
17 February 2016 - Case of the Week #379
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Dr. Julie Guilmette, Dr. Mathieu Latour and Dr. Roula Albadine, University of Montreal Hospital Center (Canada) for contributing this case and discussion. To contribute a Case of the Week, follow the guidelines on our main Case of the Week page.
Advertisement
Website news:
(1) We are excited to see that traffic keeps going up to our website. This past January we had an all time high number of visits of 11,058 to the Conferences page and 8,856 visits to the Fellowship pages. Take advantage of this, and advertise your Conference or Fellowship with us! Remember, it is never too early to post a Conference advertisement because updates are free and the advertisement will run until the date of the conference. For more information, please visit our Conferences page or Fellowships page.
(2) Calling all fans of PathologyOutlines.com: we invite you to help support our website by becoming a Member. You get a great T-shirt and other gifts, all your friends will see your name at our booth at USCAP and CAP (unless you want to be anonymous), and you will also be listed as a member on our blog and in our emails. Most importantly, you will know you are a part of making our website better. For information on institutional membership, click here. Please email us with any questions at CommentsPathout@gmail.com.
(3) Our newest Commercial Email contest winner is Dr. Indranil Chakrabarti, North Bengal Medical College. He was sent a $50 Amazon.com gift card. Click here to sign up for our Commercial Emails for a chance to win at another contest!
Visit our Blog and Subscribe to our Posts or Follow by Email (click on the box on the right side) to see recent updates to the website.
Case of the Week #379
Clinical history:
A 52 year old woman with nonalcoholic steatohepatitis was found to have a right kidney mass. Imaging studies showed a 2.5 cm, non-infiltrative exophytic mass. She underwent partial nephrectomy.
Gross description:
Gross examination revealed a partial kidney with adherent adipose tissue weighing 20 g and measuring 4.0 cm x 3.0 cm x 2.5 cm. Sectioning revealed a protruding, subcortical and well circumscribed tan mass with small hemorrhagic foci measuring 1.9 x 1.8 x 1.5 cm. There was no central scar and no foci of necrosis.
Micro images:

What is your diagnosis?
Diagnosis:
Hybrid oncocytic - chromophobe tumor
Discussion:
Immunostains were obtained:
Histopathology shows a non-infiltrative, well circumscribed intrarenal tumor composed of neoplastic cells arranged in a solid, alveolar and cystic pattern. There is a dual population of eosinophilic cells. The oncocytic cells are medium sized, round and contain granular eosinophilic cytoplasm with a round concentric nucleus and a prominent nucleolus. The chromophobe cells are large and plant-like with a distinct cell membrane and flaky eosinophilic cytoplasm. A diagnostic clue is the presence of a perinuclear halo surrounding a wrinkled raisinoid nucleus. Focally, a third population of eosinophilic cells featuring both oncocytic and chromophobe morphology are seen. Mitoses are rare.
The neoplastic cells are positive for CD117, E-cadherin and focally for CK7. Hales colloidal iron stain shows both a cytoplasmic and luminal pattern.
Hybrid oncocytic-chromophobe tumor (HOCT) is rare renal neoplasm classified as a subcategory of chromophobe renal cell carcinoma (Am J Surg Pathol 2013;37:1469). HOCT can occur in three distinct clinical settings: sporadically, associated with renal oncocytomatosis and as a component of the Birt-Hogg-Dubé syndrome (Histol Histopathol 2013;28:1257). Birt-Hogg-Dubé syndrome is an autosomal dominant inherited disorder associated with a genetic abnormality on chromosome 17p11.2 leading to a mutation in the BHD gene. Clinical manifestations include spontaneous pneumothorax, multiple benign cutaneous follicular tumors (fibrofolliculoma, trichodiscoma and acrochordon), oncocytomatosis and multifocal chromophobe renal cell tumors (Pol J Pathol 2014;65:93).
HOCT is a distinct tumor with overlapping features of oncocytoma and chromophobe renal cell tumors (ChRCC), showing histopathologic and immunophenotypic features of each. Oncocytoma is negative for CK7 and shows a luminal pattern with Hales colloidal iron, and ChRCC is diffusely positive for CK7 and shows a cytoplasmic pattern with Hales colloidal iron; HOCT expresses a mixed immunophenotypic pattern (J Clin Pathol 2014;67:97).
