
5 March 2015 - Case of the Week #344
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Feriyl Bhaijee, University of Mississippi Medical Center (USA), for contributing this case.
Advertisement
Case #344
Clinical history:
A 2 year old boy presented with itchy brown skin macules (which were biopsied) but no associated systemic lesions.
Microscopic images:
What is your diagnosis?
Diagnosis: Urticaria pigmentosa (cutaneous mastocytosis)
Stains:
Discussion:
Urticaria pigmentosa, also called maculopapular mastocytosis, is the most common form of cutaneous mastocytosis. It typically presents in children with the onset of multiple red-brown macules on the extremities. It has an unknown cause and familial cases are rare.
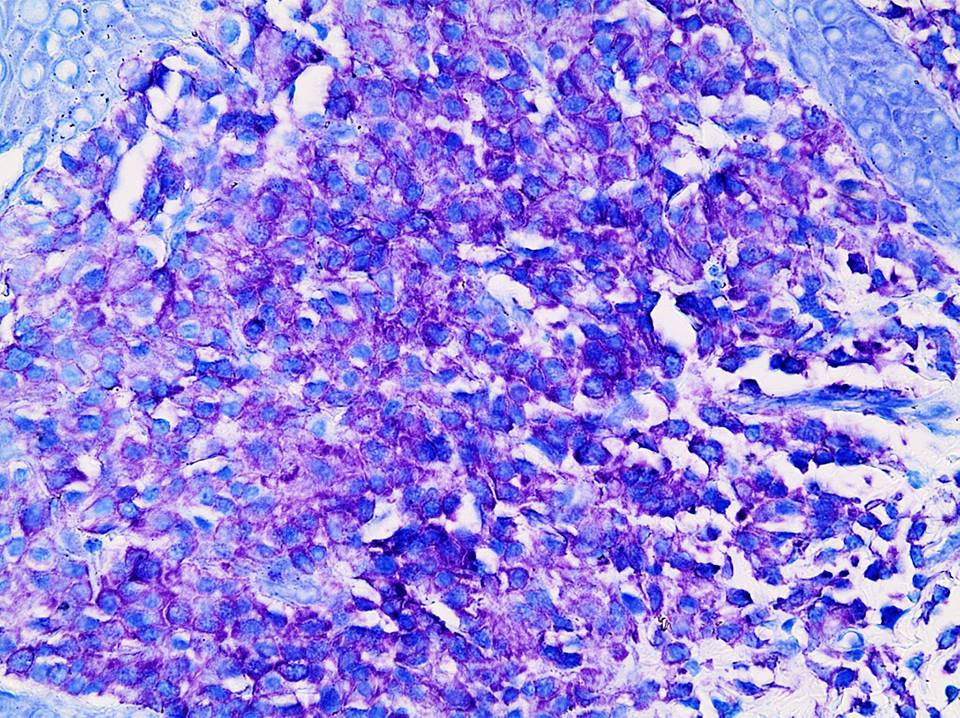
Histologically, there is mast cell infiltration of the papillary and upper reticular dermis and reactive basal hyperpigmentation of the overlying epidermis. The basophilic granules in the mast cells are metachromatic (red-purple) with toluidine blue and are often immunoreactive, as in this case, for mast cell tryptase and kit / CD117 (images not available). The differential diagnosis includes chronic dermatitis, if the mast cells are not identified.
In children, cutaneous mastocytosis is generally a benign disease that may present at birth and is often associated with mast cell mediator related symptoms including pruritus, flushing and abdominal pain with diarrhea. These symptoms may be triggered by physical stimuli, temperature changes, anxiety, medications and exercise; symptoms usually respond to topical and systemic antimediator therapy including antihistamines and cromolyn sodium (Pediatr Allergy Immunol Pulmonol 2013;26:175). Most cases undergo remission at puberty. Urticaria pigmentosa is associated with mast cell infiltration of the bone marrow in up to 60% of cases but this does not seem to predict an adverse clinical course (Am J Clin Pathol 1998;109:279).
