
Chemistry, toxicology & urinalysis
Organ specific
Adrenal
Hyperaldosteronism
Author: Renu Virk, M.D.

Last author update: 1 February 2010
Last staff update: 2 April 2020
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Hyperaldosteronism [title]
Table of Contents
Definition / general | Terminology | Diagrams / tables | Etiology | Clinical features | Laboratory | Diagnosis | Case reports | Treatment | Additional referencesCite this page: Virk R. Hyperaldosteronism. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/adrenalhyperaldosteronism.html. Accessed April 24th, 2024.
Definition / general
- Disorder caused by excess secretion of aldosterone
- See also Adrenal gland - Hyperaldosteronism
Terminology
- Primary hyperaldosteronism: cause is in the adrenal gland
- Secondary hyperaldosteronism: cause is extra-adrenal
- Tertiary hyperaldosteronism: cause is renal juxtaglomerular cells
Diagrams / tables
Images hosted on other servers:
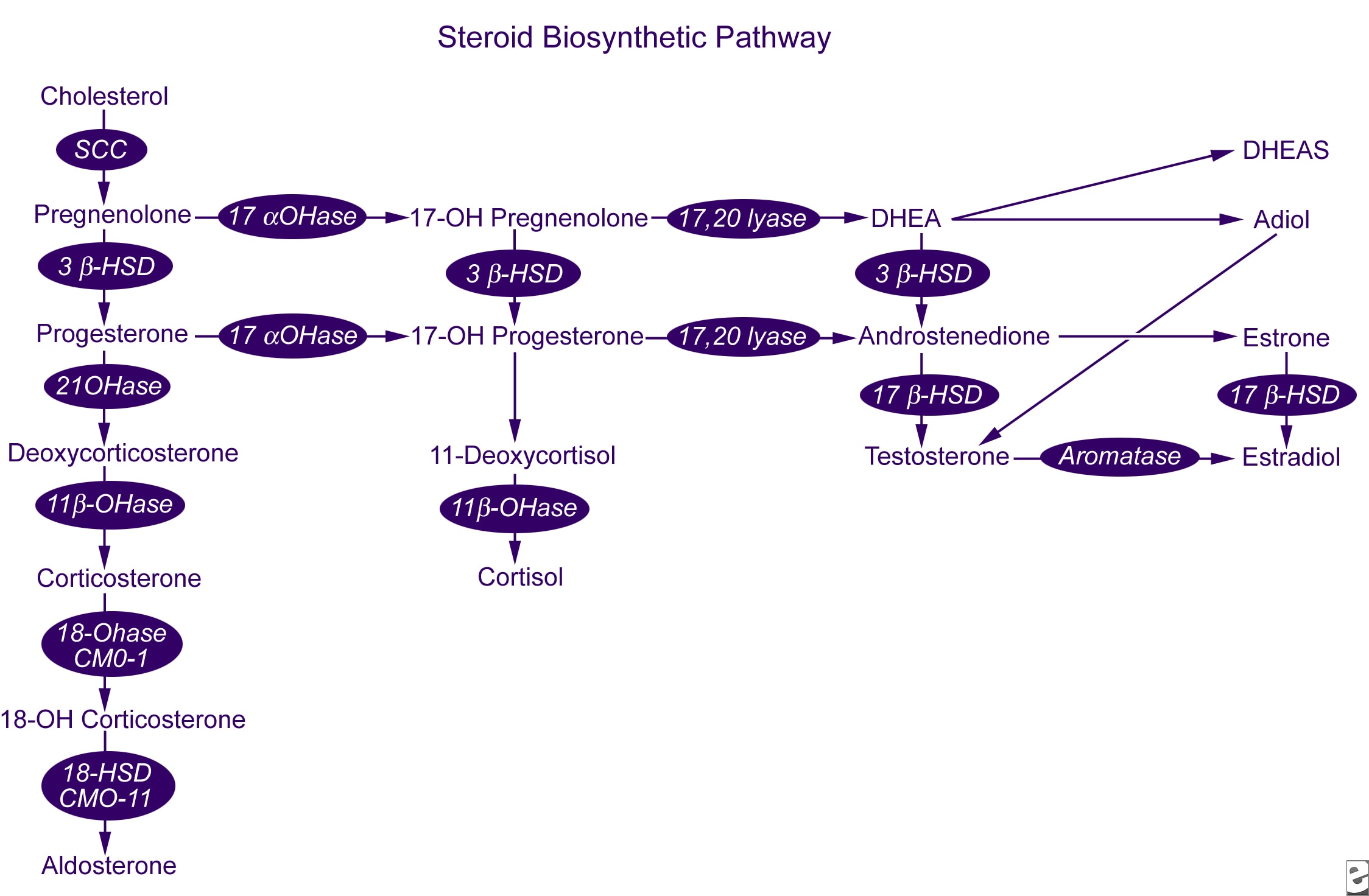
Synthesis pathway
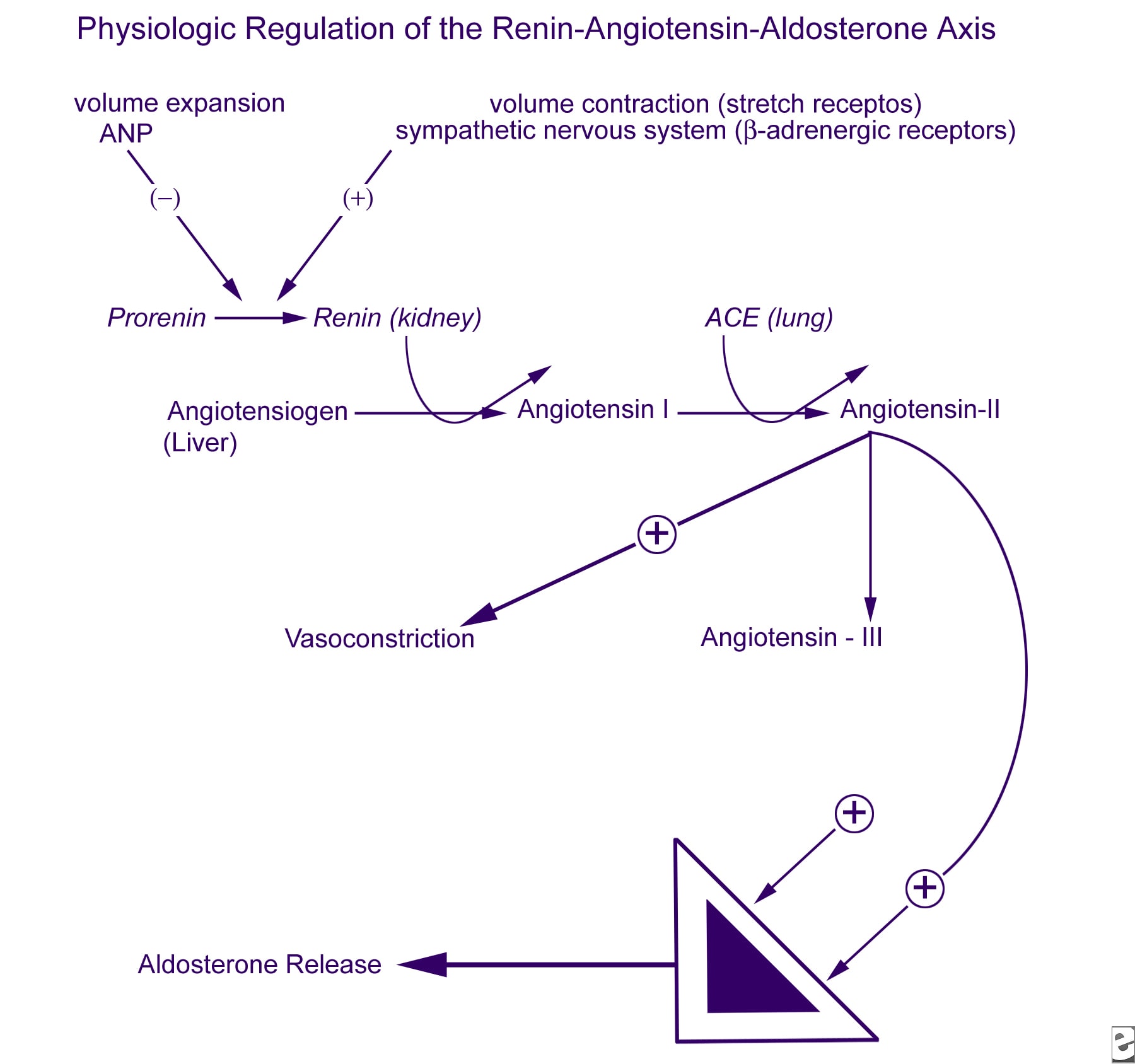
Renin-angiotensinal-dosterone axis

Diagnostic pathways
Etiology
- Primary hyperaldosteronism causes:
- Idiopathic adrenal hyperplasia: most common cause
