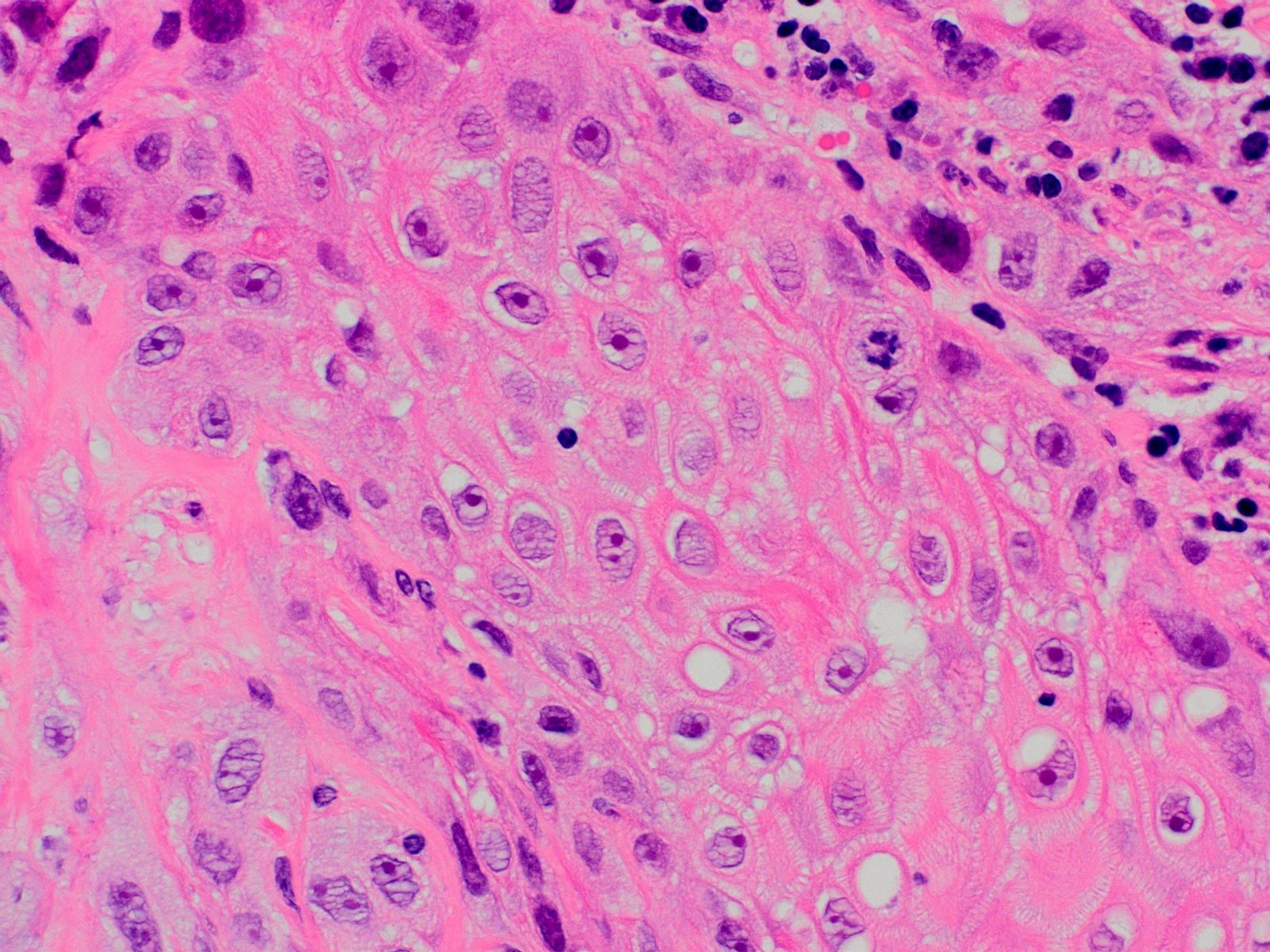
Intercellular bridges
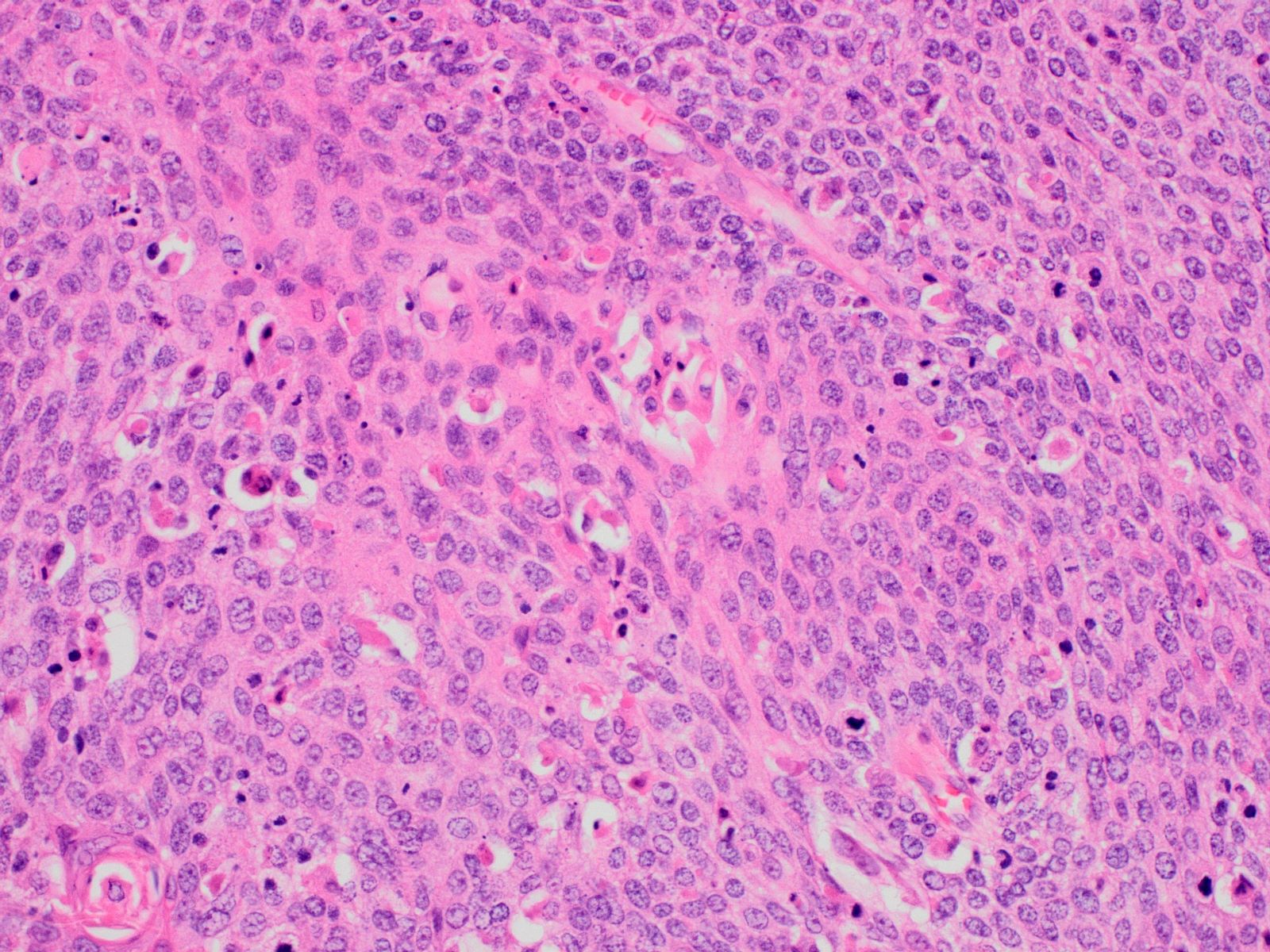
