
6 April 2016 - Case of the Week #384
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Dr. Ankur Sangoi, El Camino Hospital, California (USA) for contributing this case. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto. To contribute a Case of the Week, follow the guidelines on our main Case of the Week page.
Advertisement
Website news:
(1) In March 2016, we had a record high number of visits per day (23,986), a record number of total visits (743,594) and a record number of total pages viewed (274,6187). For more statistics, click here.
(2) In April, we are highlighting these Laboratory Accreditation / Education / CME companies on our Buyer's Guide: ARUP Laboratories, ASCP, BoardVitals, CAP and Educational Symposia. Be sure to visit our Buyer's Guide to learn more helpful information about the products and services offered by these companies for pathologists. You can also access past Feature pages through December 2015.
(3) Our newest Commercial Email Contest Winner is Dr. Kim Lorenzen, from Avera Queen of Peace Hospital in Mitchell, South Dakota. She was sent a $50 Amazon gift card. Please make sure to sign up for and read our Commercial Emails for a chance to win at another contest!
Visit our Blog and Subscribe to our Posts or Follow by Email (click on the box on the right side) to see recent updates to the website.
Case of the Week #384
Clinical history:
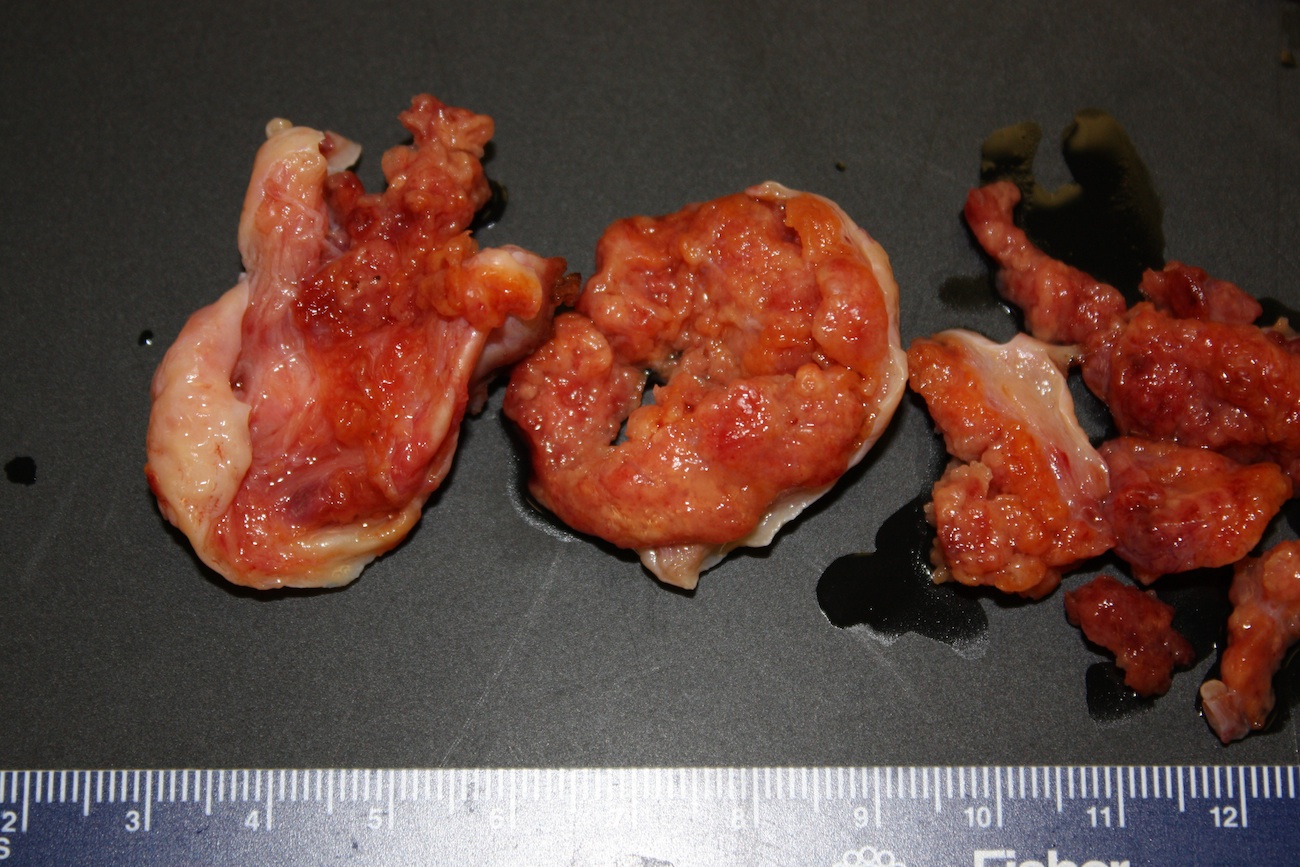
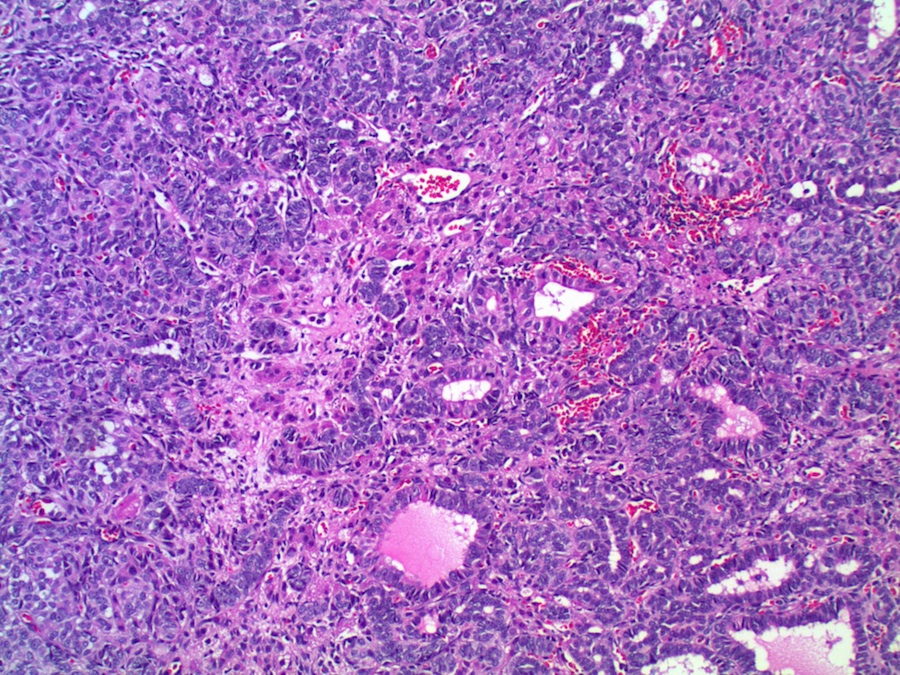
A 16 year old girl presented with hirsutism and an ovarian mass, which was excised.
Gross images:
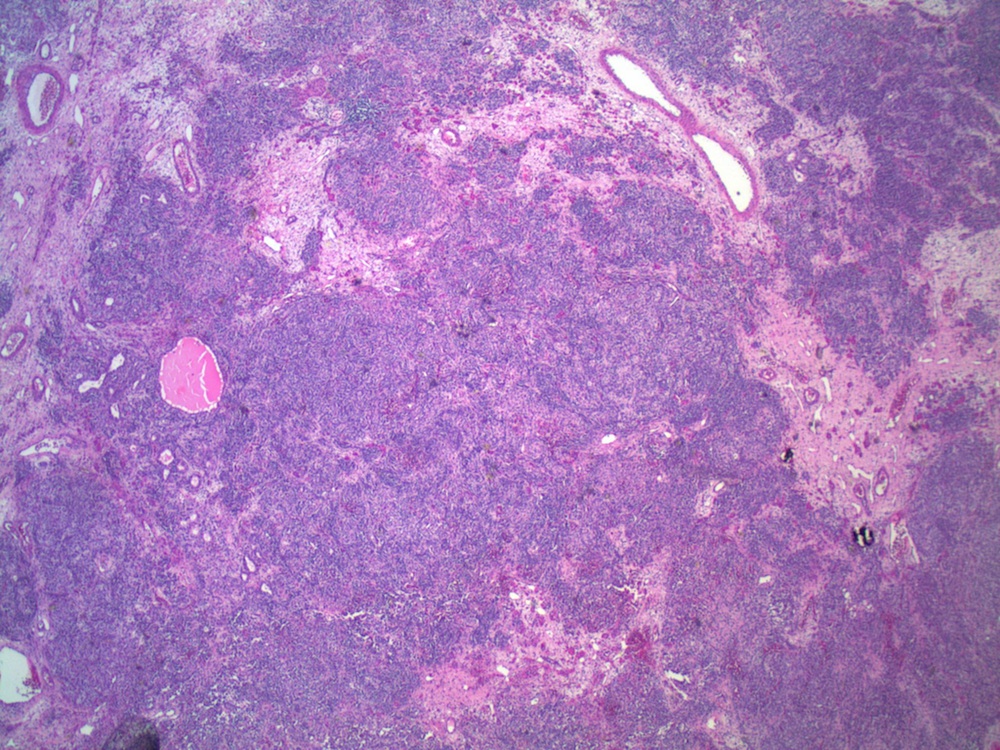
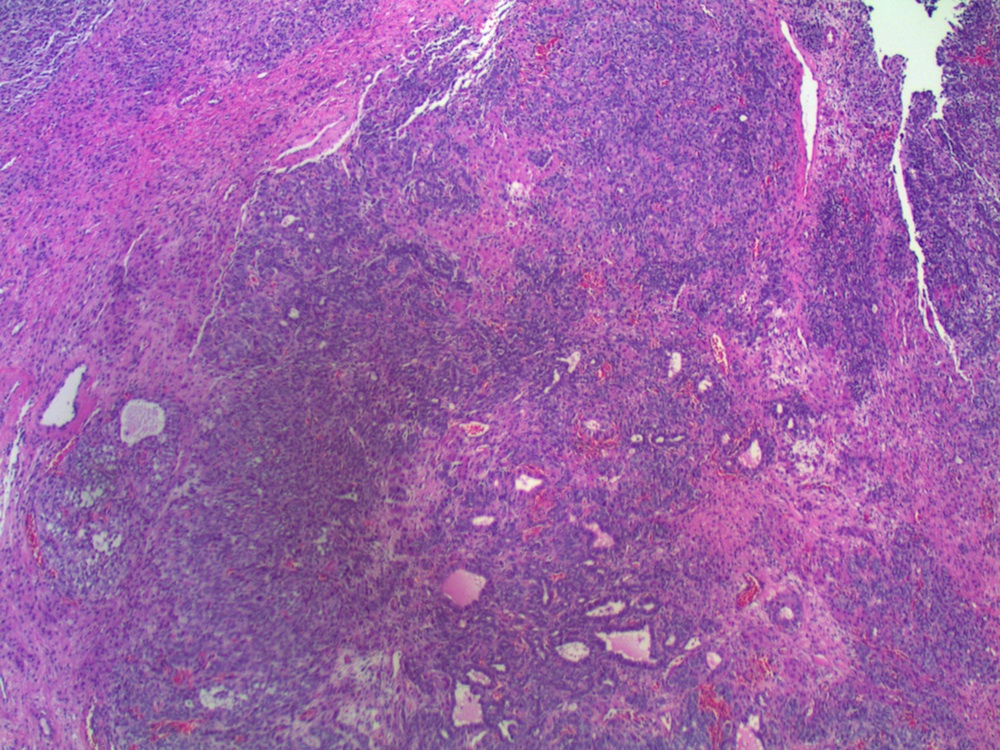
Micro images:

What is your diagnosis?
Diagnosis:
Sertoli-Leydig cell tumor, intermediate grade
Discussion:
Sertoli-Leydig cell tumors (SLCT) of the ovary are uncommon sex-cord stromal tumors. They comprise less than 0.1% of ovarian neoplasms and are usually found in young patients (average 25 years). Most tumors are unilateral and confined to the ovaries (MedGenMed 2007;9:44). These tumors are characterized by testicular structures that produce androgens, and nearly 50% are accompanied by androgen excess (amenorrhea, breast atrophy, loss of subcutaneous fat, deepening of the voice and hirsutism, Rosai and Ackerman's Surgical Pathology, 2011, MedGenMed 2007;9:44).
Grossly, they are predominantly solid, although cystic areas may be present. Microscopically, they are composed of a variable mixture of cells resembling male Sertoli and Leydig cells. Growth patterns, which may coexist in the same tumor, include well differentiated, intermediate, poorly differentiated, pure Sertoli cell, retiform, and containing heterologous elements (Rosai and Ackerman's Surgical Pathology, 2011). Well differentiated tumors are composed of tubules