
Appendix
Other nonneoplastic
Inverted appendix
Editorial Board Member: Maryam Kherad Pezhouh, M.D., M.Sc.
Deputy Editor-in-Chief: Aaron R. Huber, D.O.


Last author update: 13 December 2023
Last staff update: 13 December 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Inverted appendix
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Azimpouran M, Hutchings D. Inverted appendix. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/appendixinverted.html. Accessed April 19th, 2024.
Definition / general
- Appendix that inverts / intussuscepts and is pulled into the lumen of the cecum
Essential features
- Inverted appendix may appear as a polyp or mass in the cecum on endoscopy or imaging
- Histological clues on endoscopically retrieved specimens include
- Dome-like tissue configuration with mucosa on the convex surface
- Deep, smooth muscle component with ganglion cells (muscularis propria)
- Lymphoid aggregates or prominent submucosal adipose tissue
Terminology
- Appendiceal intussusception
ICD coding
Epidemiology
- Prevalence is estimated at 0.01% (Am J Proctol 1963:14:265)
- Most common in adult women, in the fourth to fifth decade of life (Am J Proctol 1963:14:265, Am J Surg 2009;198:122)
Sites
- Appendix; may involve distal or proximal portion giving rise to complete or partial inversion (Dis Colon Rectum 1984;27:387)
- Cecum
Pathophysiology
- Abnormal peristalsis secondary to irritation of appendix or cecum (Int J Colorectal Dis 2000;15:185)
- Anatomical factors (Int J Colorectal Dis 2000;15:185)
- Mobile mesoappendix
- Large appendiceal orifice
- Masses
- May be associated with endometriosis or appendiceal neoplasms (Histopathology 2019;74:853)
Etiology
- Can occur without any underlying abnormality (Histopathology 2019;74:853)
- May be associated with anatomical variations (e.g., mobile mesoappendix or large appendiceal orifice) (Int J Colorectal Dis 2000;15:185)
- May be associated with pathologic conditions (e.g., appendiceal neoplasms, endometriosis, parasites, cystic fibrosis, foreign bodies) (Histopathology 2019;74:853)
Clinical features
- Asymptomatic
- Abdominal pain, nausea / vomiting or melena (Am J Surg 2009;198:122)
Diagnosis
- Endoscopically appears as an elongated or polypoid mass, depending upon whether the entire appendix or only the proximal portion is inverted (Am J Surg 2009;198:122)
- May be biopsied as polyp (Histopathology 2019;74:853)
Radiology description
- Computed tomography (CT) scan: target or sausage shaped lesion (Abdom Radiol (NY) 2016;41:568)
- Ultrasound: target sign with a cystic structure < 6 mm in diameter in the center of the target (Abdom Radiol (NY) 2016;41:568)
- Barium enema: coiled spring sign or filling defect in the cecum with absence of filling of the appendix (Abdom Radiol (NY) 2016;41:568)
Radiology images
Images hosted on other servers:

CT demonstrating an intraluminal tubular structure

Intraluminal protruding mass with central fat component

Cecal thickening without visualization of appendix
Prognostic factors
- Benign lesion, unless it arises in associated with an underlying neoplasm
- Rarely, perforation with associated peritonitis may occur in polypectomy specimens (Am J Gastroenterol 1982;77:556)
Case reports
- 10 year old boy with 3 days of recurrent intermittent mild abdominal pain (Medicine (Baltimore) 2020;99:e23452)
- 39 year old woman with a 5 week history of worsening right sided sharp and burning abdominal pain (J Surg Case Rep 2018;2018:rjy044)
- 50 year old woman with cecal lesion seen on routine colonoscopy (Radiol Case Rep 2019;14:952)
- 60 year old woman with complaints of intermittent abdominal pain (BMC Surg 2019;19:168)
Treatment
- Appendectomy with resection of cecal cuff is typically recommended to reduce risk of recurrence (Am J Surg 2009;198:122)
Clinical images
Images hosted on other servers:

Elongated lesion at appendiceal orifice

Tubular structure in cecum

Endoscopy
Gross description
- Elongated to polypoid mass in the proximal cecum at the usual location of the appendiceal orifice
- May show foreskin and glans-like morphology (Histopathology 2019;74:853)
- Anatomical classification of inverted appendix; McSwain classification: 5 types of appendiceal intussusceptions (Am J Surg 2009;198:122)
- Type I: tip of the appendix is invaginated into the proximal appendix
- Type II: invagination starts at some point along the length of the appendix and the intussusception is the appendiceal body
- Type III: invagination starts at the junction of the appendix and cecum; the intussusception is the cecum
- Type IV: proximal appendix is invaginated into the distal appendix; retrograde intussusception
- Type V: appendix is completely invaginated into the cecum
Gross images
Contributed by Mahzad Azimpouran, M.D. and Danielle Hutchings, M.D.