Poorly differentiated tumor
Squamous dysplasia / carcinoma in situ
Invading muscularis propria
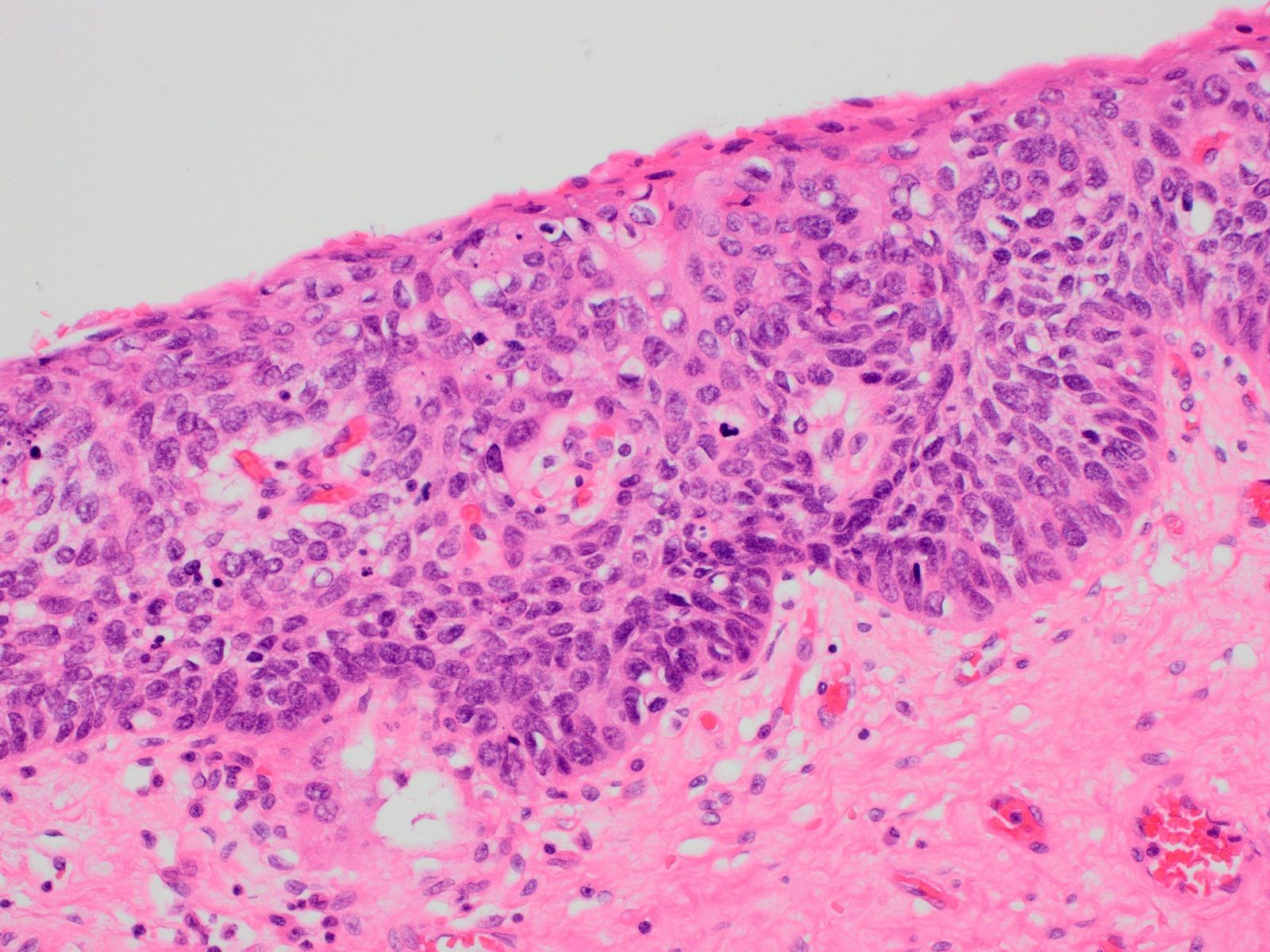
Keratinizing squamous dysplasia
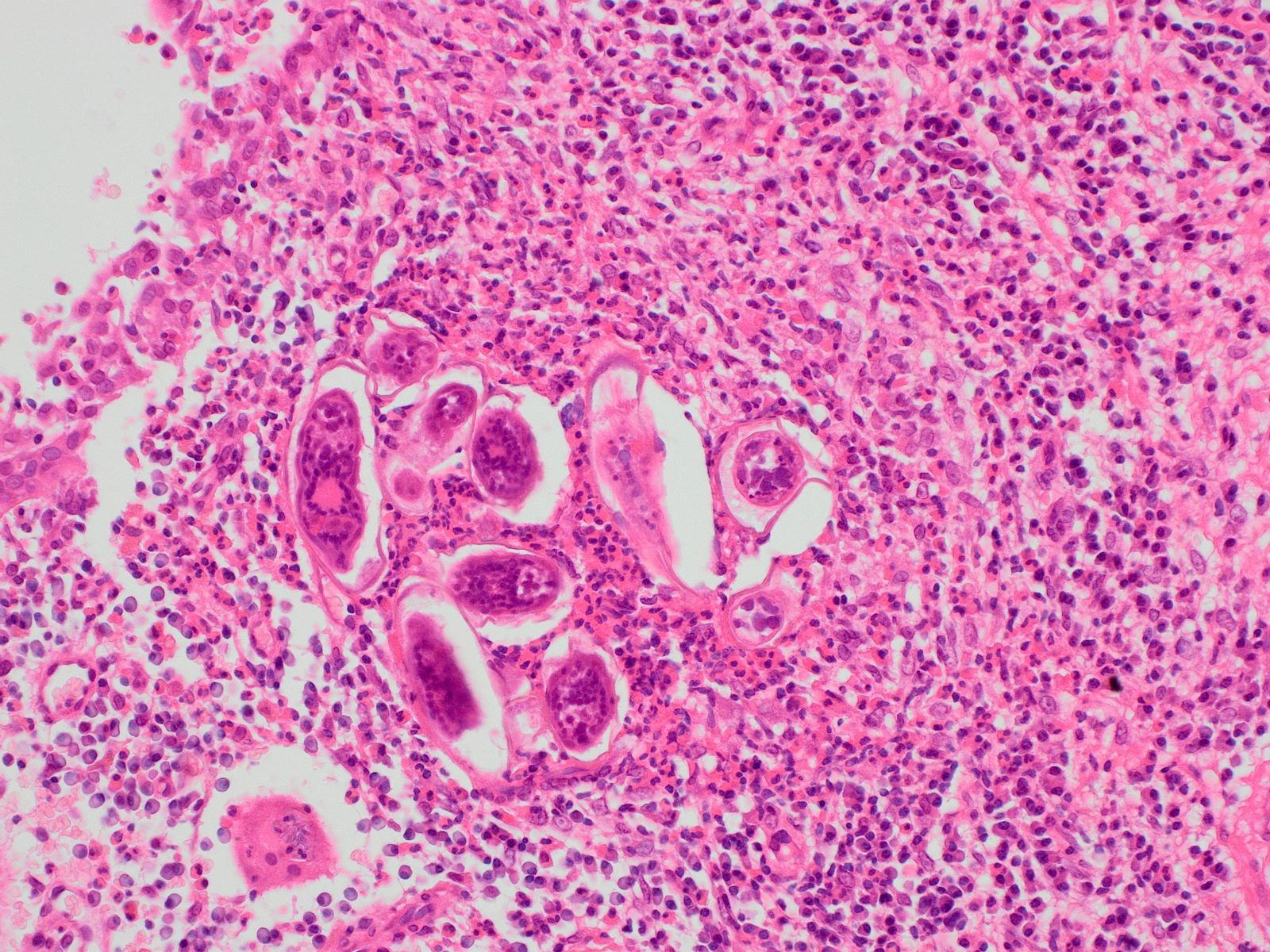