The histopathologic differential diagnosis includes other eosinophilic renal cell neoplasms including oncocytic papillary renal cell carcinoma and eosinophilic clear cell renal cell carcinoma. Oncocytic papillary renal cell carcinoma has a papillary architecture, is negative for CD117, and is associated with a worse prognosis (Arch Pathol Lab Med 2014;138:1531). Eosinophilic clear cell renal cell carcinoma is composed of sheets of neoplastic cells separated by thin fibrous septa and containing a prominent vascular network. It expresses CD10, is negative for CD117 and is also associated with a worse prognosis (Arch Pathol Lab Med 2014;138:1531).
HOCT has a good prognosis and indolent behavior (Virchows Arch 2010;456:355). Its rarity and histologic subjectivity make it a diagnostic challenge for general pathologists. If tumors are multiple, this may be a clue to a diagnosis of BHD syndrome. Communication with the clinician in this case is essential to ensure appropriate clinical investigation and follow-up.
Discussion edited by Dr. Jennifer R. Kaley, University of Arkansas for Medical Sciences (USA).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Dr. Julie Guilmette, Dr. Mathieu Latour and Dr. Roula Albadine, University of Montreal Hospital Center (Canada) for contributing this case and discussion. To contribute a Case of the Week, follow the guidelines on our main Case of the Week page.
New Books Listed on PathologyOutlines.com!


- Stocker and Dehner's Pediatric Pathology (2015, 4th ed) by Aliya Husain, J. Thomas Stocker and Louis Dehner, 1480 pages, $381 list (LWW)
- Neoplastic Mimics in Soft Tissue and Bone Pathology (2015, 1st ed) by Vickie Y. Jo and Jason L. Hornick, 192 pages, $150 list (Spr.)
To view more books recently listed on our site, visit our New Books page.
Website news:
(1) We are excited to see that traffic keeps going up to our website. This past January we had an all time high number of visits of 11,058 to the Conferences page and 8,856 visits to the Fellowship pages. Take advantage of this, and advertise your Conference or Fellowship with us! Remember, it is never too early to post a Conference advertisement because updates are free and the advertisement will run until the date of the conference. For more information, please visit our Conferences page or Fellowships page.
(2) Calling all fans of PathologyOutlines.com: we invite you to help support our website by becoming a Member. You get a great T-shirt and other gifts, all your friends will see your name at our booth at USCAP and CAP (unless you want to be anonymous), and you will also be listed as a member on our blog and in our emails. Most importantly, you will know you are a part of making our website better. For information on institutional membership, click here. Please email us with any questions at CommentsPathout@gmail.com.
(3) Our newest Commercial Email contest winner is Dr. Indranil Chakrabarti, North Bengal Medical College. He was sent a $50 Amazon.com gift card. Click here to sign up for our Commercial Emails for a chance to win at another contest!
Visit our Blog and Subscribe to our Posts or Follow by Email (click on the box on the right side) to see recent updates to the website.
Case of the Week #379
Clinical history:
A 52 year old woman with nonalcoholic steatohepatitis was found to have a right kidney mass. Imaging studies showed a 2.5 cm, non-infiltrative exophytic mass. She underwent partial nephrectomy.
Gross description:
Gross examination revealed a partial kidney with adherent adipose tissue weighing 20 g and measuring 4.0 cm x 3.0 cm x 2.5 cm. Sectioning revealed a protruding, subcortical and well circumscribed tan mass with small hemorrhagic foci measuring 1.9 x 1.8 x 1.5 cm. There was no central scar and no foci of necrosis.
