
9 March 2016 - Case of the Week #381
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Dr. Nikhil Sangle, London Health Sciences Centre (LHSC) and St. Joseph's Health Care (Canada) for contributing this case and discussion. To contribute a Case of the Week, follow the guidelines on our main Case of the Week page.
Advertisement
Website news:
(1) On 1 March 2016, we had our second highest traffic day with 29,919 visits. Thanks for your support and suggestions.
We are nearing completion of our new Books pages, with about ~1300 pathology related books, sorted by publisher, specialty and date posted. You can also search by author and words in the title. The books have all been converted to the new format, but we are verifying that we haven't missed any books, and that the system is operating properly. The new books pages should be available by the USCAP '16 meeting in mid March.
(2) Our newest Commercial Email contest winner is Dr. Matt Kubica, a resident at Western University in Ontario, Canada. He was sent a $50 Amazon gift card. Please make sure to sign up for and read our Commercial Emails for a chance to win at another contest.
(3) Visit our Blog and Subscribe to our Posts or Follow by Email (click on the box on the right side) to see recent updates to the website.
Case of the Week #381
Clinical history:
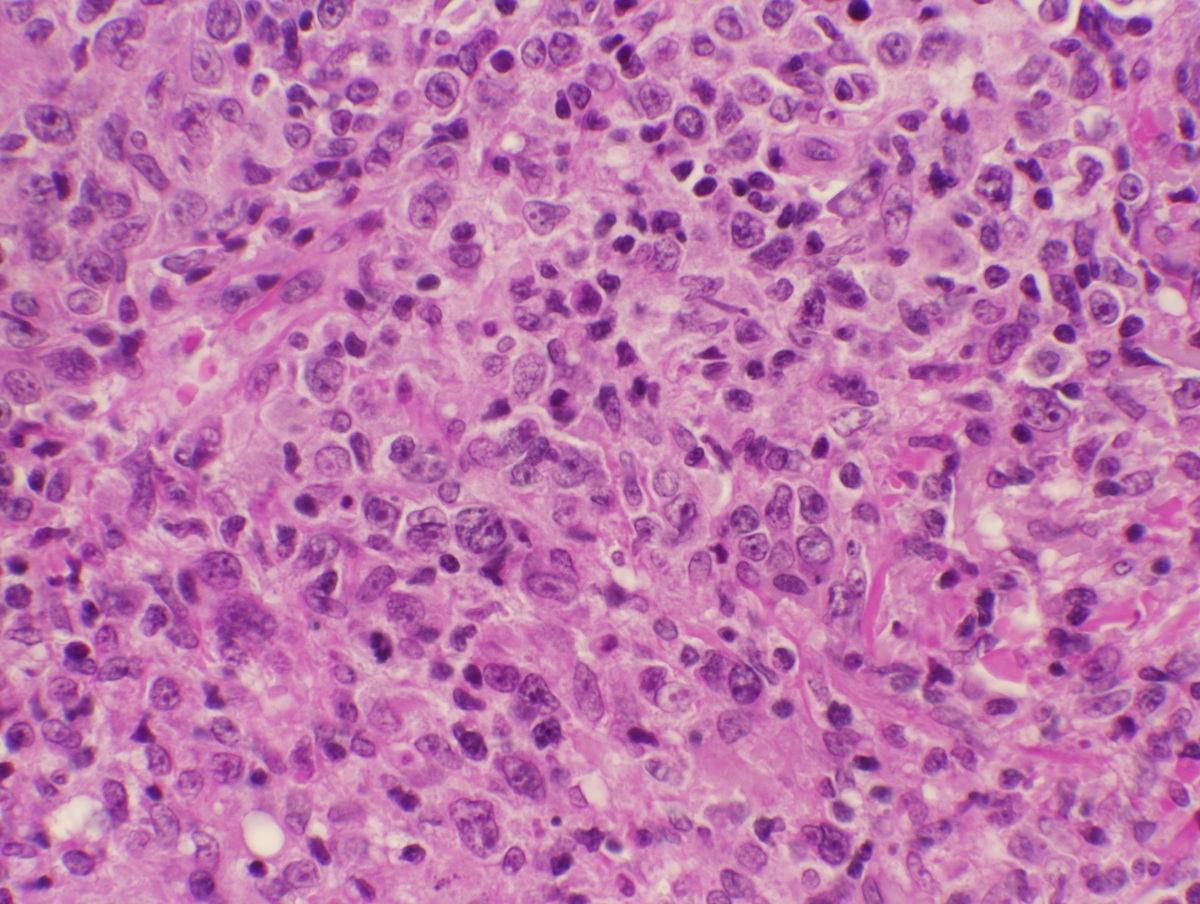
A 57 year old woman presented with rapidly growing lesions on her face and forehead. She had a lifelong history of rheumatoid arthritis and had been taking methotrexate for many years. She denies sweats, chills, appetite change or shortness of breath. A 1.5 cm skin nodule was biopsied.