Schistosoma haematobium eggs
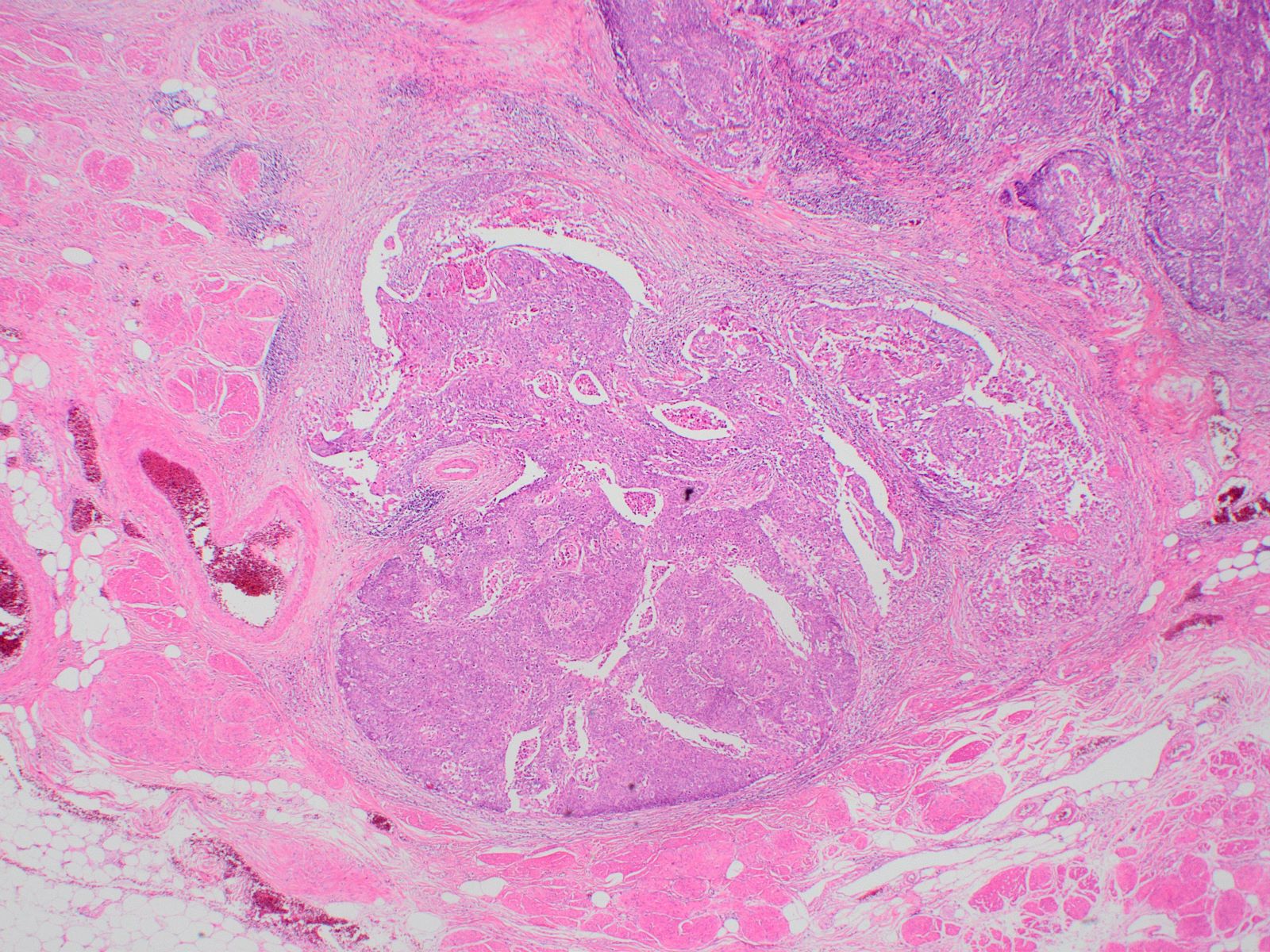
Renal pelvis
Contributed by Nicole K. Andeen, M.D.
