
14 December 2016 - Case of the Week #410
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Dr. Natalya Shlyakhova, University of California Irvine Medical Center (USA) for contributing this case. To contribute a Case of the Week, follow the guidelines on our main Case of the Week page.
Advertisement
Website news:
(1) Thank you for your support of The Detroit College Promise, the charity we sponsor. At this time of year, we are asking for your help to strengthen public education in Detroit by making a charitable contribution. Last year, the Detroit College Promise merged with the Detroit Public School Foundation to have a greater impact on improving public education in Detroit. This past summer, we awarded 47 students over $25,000 in funds. With your support, we can continue to encourage Detroit students to be the best they can be. To donate, click here.
(2) Need to find a What's New newsletter? Just click on the Newsletter link at the top of the Home Page. All past newsletters are listed, as well as the schedule for future What's New newsletters.
(3) Please bookmark and use our Amazon.com link to remember to help PathologyOutlines.com while doing your Christmas shopping. We receive a commission (~ 5%) from all purchases made through this link, whether pathology related or not, at no cost to you. You get the benefit of wide selection of products and sellers, product reviews, a low price, and the knowledge that you are helping us maintain and expand our free website for the pathology community.
Visit and follow our Blog to see recent updates to the website.
Case of the Week #410
Clinical history:
A 68 year old man with a history of microscopic colitis had gastric thickening on CT scan, leading to esophagogastroduodenoscopy (EGD) with biopsy.
Micro images:
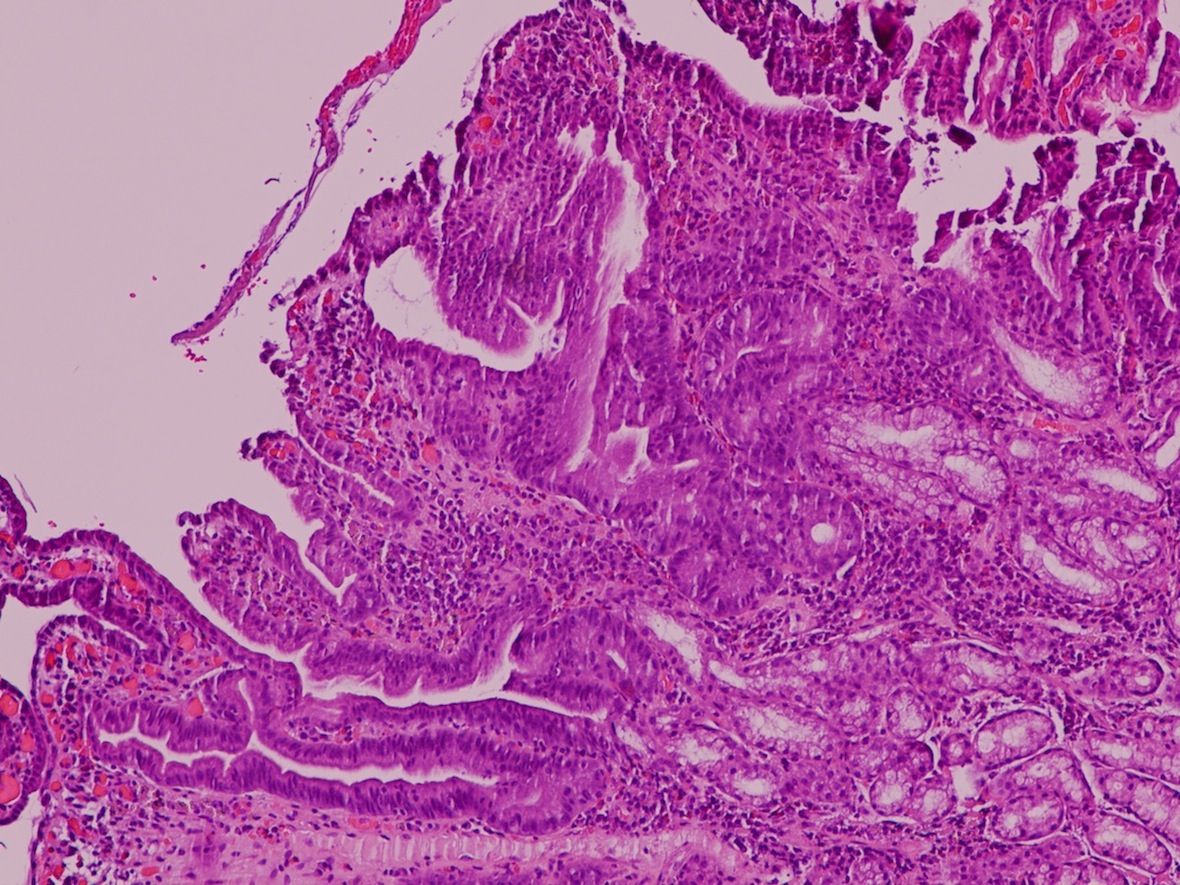

What is your diagnosis?