Micro images:



What is your diagnosis?
Diagnosis:
Iatrogenic immunodeficiency associated B cell lymphoproliferative disorder (IALPD)
Discussion:
Immunostains were obtained:

Iatrogenic immunodeficiency associated B cell lymphoproliferative disorders (IALPDs) are a subset of immunodeficiency associated lymphoproliferative disorders occurring in patients receiving immunosuppressive therapy, particularly methotrexate (MTX) or anti-TNF (tumor necrosis factor) agents for autoimmune diseases such as rheumatoid arthritis or inflammatory bowel disease (Am J Hematol 2010;85:627). An association between methotrexate use and LPDs has been reported in patients treated for rheumatoid arthritis, dermatomyositis and less commonly psoriasis. In patients with rheumatoid arthritis (RA), some uncertainty has been described as to whether the LPD is due to the hyperimmune state in RA or to the immunosuppressive state induced by MTX administration (Am J Med 1985;78:15). Regression of LPD after withdrawal of MTX is considered strong evidence for the carcinogenic potential of MTX (J Clin Oncol 1996;14:1943). On the other hand, patients with RA develop LPD at a rate 2.0 to 5.5 times higher than the general population, with or without MTX treatment. While the etiology of increased incidence of LPD in the setting of autoimmune diseases may be uncertain, there does appear to be an association between therapies for these conditions and the development of LPDs (J Clin Oncol 1996;14:1943, N Engl J Med 1993;328:1317, J Rheumatol 1991;18:1741, Blood 2002;99:3909).
Methotrexate associated LPDs can present with a heterogeneous group of disoders similar to post transplant lymphoproliferative disorders (PTLDs), ranging from reactive polyclonal hyperplasia to aggressive non Hodgkin lymphoma (Annu Rev Med 2005;56:29). Most PTLDs and IALPDs are of B cell origin. While 90% of PTLDs are associated with the Epstein Barr virus (EBV), only 40% of IALPDs are EBV associated.