The major concern is progression to systemic mastocytosis. In adolescents or adults, many of these cases may represent cutaneous involvement by systemic mastocytosis, which requires aggressive treatment (Mod Pathol 2014;27:19). Bone marrow studies are recommended if there is suspicion of progression of disease to an adult form, if cytoreductive therapy is contemplated or if skin lesions remain present or tryptase levels remain elevated after puberty (Am J Clin Dermatol 2011;12:259).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Feriyl Bhaijee, University of Mississippi Medical Center (USA), for contributing this case.

- WHO Classification of Tumours of Soft Tissue and Bone (2013) edited by C. D. M. Fletcher, J. A. Bridge, P. Hogendoorn and F. Mertens is the fifth volume of the 4th Edition of the WHO series on histological and genetic typing of human tumours.
- WHO Classification of Tumours of the Female Reproductive Organs (2014) by R.J. Kurman, M.L. Carcangiu, C.S. Herrington and R.H. Young is the sixth volume in the Fourth Edition of the WHO series on histological and genetic typing of human tumors. .
For more information, visit our Books page.
Case #344
Clinical history:
A 2 year old boy presented with itchy brown skin macules (which were biopsied) but no associated systemic lesions.
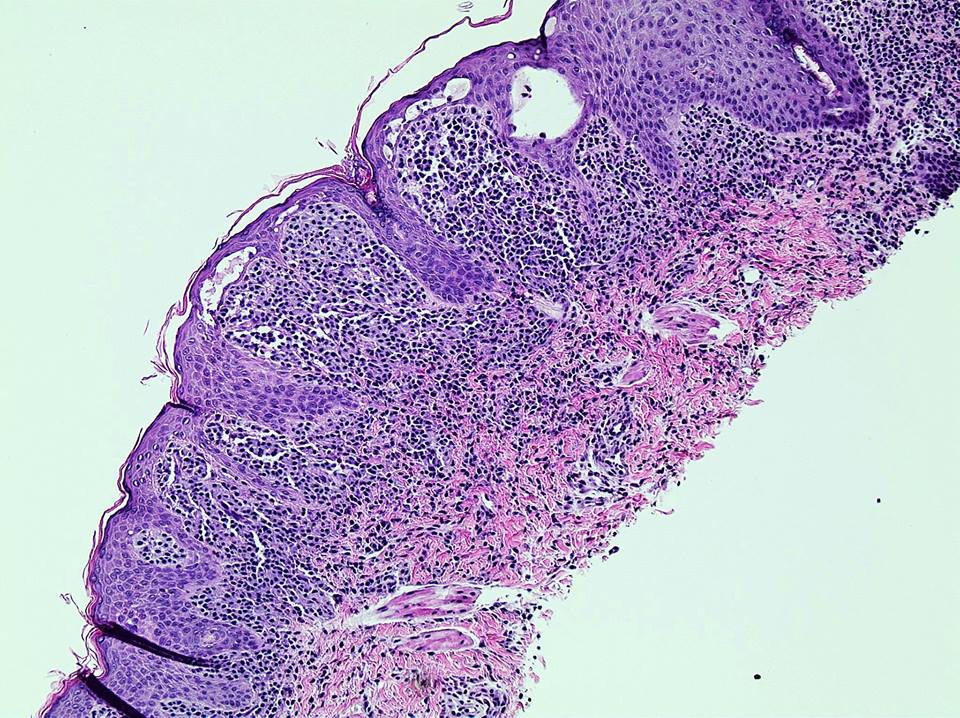
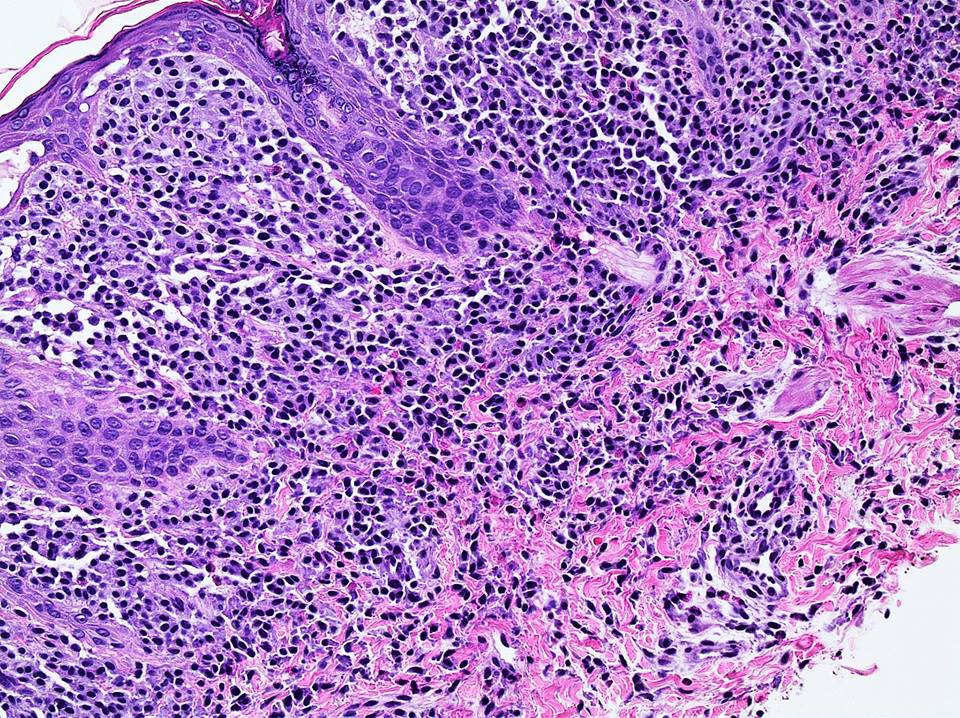
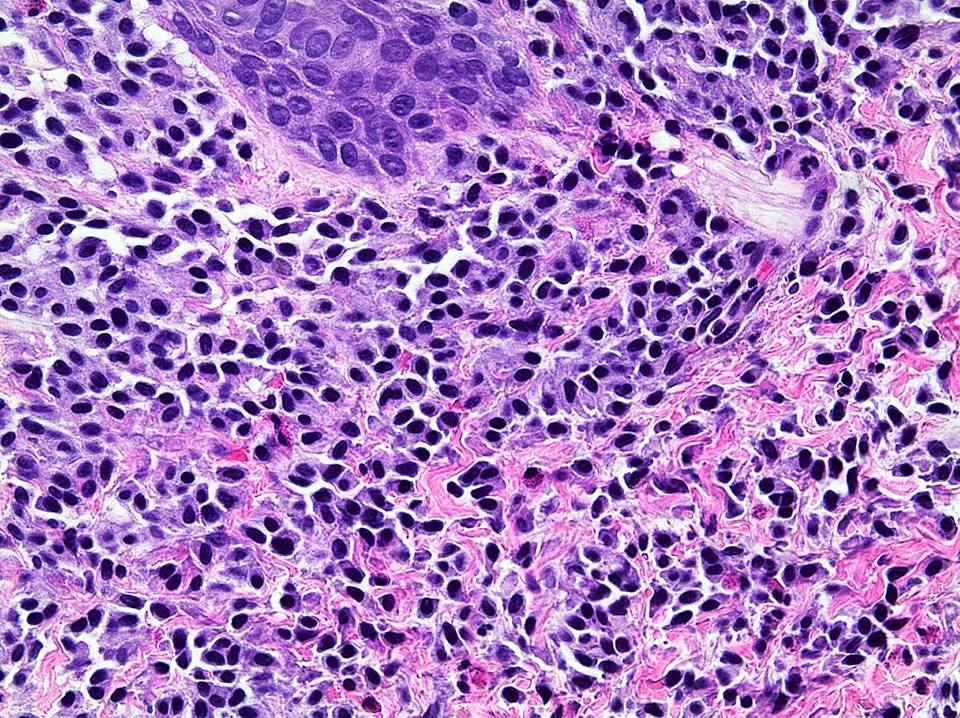
Microscopic images:
H&E
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Urticaria pigmentosa (cutaneous mastocytosis)
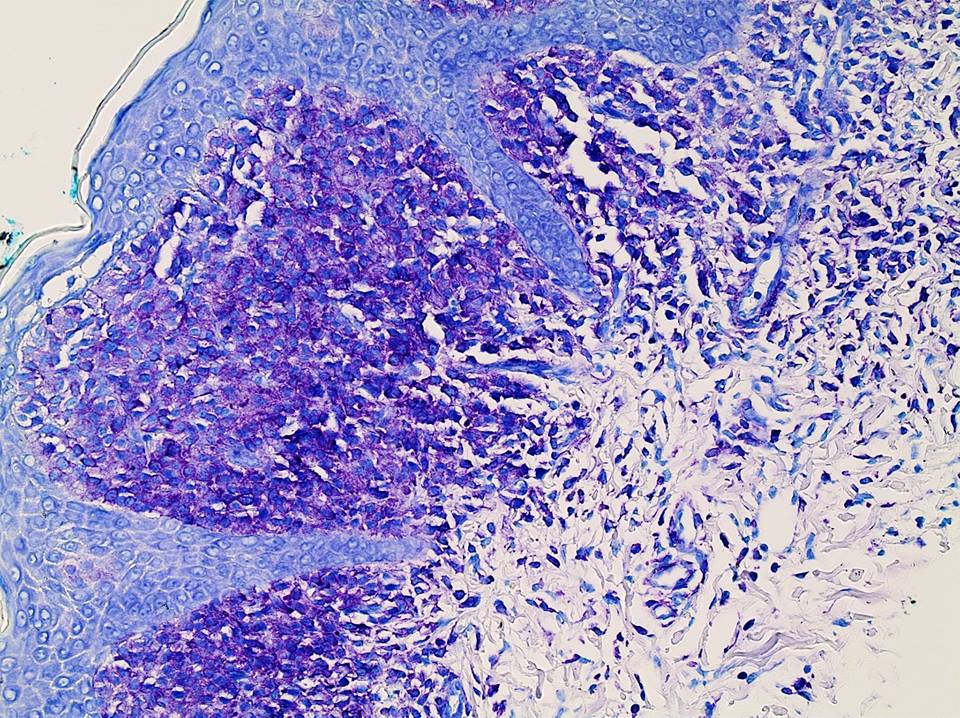
Stains:
Toluidine blue
Discussion:
Urticaria pigmentosa, also called maculopapular mastocytosis, is the most common form of cutaneous mastocytosis. It typically presents in children with the onset of multiple red-brown macules on the extremities. It has an unknown cause and familial cases are rare.
Histologically, there is mast cell infiltration of the papillary and upper reticular dermis and reactive basal hyperpigmentation of the overlying epidermis. The basophilic granules in the mast cells are metachromatic (red-purple) with toluidine blue and are often immunoreactive, as in this case, for mast cell tryptase and kit / CD117 (images not available). The differential diagnosis includes chronic dermatitis, if the mast cells are not identified.
In children, cutaneous mastocytosis is generally a benign disease that may present at birth and is often associated with mast cell mediator related symptoms including pruritus, flushing and abdominal pain with diarrhea. These symptoms may be triggered by physical stimuli, temperature changes, anxiety, medications and exercise; symptoms usually respond to topical and systemic antimediator therapy including antihistamines and cromolyn sodium (Pediatr Allergy Immunol Pulmonol 2013;26:175). Most cases undergo remission at puberty. Urticaria pigmentosa is associated with mast cell infiltration of the bone marrow in up to 60% of cases but this does not seem to predict an adverse clinical course (Am J Clin Pathol 1998;109:279).
The major concern is progression to systemic mastocytosis. In adolescents or adults, many of these cases may represent cutaneous involvement by systemic mastocytosis, which requires aggressive treatment (Mod Pathol 2014;27:19). Bone marrow studies are recommended if there is suspicion of progression of disease to an adult form, if cytoreductive therapy is contemplated or if skin lesions remain present or tryptase levels remain elevated after puberty (Am J Clin Dermatol 2011;12:259).