- Conn syndrome: aldosterone producing adrenal adenoma, rarely adrenal carcinoma
- Secondary hyperaldosteronism causes:
- Increased levels of plasma renin from non-adrenal pathology
- Includes:
- Congestive heart failure
- Pregnancy (due to estrogen)
- Decreased renal perfusion (renal arterial stenosis, nephrosclerosis)
- Gypoalbuminemia
- Ovarian tumor
- Hyperthyroidism
- Tertiary hyperaldosteronism (Bartter syndrome):
- Hypertrophy and hyperplasia of renal juxtaglomerular cells, causing elevated plasma renin, angiotensin II and aldosterone, hypokalemic alkalosis but no hypertension
- Some cases are autosomal recessive
- Infants or adults (eMedicine - Bartter Syndrome, Wikipedia - Bartter syndrome)
- Glucocorticoid suppressible hyperaldosteronism:
- Also called familial hyperaldosteronism type I
- Rare, familial
- Due to mutation which causes developmental derangement of cortical zonation, with hybrid cells between glomerulosa and fasciculata that are under the influence of ACTH, but can be suppressed by dexamethasone
- Familial cases:
- Early onset hypertension and severe target organ damage
Clinical features
- Causes urinary loss of potassium and hypokalemia, sodium retention and hypertension