Elongated tubular lesion

Inversion of appendiceal base

Associated with mucinous neoplasm

Serosal surface
Microscopic (histologic) description
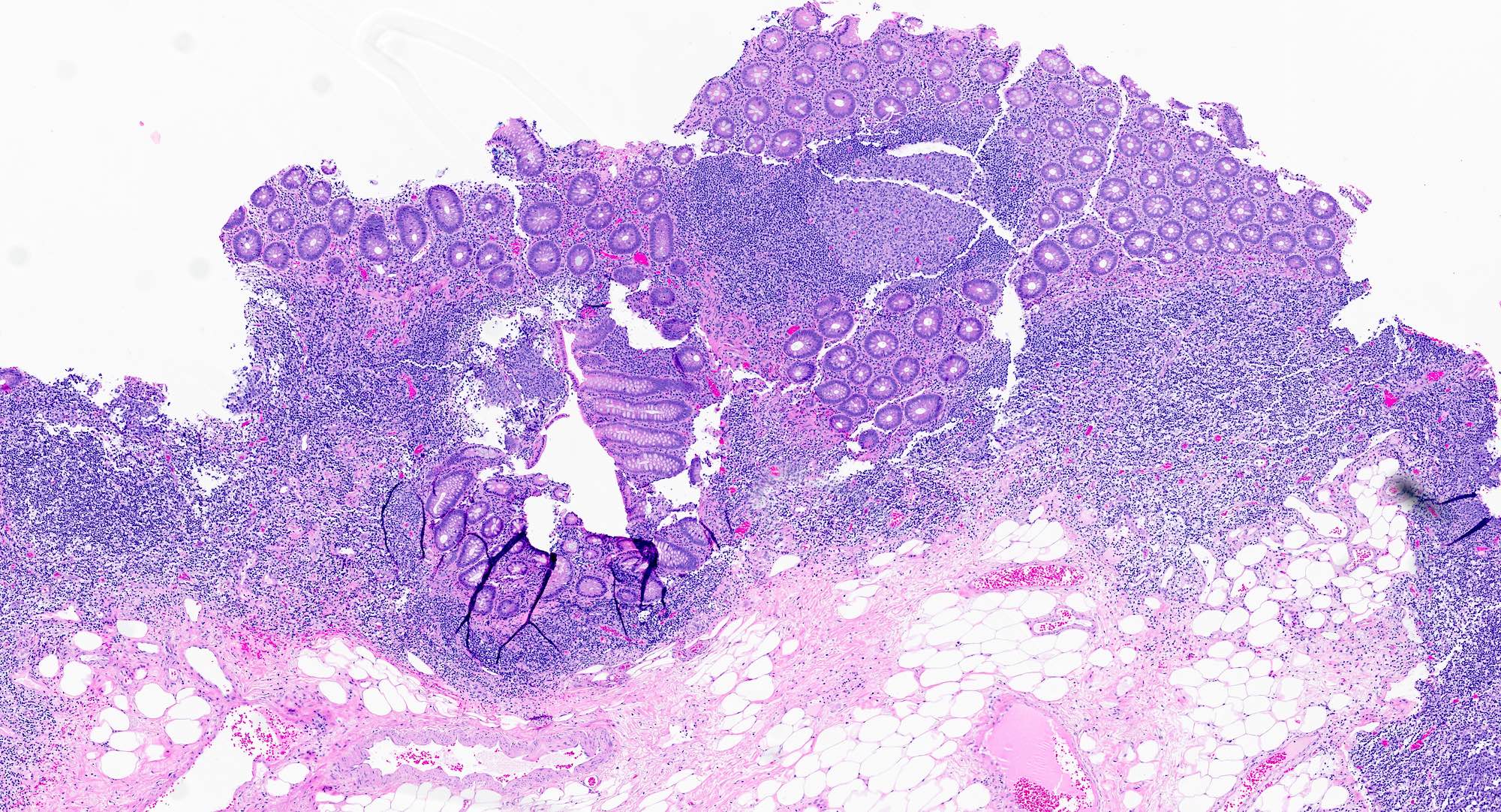