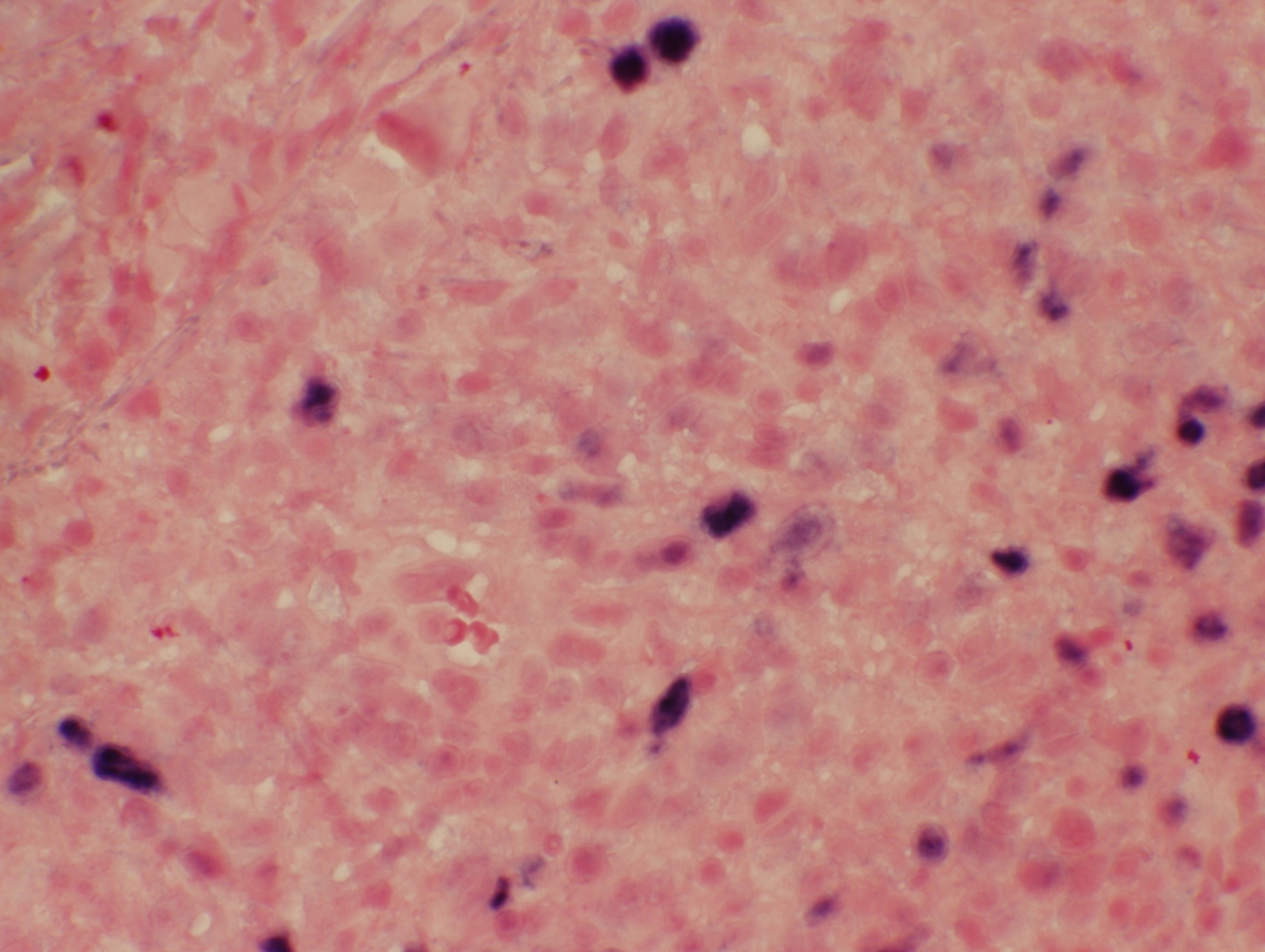
Histologic examination shows morphologic and immunophenotypic characteristics of the type of lymphoma encountered. In this case, there is a dense lymphoid infiltrate of large atypical lymphoid cells that are immunoreactive for CD20, CD30, PAX5 and EBER, but CD15, CD45 and EMA are negative. These morphologic and immunophenotypic features, together with the patient history of methotrexate therapy, are consistent with EBV+ iatrogenic immunodeficiency associated B cell lymphoproliferative disorder (IALPD).
Prognosis and treatment vary based on the type of lymphoproliferative disorder. Several reports have described complete remission following withdrawal of the immunosuppressive agent.
Additional References: J Clin Oncol 1996;14:1943, Arthritis Rheum 2007;56:1433, J Rheumatol 2007;34:322, Arch Dermatol 1997;133:867, Rev Rhum Engl Ed 1998;65:267
Discussion edited by Dr. Jennifer R. Kaley, University of Arkansas for Medical Sciences (USA).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Dr. Nikhil Sangle, London Health Sciences Centre (LHSC) and St. Joseph's Health Care (Canada) for contributing this case and discussion. To contribute a Case of the Week, follow the guidelines on our main Case of the Week page.