Micro images:
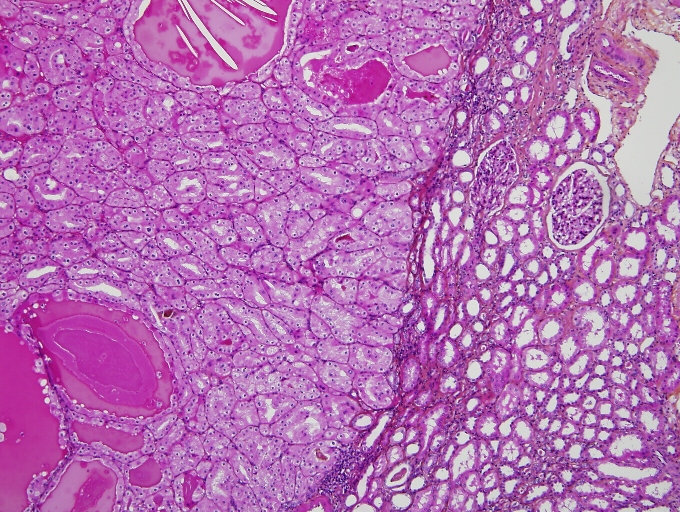
10x
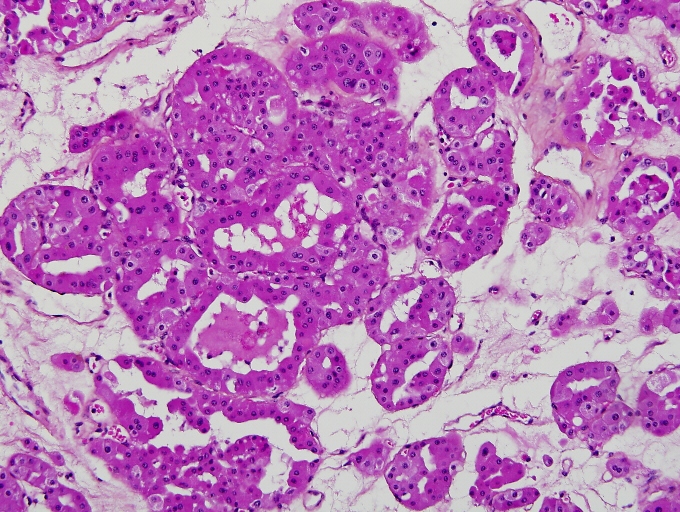
20x
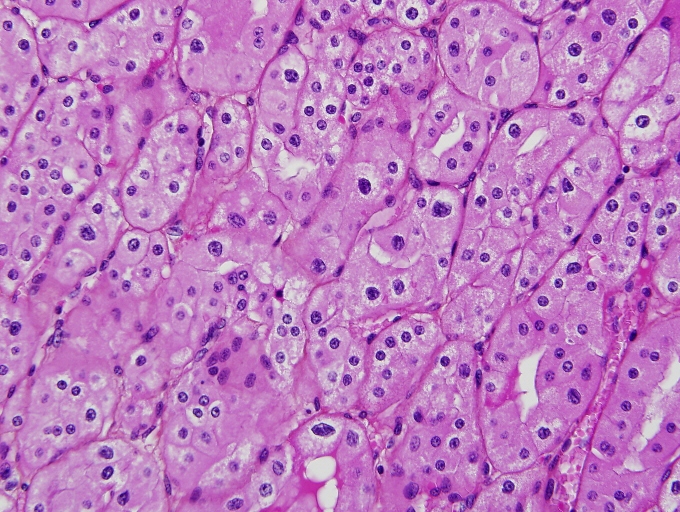
40x
What is your diagnosis?
Diagnosis:
Hybrid oncocytic - chromophobe tumor
Discussion:
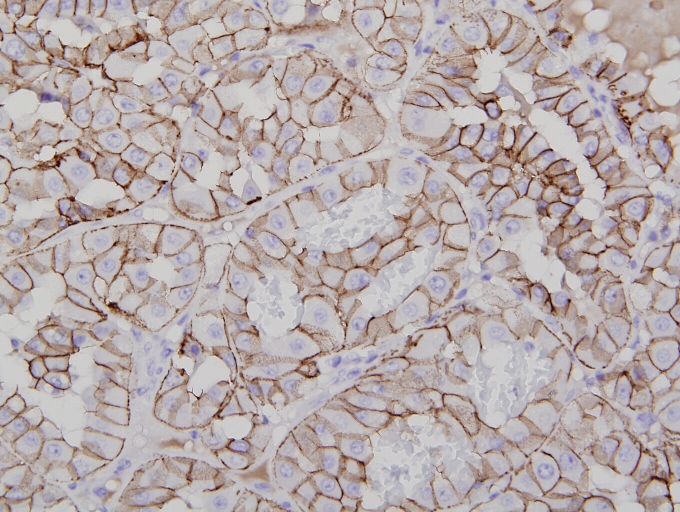
Immunostains were obtained:
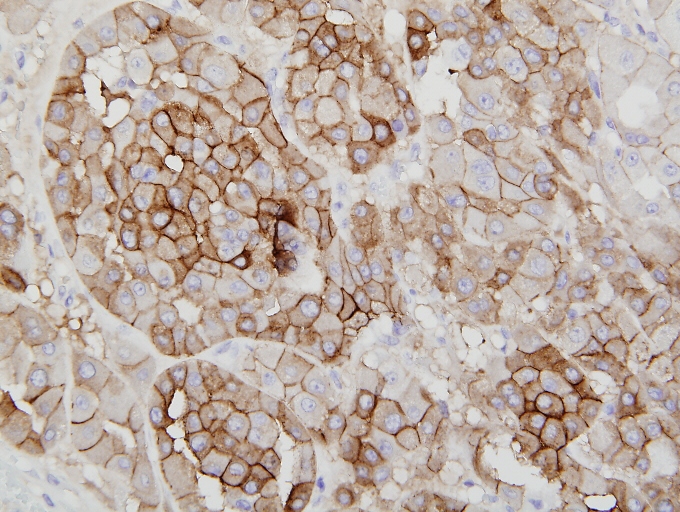
CD117
E-cadherin
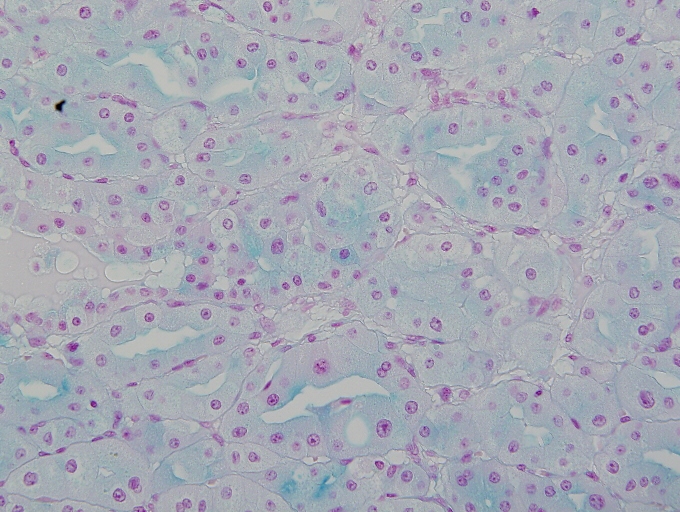
Hales colloidal iron
Histopathology shows a non-infiltrative, well circumscribed intrarenal tumor composed of neoplastic cells arranged in a solid, alveolar and cystic pattern. There is a dual population of eosinophilic cells. The oncocytic cells are medium sized, round and contain granular eosinophilic cytoplasm with a round concentric nucleus and a prominent nucleolus. The chromophobe cells are large and plant-like with a distinct cell membrane and flaky eosinophilic cytoplasm. A diagnostic clue is the presence of a perinuclear halo surrounding a wrinkled raisinoid nucleus. Focally, a third population of eosinophilic cells featuring both oncocytic and chromophobe morphology are seen. Mitoses are rare.
The neoplastic cells are positive for CD117, E-cadherin and focally for CK7. Hales colloidal iron stain shows both a cytoplasmic and luminal pattern.
Hybrid oncocytic-chromophobe tumor (HOCT) is rare renal neoplasm classified as a subcategory of chromophobe renal cell carcinoma (Am J Surg Pathol 2013;37:1469). HOCT can occur in three distinct clinical settings: sporadically, associated with renal oncocytomatosis and as a component of the Birt-Hogg-Dubé syndrome (Histol Histopathol 2013;28:1257). Birt-Hogg-Dubé syndrome is an autosomal dominant inherited disorder associated with a genetic abnormality on chromosome 17p11.2 leading to a mutation in the BHD gene. Clinical manifestations include spontaneous pneumothorax, multiple benign cutaneous follicular tumors (fibrofolliculoma, trichodiscoma and acrochordon), oncocytomatosis and multifocal chromophobe renal cell tumors (Pol J Pathol 2014;65:93).