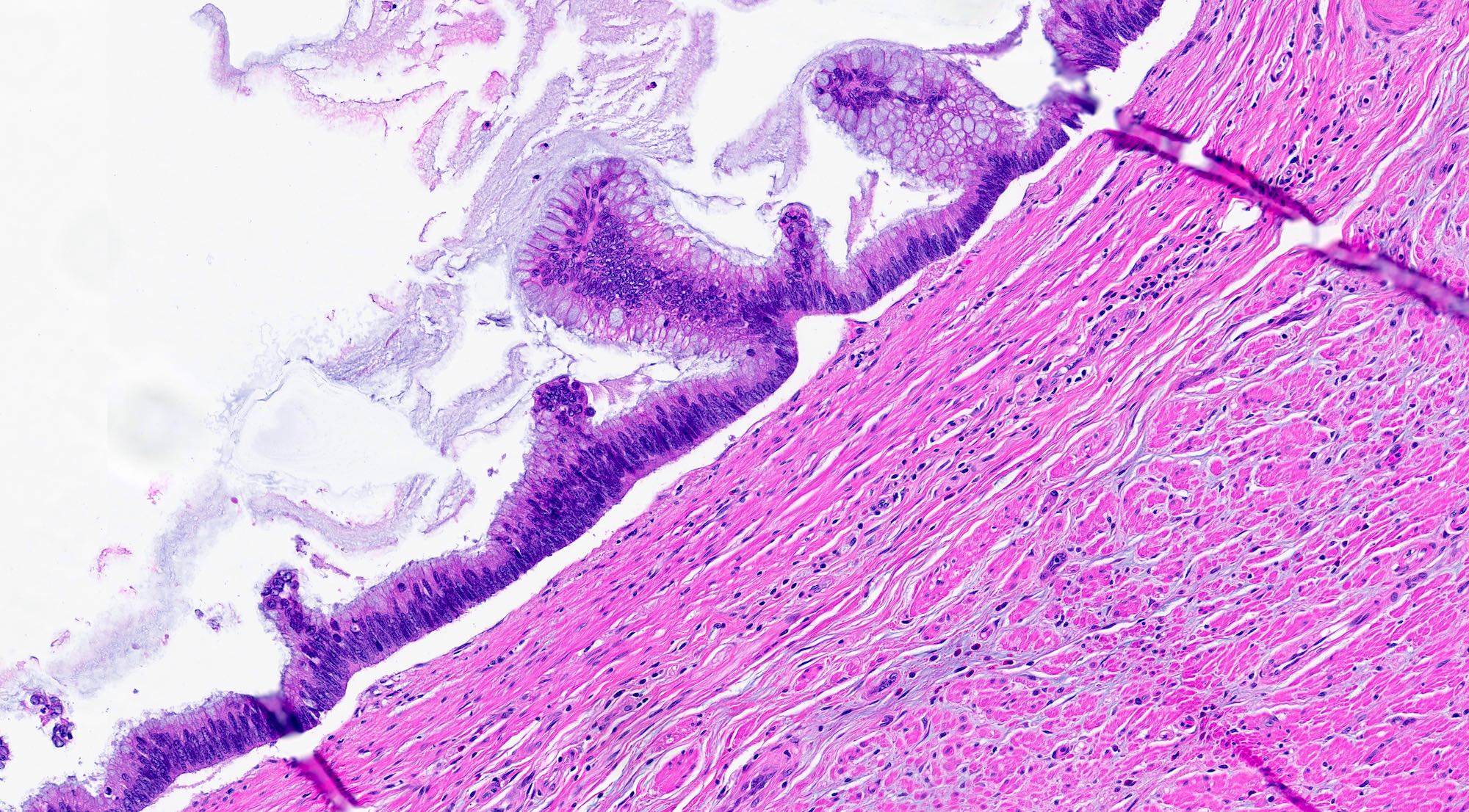
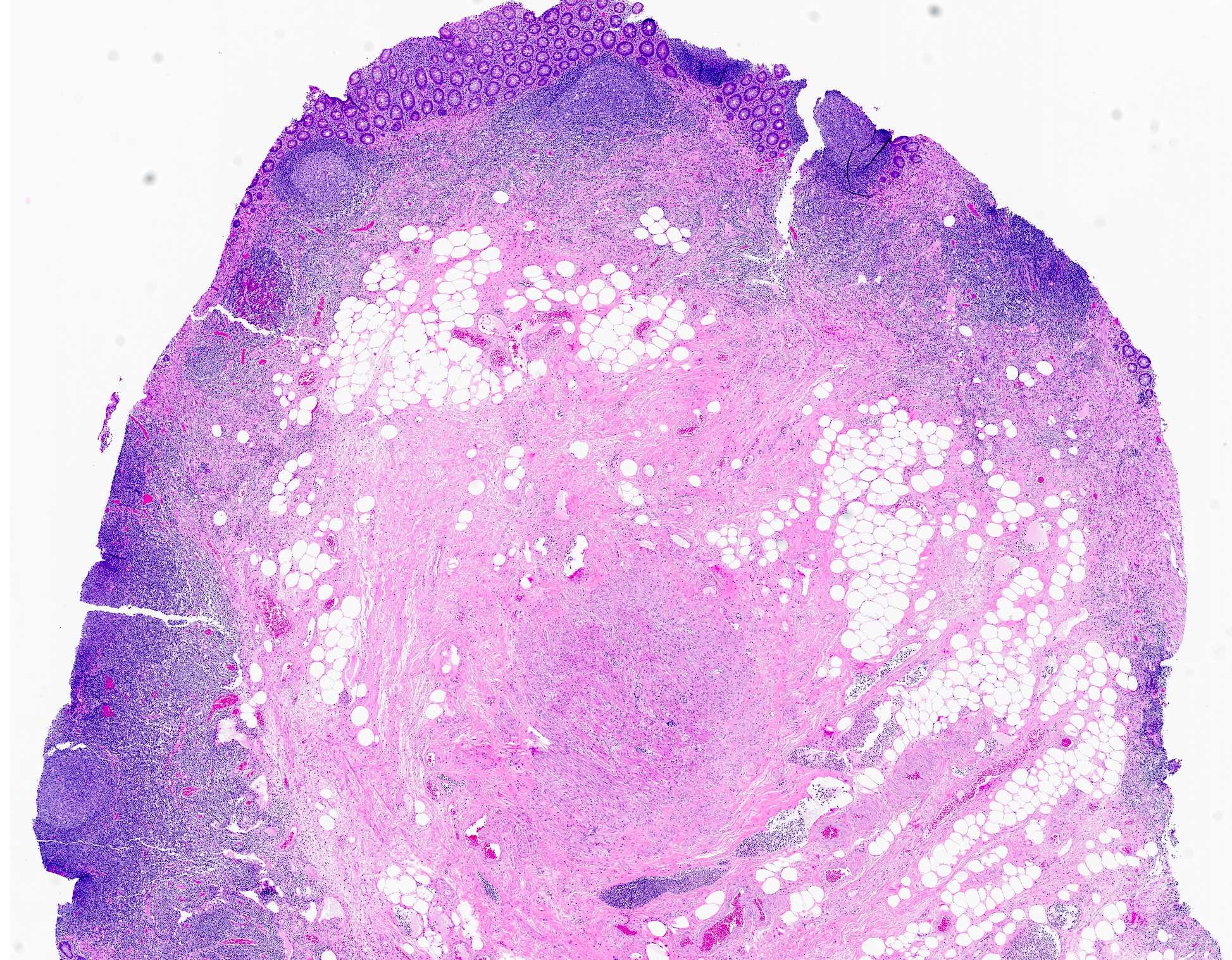
- Dome shaped configuration of tissue covered by colonic mucosa on the outer surface
- Presence of thick smooth muscle with ganglion cells (muscularis propria)
- Lymphoid aggregates
- Submucosal adipose tissue
- Reference: Histopathology 2019;74:853
Microscopic (histologic) images
Contributed by Mahzad Azimpouran, M.D. and Danielle Hutchings, M.D.