New Books Listed on PathologyOutlines.com


- Circulating Tumor Cells (2016, 1st ed) by Richard Cote and Ram Datar, 333 pages, $209 list (Springer)
- Diagnostic Pathology: Head and Neck (2016, 2nd ed) by Lester Thompson and Bruce Wenig, 1192 pages, $295 list (Elsevier)
To view more books recently listed on our site, visit our New Books page.
Website news:
(1) On 1 March 2016, we had our second highest traffic day with 29,919 visits. Thanks for your support and suggestions.
We are nearing completion of our new Books pages, with about ~1300 pathology related books, sorted by publisher, specialty and date posted. You can also search by author and words in the title. The books have all been converted to the new format, but we are verifying that we haven't missed any books, and that the system is operating properly. The new books pages should be available by the USCAP '16 meeting in mid March.
(2) Our newest Commercial Email contest winner is Dr. Matt Kubica, a resident at Western University in Ontario, Canada. He was sent a $50 Amazon gift card. Please make sure to sign up for and read our Commercial Emails for a chance to win at another contest.
(3) Visit our Blog and Subscribe to our Posts or Follow by Email (click on the box on the right side) to see recent updates to the website.
Case of the Week #381
Clinical history:
A 57 year old woman presented with rapidly growing lesions on her face and forehead. She had a lifelong history of rheumatoid arthritis and had been taking methotrexate for many years. She denies sweats, chills, appetite change or shortness of breath. A 1.5 cm skin nodule was biopsied.
Micro images:
What is your diagnosis?
Diagnosis:
Iatrogenic immunodeficiency associated B cell lymphoproliferative disorder (IALPD)
Discussion:
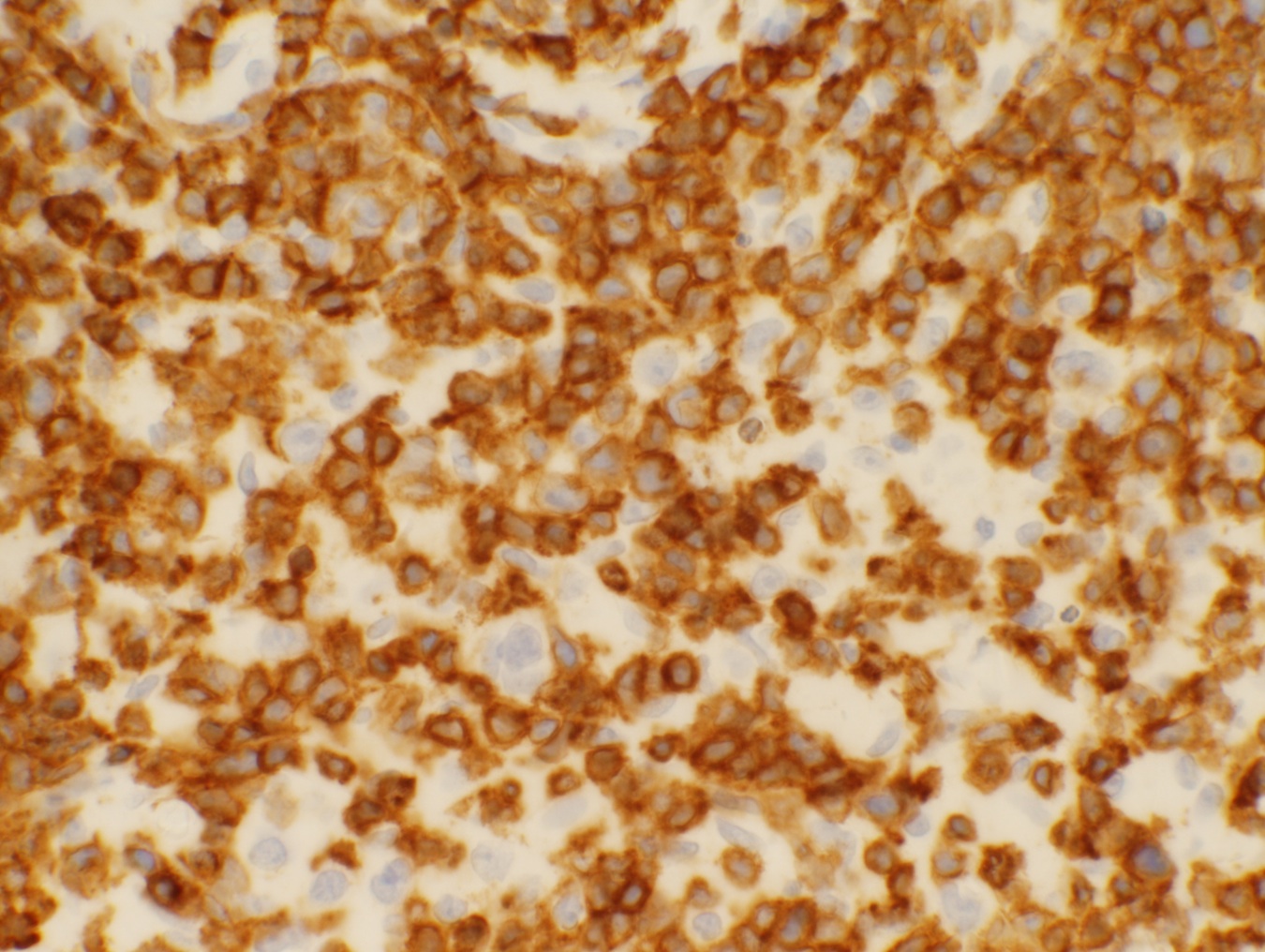
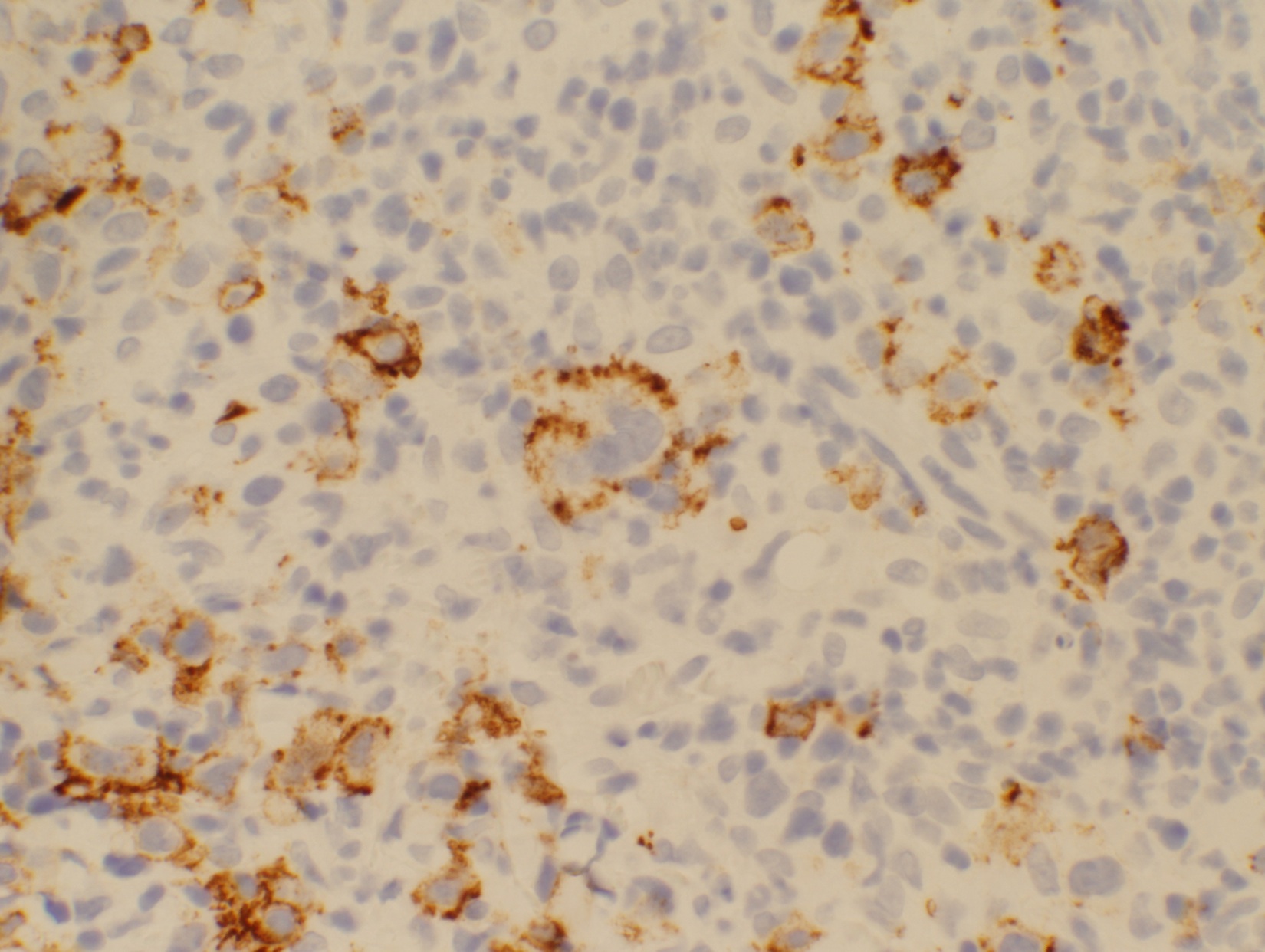
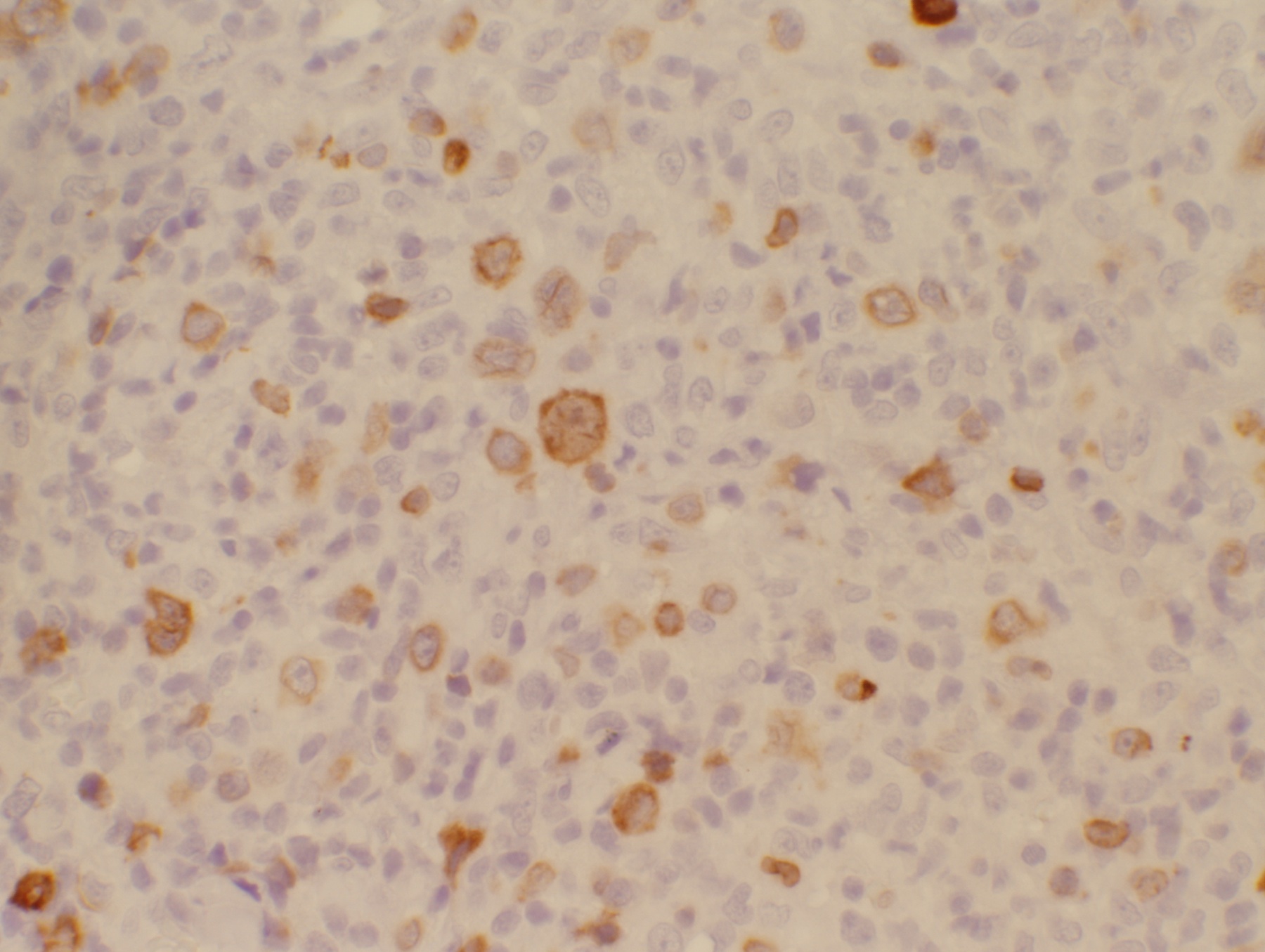
Immunostains were obtained:
CD3
CD20
CD30
CD79a
EBV-EBER
Iatrogenic immunodeficiency associated B cell lymphoproliferative disorders (IALPDs) are a subset of immunodeficiency associated lymphoproliferative disorders occurring in patients receiving immunosuppressive therapy, particularly methotrexate (MTX) or anti-TNF (tumor necrosis factor) agents for autoimmune diseases such as rheumatoid arthritis or inflammatory bowel disease (Am J Hematol 