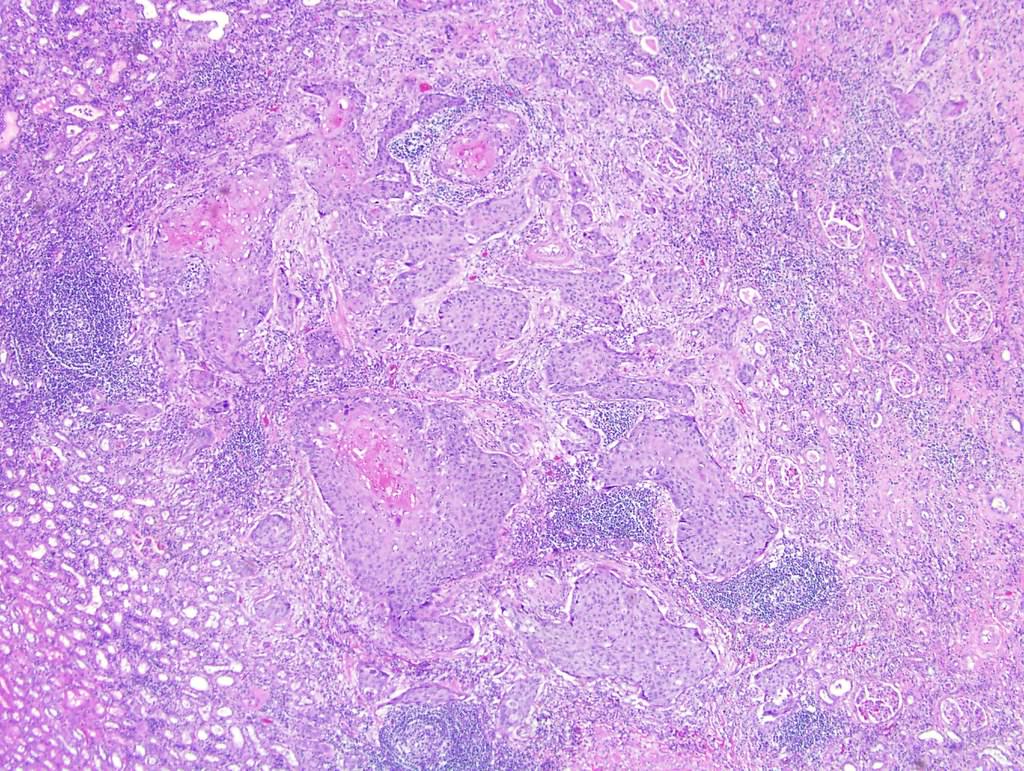
Invasive tumor
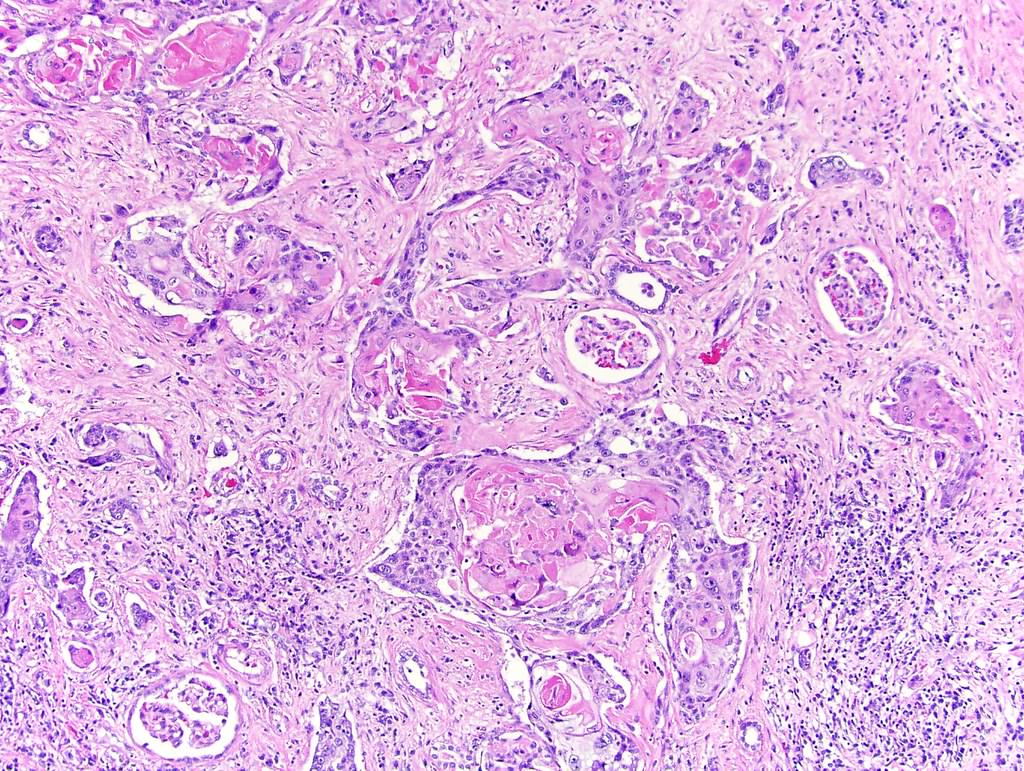
Entrapped glomeruli
No urothelial differentiation
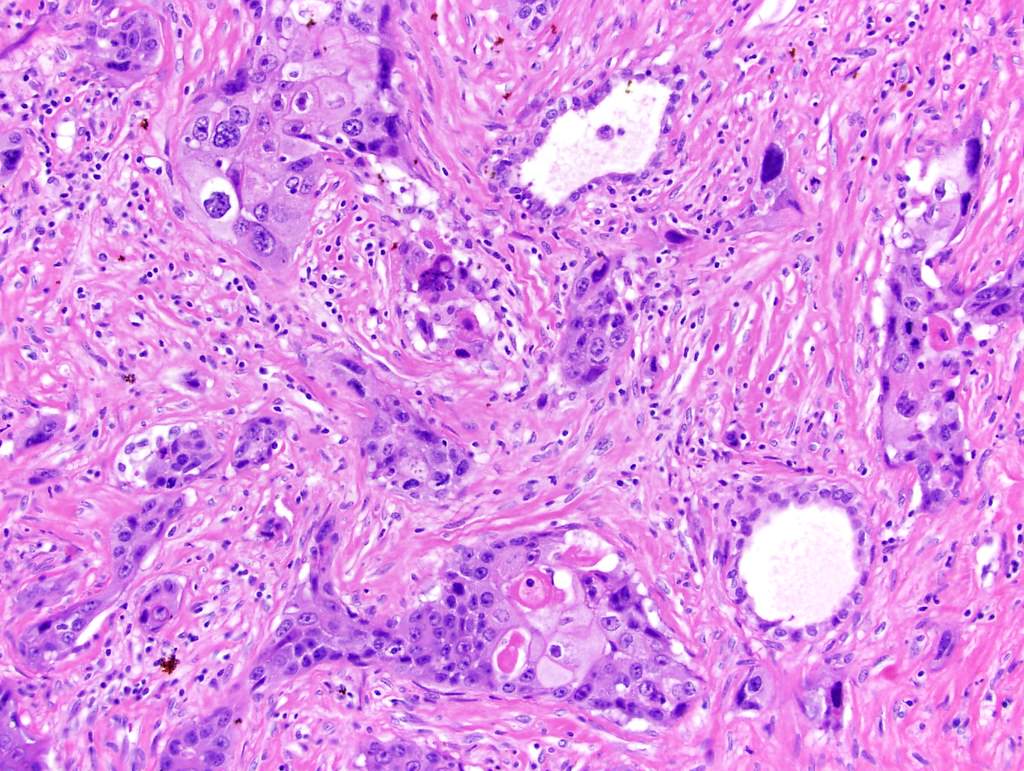
Individual cell keratinization
Entrapped renal tubules
Cytology description
- Keratinized cells demonstrate dense orangeophilic cytoplasm on Pap stain
- Hyperchromatic nuclei with irregular nuclear membranes
- Often necroinflammatory background
Cytology images
Contributed by Susan Prendeville, M.D. and Bonnie Choy, M.D.
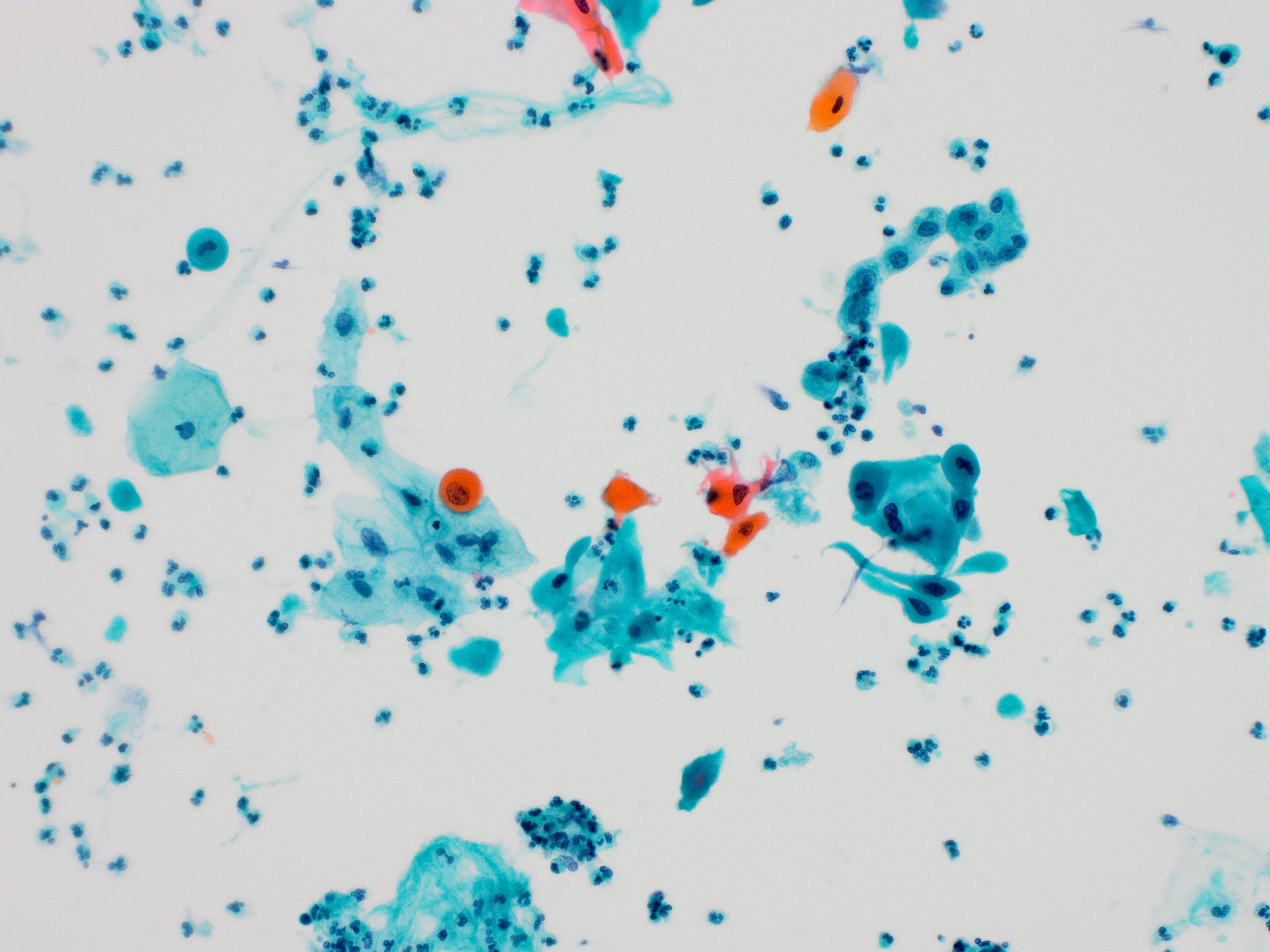
Malignant squamous cells
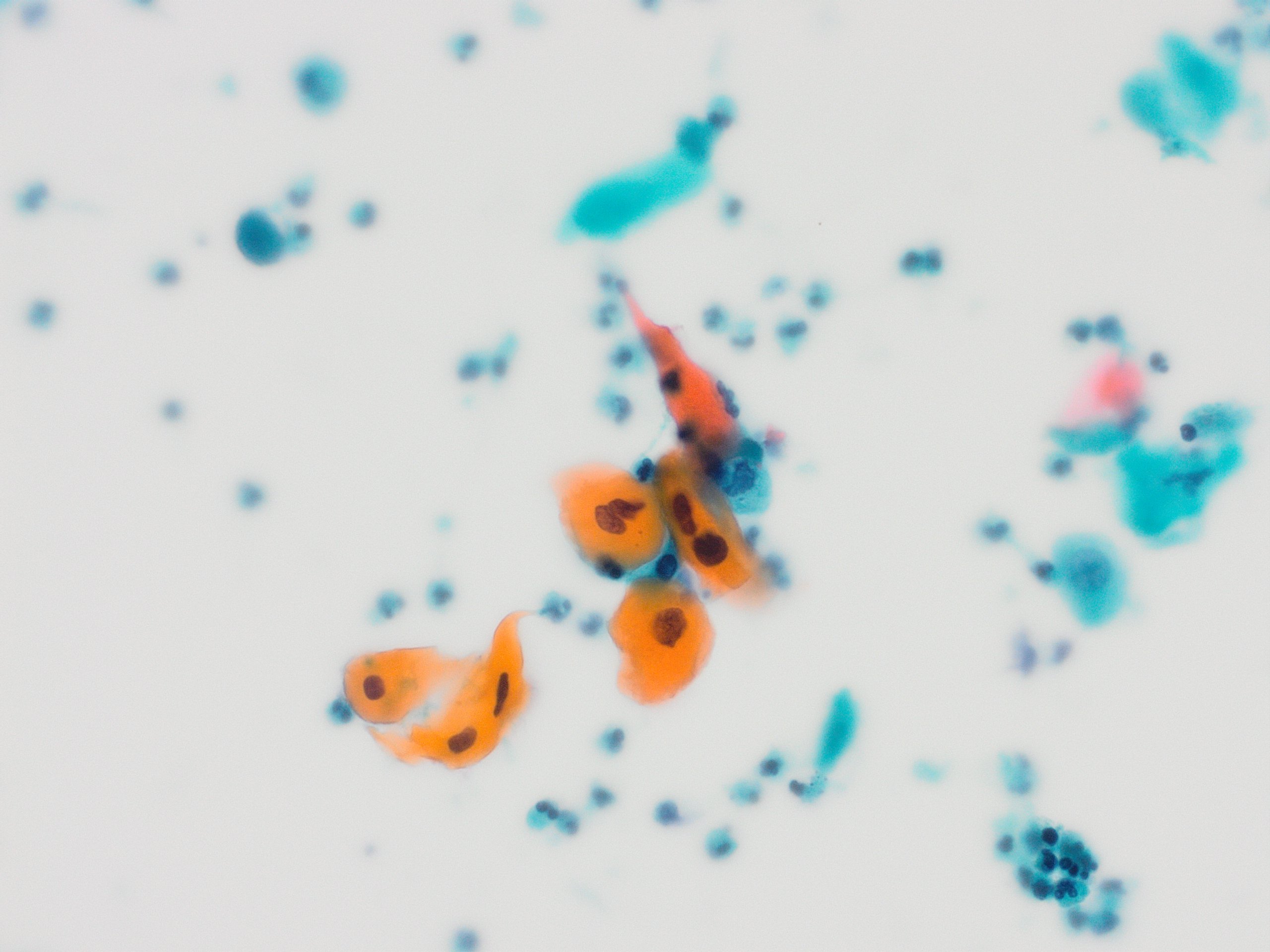
Keratinized malignant cells

Squamous cell carcinoma
Negative stains
- Generally negative or reduced expression of urothelial markers GATA3, uroplakin II, S100P (Hum Pathol 2013;44:164)
- p16 expression in a proportion of cases (25 - 31%); does not correlate with HPV infection (Mod Pathol 2012;25:1526, Urology 2020;144:158, Pathol Res Pract 2020;216:153084)
- CK20
Molecular / cytogenetics description
- HPV DNA in situ hybridization negative; HPV positivity may be seen in association with condyloma or chronic injury (Am J Surg Pathol 2019;43:1547, Urology 2020;144:158)