Diagnosis:
Russell body gastritis
Discussion:
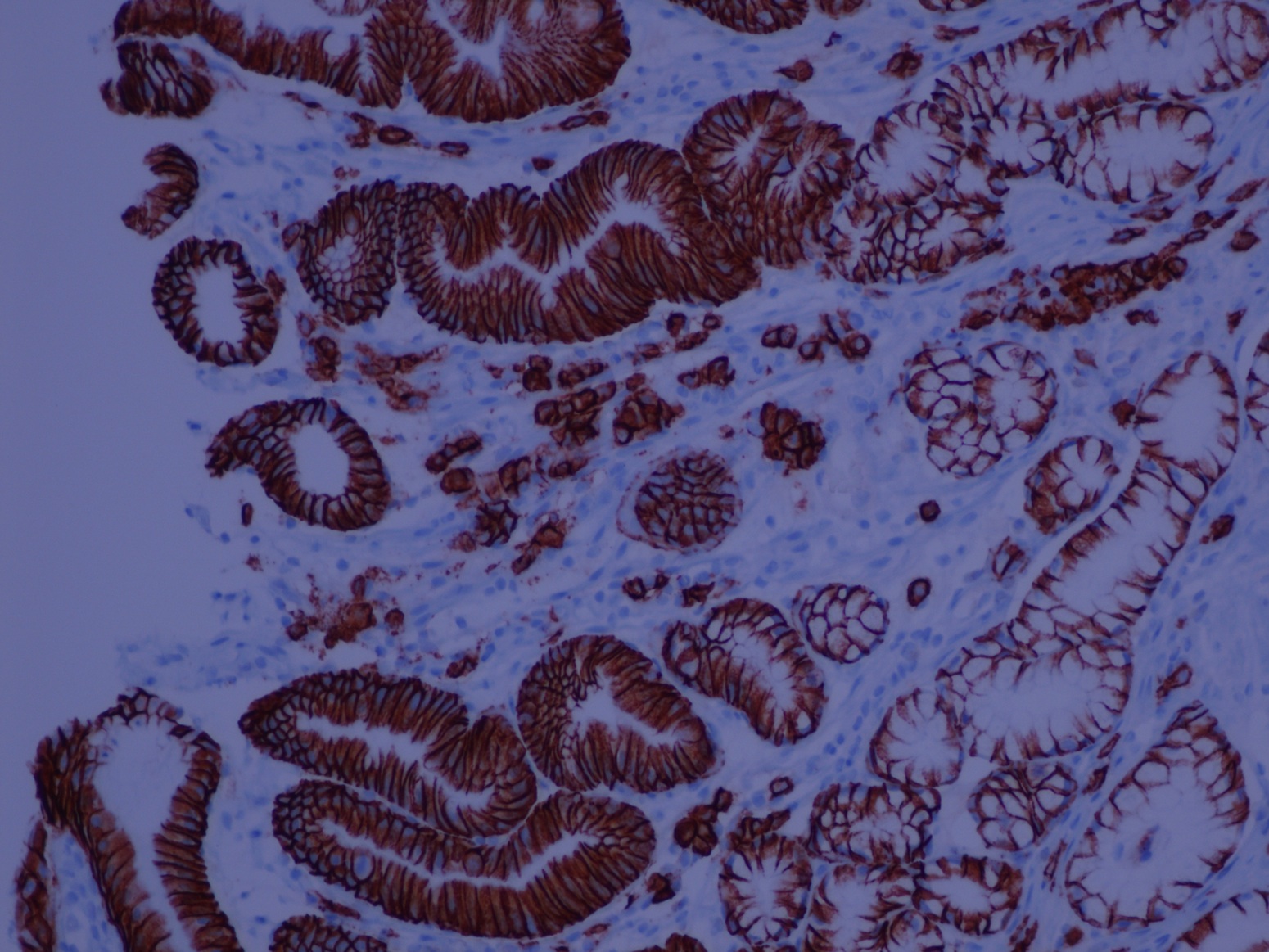
Special stains:
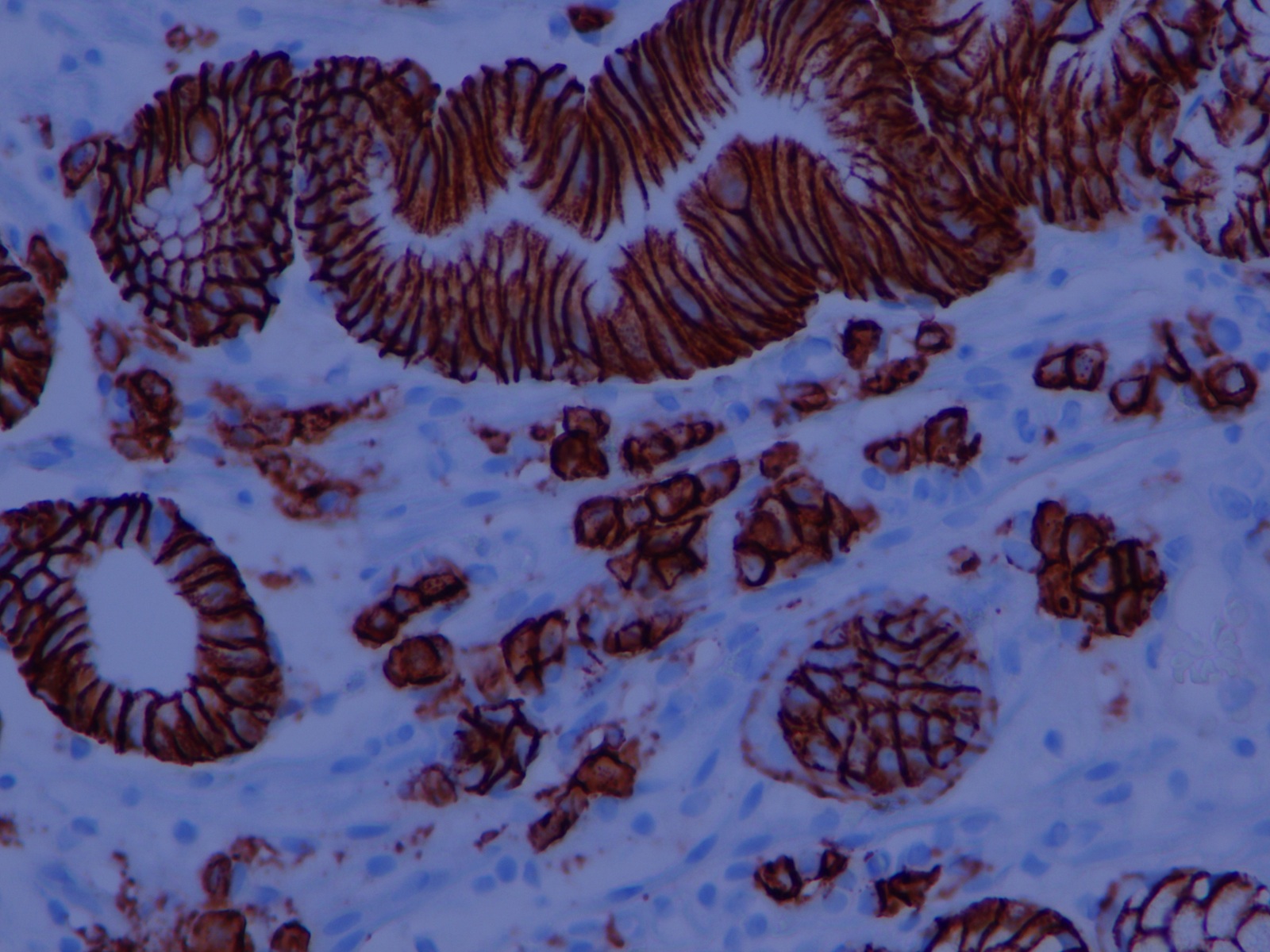
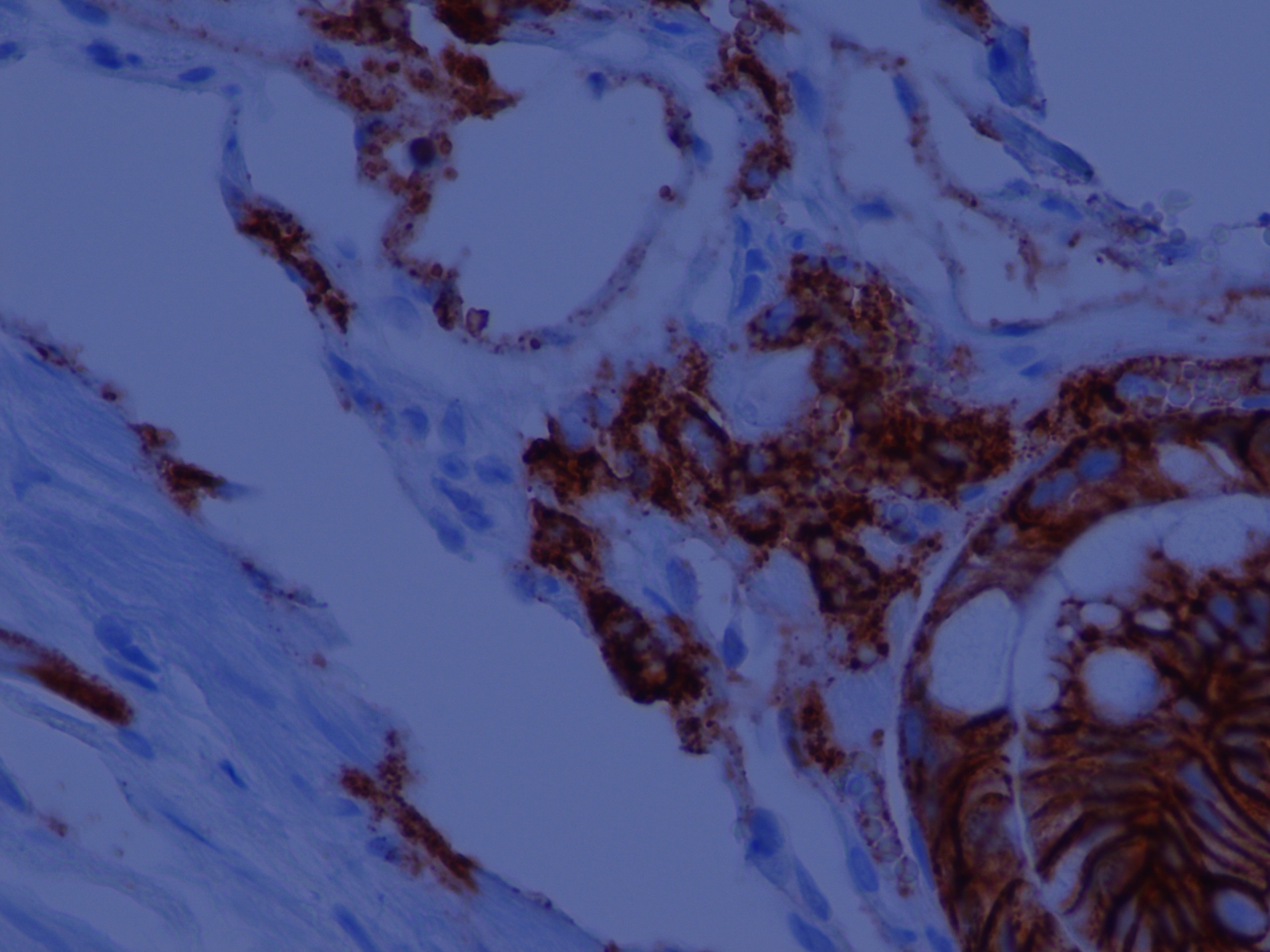
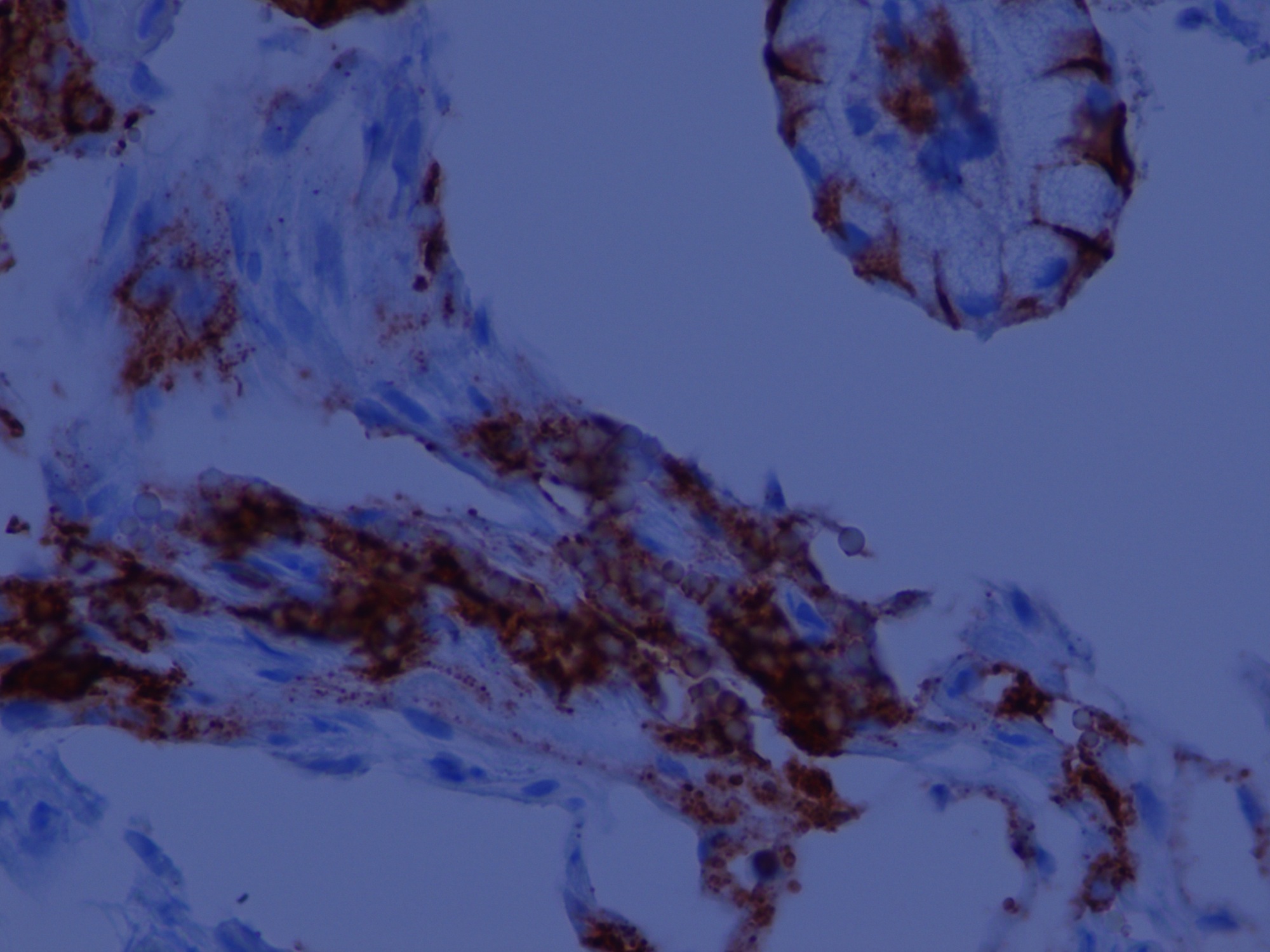
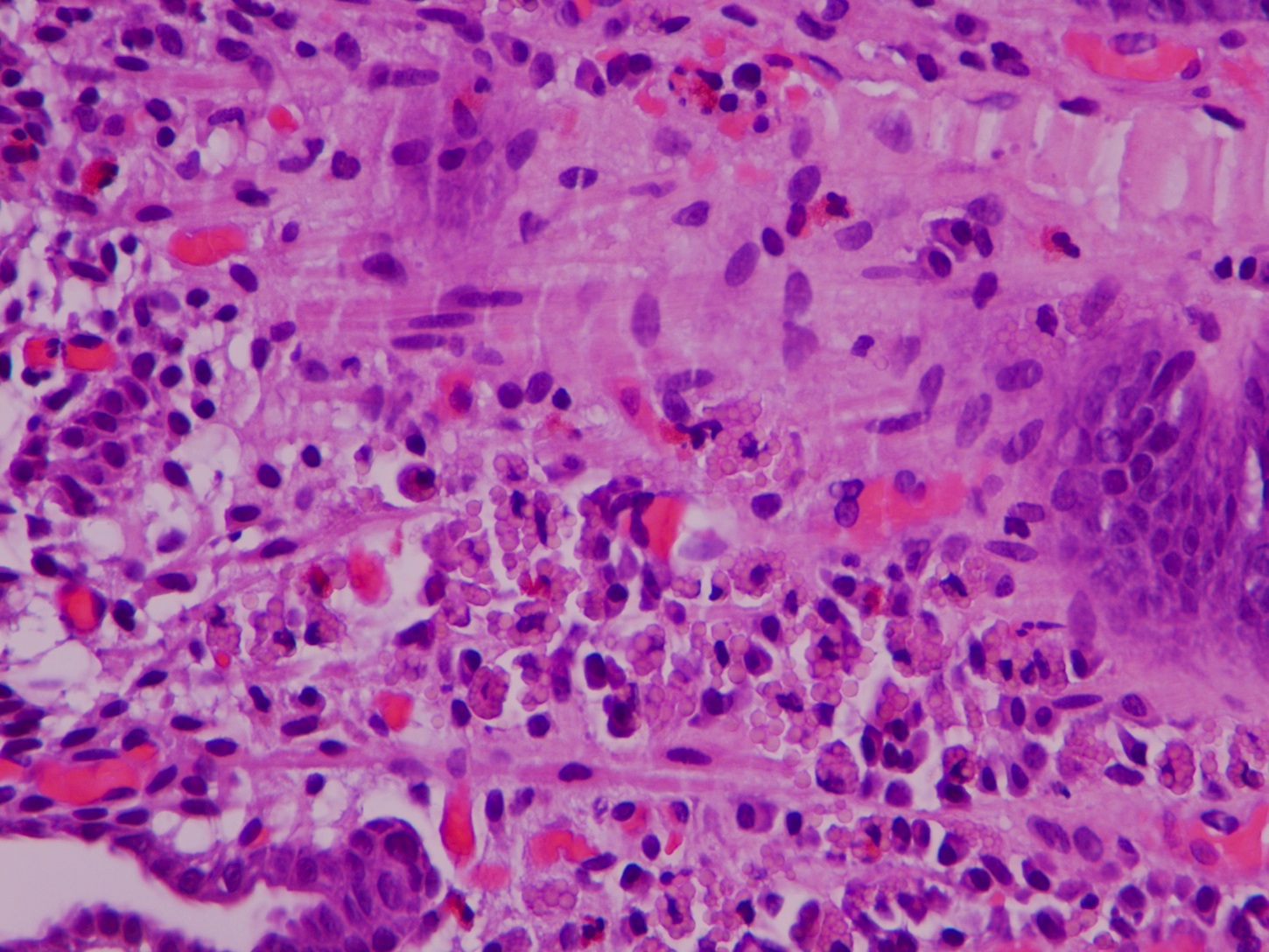
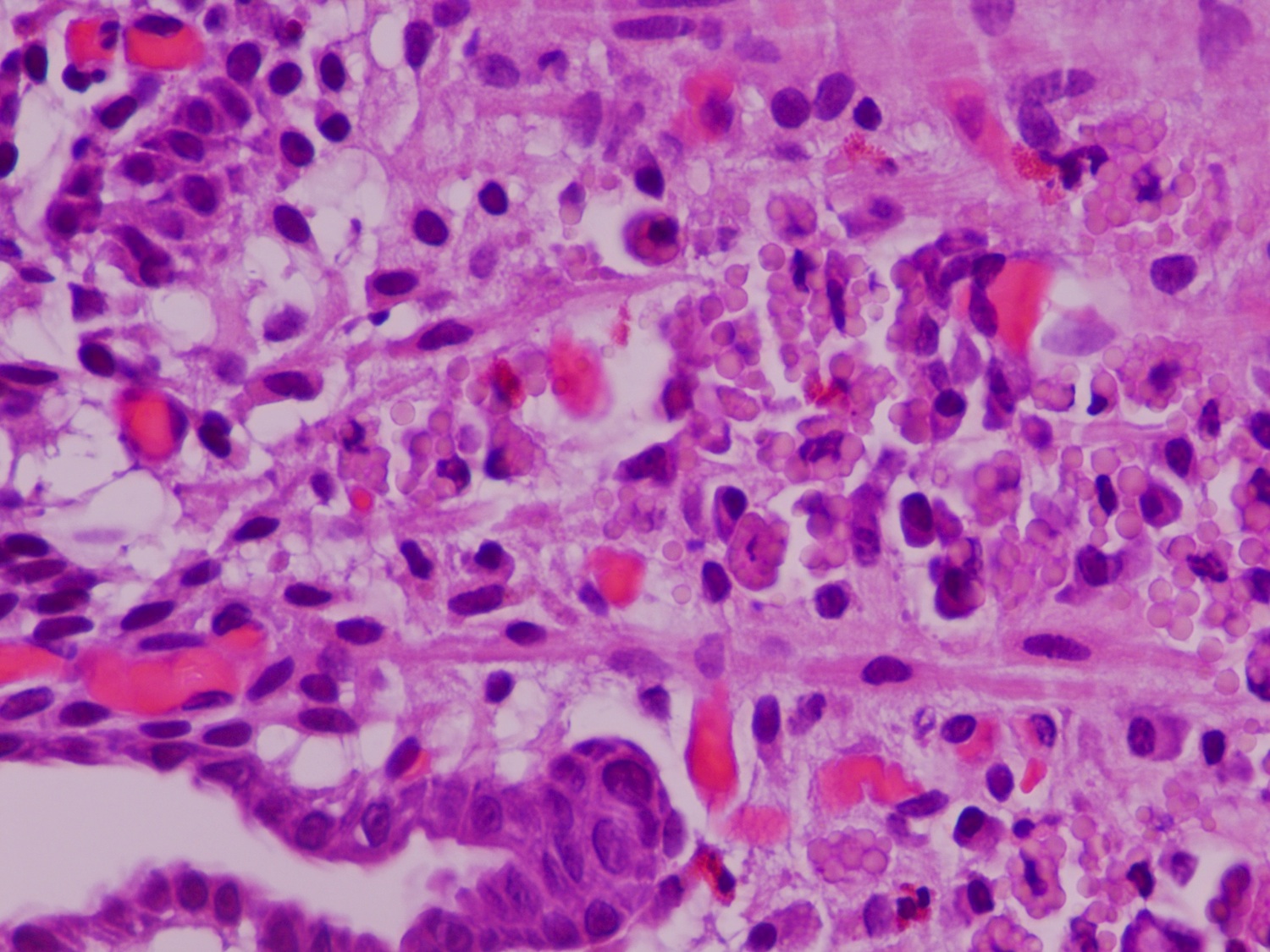
Russell body gastritis (RBG) is a very rare, well circumscribed lesion of plasma cells containing Russell bodies in the mucosa of the stomach. Russell bodies are round, cytoplasmic, eosinophilic globules composed of immunoglobulins, not to be confused with Dutcher bodies, which