HOCT is a distinct tumor with overlapping features of oncocytoma and chromophobe renal cell tumors (ChRCC), showing histopathologic and immunophenotypic features of each. Oncocytoma is negative for CK7 and shows a luminal pattern with Hales colloidal iron, and ChRCC is diffusely positive for CK7 and shows a cytoplasmic pattern with Hales colloidal iron; HOCT expresses a mixed immunophenotypic pattern (J Clin Pathol 2014;67:97).
The histopathologic differential diagnosis includes other eosinophilic renal cell neoplasms including oncocytic papillary renal cell carcinoma and eosinophilic clear cell renal cell carcinoma. Oncocytic papillary renal cell carcinoma has a papillary architecture, is negative for CD117, and is associated with a worse prognosis (Arch Pathol Lab Med 2014;138:1531). Eosinophilic clear cell renal cell carcinoma is composed of sheets of neoplastic cells separated by thin fibrous septa and containing a prominent vascular network. It expresses CD10, is negative for CD117 and is also associated with a worse prognosis (Arch Pathol Lab Med 2014;138:1531).
HOCT has a good prognosis and indolent behavior (Virchows Arch 2010;456:355). Its rarity and histologic subjectivity make it a diagnostic challenge for general pathologists. If tumors are multiple, this may be a clue to a diagnosis of BHD syndrome. Communication with the clinician in this case is essential to ensure appropriate clinical investigation and follow-up.
Discussion edited by Dr. Jennifer R. Kaley, University of Arkansas for Medical Sciences (USA).