lined by Sertoli-like cells separated by variable numbers of Leydig-like cells. Intermediate grade tumors are characterized by sheets and cords of Sertoli-like cells, separated by spindle stromal cells and recognizable Leydig cells. Poorly differentiated tumors show spindle cells in a sarcomatoid pattern. Pure Sertoli cell tumors are composed entirely of Sertoli cells. Tumors with heterologous elements account for 20% of Sertoli-Leydig cell tumors and contain mesenchymal cells including bone, cartilage or skeletal muscle, or endodermal elements such as cysts or glands (MedGenMed 2007;9:44). Tumors with heterologous mesenchymal elements are usually poorly differentiated, but those with endodermal elements typically are of intermediate differentiation (Arch Gynecol Obstet 2001;264:206). In the retiform variant, tumor cells coexist with formations resembling the rete of the ovary or testis. Bizarre nuclei may be seen in all variants, with no apparent prognostic significance.
The gonadal component strongly expresses inhibin, the areas of Sertoli differentiation stain for keratin and SOX9, and WT1 is usually positive in both components (Rosai and Ackerman's Surgical Pathology, 2011).
The differential diagnosis of Sertoli-Leydig cell tumor with heterologous elements includes carcinosarcoma, and IHC is useful in making this determination (Rosai and Ackerman's Surgical Pathology, 2011).