2010;85:627). An association between methotrexate use and LPDs has been reported in patients treated for rheumatoid arthritis, dermatomyositis and less commonly psoriasis. In patients with rheumatoid arthritis (RA), some uncertainty has been described as to whether the LPD is due to the hyperimmune state in RA or to the immunosuppressive state induced by MTX administration (Am J Med 1985;78:15). Regression of LPD after withdrawal of MTX is considered strong evidence for the carcinogenic potential of MTX (J Clin Oncol 1996;14:1943). On the other hand, patients with RA develop LPD at a rate 2.0 to 5.5 times higher than the general population, with or without MTX treatment. While the etiology of increased incidence of LPD in the setting of autoimmune diseases may be uncertain, there does appear to be an association between therapies for these conditions and the development of LPDs (J Clin Oncol 1996;14:1943, N Engl J Med 1993;328:1317, J Rheumatol 1991;18:1741, Blood 2002;99:3909).
Methotrexate associated LPDs can present with a heterogeneous group of disoders similar to post transplant lymphoproliferative disorders (PTLDs), ranging from reactive polyclonal hyperplasia to aggressive non Hodgkin lymphoma (Annu Rev Med 2005;56:29). Most PTLDs and IALPDs are of B cell origin. While 90% of PTLDs are associated with the Epstein Barr virus (EBV), only 40% of IALPDs are EBV associated.
Histologic examination shows morphologic and immunophenotypic characteristics of the type of lymphoma encountered. In this case, there is a dense lymphoid infiltrate of large atypical lymphoid cells that are immunoreactive for CD20, CD30, PAX5 and EBER, but CD15, CD45 and EMA are negative. These morphologic and immunophenotypic features, together with the patient history of methotrexate therapy, are consistent with EBV+ iatrogenic immunodeficiency associated B cell lymphoproliferative disorder (IALPD).
Prognosis and treatment vary based on the type of lymphoproliferative disorder. Several reports have described complete remission following withdrawal of the immunosuppressive agent.
Additional References: J Clin Oncol 1996;14:1943, Arthritis Rheum 2007;56:1433, J Rheumatol 2007;34:322, Arch Dermatol 1997;133:867, Rev Rhum Engl Ed 1998;65:267
Discussion edited by Dr. Jennifer R. Kaley, University of Arkansas for Medical Sciences (USA).