- May cause up to 14% of cases of refractory hypertension (Arq Bras Cardiol 2009;92:39)
- Hypokalemia (present in 63%, Dtsch Arztebl Int 2009;106:305) causes weakness, paresthesias, visual disturbances, tetany
- Sodium retention causes volume overload which suppresses the renin-angiotensin system and reduces plasma renin activity
- Volume overload causes polyuria, polydipsia, nocturia, hypertension, alkalosis, hypernatremia
Laboratory
- High serum sodium, low serum potassium, metabolic alkalosis
Diagnosis
Tests for primary hyperaldosteronism
- Nonsuppressible aldosterone excretion with normal cortisol excretion, low plasma renin
- Screening tests:
- Preferred screening test is Ratio of plasma aldosterone concentration (PAC, in ng/dl) to plasma renin activity (PRA, in ng/ml/hr)
- Ratio >30 is strongly suggestive of primary hyperaldosteronism
- Confirmatory test:
- Serum aldosterone level, urine aldosterone levels, saline suppression test
Case reports
- 28 year old woman with adrenal adenoma also causing hypocalcemia (J Korean Med Sci 2009;24:1220)
Treatment
- Surgery for adenoma
- Patients with bilateral adrenal hyperplasia need spironolactone or other antihypertensive drugs
Additional references