Prognosis correlates with tumor stage and differentiation (MedGenMed 2007;9:44). The overall incidence of clinical malignancy in one large series was 18%; all well differentiated tumors had benign behavior, but 19% with heterologous elements and 59% of poorly differentiated tumors had malignant behavior (Am J Surg Pathol 1985;9:543). In intermediate or poorly differentiated SLCT, a survival rate of 92% was noted at both 5 and 10 years (Am J Surg Pathol 1984;8:405).
Discussion by Dr. Jennifer R. Kaley, University of Arkansas for Medical Sciences (USA).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Dr. Ankur Sangoi, El Camino Hospital, California (USA) for contributing this case. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto. To contribute a Case of the Week, follow the guidelines on our main Case of the Week page.
Advertisement
Website news:
(1) In March 2016, we had a record high number of visits per day (23,986), a record number of total visits (743,594) and a record number of total pages viewed (274,6187). For more statistics, click here.
(2) In April, we are highlighting these Laboratory Accreditation / Education / CME companies on our Buyer's Guide: ARUP Laboratories, ASCP, BoardVitals, CAP and Educational Symposia. Be sure to visit our Buyer's Guide to learn more helpful information about the products and services offered by these companies for pathologists. You can also access past Feature pages through December 2015.
(3) Our newest Commercial Email Contest Winner is Dr. Kim Lorenzen, from Avera Queen of Peace Hospital in Mitchell, South Dakota. She was sent a $50 Amazon gift card. Please make sure to sign up for and read our Commercial Emails for a chance to win at another contest!
Visit our Blog and Subscribe to our Posts or Follow by Email (click on the box on the right side) to see recent updates to the website.
Case of the Week #384
Clinical history:
A 16 year old girl presented with hirsutism and an ovarian mass, which was excised.
Gross images:
Micro images:
What is your diagnosis?
Diagnosis:
Sertoli-Leydig cell tumor, intermediate grade
Discussion:
Sertoli-Leydig cell tumors (SLCT) of the ovary are uncommon sex-cord stromal tumors. They comprise less than 0.1% of ovarian neoplasms and are usually found in young patients (average 25 years). Most tumors are unilateral and confined to the ovaries (MedGenMed 2007;9:44). These tumors are characterized by testicular structures that produce androgens, and nearly 50% are accompanied by androgen excess (amenorrhea, breast atrophy, loss of subcutaneous fat, deepening of the voice and hirsutism, Rosai and Ackerman's Surgical Pathology, 2011, MedGenMed 2007;9:44).
Grossly, they are predominantly solid, although cystic areas may be present. Microscopically, they are composed of a variable mixture of cells resembling male Sertoli and Leydig cells. Growth patterns, which may coexist in the same tumor, include well differentiated, intermediate, poorly differentiated, pure Sertoli cell, retiform, and containing heterologous elements (Rosai and Ackerman's Surgical Pathology, 2011). Well differentiated tumors are composed of tubules lined by Sertoli-like cells separated by variable numbers of Leydig-like cells. Intermediate grade tumors are characterized by sheets and cords of Sertoli-like cells, separated by spindle stromal cells and recognizable Leydig cells. Poorly differentiated tumors show spindle cells in a sarcomatoid pattern. Pure Sertoli cell tumors are composed entirely of Sertoli cells. Tumors with heterologous elements account for 20% of Sertoli-Leydig cell tumors and contain mesenchymal cells including bone, cartilage or skeletal muscle, or endodermal elements such as cysts or glands (MedGenMed 2007;9:44). Tumors with heterologous mesenchymal elements are usually poorly differentiated, but those with endodermal elements typically are of intermediate differentiation (Arch Gynecol Obstet 2001;264:206). In the retiform variant, tumor cells coexist with formations resembling the rete of the ovary or testis. Bizarre nuclei may be seen in all variants, with no apparent prognostic significance.
The gonadal component strongly expresses inhibin, the areas of Sertoli differentiation stain for keratin and SOX9, and WT1 is usually positive in both components (Rosai and Ackerman's Surgical Pathology, 2011).
The differential diagnosis of Sertoli-Leydig cell tumor with heterologous elements includes carcinosarcoma, and IHC is useful in making this determination (Rosai and Ackerman's Surgical Pathology, 2011).
Prognosis correlates with tumor stage and differentiation (MedGenMed 2007;9:44). The overall incidence of clinical malignancy in one large series was 18%; all well differentiated tumors had benign behavior, but 19% with heterologous elements and 59% of poorly differentiated tumors had malignant behavior (Am J Surg Pathol 1985;9:543). In intermediate or poorly differentiated SLCT, a survival rate of 92% was noted at both 5 and 10 years (Am J Surg Pathol 1984;8:405).
Discussion by Dr. Jennifer R. Kaley, University of Arkansas for Medical Sciences (USA).