- Basal / squamous molecular subgroup of muscle invasive bladder cancer show frequent mutations in TP53 and RB1 (Eur Urol 2020;77:420)
Sample pathology report
- Bladder, tumor left lateral wall, transurethral resection:
- Invasive poorly differentiated carcinoma with extensive squamous differentiation
- No evidence of in situ carcinoma (urothelial or squamous) in this biopsy material (see comment)
- Comment: The differential includes pure squamous cell carcinoma and urothelial carcinoma with extensive squamous differentiation. This distinction requires evaluation of the entire resected tumor. In addition, clinical / radiological correlation is advised to ensure the tumor is compatible with a bladder primary.
- Bladder and prostate, robotic radical cystoprostatectomy:
- Bladder with invasive squamous cell carcinoma, moderately differentiated (see synoptic report)
- Prostate, negative for carcinoma
Differential diagnosis
- Urothelial carcinoma with squamous differentiation:
- Squamous differentiation is common in urothelial carcinoma and may be extensive
- Careful search for conventional urothelial carcinoma component or urothelial carcinoma in situ (may be focal)
- Immunohistochemistry is of limited utility in this differential due to overlapping profiles; a panel approach may aid diagnosis in some cases: (squamous markers CK14 / desmoglein 3 with urothelial markers GATA3 / uroplakin / S100P) (Hum Pathol 2013;44:164)
- Metastasis or direct extension of squamous cell carcinoma primary to another site, e.g. cervix, penis, anus:
- Requires clinical and radiological correlation
- p16 expression not of use in this differential
- In situ hybridization for HPV DNA supports cervical primary (expressed in majority of cervical but not bladder squamous cell carcinoma) (Am J Surg Pathol 2014;38:e20)
- Verrucous squamous cell carcinoma:
- Well differentiated tumor showing minimal cytologic atypia
- Hyperkeratotic papillary or undulating projections with a pushing type of invasion at the base comprising rounded, broad based tongues of epithelium
- Absence of irregular infiltrating nests
Board review style question #1
A 65 year old man underwent radical cystectomy for a bladder mass and the entire tumor looked like the histologic image shown above. Which of the following is true regarding this type of tumor arising in the urinary bladder?
- Gross examination usually shows a small tumor
- Hematuria is not a clinical feature
- It is associated with Schistosoma haematobium infection
- It is the most common type of bladder carcinoma
- Smoking is not a risk factor
Board review style answer #1
C. It is associated with Schistosoma haematobium infection
Comment Here
Reference: Bladder squamous cell carcinoma
Comment Here
Reference: Bladder squamous cell carcinoma
Board review style question #2
Which of the following is true about squamous cell carcinoma of the urinary bladder?
- It is associated with keratinizing squamous metaplasia / dysplasia of the bladder mucosa
- It is negative for CK5/6
- It is negative for p63
- It is the same as urothelial carcinoma with squamous differentiation
- p16 immunohistochemistry is reliable to distinguish between a bladder and cervical primary
Board review style answer #2
A. It is associated with keratinizing squamous metaplasia / dysplasia of the bladder mucosa
Comment Here
Reference: Bladder squamous cell carcinoma
Comment Here
Reference: Bladder squamous cell carcinoma