are intranuclear inclusions in plasma cells (a plasma cell with Russell bodies is called a Mott cell). Russell bodies are thought to arise from excess immunoglobulins due to dysfunctional secretion (Arch Pathol Lab Med 2004;128:915). As seen in this case, extracellular Russell bodies can be present in the stroma (Hum Pathol 2010;41:134).
Patients with RBG generally present with epigastric pain and dyspepsia, which prompts endoscopic evaluation, typically showing a swelling or nodule, but possibly a fungating, ulcerated mass resembling malignancy (BMJ Case Rep 2014 Mar 26;2014, J Gastrointestin Liver Dis 2012;21:97).
Most reported cases are associated with H. pylori infection, and resolve after eradication treatment (BMJ Case Rep 2014 Mar 26;2014, ACG Case Rep J 2016;3:e96). However, upon further evaluation, some patients may have monoclonal gammopathy of undetermined significance (MGUS), which is also associated with H. pylori infection (Arch Pathol Lab Med 2004;128:915), and co-existence with myeloma has been reported (BMJ Case Rep 2014 Mar 26;2014). One reported case with both H. pylori and MGUS showed lamba light chain restriction. Therefore, the clinical significance of RBG - whether reactive / inflammatory or potentially neoplastic - is uncertain (World J Gastrointest Endosc 2015;7:73).
It is important to recognize RBG because it can simulate signet ring cell adenocarcinoma and MALT lymphoma. On low power, the Mott cells may resemble signet rings, but on high power, the cytoplasmic inclusions are eosinophilic, not clear, and the plasma cells in RBG lack nuclear atypia. Staining for PAS may be a pitfall, because Russell bodies stain positive similar to signet ring cells; however, mucin stains are negative in the Mott cells and positive in signet ring cells. In difficult cases, immunohistochemistry can help, as plasma cells are negative for keratins (Montgomery: Biopsy Interpretation of the Gastrointestinal Tract Mucosa: Volume 1: Non-Neoplastic, 2nd ed, 2011).
RBG can be distinguished from MALT lymphoma because it lacks lymphoepithelial lesions, atypia and Dutcher bodies; additionally, almost all RBG cases lack light chain restriction. However, plasma cells with Russell bodies can be seen both in MALT lymphoma and signet ring cell cancers, and have even been reported in a case with both MALT lymphoma and adenocarcinoma (Histopathology 2011;58:1178, Hum Pathol 2010;41:134), so malignancy should be carefully ruled out before rendering a diagnosis of RBG.
Discussion by: Dr. Hillary Z. Kimbrell, Myriad Genetics, Inc., Utah (USA), with special thanks to Dr. John Schmieg, Tulane University, Louisiana (USA)
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Dr. Natalya Shlyakhova, University of California Irvine Medical Center (USA) for contributing this case. To contribute a Case of the Week, follow the guidelines on our main Case of the Week page.