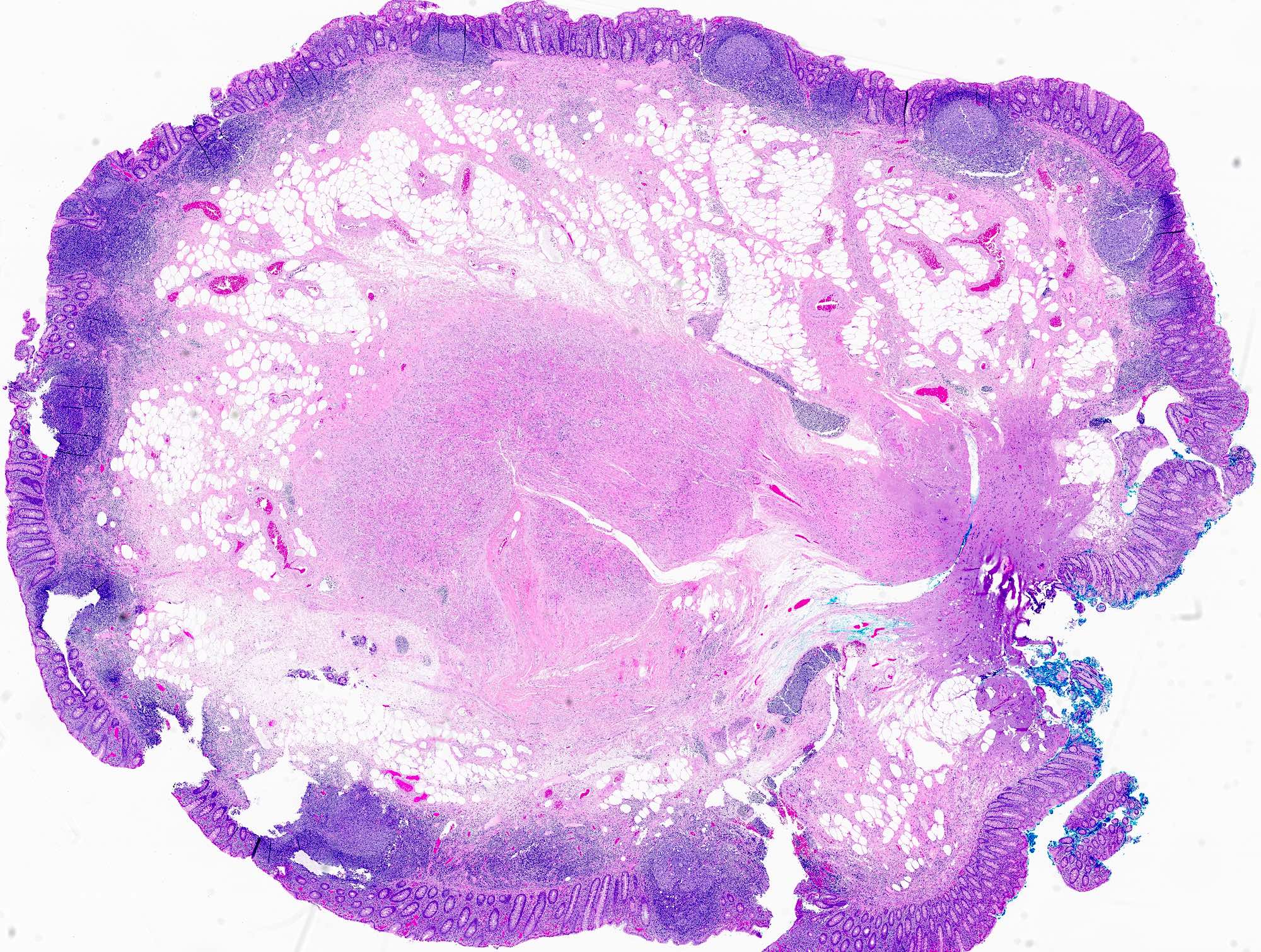
Dome shaped configuration
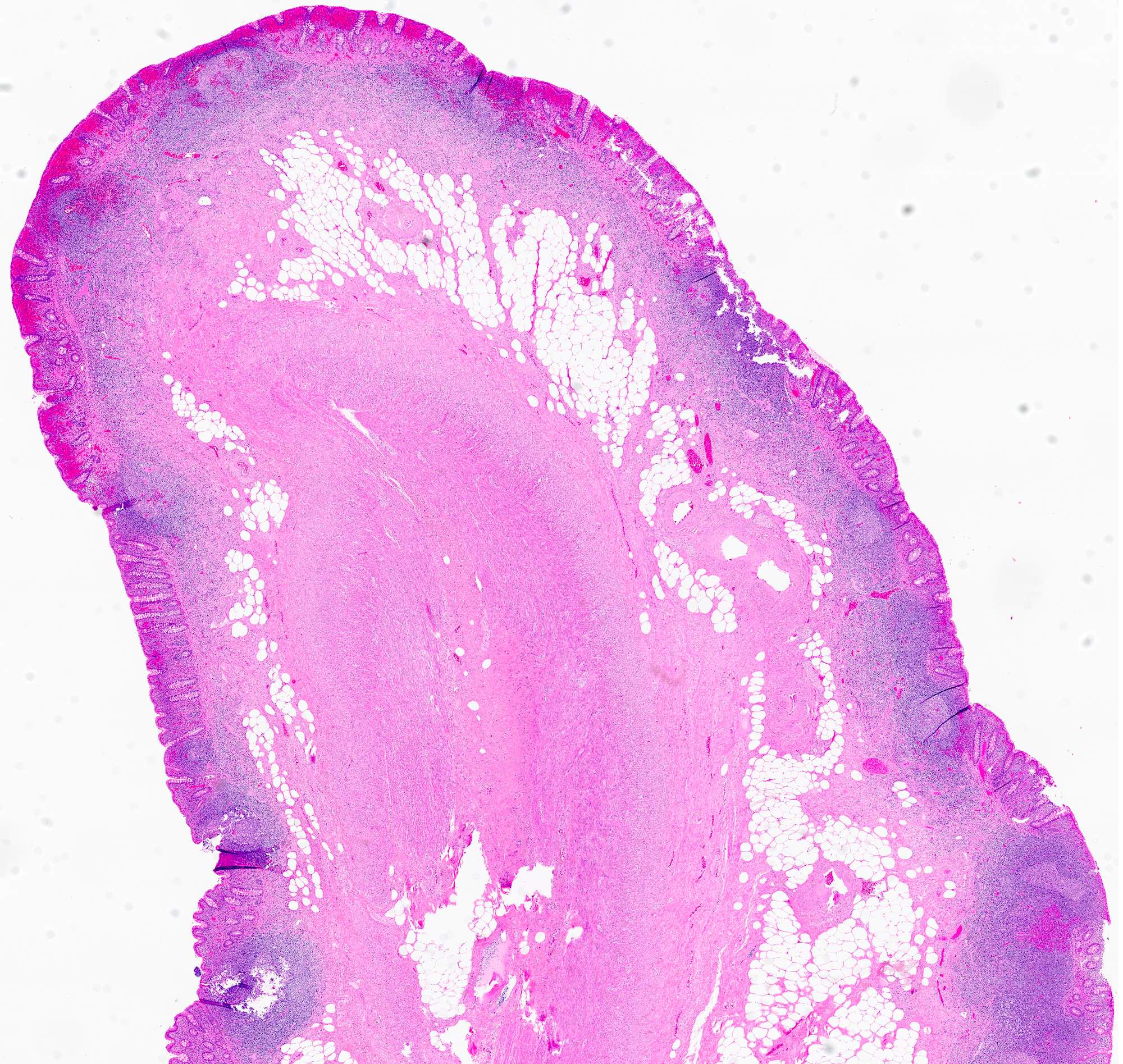
Polypoid configuration
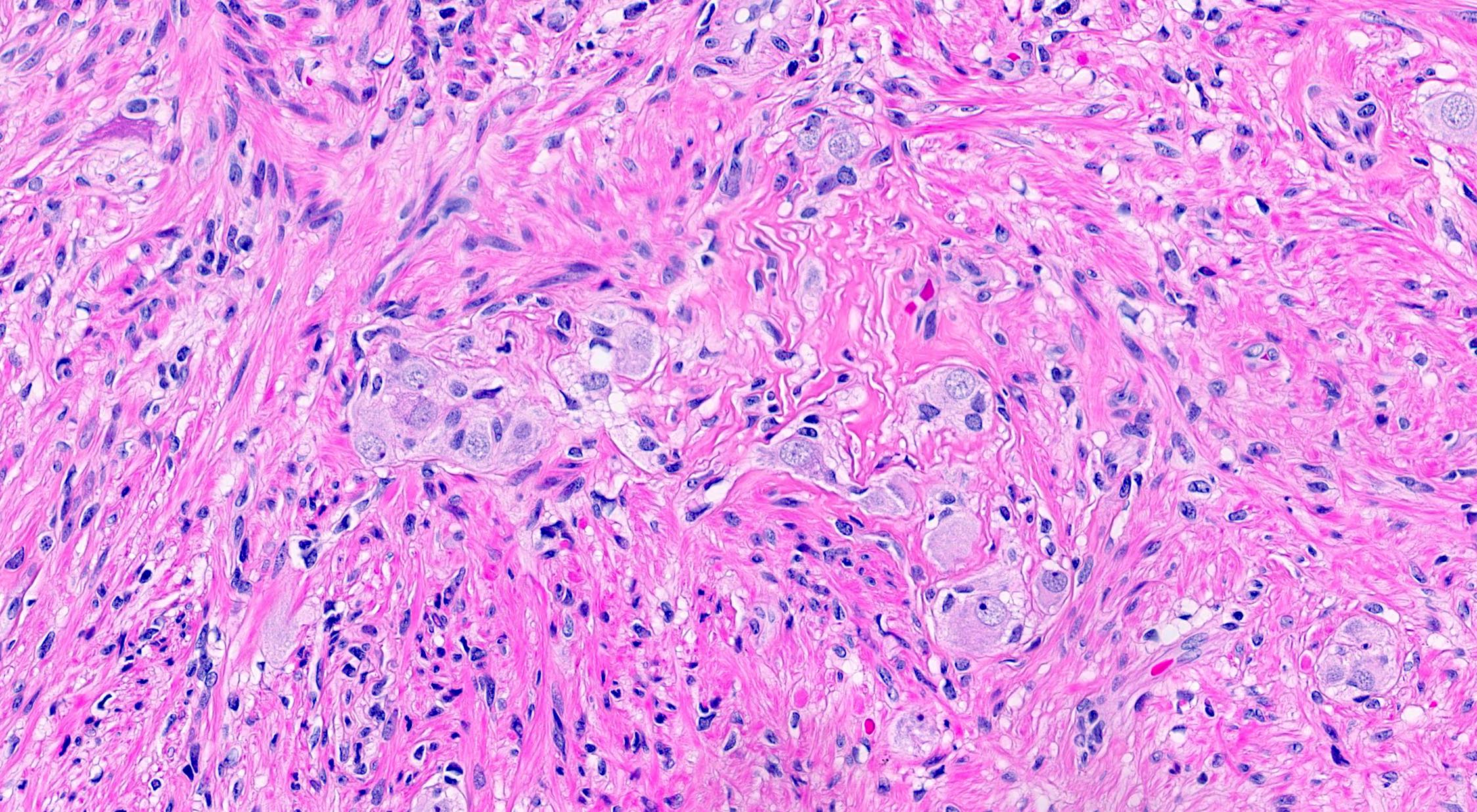
Ganglion cell aggregates
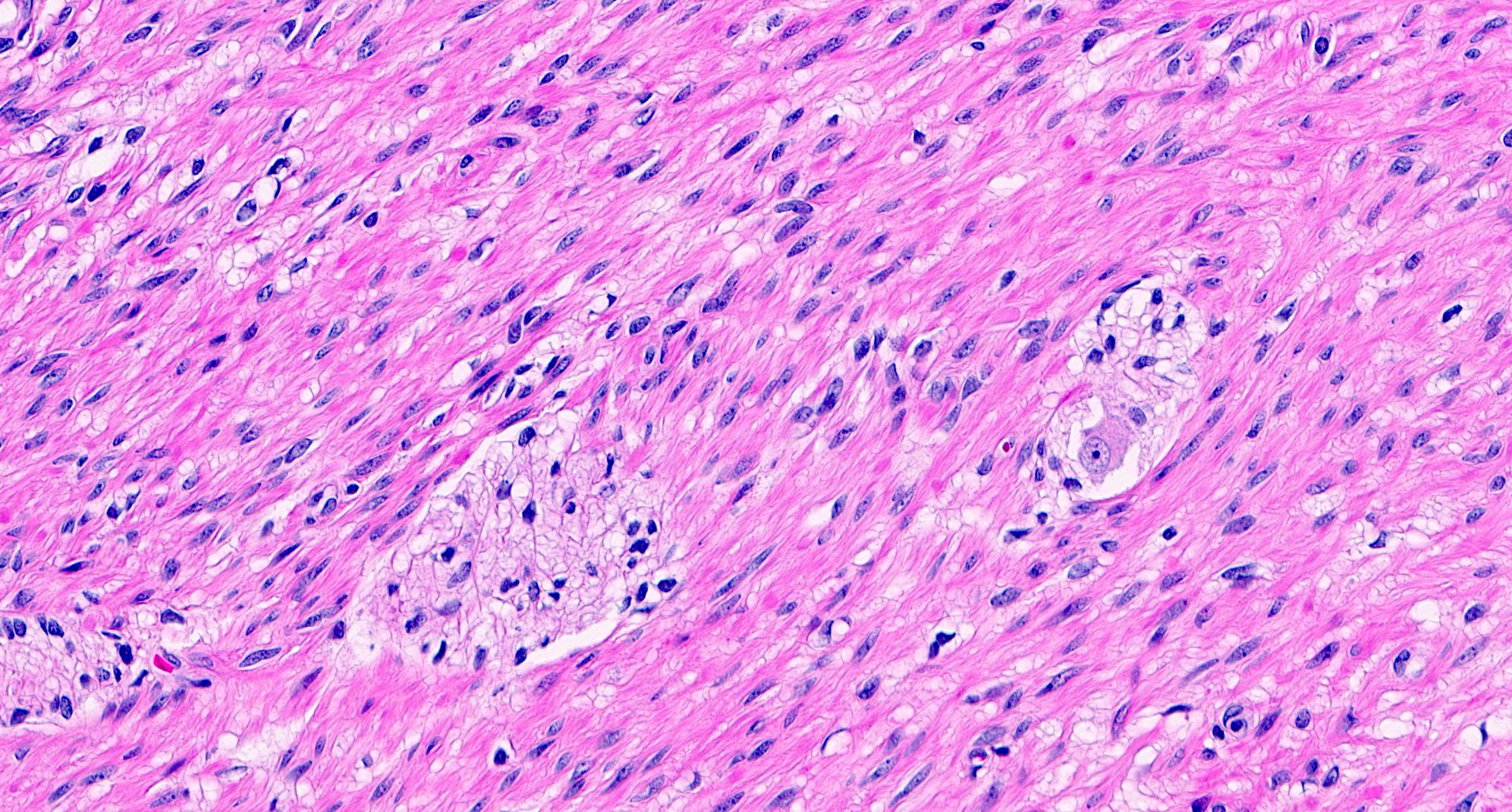
Ganglion cells and nerves
Lymphoid aggregates
Appendiceal mucinous neoplasm
Positive stains
Sample pathology report
- Appendix, appendectomy:
- Inverted appendix
- No dysplasia or malignancy identified
- Cecal polyp, polypectomy:
- Polypoid colonic tissue with underlying adipose tissue and muscularis propria consistent with inverted appendix
Differential diagnosis
- Polyps:
- Microscopic findings depend on the type of polyp (e.g., adenoma, sessile serrated lesion)
- May show dysplasia
- Ileocecal intussusception:
- Most common in infants and young children (Gastroenterol Res Pract 2009:2009:579501)
