















































































































































































































































































Primary tumor (pT)
- pTX: Primary tumor cannot be assessed
- pT0: No evidence of primary tumor
- pTis: Carcinoma in situ
- pT1: Tumor ≤ 2 cm without extraparenchymal extension
- pT2: Tumor > 2 cm but ≤ 4 cm without extraparenchymal extension
- pT3: Tumor > 4 cm or tumor with extraparenchymal extension
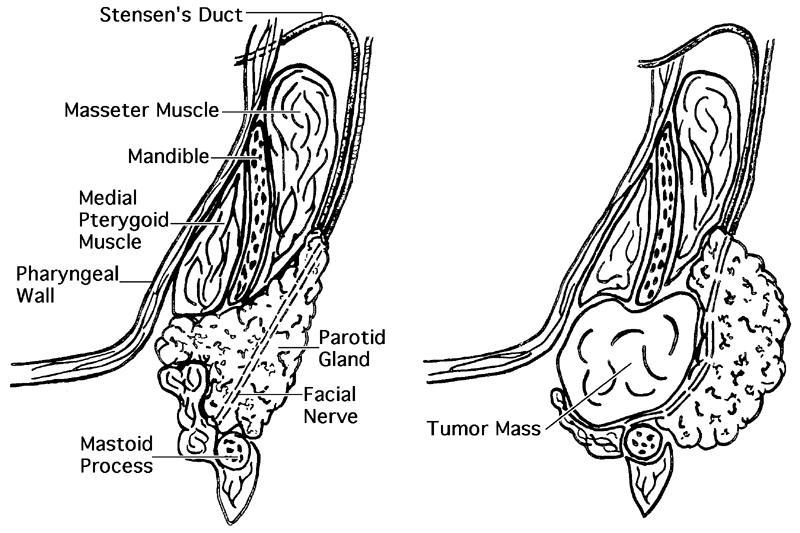
- pT4a: Tumor of any size invading skin, mandible, ear canal or facial nerve
- pT4b: Tumor of any size invading skull base or pterygoid plates or encases carotid artery
Notes:
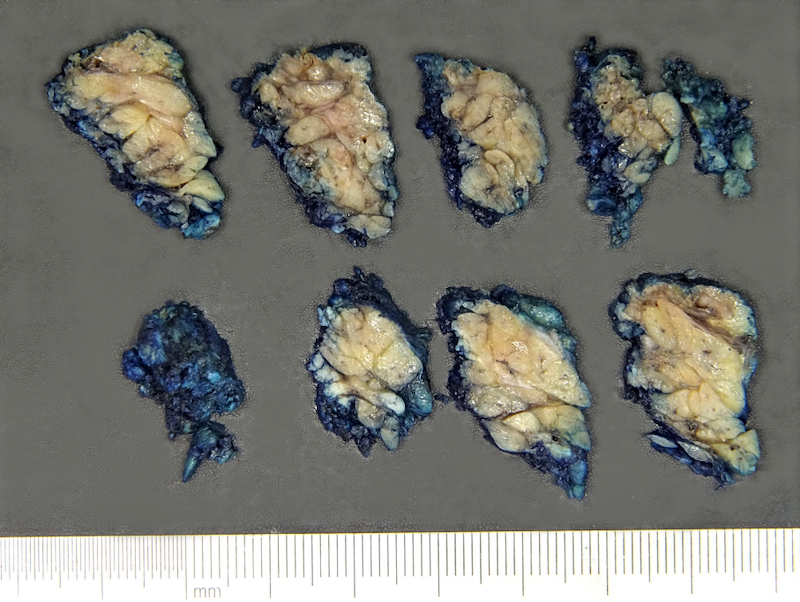
- Extraparenchymal extension is clinical or macroscopic evidence of invasion of soft tissues
- Microscopic evidence alone does not constitute extraparenchymal extension for classification purposes