Top Books Listed on PathologyOutlines.com!
Click here to view more Top Books listed on our site.
Website news:
(1) Thank you for your support of The Detroit College Promise, the charity we sponsor. At this time of year, we are asking for your help to strengthen public education in Detroit by making a charitable contribution. Last year, the Detroit College Promise merged with the Detroit Public School Foundation to have a greater impact on improving public education in Detroit. This past summer, we awarded 47 students over $25,000 in funds. With your support, we can continue to encourage Detroit students to be the best they can be. To donate, click here.
(2) Need to find a What's New newsletter? Just click on the Newsletter link at the top of the Home Page. All past newsletters are listed, as well as the schedule for future What's New newsletters.
(3) Please bookmark and use our Amazon.com link to remember to help PathologyOutlines.com while doing your Christmas shopping. We receive a commission (~ 5%) from all purchases made through this link, whether pathology related or not, at no cost to you. You get the benefit of wide selection of products and sellers, product reviews, a low price, and the knowledge that you are helping us maintain and expand our free website for the pathology community.
Visit and follow our Blog to see recent updates to the website.
Case of the Week #410
Clinical history:
A 68 year old man with a history of microscopic colitis had gastric thickening on CT scan, leading to esophagogastroduodenoscopy (EGD) with biopsy.
Micro images:
What is your diagnosis?
Diagnosis:
Russell body gastritis
Discussion:
Special stains:
CD138
Russell body gastritis (RBG) is a very rare, well circumscribed lesion of plasma cells containing Russell bodies in the mucosa of the stomach. Russell bodies are round, cytoplasmic, eosinophilic globules composed of immunoglobulins, not to be confused with Dutcher bodies, which are intranuclear inclusions in plasma cells (a plasma cell with Russell bodies is called a Mott cell). Russell bodies are thought to arise from excess immunoglobulins due to dysfunctional secretion (Arch Pathol Lab Med 2004;128:915). As seen in this case, extracellular Russell bodies can be present in the stroma (Hum Pathol 2010;41:134).
Patients with RBG generally present with epigastric pain and dyspepsia, which prompts endoscopic evaluation, typically showing a swelling or nodule, but possibly a fungating, ulcerated mass resembling malignancy (BMJ Case Rep 2014 Mar 26;2014, J Gastrointestin Liver Dis 2012;21:97).
Most reported cases are associated with H. pylori infection, and resolve after eradication treatment (BMJ Case Rep 2014 Mar 26;2014, ACG Case Rep J 2016;3:e96). However, upon further evaluation, some patients may have monoclonal gammopathy of undetermined significance (MGUS), which is also associated with H. pylori infection (Arch Pathol Lab Med 2004;128:915), and co-existence with myeloma has been reported (BMJ Case Rep 2014 Mar 26;2014). One reported case with both H. pylori and MGUS showed lamba light chain restriction. Therefore, the clinical significance of RBG - whether reactive / inflammatory or potentially neoplastic - is uncertain (World J Gastrointest Endosc 2015;7:73).
It is important to recognize RBG because it can simulate signet ring cell adenocarcinoma and MALT lymphoma. On low power, the Mott cells may resemble signet rings, but on high power, the cytoplasmic inclusions are eosinophilic, not clear, and the plasma cells in RBG lack nuclear atypia. Staining for PAS may be a pitfall, because Russell bodies stain positive similar to signet ring cells; however, mucin stains are negative in the Mott cells and positive in signet ring cells. In difficult cases, immunohistochemistry can help, as plasma cells are negative for keratins (Montgomery: Biopsy Interpretation of the Gastrointestinal Tract Mucosa: Volume 1: Non-Neoplastic, 2nd ed, 2011).
RBG can be distinguished from MALT lymphoma because it lacks lymphoepithelial lesions, atypia and Dutcher bodies; additionally, almost all RBG cases lack light chain restriction. However, plasma cells with Russell bodies can be seen both in MALT lymphoma and signet ring cell cancers, and have even been reported in a case with both MALT lymphoma and adenocarcinoma (Histopathology 2011;58:1178, Hum Pathol 2010;41:134), so malignancy should be carefully ruled out before rendering a diagnosis of RBG.
Discussion by: Dr. Hillary Z. Kimbrell, Myriad Genetics, Inc., Utah (USA), with special thanks to Dr. John Schmieg, Tulane University, Louisiana (USA)