- Abdominal ultrasound is the helpful for preoperative diagnosis (Gastroenterol Res Pract 2009:2009:579501)
- Lipoma:
- Benign, well circumscribed adipose tissue
- Lack of muscularis propria
- Leiomyoma:
- Majority arise in rectosigmoid (Arch Pathol Lab Med 2011;135:1311)
- Lack interspersed ganglion cells and nerves of myenteric plexus
- Ganglioneuroma:
Additional references
Board review style question #1
A 44 year old woman underwent screening colonoscopy. The endoscopist noted a polypoid mass arising in the cecum and performed endoscopic polypectomy. The findings are pictured above. Which of the following is a key microscopic feature of this entity?
- Absence of ganglion cells
- Absence of submucosal adipose tissue
- Ganglion cells embedded in thick smooth muscle bundles
- Sessile configuration of the lesion
Board review style answer #1
C. Ganglion cells embedded in thick smooth muscle bundles. The presence of thick smooth muscle bundles of muscularis propria containing ganglion cells and nerve fibers is a key microscopic feature. Answer B is incorrect because the presence, rather than absence, of submucosal adipose tissue is a microscopic feature of inverted appendix. Answer A is incorrect because the presence of ganglion cells is a key to the identification of muscularis propria. Answer D is incorrect because the lesion is typically elongated, polypoid or dome shaped rather than sessile.
Comment Here
Reference: Inverted appendix
Comment Here
Reference: Inverted appendix
Board review style question #2
A 56 year old woman with a history of cecal mass on imaging underwent partial cecectomy with appendectomy. The gross findings are pictured above. What is true of this diagnosis?
- It is associated with endometriosis
- More common in men than women
- Resection of the lesion is necessary for the diagnosis
- Resection was inappropriate management for this patient
Board review style answer #2
A. It is associated with endometriosis. The lesion shown is an inverted appendix, which can occur without any underlying abnormality or may be associated with anatomical variations or pathologic conditions, such as endometriosis or appendiceal neoplasm. Answer B is incorrect because inverted appendix is more common in women than men. Answer C is incorrect because though it may be diagnostically challenging in some cases, it is possible to diagnose on radiographic imaging or colonoscopy. Answer D is incorrect because appendectomy with resection of cecal cuff is generally recommended for inverted appendix to avoid recurrence.
Comment Here
Reference: Inverted appendix
Comment Here
Reference: Inverted appendix
